
Abstract
Objective:
Numerous reviews have examined risk and protective factors for alcohol-related negative consequences, but no equivalent review of risk and protective factors exists for cannabis-related negative consequences (CRNCs)-a gap filled by the present study. This scoping review examined survey-based research of risk and protective factors for CRNCs such as neglecting responsibilities, blacking out, or needing more cannabis.
Methods:
Three databases (PubMed, PsycINFO, and Google Scholar) were searched for peer-reviewed manuscripts published between January 1, 1990, and December 31, 2021. A qualitative synthesis was performed using the matrix method and the results were organized using the socioecological model as a framework.
Results:
Eighty-three studies were included in the review. There was considerable variation in measures and operationalizations of CRNCs across studies. Risk factors were identified in the intrapersonal (depression, social anxiety, PTSD, impulsivity, sensation seeking, motives, expectancies), interpersonal/community (trauma, victimization, family and peer substance use, social norms), and social/policy (education, employment, community attachment, legalization, availability of substances) domains of influence. Protective behavioral strategies were a robust protective factor for CRNCs. Males consistently reported more CRNCs than females, but there were no differences observed across race.
Conclusions:
Future research should identify person- and product-specific patterns of CRNCs to refine theoretical models of cannabis misuse and addiction. Public health interventions to reduce the risk of negative consequences from cannabis should consider utilizing multilevel interventions to attenuate the cumulative risk from a combination of psychological, contextual, and social influences.
From policy to practice, there have been notable changes in the public perception of cannabis use including public support for state-level changes in the medicalization and legalization of cannabis throughout the United States,1,2 and changes in modes of consumption including the rise of “vaping” THC.3,4 Not surprisingly, as attitudes toward cannabis use (or marijuana use) have become more favorable, the prevalence of cannabis use has increased from 10.4% in 2002 to 15.4% in 2017, 5 and among adults in the United States, cannabis use disorder (CUD; being unable to stop using cannabis despite it causing health and social problems) treatment rates have increased. Cannabis use has been linked to long-term adverse health outcomes including vaping-induced lung injury, cardiovascular problems, and mental illness.6-8 Therefore, identifying what factors are associated with the proximal consequences of cannabis use is an important step toward developing prevention and intervention programs that can interrupt the progression toward disorder (eg, cannabis use disorder) and potential downstream negative outcomes.
Cannabis-related negative consequences (CRNCs) are defined here as the harmful effects for users in the psychological (needing more cannabis to get high, etc.), interpersonal (getting into fights with friends or family, etc.) and social (being late for school/work, etc.) domains. 9 While there are merits to examining the associations between substance use and specific consequences—such as driving under the influence—most research tends to aggregate negative consequences to ascertain the global burden of substance use on overall health and well-being. Self-report assessments measuring CRNCs include, among others, the Marijuana Problem Scale (19-items; example “Has marijuana ever caused you to neglect your family”), 10 the Marijuana Problem Index (29-items, example “Passed out or fainted suddenly”), 11 the Cannabis Problems Questionnaire (27-items, example “Have you felt more antisocial after smoking?”), 12 and the Marijuana Consequences Questionnaire (50-items, example “I haven’t been as sharp mentally because of my marijuana use”), 13 Reviews of psychometric properties and the application of these scales in community and clinical practice are available elsewhere.14,15
Some of the aforementioned scales assessing CRNCs have been adopted from research investigating alcohol-related negative consequences (ARNCs) with “marijuana” being substituted for “alcohol” in some cases. As such, it is pertinent to consider the breadth of evidence explaining experiences of ARNCs as this has likely influenced the existing work done to document and describe experiences of CRNCs. To date, there have been several reviews of ARNCs, or problem alcohol use, across multiple populations (youth, college students, adults, treatment seeking populations, clinical populations, etc.). Zucker et al 16 reviewed early developmental processes in relation to underage drinking and problem drinking while other researchers have focused on predictors of co-occurring problems involving alcohol 17 or initiation of alcohol in adolescence leading to future problem alcohol use. 18 Grigsby et al 19 documented risk and protective factors for ARNCs among adolescents noting important psychological (eg, impulsivity and sensation seeking), interpersonal (eg, peer use, family history) and societal influences (eg, media exposure) as well as differences by demographic characteristics (such as sex or gender and race or ethnicity). Not surprisingly, most reviews on ARNCs have focused on college student populations20-23 as these are the peak years for risky alcohol use behavior and diagnosis of alcohol dependence. 24
This is not the first review to explore the causes and consequences of cannabis use though many have focused on a narrow set of adverse physical, behavioral, or social outcomes. A review of neuropsychological studies 25 found that adolescents who use cannabis heavily tend to have disadvantaged attention, learning, and processing speed; subtle abnormalities in brain structure; increased activation during cognitive tasks despite intact performance; and compromised objective indicators of sleep quality. Gordon et al 26 described the extant evidence base indicating that cannabis has physical health effects on humans—particularly diseases of the liver—aside from mental and behavioral health, and societal morbidity. Blavos et al 27 reviewed cannabis use among college students and identified 7 studies assessing CRNCs measured as academic problems, legal issues, enrollment disruptions and unsafe sexual practices and a few that focused on substance-related traffic risk, including driving while high or riding with a driver who was high. Two of the studies examined neurobiological consequences and reasons for cannabis use, and one focused on physical health outcomes. One meta-analysis 28 identified cannabis use frequency and quantity had a medium-sized association with consequences although there were high levels of heterogeneity and differences across the self-report measure used. Pearson 28 concluded that additional factors—psychological, behavioral, and social correlates of substance (ie, risk and protective factors)—are likely important in predicting who does and does not experience CRNCs. As such, this review fills an important gap in the literature by synthesizing existing research focused on risk and protective factors for CRNCs in non-institutionalized populations across multiple domains of functioning using standardized measures (described above). In addition to explaining factors that might contribute to risk for experiencing CRNCs beyond cannabis use behavior itself, this review can assist practitioners with identifying potential intervention targets.
Organization and categorization of results in this review are guided by asocial-ecological framework. 29 The social-ecological model considers the complex interplay between individual, relational, community, and societal factors in predicting and explaining health behaviors. Moreover, this model can benefit practitioners by identifying intervention targets for reducing cannabis use and related consequences by summarizing the independent and combined contributions of individual (eg, expectancies, motives, beliefs, and attitudes), relational (eg, peers, family, teachers), community (eg, media messaging, school, and work policies), and societal factors (eg, media, policy, built environment) that influence the likelihood of experiencing CRNCs. This is crucial for the development of community-based intervention programs. While the social ecological model can inform social or policy intervention targets—changes beyond the individual level—it does not provide guidance on specific variables within those levels of influence that should be targeted. As such, identifying mediators (ie, a variable that explains the process through which 2 variables are related) and moderators (ie, variables that influence the strength or direction of a relationship between 2 variables) at various levels of influence can increase the efficacy of interventions and improve our ability to customize them for specific populations or across contexts.
Current study
Experiencing recurring CRNCs is likely indicative of a pattern of misuse, and potentially an early warning sign of addiction and future diagnosis of CUD. 30 Describing the methods, measures and correlates used to study the incidence, prevalence, and etiology of CRNCs can guide clinical and public health professionals in developing screening and early intervention protocols for cannabis users experiencing use related negative consequences. The goal of the present review is to examine the literature on risk and protective factors for CRNCs (ie, problematic cannabis use) in observational research with community populations.
Methods
The PRISMA for Scoping Reviews (PRISMA-ScR) statement 31 has been followed where applicable to ensure accuracy and transparency of this review and its methodology (Supplemental Table 1). No protocol was published in advance. Computer-based searches of Google Scholar, PubMed, and PsycINFO were conducted to search for publications between January 1, 1990, and December 31, 2021 (see Supplemental Table 2 for sample search strategy). We combined search terms for cannabis use (marijuana, cannabis, THC), negative consequences (abuse, misuse, problem, problematic, “negative consequence”), and study design (survey, questionnaire, self-report). Additionally, we searched the “cited by” articles in Google Scholar of validated CRNC scales described in the introduction. The combination of reference and keyword searches increases the likelihood of identifying articles using validated and non-validated measures of CRNCs. A total of 83 manuscripts were included in the final review. Figure 1 provides a flow diagram for the literature search and selection process.
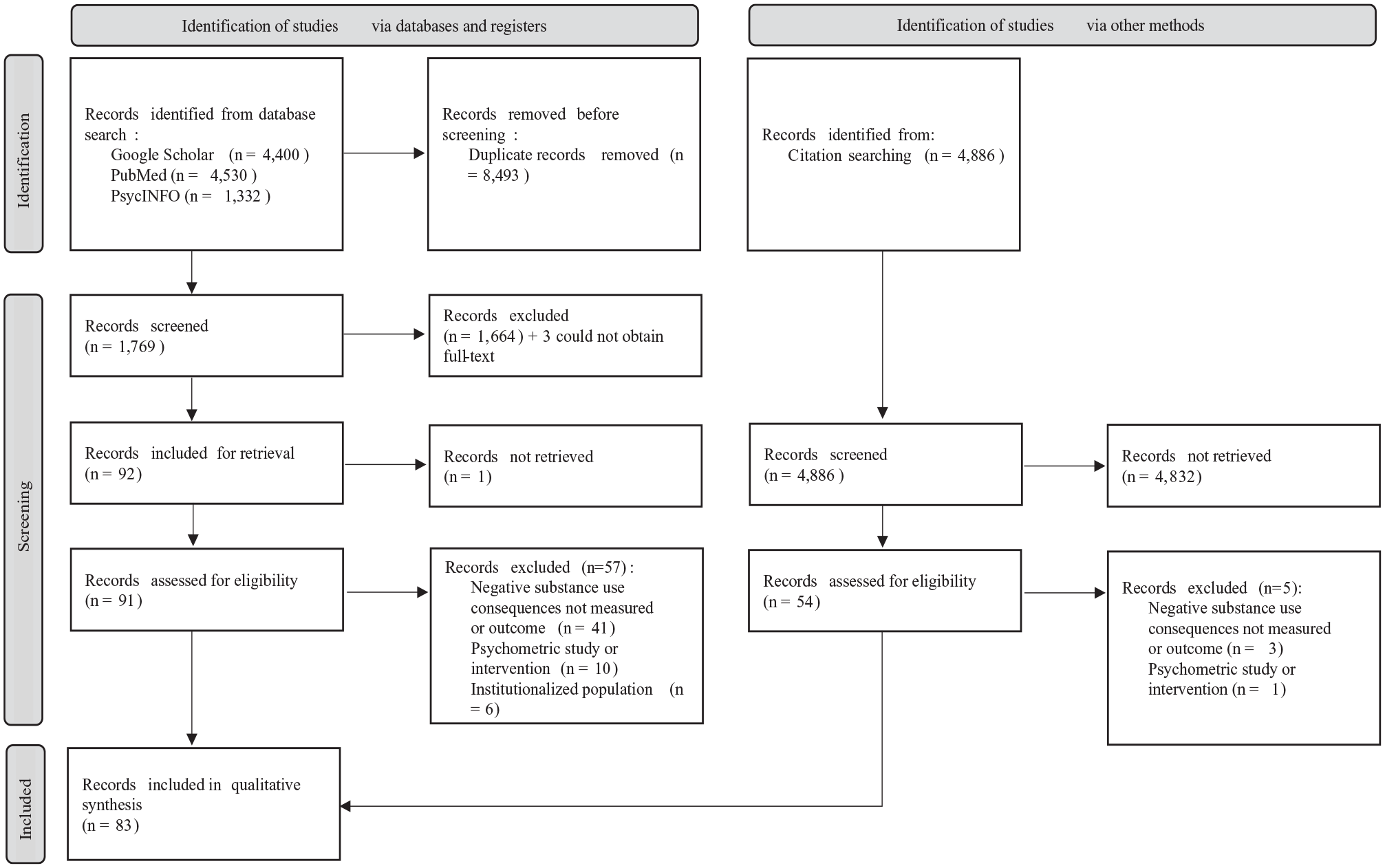
PRISMA flow chart.
The following inclusion criteria were used to select articles for the review: (1) the outcome was cannabis-related negative consequences, (2) the data were from observational research with any time frame (cross-sectional, prospective, retrospective), (3) the sample was non-clinical, and (4) the work was published in an English language peer-reviewed journal. Articles were excluded if (a) authors reported consequences of alcohol use or other drugs (eg, stimulants, opioids, hallucinogens) as the sole outcome, (b) CRNCs were a predictor of other health or behavior outcomes, (c) the study reported results of an intervention or treatment to reduce CRNCs, or (d) the article was a methodological study, experimental study, or a non-peer reviewed work. Studies that defined the outcome of interest as a risky behavior (eg, escalation of use, transition from one drug to another) were not considered as we were not interested in frequency or quantity of use as the outcome, but rather in the negative consequences that result from cannabis use (eg, accidents, injuries, neglecting responsibilities). Articles were screened at the title and abstract stage by 2 co-authors and the at the full-text stage by the lead author. Differences of views about inclusion were resolved through discussion and consensus with the other authors.
Data extraction and information synthesis
We consulted the Matrix Method guidelines 32 for data extraction and information synthesis of the literature. The lead author and 2 co-authors abstracted author names and year of publication, study design (cross sectional, follow-up with data from 2 time points or longitudinal with data from 3 or more time points), sample characteristics (sample size, age, sex or gender, race or ethnicity), hypothesized predictors, mediators, moderators, and covariates, measurement and operationalization of negative consequences, and a summary of the main findings. We structured the results section and associated tables using the social-ecological model as a framework. As such, themes of risk and protective factors for CRNCs are presented within the theoretical domain (eg, level of influence) of the appropriate predictor including intrapersonal factors (those influencing behavior such as knowledge, attitudes, beliefs, mental health, and personality), interpersonal factors (social norms and relationships with family and peers), and social/policy factors (community attachment, drug use policy and availability, social determinants of health). We also investigated the influence of frequency and quantity of use. Finally, we explore gender and racial/ethnic differences in (a) predictors of CRNCs and (b) types and patterns of CRNCs experienced.
Results
Cannabis-related negative consequences (CRNCs) were the main outcome of all studies; however, some reports described the outcome as “cannabis abuse,” “problem use,” “cannabis use problems,” “cannabis misuse,” or “problematic cannabis use.” When interpreting the findings of this review there are 2 important considerations; first, a combination of validated, investigator-modified, and investigator-created self-report measures were used (Table 1), and the conceptualization and operationalization of CRNCs varied as a result—like review findings for alcohol-related negative consequences. 19 Second, negative consequences were observed over different time periods (ie, past week, past month, past year, etc.) and settings (ie, school based, community based). As shown in Table 1, the majority of studies (n = 83) identified in this review were cross-sectional (75.9%). The main findings of studies are presented in Supplemental Table 1.
Authors and year of publication, CRNC scale used, research design/setting, and sample characteristics for studies included in review.

Abbreviations: C, cross sectional; F-U, follow-up (2 time points); L, longitudinal (3+ time points).
Cannabis use behaviors (Age of onset, frequency & quantity of use, product type)
There was no evidence of a linear, or dose-response, association between frequency of cannabis use (number of times used over a predefined time frame) and experience of CRNCs across 3 longitudinal,33-35 2 cross-sectional36,37 studies. Age of initiation was discussed in several cross-sectional studies,38-43 but the association between age at first use and the risk of experiencing CRNCs remains unclear with no evidence of direct effects. Frequency of use was a significant mediator for substance use motives 44 and experiencing CRNCs in another cross-sectional study. Frequency of use reduced the significant association between urgency and cannabis problems to non-significance in one cross-sectional study 45 and Luba et al ’s 46 cross-sectional analysis showed that as the level of savoring (ie, the ability to recognize and appreciate positive experiences) decreased, the association between frequency of cannabis use and related consequences increased. High potency THC concentration was associated with increased odds of experiencing CRNCs among adolescents in a longitudinal study 47 and young adult college students in a cross-sectional study, 48 but potency did not predict dependence scores in another cross-sectional study of adults. 49 One cross-sectional analysis 50 identified a frequency-by-quantity interaction where CRNCs decreased as frequency increased, and vice versa while another cross-sectional study found wide variation in perceptions, use, and CRNCs. 51 Two longitudinal studies52,53 and 2 cross-sectional studies36,37 suggest severity of CRNCs may be a function of cannabis product use, product types, and patterns. Lastly, one cross-sectional study reported young adults endorsing CUD criteria reported more types of cannabis related problems, 54 and another longitudinal study showed that problems grow as individuals transition from adolescence to young adulthood. 55
Intrapersonal influences
Anxiety and depression
Experiencing stressful life events and reporting higher perceived stress is associated with more CRNCs and were moderated by level of emotion dysregulation in one cross-sectional study. 56 Multiple forms of anxiety were investigated in relation to CRNCs; however, all studies were cross-sectional in nature. There is limited and mixed evidence to support social anxiety as a direct predictor of CRNCs.57,58 Social anxiety may moderate the association between social norms and cannabis use problems, 59 and one study reported social anxiety was indirectly associated with cannabis-related problems through solitary use frequency. 60 Social anxiety was also associated with CRNCs via underutilization of protective behavioral strategies (ie, planned behaviors to decrease the use of cannabis) and serial effects with cannabis use frequency and peak quantity 61 as well as the effect on negative and positive affect and sequential effects on frequency of use and problems. 62 For men, but not women, the association between social anxiety symptoms and cannabis use problems may be mediated by safety behaviors—cognitive or behavioral strategies used to mitigate social anxiety, such as avoiding eye contact. 63 Anxiety sensitivity might also be a correlate of CRNCs 64 though evidence is scant. One study identified symptom severity of obsessive-compulsive disorder (OCD) as a significant correlate of CRNCs after adjusting for stress, depression, and general anxiety 65 while another study found features of schizotypy a were associated with CRNCs cross-sectionally and prospectively. 33 Psychological factors were examined in several studies as a predictor and mediator of CRNCs. Depression and depressive symptomology were a significant predictor of CRNCs in one longitudinal study 34 and across 3 cross-sectional studies58,60,66 and was a confounder of associations in a cross-sectional study. 67
Impulsivity and sensation seeking
Impulsivity is acting, or tending to act suddenly, without careful forethought of the outcome of ones’ actions that has been conceptualized as a multidimensional construct comprising elements of a state (thoughts or behaviors unique to a point in time) and trait (a pattern of characteristics that generalize across time). 68 Several cross-sectional studies described an association between higher scores on self-reported impulsivity measures and the experiences of CRNCs.44,57,69-71 Sensation seeking—the trait of seeking novel and intense experiences—was also significantly associated with CRNCs45,70,72 with one exception, a significant, negative association to CRNCs among persons with relatively low use of protective behavioral strategies (ie, acting as a mediator for the risk and protective factors of cannabis consequences). 73 There were no longitudinal studies investigating this relationship identified in our search.
Motives and expectancies
Substance use motives refer to reasons for using drugs, such as coping with distress or enhancing a positive mood, whereas expectancies represent “if-then” contingencies regarding the outcome of a substance use behavior. Motives were generally categorized as positive (including social and enhancement motives) and negative (including conformity and coping motives). One longitudinal study showed CRNCs were associated with positive motives 74 whereas reporting more negative motives, specifically coping motives, were associated with more CRNCs in cross sectional studies38,44,64,73,75-77 though one cross-sectional study found CRNCs were associated with both positive and negative motives. 78 One longitudinal study of cannabis users 74 reported expansion motives as having the strongest association to CRNCs with conformity motives having a null association with cannabis problems when all motives were modeled simultaneously while another follow-up (2 time point) study indicated coping-related motives prospectively predicted problems. 79 Three cross-sectional studies suggested that motives mediate the association between psychological symptoms and CRNCs65,80 and hostility and CRNCs. 75 One longitudinal study 81 found that reporting a high number of motives to abstain buffered the influence of negative reinforcement motives on the experience of cannabis-related problems in young adulthood. Only 3 cross-sectional studies examined the role of expectancies with CRNCs. One described how an individuals’ expectancies that cannabis causes cognitive and behavioral impairment was negatively associated with cannabis use disorder criteria. 40 The second found that higher scores on the cessation expectancy questionnaire and Marijuana Effects Expectancy Questionnaire predicted higher scores on the Drug Abuse Screening Test (DAST—a self-report assessment that screens for drug abuse and drug dependence disorders) among young adult users. 82 Finally, a latent class analysis of motives and expectancies 83 identified the “high motives and high expectancies” class scored significantly higher than the “low motives and low expectancies” class on the total score and both subscales of the Cannabis Use Problems Identification Test (CUPIT—a self-report assessment that identify present and potential harmful cannabis use), indicating worse problematic cannabis use and impaired control.
Protective Behavioral Strategies (PBS)
PBS are behaviors that individuals use before, during, or after initiating substance use to reduce consumption, intoxication, and related adverse outcomes such as blacking out. Examples of PBS include setting limits on how much or how often one uses, not mixing cannabis with other substances, and using only around trusted peers. The measurement used to assess PBS for cannabis misuse across identified studies was the Protective Behavioral Strategies for Marijuana Scale. Across 8 cross-sectional studies there was clear evidence that reporting more PBS is associated with fewer negative consequences from cannabis use.38,73,78,84-88 PBS were also found to mediate, cross-sectionally, the association between risk factors and CRNCs, such as risk and experience seeking, 84 demographic factors (eg, sexual orientation 85 ), and cannabis self-identity, 89 Of note, one study 78 found that no single PBS was significantly associated with CRNCs using a within-subject statistical approach which may suggest that cumulative PBS, rather than specific PBS, are beneficial to reducing CRNCs. No longitudinal investigations of direct relationships between PBS and CRNCs were identified.
Other potential intrapersonal influences
There is emerging evidence from 2 cross-sectional studies that higher scores on measures of refusal self-efficacy might be associated with reduced frequency of CRNCs.86,90 One longitudinal study 35 and one cross sectional study 91 identified that using cannabis as a sleep aid was associated with past month and past year CRNCs, respectively, but not daily consequences as shown in one follow-up study. 92 Finally, one cross-sectional study indicated that insomnia severity was a predictor of CRNCs in another study and possibly mediated by mood and moderated by gender. 93 Delayed memory was not associated with CUD onset among teens in one longitudinal study, 94 and findings of a cross-sectional study suggest dimensions of repetitive negative thinking is not associated with cannabis use problem severity although dimensions of metacognitive thinking are. 95 In a longitudinal study, cannabis-harm implicit association test scores significantly predicted concurrent risk of CUD and use such that stronger cannabis-harm associations were associated with less use and risk of CUD. 96 Finally, harmonious passion was a stronger predictor of increased consumption than was obsessive passion, whereas obsessive passion was a stronger predictor of CRNCs longitudinally. 97
Interpersonal influences
Experiences of stigma and trauma
Cross-sectional evidence suggests that unlike internalized stigma (ie, an individual applies negative beliefs of their mental illness to oneself), perceived stigma (ie, an individual’s viewpoints on how others discriminated) was not associated with CRNCs, 98 but CRNCs were associated with experiences of general victimization. 81 Lastly, cross-sectional studies suggest exposure to traumatic events (eg, adverse childhood experiences or childhood trauma) is associated with CRNCs39,99 and may be mediated by negative urgency. 45 In a longitudinal study, posttraumatic stress disorder (PTSD—a psychiatric condition that may affect individuals who see or go through a traumatic event) was prospectively associated with CUD symptoms in a sample of veterans. 34 In a cross-sectional study using a double mediation model, 100 PTSD was associated with use of fewer PBS strategies that in turn was associated with higher cannabis use frequency/quantity, which was associated with more CRNCs.
Family and friends
One longitudinal study showed that obtaining cannabis from family or friends was associated with reduced odds of experiencing cannabis problems compared to purchasing cannabis for medicinal or recreational purposes. 101 In a cross-sectional study, the number of friends reported using cannabis mediated the relationship between cannabis onset age use and CRNCs. 102
Social norms
Several cross-sectional studies, but no longitudinal studies, investigated the relationship of social norms and CRNCs. In a college student sample, descriptive norms (ie, how people behave based on our observations) and injunctive norms (ie, what we think others approve or disapprove of) had unique negative direct effects on CRNCs. 70 In another college sample, for students reporting cannabis use as central to their identity, injunctive norms were positively associated with consequences. 89 Descriptive norms were positively associated with CRNCs for students with a “weak marijuana identity” but were negatively associated with consequences for those with a “strong marijuana identity.” 70 Ecker and Buckner 59 identified a significant interaction between social anxiety and peer descriptive norms as well as social anxiety and parental injunctive norms on cannabis use problems while Ecker et al and colleagues found African-American college students reported more permissive perceived parental injunctive norms was related to greater severity of cannabis-related problem severity. 103
Societal/policy influences
Community membership
Two longitudinal studies,101,104 one cross-sectional study 105 showed that possessing a medicinal cannabis card (provided by a medical doctor to purchase cannabis for medicinal purposes) was associated with an increased odds of experiencing CRNCs. However, in a cross-sectional study of medicinal users, those reporting use for chronic pain reported fewer problems than those using it for other medicinal purposes. 106
College cannabis use culture, where affinity for use was greater, mediated the effects of sensation seeking and impulsivity on CRNCs in a cross-sectional analysis. 70 Dyar et al 107 found that among cisgender minority women and minority non-binary individuals, using cannabis with sexual minority women and non-binary individuals, but not with sexual minority men, heterosexual men, or women, was associated with increases in problematic use 6-months later.
Drug use policy and availability
Legalization of cannabis predicted 17% of the variance of CRNCs in a study of young adults, but legalization status did not moderate the association between impulsivity and CRNCs. 69 Individuals with the strongest belief that legalization impacted their attitudes and beliefs about cannabis use reported the greatest number of CRNCs. 108 Estoup et al 109 reported that cannabis legalization and perceived risk of use explained 22% of the variance in reported CRNCs, and perceived risk mediated the association between legalization and consequences. There were no longitudinal studies investigating the effect of legalization on experiences of CRNCs.
One recent longitudinal study found that increases in the total number of cannabis sources (dispensary, retailer, family, friend, stranger/dealer) was associated with increases in CRNCs and cannabis use disorder symptoms. 101 Moreover, the researchers noted that the total number of consequences was significantly greater for persons acquiring cannabis from strangers/dealers or institutions relative to family and friends. A cross-sectional study 110 found that availability and exposure to consumption situations was associated with problematic cannabis use among men, but not women. Finally, exposure to cannabis advertisements on social media platforms was associated with an increased odds of CUD among adolescents in a cross-sectional analysis. 111
Education, employment, and socioeconomic status
In a longitudinal study, men between 18 and 33 years of age with limited postsecondary education had the highest rates of cannabis-related problems. 112 In another longitudinal study, cannabis use frequency and related problems were strongly related in disadvantaged communities, whereas in less disadvantaged communities, cannabis use quantity and problems were not significantly associated. 113 A cross-sectional study evidenced that psychological consequences from cannabis use were more common among individuals with lower educational attainment. 41 One cross-sectional study 114 reported that income was associated with cannabis use problems, but specific associations were not presented while another cross-sectional study in Spain 110 identified education level and work status as important correlates of problem cannabis use with higher proportions of problem users in the lower education and unemployed categories.
Overall differences by sex and gender
Of the 3 longitudinal studies,11,74,101 8 cross-sectional studies38,55,58,86,91,99,110,115 that explored sex and gender differences, males consistently reported more cumulative negative consequences than females. One moderated mediation analysis found that coping motives had a stronger mediational association between distress tolerance scores and cannabis related problems among distress intolerant women compared to men—though a cross-sectional approach was used. 80 One longitudinal study and one cross-sectional study reported no difference in the experience of CRNCs between men and women.46,107 Readers should note that the terms sex and gender were used interchangeably across studies and did not necessarily reflect one’s sex assigned at birth compared to their preferred identity.
Overall differences by race
While multiple studies controlled for race or ethnicity as a covariate in analyses, only 3 cross-sectional studies investigated race differences in CRNCs.91,103,114 Drazdowski et al 91 found no differences in past month or past year CRNCs between White and non-White participants. Race moderated the relationship between injunctive norms regarding parents and cannabis-related problem severity for African-American, but not Caucasian college students. 103 Specifically, more permissive perceived parental injunctive norms was related to greater cannabis-related problem severity (but not cannabis use frequency) for African-American participants. Finally, Brooks Holliday and Pedersen 114 noted significant race differences in cannabis misuse but did not elaborate on specific associations.
Discussion
As there have been no previous literature reviews describing risk and protective factors for negative consequences of drugs other than alcohol, this review builds on extant literature documenting the complexity of interactions that contribute to risk for negative consequences associated with cannabis use behavior. In line with previous reviews, 28 there was a modest, yet varied, association between frequency or quantity of cannabis use and experiences of related negative consequences—a finding also observed with alcohol use consequences. 116 It is likely that the associations between cannabis use frequency and a sum of predefined number of self-reported negative consequence items represents an artificial upper boundary of associations between cannabis use and adverse outcomes 28 or that self-report assessments do not sufficiently capture individual differences in patterns of substance misuse (ie, patterns of consequences may be unique to individuals or there are adverse outcomes that are not being assessed in existing measures leading to underreporting). In examining negative events resulting from cannabis use as independent outcomes, compared with a sum of experiences, researchers may be better positioned to identify person-centered patterns of CRNCs and develop effective secondary prevention programs to reduce immediate risk of harm and chances of escalating to the threshold of CUD. In addition, researchers can characterize cannabis misuse with greater specificity by ascertaining multiple measures of use—including frequency, quantity, and duration of use—that contextualize the patterns of use amongst those experiencing CRNCs.
Similar to reviews on alcohol-related negative consequences, 19 most studies included in the present review investigated intrapersonal (ie, psychological) predictors of CRNCs. Mental health issues, such as anxiety and psychological distress, appear to be important correlates of CRNCs and should be addressed in substance misuse prevention programing. Some individuals undergoing treatment for a substance use disorder might also require services that address concurrent mental illness, 117 a finding that underscores the need to address ongoing mental health concerns among individuals reporting substance misuse. 118 Personality traits might also play an important role in our understanding of who does and does not experience CRNCs as they do in research on alcohol consequences. 19 A review of controlled laboratory studies 119 identified impulsivity as a facilitator and consequence of drug use which suggests that some personality traits, like impulsivity, are exacerbated by drug use and might contribute to more frequent, and perhaps more severe consequences as use escalates. In fact, low levels of impulsivity has been described as a predictor of treatment success. 120 The next logical step in this line of inquiry is to explore whether interventions to lower impulsivity would predict success in secondary prevention interventions to reduce CRNCs among those who do not have a clinical disorder (ie, CUD).
Such associations may not be limited to impulsivity alone as we found evidence that sensation- and risk-seeking might engender problematic cannabis use behaviors as well. As demonstrated previously, sensation-seeking is a quantitatively distinct phenomenon from impulsivity 68 and more work is needed to explore how these unique traits influence problematic cannabis use. To accomplish this, longitudinal studies that can establish baseline personality traits and examine trends over time as individuals initiate and escalate their cannabis use are needed. Motives, but not expectancies, were investigated frequently as a predictor of CRNCs with coping motives emerging as a robust risk factor.38,73,79 As suggested by mediational findings, individuals using substances to cope with underlying mental health issues are likely at risk for problematic substance use. The only protective factor identified in this review that would be more amenable to modification were protective behavioral strategies (PBS)—a trend that aligns with alcohol research. PBS were generally defined as the approaches individuals used to reduce the quantity and frequency of cannabis use in order to avoid adverse outcomes (ie, CRNCs). Of note, it appears no single PBS reduces the odds of experiencing CRNCs, but that the use of multiple PBS can attenuate the risk of experiencing adverse outcomes following cannabis use. As such, interventions should prioritize the teaching of multiple methods or consider developing individualized plans for users based on their perceived helpfulness of a particular strategy, self-efficacy to employ a specific strategy, and patterns of use. Researchers should also consider investigating other factors (eg, religiosity) that have been identified as protective against alcohol-related consequences,19,121 but have not been examined in relation to cannabis.
While the literature has documented the influence of peers and family members on substance use initiation and frequency/quantity of use,122-124 there is significantly less research exploring the role of peer/family influence on experiences of CRNCs. Given the clear association between peer/family use and alcohol consequences19,125,126 more work is needed to understand the importance of peer and family influences to determine whether family-based or social network interventions could facilitate a reduction in CRNCs among cannabis users. Previous research has described the impact of social and cultural norms in initiation of drug use,127,128 and findings from this review suggest that social norms also contribute to CRNCs. Injunctive norms may be particularly important for youth who have not fully established their personal and social identity and turn to peers for approval of their beliefs and actions. Conversely, norms-focused interventions (eg, normative feedback) have shown effectiveness at reducing alcohol use and related consequences 129 as well as general substance use 130 and should continue being used to offset pro-drug use social and cultural norms that might influence experiences of CRNCs.
Education and income were 2 important social determinants that had an inverse association with CRNCs. That is, the odds or frequency of CRNCs decreased as education and income increased. Policies addressing these social determinants can have sweeping, downstream effects on health and continued efforts to address ongoing economic disparities can reduce the economic and social costs associated with problematic cannabis use. At the community level, efforts are needed to reduce pro-drug cultures (eg, alcohol and drug use are commonplace in college culture) that promote heavy or more frequent use that can lead for example, to more college students experiencing CRNCs. Similarly, initiatives to protect vulnerable communities, such as sexual and gender diverse populations and veterans from experiences of trauma and stigma, important risk factors for SRNCs identified in the present review, may help mitigate risk for CRNCs. As policies challenging the legality of cannabis and new state-level policies across the US decriminalize or legalize recreational cannabis use; more comparative work is needed to understand the role of policy in the severity of problematic use.
We also investigated demographic differences in CRNCs. Overall, males appear to be at a greater risk of experiencing CRNCs relative to females which aligns with findings that clinical populations in treatment for substance use disorder are disproportionately male. 131 Males, particularly adolescent or young adult males, should be considered a priority population for cannabis misuse interventions aimed at reducing CRNCs. Far more research focusing on sexual and gender minority populations is needed as the evidence to date suggests that correlates and experiences of SRNCs among sexual and gender minority youth and young adults have not been adequately studied. Similarly, there is a dearth of literature examining racial/ethnic differences in CRNCs. The samples for many studies included in this review were majority non-Hispanic White and female therefore more attention should be given to identifying risk and protective factors for CRNCs in racially and ethnically diverse samples.
Limitations of the literature
First, most of the research identified in this review relied solely on self-reported survey-based responses. No studies reported collecting corroborating evidence such as peer or family reports of CRNCs experienced by the user. Additionally, the majority of included studies (75.9%) were cross-sectional limiting our results to describing associations with little confidence that identified risk and protective factors could be described as casual mechanisms of CRNCs. Second, a burgeoning literature examining correlates of simultaneous and concurrent substance use, with an emphasis on consequences of combinations of alcohol and cannabis, was not captured here. A review of polysubstance use research is needed to compare to extant work examining the consequences of alcohol, cannabis, and other drugs independently.
Third, most studies identified and included in this review were comprised of relatively young samples—primarily adolescents and young adults, and most research with young adults sampled college students who may not represent the broader population of young adults. Future research would benefit from examining differences in CRNCs across the lifespan. As evidenced by Schepis et al 132 the prevalence, typology, motives, and risk factors of prescription drug misuse can vary considerably across age groups. Given that most individuals mature out of risky alcohol and substance use in early adulthood,133,134 users who continue to practice unsafe substance use into middle or late adulthood are likely at increased risk for cannabis use disorder but remain an understudied group.
Limitations of this review and conclusions
This review is not without limitations. First, we did not search for specific substance use consequences—such as driving under the influence—and cannot draw conclusions regarding independent consequences of use as a result. Second, we may not have captured the entirety of literature due to the search terms used, repositories searched, and publication bias leading to an underreporting of null findings. Moreover, we limited our search to self-report studies of CRNCs—akin to previous reviews on alcohol-related negative consequences. Therefore, the scope of other methodological approaches, such as qualitative research, that might provide insights into lived experiences of individuals experiencing cannabis misuse was not described. Third, the time frame for cannabis use and associated consequences varied across studies (eg, past week, past month, past year) and caution should be exercised when considering the nature of the associations between various risk and protective factors with patterns of CRNCs. Lastly, the utilized electronic databases utilized in this review may not have captured earlier research not indexed online.
Notwithstanding the limitations of the existing literature and present review, the findings highlight the need for multilevel strategies public health interventions that can reduce the risk of negative cannabis use consequences to attenuate the cumulative risk of psychological, social, and contextual influences. Importantly, future research should aim to identify relevant protective factors for CRNCs and prioritize the investigation of environmental, interpersonal, and policy factors associated with problematic cannabis use, especially in racially and ethnically diverse populations. Addressing the current gaps in this literature will bolster the effectiveness of future primary and secondary multi-level prevention programs.
Supplemental Material
sj-docx-1-sat-10.1177_11782218231166622 – Supplemental material for A Scoping Review of Risk and Protective Factors for Negative Cannabis Use Consequences
Supplemental material, sj-docx-1-sat-10.1177_11782218231166622 for A Scoping Review of Risk and Protective Factors for Negative Cannabis Use Consequences by Timothy J. Grigsby, Andrea Lopez, Larisa Albers, Christopher J. Rogers and Myriam Forster in Substance Abuse: Research and Treatment
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The publication fees for this article were supported by the UNLV University Libraries Open Article Fund.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Conceptualization: TG and MF. Literature search: TG, AL, and LA. Data extraction: AL and LA. Data synthesis and Writing – Original Draft: TG. Writing – Review and editing: All authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.