
Abstract
Objectives:
With one of the highest prevalence rates for marijuana use in the United States, Colorado provides a great opportunity for insight on common encounters with consumers in the community pharmacy setting. Currently, there is limited data on community pharmacists and their experiences with patients and marijuana. This study aims to identify the most common questions community pharmacists receive about marijuana, how comfortable they are in answering those questions, and to identify knowledge gaps regarding marijuana and pharmaceutical care.
Methods:
A cross-sectional study design was chosen to survey community pharmacists. A convenience sample of community pharmacists from the greater Denver metro area counties were surveyed about recreational and medical marijuana questions they receive from patients and consumers. Statistical methods included descriptive statistics, Chi-square, Kruskal–Wallis, and Mann–Whitney.
Results:
Of the 51 pharmacists who completed the survey, 20% received questions about medical marijuana daily or weekly, 57% monthly, and 22% never, while 16% received questions about recreational marijuana weekly, 41% monthly, and 43% never. In addition, 53% were comfortable answering questions about medical marijuana, while 41% were comfortable answering questions about recreational marijuana. The most common questions received were related to indications, uses, and efficacy (33%), followed by drug interactions (30%).
Conclusion:
The increased acceptance of marijuana by patients warrants pharmacists and other healthcare providers to be confident and familiar with its use. Our findings suggest that the majority of pharmacists are not asking about marijuana use/consumption, and this may be a gap in care. Studies support that other healthcare providers also exhibit hesitancy in initiating these conversations. Consumers are using marijuana products now, so increasing marijuana education for all healthcare professionals during both didactic education and continuing education will be key to ensuring patients have access to evidence-based care regarding the use of marijuana, rather than care based on belief, alone.
Keywords
Introduction
As of 1 January 2019, more than half of the United States have legalized Cannabis sativa for medical or recreational use. Other terms regarding Cannabis may include Cannabis indica or even Cannabis ruderalis; however, based on anatomical, genetic, morphological, and phytochemical studies, these are considered to be varieties of the polymorphic strain Cannabis sativa L., rather than truly separate strains.1,2 For the purpose of this article, the colloquial term, “marijuana” will be used.
Currently, there are 33 states plus Washington, D.C., legalizing marijuana for medical purposes, and 11 states plus Washington, D.C., approving marijuana for recreational use. 3 In 2012, Colorado became the first state in the United States, along with Washington, to legalize recreational marijuana. 3 As more than 1 in 4 adults aged 18 and older used marijuana in 2017, Colorado has the third highest prevalence rate of marijuana use in the United States and provides a great opportunity for insight on common encounters with consumers in the community pharmacy setting. 4 Community pharmacists currently practicing in Colorado have received little to no formal education on how to counsel patients utilizing marijuana. 5 Pharmacy care deficiencies include the lack of information available on clinically significant marijuana interactions, and the lack of human data on topical and transdermal formulations of cannabis. There is growing literature providing information based on clinical trials of pharmaceuticals, Epidiolex® (cannabidiol, approved in June 2018 in the United States as an orphan drug for treatment of seizures associated with Lennox-Gastaut syndrome or Dravet syndrome in patients 2 years and older), Sativex® (cannabidiol plus tetrahydrocannabinol used for pain and spasticity associated with multiple sclerosis, not approved for use in the United States) and dronabinol (synthetic oral preparation of delta-9-tetrahydrocannabinol, approved in May 1985 in the United States for treatment of chemotherapy induced nausea and vomiting and anorexia in patients with acquired-immunodeficiency syndrome (AIDS)).6–8 Unfortunately, the drug information regarding these products is not applicable to the marijuana products available from local marijuana/cannabis dispensaries. Products sold in Colorado marijuana dispensaries come in many formulations and strengths, and may be administered via inhalation, an edible, oral liquid, topical patch, topical cream, transdermal cream and so on; the list is exhaustive. Evidenced-based tertiary literature resources, such as Lexicomp, Micromedex (Martindale’s) and Clinical Pharmacology, provide pharmacodynamic and pharmacokinetic parameters based on primary literature from the clinical trials of these specific pharmaceutical formulations (Epidiolex®, Sativex® and dronabinol). These parameters should not be extrapolated to be equitable or similar in regard to non-regulated marijuana products. Pharmacies often have internet restrictions in place that prohibit pharmacists from accessing resources available outside of approved sources. This may lead to some discomfort in counseling when the only available resources are those specific to FDA approved medications. Another barrier presented to pharmacists is the lack of direct communication with prescribers. Electronic health records are not accessible to pharmacists and thus they are unable to document on patient charts or to review patient history. In an ideal setting, community pharmacists would have access so prescriber and pharmacist communication would not be delayed, and information gained in the community could be easily shared with the prescriber, and pharmacists would have a better understanding of patient history to support appropriate medication counseling.
Cytochrome (CYP) P450 enzymes, including CYP2A6, 2B6, 2C9, 2D6, 3A4 and 1A2, are involved in the metabolism of cannabinoids.9–15 Table 1 provides an overview of known CYP activity with selected cannabinoids. CYP2C9, CYP2D6 and CYP3A4 are responsible for the metabolism of or targets of inhibition and induction for numerous medications.10–16 To add to the complexity of the matter, individual cannabinoids differ in affinity for CYP enzymes. In other words, different forms of marijuana (oral tinctures, topical creams, edibles, transdermal patches, different strains of cannabis such as Cannabis sativa versus Cannabis indica) contain different cannabinoids at varying concentrations, all in which can impact the clinical significance of the interactions with CYP enzymes. In-vivo data on CYP interactions is limited to oral formulations. 15 To put it into perspective, the top 20 drugs in the United States are listed in Table 2. 16 The CYP activity of these commonly used drugs is listed in comparison to CYP activity with cannabinoids. In addition, food-drug interactions are also possible. Grapefruit is a food with well-known CYP3A4 inhibition, so consuming this food and marijuana may lead to increased exposure to cannabinoids and their mechanism of action. 17 As there is a possibility for both drug and food interaction, patients should be monitored and the interactions documented, as the majority of interactions known with marijuana products are from clinical trials with very specific disease states (epilepsy, multiple sclerosis, and cancer) that are not reflective of the general patient population. Asking patients if they are using marijuana products is necessary because these interactions will not be caught without the awareness of marijuana use.

CYP: Cytochrome; THC: Tetrahydrocannabinol; W: Weak inhibition; X: Inhibition.

CYP: Cytochrome; CBN: Cannabinol; CBD: Cannabidiol; THC: Tetrahydrocannabinol.
↑↑ = inhibition, may increase drug exposure;
↑ = weak inhibition, may slightly increase drug exposure.
Marijuana products sold in dispensaries may also have additional cannabinoids not yet discovered or understood, which adds to the complication of drug-drug interactions and drug-disease interaction/considerations. It is important to recognize the possibility of drug interactions that have yet to be identified, which warrants counseling and careful monitoring in patients considering marijuana use, regardless if they are on other drugs, or supplements.
In addition to the variation in “active” compounds (cannabinoids), there is also concern for mislabeling and contamination. Marijuana products are not regulated in a manner to ensure safety or efficacy. The FDA has tested CBD products and has found many of them do not contain the amount that they state on their product labeling. 18 Contamination is another concern with these unregulated products. Researchers have determined three different ways in which there is concern for heavy metal accumulation within the cannabis plant: bio accumulative capacity, (ability to remove heavy metals from the soils and deposit these metals in the cannabis plant), cross-contamination during processing, and post processing adulteration, in which metals are added to increase weight and thus value of the product. 19 Additional contaminants found include microbial contamination and pesticides. 19
As medication experts, pharmacists need to be prepared to answer questions on safety, efficacy and interactions of marijuana. In a study evaluating pharmacy students and their education and experience regarding marijuana, students reported they “did not feel comfortable answering consumer questions regarding efficacy, safety, or potential drug interactions with medical marijuana.” 20 A more recent study showed that California pharmacists who are educated on medical marijuana are more likely to be comfortable with counseling. 5 Pharmacists are not the only healthcare professionals feeling a deficiency in training regarding marijuana and its constituents. A study evaluating primary care providers reported that half of the providers did not want to address patient questions regarding medical cannabis. 21 The majority of providers wanted to learn more about marijuana for their training. 21 These results support the importance of marijuana education, and our study aimed to determine specifically what pharmacists in the community pharmacy are being asked regarding marijuana to support the need for additional education and training in the future. Importantly, this training should be for all healthcare professionals, not just pharmacists. Pharmacist-received questions provide examples of what patients are asking once they have left the prescriber’s office.
There is a paucity of published literature describing the type of questions asked by patients about marijuana, and pharmacist levels of comfort answering such questions. By determining the most common questions received in the community regarding marijuana, health professional education can be developed in accordance to what is being asked and deficiencies in education can be addressed. A recent survey of pharmacy students at Ohio State indicated that more education is needed regarding medical marijuana, and that pharmacists should be able to counsel patients on medical marijuana. 22 The same authors surveyed pharmacy school educators of which 64% (51/76) colleges indicated that they teach medical marijuana in a required course. In a survey of Connecticut pharmacists, only 29.3% (98/334) who responded thought that they were knowledgeable enough about the side effects of medical cannabis to provide appropriate counseling to patients. 23 Another survey of patients showed that 44% (35/79) were taking other medications while taking medical marijuana and 38% (30/79) reported receiving no information on dosage or frequency of use. 24
As social stigma remains regarding marijuana as an illicit drug, patients and providers may not be comfortable discussing marijuana. One aspect of the survey examines pharmacist levels of comfort in asking patients about marijuana use. This study aims to identify the Colorado community pharmacists’ comfort level answering questions about marijuana, how often pharmacists ask about marijuana use while counseling patients, and the most common questions received.
Methods
An 11-question survey was developed to assess community pharmacist engagement with patients and customers about recreational and medical marijuana. The survey is not a validated tool but was pilot-tested by a small subset of community pharmacists prior to the study taking place. In addition to demographics, questions included the frequency and type of questions patients and customers ask about marijuana, pharmacist comfort with answering these questions, whether the pharmacist asks about marijuana use during counseling, and resources used to find answers to questions about marijuana (see Figure 1). Surveys were considered complete if all questions were answered.

Frequency of questions regarding marijuana.
Following approval by the institutional review board, a convenience sample of at least seven community pharmacies in each of the counties comprising the greater Denver metropolitan area was chosen. Pharmacists were eligible to participate if they worked at a community pharmacy in one of the following counties: Adams, Arapahoe, Boulder, Denver, Douglas, Jefferson and Larimer. Participation in the survey was voluntary. Surveys were hand delivered during summer of 2018 and picked up after 3 days or completed the day of delivery depending upon whether the pharmacist had time to answer the survey. Hand-delivery of surveys provides a high response rate and was chosen as the delivery method over an Internet-based survey. 25 In addition, some pharmacies have Internet restrictions that prohibit access to take an online survey. To preserve confidentiality, each survey was given a unique identifier known only to the researchers.
Statistical methods include descriptive statistics for all study variables, Chi-square for binomial comparisons, Kruskal–Wallis for multi-group comparisons and Mann–Whitney for between-group differences. The questionnaire was coded, checked for accuracy and statistics analyzed using the Statistical Package for Social Sciences (SPSS). Participating pharmacists had the option to receive a copy of the results after completion of the study.
This study was approved by the Regis University Institutional Review Board, ID #1238975-1.
Results
A total of 51 pharmacists completed the survey of which 88% worked at a national chain pharmacy. Most of the pharmacists were managers (45%), staff (29%), or floaters (24%), and were practicing for 6 years or longer (59%). Of the 51 pharmacists who completed the survey, 20% received questions about medical marijuana daily or weekly, 57% monthly, and 22% never, while 16% received questions about recreational marijuana weekly, 41% monthly, and 43% never. Figure 1 provides a depiction of the frequency of marijuana questions received. In addition, 53% were comfortable answering questions about medical marijuana, while 41% were comfortable answering questions about recreational marijuana. Figure 2 provides a depiction of pharmacist perceived comfort, and Figure 3 provides a list of all marijuana questions asked of community pharmacists in this study.

Pharmacist response regarding perceived comfort in answering questions about marijuana.
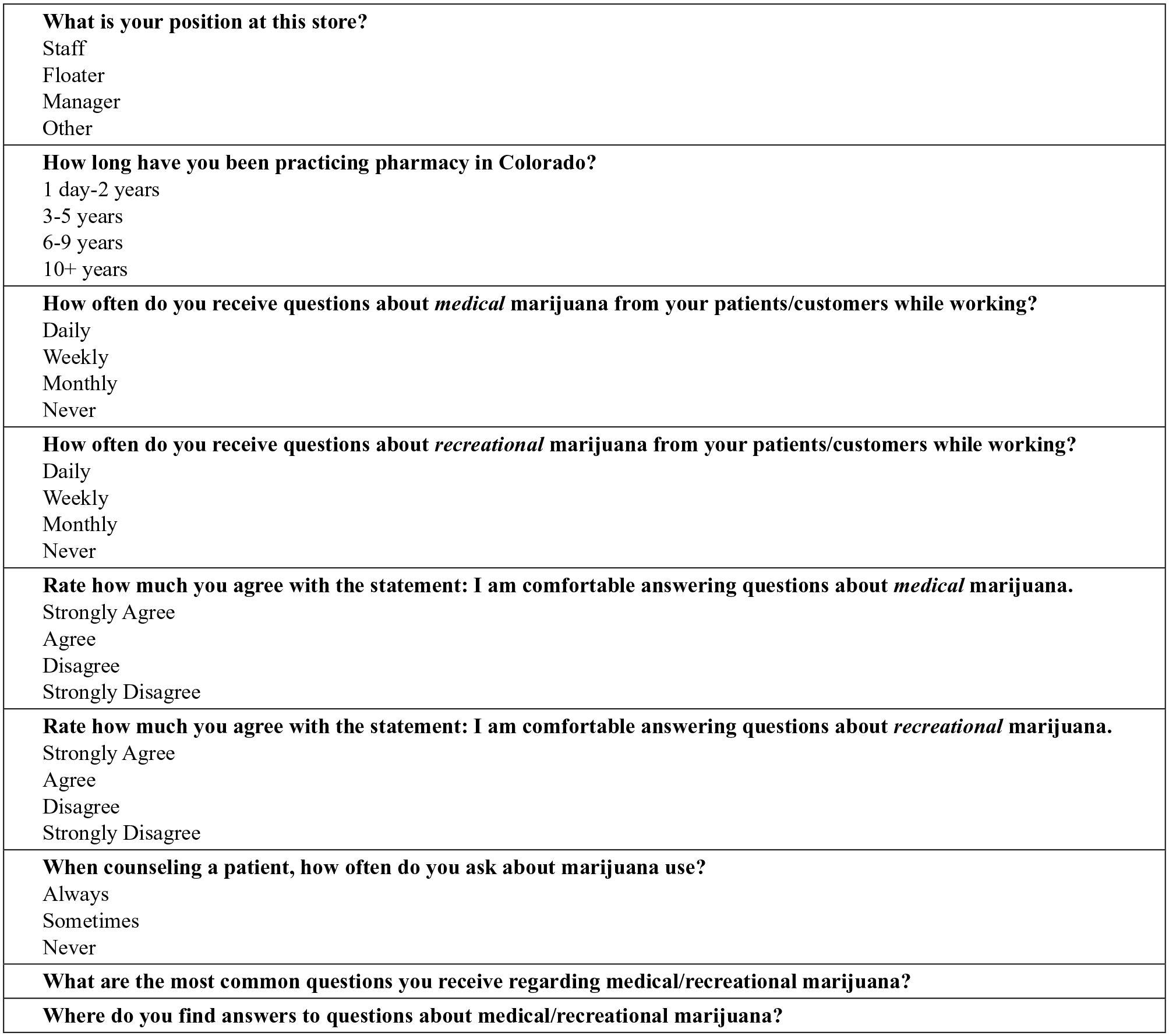
Survey questions.
One of the survey questions asked when counseling a patient how often the pharmacist asked about marijuana use. The majority (59%) responded that they never asked about marijuana use.
When comparing pharmacists with 6 or more years of experience (n = 30) to those with less than 6 years of experience (n = 21), 60% and 43% of pharmacists were comfortable answering questions about medical marijuana, and 43% and 34% were comfortable answering questions about recreational marijuana, respectively.
Compared to pharmacists who do not ask about marijuana use during counseling, pharmacists who ask are more comfortable answering questions about medical (p = 0.023) and recreational (p = 0.012) marijuana and receive more questions about medical (p = 0.008) and recreational (p = 0.001) marijuana. In addition, compared to pharmacists practicing for less than 6 years, those practicing for 6 years or longer are more likely to receive questions about medical marijuana (p = 0.003).
The most common questions received were related to indications, uses, and efficacy (33%), followed by drug interactions (30%), where to purchase (19%), and how long marijuana is detected in the body (12%). To answer questions about marijuana, surveyed pharmacists used clinical resources such as tertiary drug databases (Lexicomp, Micromedex, Facts and Comparisons, etc.), primary literature (38%), the Internet (30%) and personal knowledge or peers (16%). Tertiary drug databases and primary literature were combined in this analysis. Some pharmacists are able to access primary literature from resources such as PubMed, whereas some pharmacies have Internet restrictions and only have access to approved tertiary databases that provide select primary literature respective to approved pharmaceuticals. Roughly, 16% did not know where to research a question about marijuana. A common dilemma in some community pharmacy settings is a restriction on Internet access, whereas only approved tertiary references are available for pharmacists to access.
Discussion
There is variability in comfort regarding marijuana counseling and education. Pharmacies often have internet restrictions in place that prohibit access to numerous clinical resources outside of what has been approved for the pharmacy. This may lead to some discomfort in counseling when the only available resources are those specific to FDA approved medications. If an individual is interested in using a marijuana edible for a sleep-aid, data from Epidiolex® or Sativex® pharmacokinetics will not be applicable. Currently, known side effects/precautions are based on clinical data from pharmaceutical products such as Epidiolex and Sativex, which vary significantly from the formulations available in medical marijuana dispensaries (or recreational marijuana dispensaries). For example, Epidiolex is an oral solution containing only one cannabinoid, cannabidiol. The cannabidiol is provided in a 100 mg/mL solution that comes with two 5 mL measured oral syringes. Dosing is determined based on the weight of the patient, and alanine aminotransferase (ALT), aspartate aminotransferase (AST) and total bilirubin levels are required to be drawn prior to the administration of this drug due to the risk of hepatocellular injury. 7 Cannabidiol formulations in dispensaries may or may not include other cannabinoids. Oral solutions in marijuana dispensaries come with varying administration devices, including “droppers” which lack consistency in dosing. Sativex is a combination product of dronabinol and cannabidiol in doses of 2.5 mg ad 2.7 mg per 100 microliter buccal spray, respectively. 8 The consistency of the doses provided in Epidiolex and Sativex enable providers to determine appropriate dosing and response, whereas the dosing variability in dispensary products leaves a large area of gray in determining patient response and appropriate dosing.
It is evident that the longer the pharmacist had been in practice, the more likely they would be comfortable counseling, or at least, discussing marijuana with their patients. This highlights that without a patient sharing that they are using marijuana, it may not come up in conversation with a pharmacist. It is common practice for many pharmacists to ask if a patient uses tobacco. Is adding marijuana use to that common question the next step for holistic care? In the study surveying primary care providers, 38.7% of the providers reported a belief that marijuana interacted significantly with medical therapies. 21 This report provides insight that providers are aware of the possibilities of interactions, but the medical and pharmacy community will need to work together to document suspected interactions and/or side effects that may be occurring with the use of the non-regulated marijuana products. Determining interactions will be crucial when patients are using non-FDA products for indications outside of those studied in clinical trials. Considerations to ensuring that a marijuana discussion occurs for the majority of patients may be to include a marijuana section on all intake forms. Currently, intake forms may have a section for stating the use of marijuana, but it is following the question pertaining to the use of “illegal substances.” This provides stigma and may create a barrier to patients honestly documenting their use of marijuana.
Physicians, pharmacists, physician-assistants, nurses, and all allied-health clinicians must consider the marijuana discussion with patients. There may be a conflict between evidenced-based medicine and the use of marijuana in some patients, but the importance of documentation and counseling remains. Regardless of one’s personal views on the use of marijuana, marijuana products are widely available, and consumers are using them. Counseling and confidence in initiating the discussion is necessary to ensure patient safety.
As the majority of Colorado community pharmacists surveyed do not feel comfortable answering questions about recreational marijuana, and slightly more than half feel comfortable answering questions about medical marijuana, an emphasis should be placed on continuing education (CE) for marijuana. This is an unprecedented setting because pharmacists are trained to provide evidenced-based care, and marijuana products available to the public are lacking in clinical research and the safety and efficacy data that support evidenced-based care. It makes complete sense why pharmacists may be wary to take part in providing counseling for marijuana. This creates a community pharmacy setting that acts as one of many pseudo-clinical trials of unregulated products. Regardless that the use of marijuana for the general patient population is unprecedented, it is time to modify the standard of care so that pharmacists can, at least, be accessible healthcare team members that will promote the safest use of these products as possible. Pharmacists that are placed in the role of dispensing marijuana in the states of Connecticut, Minnesota, and New York may be excellent resources in learning how best to care for patients, evaluate and monitor those utilizing these marijuana products that have not been studied in clinical trials. Although the trial by error is not ideal, it is reassuring to know that medical professionals are a requirement in the dispensing of these unknown products. It is likely there will be a lot to learn from these pharmacists in the years to come. The Connecticut Pharmacists Association offers a “Medical Marijuana Academy” for pharmacists, and the state of New York requires that pharmacists complete a state-approved course before they are allowed to counsel on medical marijuana.26–28 New York has two approved courses.27,28 These education opportunities require registration, but they may provide pharmacists with additional concepts to navigate caring for patients considering marijuana outside the context of pharmaceutical, clinical-trial drugs. In addition, New York has a marijuana adverse event reporting system. 29 This adverse event reporting system is a valuable tool for practitioners to update what the medical community knows of patient adverse events related to marijuana. Hopefully, the New York pharmacy community in roles of dispensing will add to medical literature, as they will be able to report adverse events, in the context of knowing more about the patient’s condition, what they are using the product for, as well as what other medications the patient may be on. This will be valuable information.
Based on the results of our study, pharmacist education should emphasize the importance of asking about marijuana use with all patients, what efficacy information is available, and what interactions are possible. These findings are applicable to all healthcare providers, as there are many gaps of knowledge to fill in determining safe practice in the utilization of these new and unregulated products.
Recognizing resources available to stay up-to-date in the changing climate of marijuana accessibility is an important step in staying informed. The National Conference of State Legislatures (NCSL) website provides valuable information regarding state versus federal laws. 3 According to federal law, marijuana remains classified as a schedule 1 substance. Federal law prohibits prescriptions for class 1 substances, so a prescriber cannot truly write a prescription for marijuana. In December 2018, the Farm Bill was signed into law. 25 The Farm Bill removed hemp and its constituents from the definition of marijuana in the Controlled Substance Act. 25 Cannabis sativa L. with no more than 0.3% tetrahydrocannabinol (THC) is no longer defined as marijuana, however that does not enable it to be used as a dietary supplement. 30 Subsequent to this bill, CBD products are now available in grocery stores, spas, coffee shops, and so on, regardless that it is still considered illegal on a federal level.
In Colorado and other states that have approved marijuana for medical purposes, the terms used in statutory language (propositions, amendments, measures, etc.) varies from prescriber “certifications” to “recommendations”; the recommendations/certifications given to a patient are not truly “prescriptions” since marijuana remains a schedule 1. With regard to the marijuana products, there is no difference in the state of Colorado between “medical marijuana” and “recreational marijuana.” Therefore, counseling and education points may be similar, regardless if the patient is using marijuana medically or recreationally. The difference between medical marijuana and recreational marijuana in the state of Colorado is the amount of marijuana purchased at one time, the cost, and the legal consequences if found in possession. However, it is important to recognize that there may be differences in marijuana “medical products” versus “recreational products” in other states. This article focuses on the marijuana experience where marijuana is determined state-legalized for both medical and recreational purposes. The states of Connecticut, Minnesota, and New York have language requiring pharmacists to be involved in the dispensing of marijuana, and this changes the experience significantly.
Variability exists in possible interactions based on the cannabinoids present in the marijuana product being utilized, the concentration of each cannabinoid, and the dosage form. Individuals may use predominately CBD products due to their lack of psychotropic activity, but the possibility of drug interactions is not benign for CBD products, and should be evaluated carefully. As a reminder, Table 1 provides examples of CYP activity based on cannabinoids most heavily studied and understood in marijuana. Please note there are many other compounds found in marijuana. This table is designed to act as a reminder of the importance of having ongoing discussions with patients about marijuana use. Asking patients if they are using marijuana, either for medical or recreational reasons, is important in order to ensure patient safety, and to enable documentation of adverse reactions, side effects, and drug interactions that may be occurring or impacted as a result of the marijuana product.
Limitations
A one-time cross-sectional study was conducted in which a convenience sample of community pharmacies was chosen. The sample may not represent the population of all Colorado community pharmacists. A convenient sample of community pharmacists in the greater Denver area was used, which potentially limits generalizability of results to community pharmacists working outside of the greater Denver area. Surveys were hand-delivered because many pharmacists have limited access to the internet during working hours. As we were able to hand-deliver surveys, we only accounted for those surveys that were completed and did not account for those surveys that were not completed. A limitation to this study was that sample-size was not calculated. In addition, there were inconsistencies among several of the surveys completed. For example, several pharmacists circled two answers when answering how often they received questions about marijuana, while others circled “never” but wrote out a question they received. One pharmacist stated that over her 10-year pharmacy career, she had received 1 question about marijuana, but still circled she had never received a question. Finally, numerous responses for additional comments were vague. For example, when asked what resources were used to search for questions about marijuana, several answers included, “Internet,” “web,” and “online websites.” Answers such as these were categorized as using the “Internet” as opposed to “clinical resources,” though one cannot definitively say that is the case.
Conclusion
The most common type of questions that community pharmacists received about marijuana were related to indications, efficacy, and interactions. This demonstrates that consumers are more curious about what marijuana can be used for, and how it interacts with their medications. Our findings suggest that the majority of pharmacists are not asking about marijuana use/consumption, and this may be a gap in care. Studies support that other healthcare providers also exhibit hesitancy in initiating these conversations. Consumers are using marijuana products now, so increasing marijuana education for all healthcare professionals during both didactic education and CE will be key to ensuring patients have access to evidence-based care regarding the use of marijuana, rather than care based on belief, alone.
Footnotes
Author’s note
Some of these findings were previously presented in 2018 at poster sessions at the ACCP annual meeting and ASHP Midyear Meetings.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Regis University INSTITUTIONAL REVIEW BOARD, Denver, CO, Approval Number: 1238975-1.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.