
Abstract
OBJECTIVE:
Few studies have examined cannabis motives in adults and, although associations between cannabis use and psychiatric conditions are well documented, there has been limited investigation of the intersection of cannabis use, cannabis motives, and psychopathology. In a sample of community adults, the present study examined cannabis motives in relation to cannabis misuse, and investigated whether motives linked cannabis misuse with concurrent psychiatric symptoms.
METHOD:
Participants (N = 395; Mage = 34.8; %F = 47.6; % White = 81.3%) completed assessments related to cannabis misuse, cannabis use motives, and symptoms of depression, anxiety, PTSD, and somatic experiences. Bivariate correlations, hierarchical regressions, and indirect effect analyses were performed to examine associations between motives and cannabis misuse and to investigate mechanistic relationships between psychiatric symptoms and cannabis misuse.
RESULTS:
Regressions revealed significant associations between cannabis misuse and social (β = .13, P < .02), enhancement (β = .12, P < .02), and coping motives (β = .48, P < .001). Indirect effects were present such that coping motives consistently linked psychiatric and somatic symptoms with cannabis misuse (anxiety: unstandardized effect = 0.26,and 95% CI = 0.17-0.37; depression: unstandardized effect = 0.12, CI = 0.11-0.25; PTSD: unstandardized effect = 0.07, CI = 0.04-0.10; somatic symptoms: unstandardized effect = 0.20, CI = 0.11-0.30). In addition, enhancement motives exhibited an indirect effect (unstandardized effect = 0.02, CI = 0.002-0.04) between depressive symptoms and cannabis misuse.
CONCLUSION:
These results support a negative reinforcement motivational profile as the predominant pattern in adult cannabis users, albeit with links to enhancement and social motives. This motivational profile is especially pronounced with regard to comorbid psychopathology and cannabis misuse. These results support the importance of treatment strategies targeting maladaptive coping to address cannabis misuse and co-occurring psychopathology.
Introduction
Cannabis is the third most commonly used controlled substance worldwide, with estimates that around 3.9% of the global adult population has used it in the previous year. 1 Rates of use are higher in developed nations; for example, in Canada, over half of individuals aged 15 and over have reported trying cannabis at least once in their lifetime. 2 Importantly, the 12-month prevalence of cannabis use among adults and the perception of no risk from cannabis use has significantly increased over the last fifteen years. 3 While many use cannabis without problems, 1 in 5 are estimated to develop cannabis use disorder (CUD) and, among those that use weekly or more, this risk increases to one in three. 4
Beyond CUD, cannabis use has been repeatedly linked to psychiatric disorders such as depression, anxiety, and posttraumatic stress disorder (PTSD).5-9 Two national epidemiological studies conducted in the US found strong associations between CUD and mood disorders, anxiety disorders, and PTSD.7,9 Further, the strength of these associations increased as CUD severity increased. 7 Other research has implicated cannabis use as both a predictor and exacerbator of these psychiatric disorders.10,11 One epidemiological review on cannabis use, depression, and anxiety found that cannabis use increased risk of later depression (especially in females, those that started using earlier, and those that use more heavily), and that cannabis was used as a coping mechanism for depressive symptoms. 10 Other research has found that chronic use strengthened the association between cannabis use and depression. 12 Associations between cannabis use and anxiety have also been reported, where evidence suggested cannabis use both initiated and exacerbated pre-existing anxiety. 10 A nationally representative study conducted in the US found that lifetime and current PTSD diagnoses were associated with greater odds of lifetime and past year daily cannabis use, even after accounting for relevant demographic variables. 5 Another study found that lifetime PTSD was significantly associated with CUD. 8 Because cannabis use is popular and has a robust relationship with psychiatric disorders, understanding the mechanisms that underlie this relationship is important.
In a contemporary biopsychosocial model of substance use, 13 drug use motives are important psychological determinants for the development and maintenance of use. In the case of cannabis, Simons et al and colleagues 14 developed a scale to measure motives for cannabis use, finding evidence for 5 motives, later replicated by other research groups.15,16 These include motives to use cannabis for Enhancement (i.e., to enjoy its psychoactive effects), Coping (i.e., to experience relief from distress, such as to alleviate symptoms of anxiety, depression, or pain), Social (i.e., to enhance a social experience), Conformity (i.e., to fit in with others who are using cannabis) and Expansion (i.e., to experience heightened perceptions or mental sensibility).
Cannabis motives, particularly, coping motives, have been demonstrated to predict cannabis use even after accounting for relevant variables such as sex, age at first use, tobacco use, and alcohol use.15,17,18 Other studies have implicated motives as unique predictors of cannabis problems and impairment. 19 While these individual studies use a variety of criterion variables (eg, cannabis use frequency, cannabis use problems, CUD symptoms, cannabis use related impairment), common to all is the implication of coping motives as a significant predictor of negative outcomes. The importance of coping motives is consistent with the negative reinforcement model of substance use, which proposes that those with substance use disorders often use substances to alleviate feelings of mental distress (eg, depression, anxiety) or physical discomfort (eg, pain), which effectively strengthens drug-taking behavior. 20 Supporting these individual findings is a recent meta-analysis which found that, compared to other motives, coping motives were most robustly associated with cannabis related negative outcomes such as use frequency, problems, and CUD symptoms. 21 This meta-analysis also highlighted an important limitation to this area of research, namely, the paucity of studies that include a broad sample of community adults. Nearly half of the included samples used university student or young adult samples. The other half used community samples, but generally young adults in the early- to mid-twenties. Only 2 studies reported an average age of 30 or older22,23 and both recruited from specialized locations.
Beyond indicators of cannabis involvement, some studies have implicated coping as a particularly important motive related to the relationship between cannabis misuse and various psychiatric disorders. For example, studies that investigated the relationship between cannabis misuse, motives, and psychiatric disorders such as social anxiety, obsessive compulsive disorder (OCD), and PTSD found that coping motives mediated the relationship between cannabis misuse and these various disorders.24-26 To date, this literature is limited to 3 studies. Further, these studies have focused on specialized samples such as adolescent and young adult samples, 26 and veterans. 25 One study used a community adult sample and found that coping and conformity motives partially mediated the relationship between social anxiety and cannabis-related problems in men, but not women. 24 However, this study was limited to exploring relationships between cannabis misuse in social anxiety, specifically. Additionally, participants were individuals that responded to advertisements to participate in a tobacco cessation program and thus may not by generalizable to a wider community adult population.
In summary, there is limited research on cannabis motives in relation to cannabis misuse in general community adults and necessarily limited research on links between motives and symptoms of psychiatric disorders, such as anxiety, depression, and PTSD, in that population. The present study was conducted to address these gaps by pursuing 2 primary aims: (1) to examine motivational indicators in relation to cannabis misuse in a general community adult population, and (2) to investigate whether the implicated motives clarify relationships between cannabis misuse and psychiatric symptoms. Given findings from past literature, it was hypothesized that coping motives would be associated with cannabis misuse. Finally, it was predicted that coping motives would partially account for the relationships between cannabis misuse and both psychiatric and somatic symptoms.
Method
Participants
Participants were enrollees in a research registry at the Peter Boris Centre for Addictions Research at St. Joseph’s Healthcare, Hamilton in Hamilton, Ontario. This is a cohort of community adults who participated in a one-time broad-spectrum non-invasive assessment to be a member of a research database of potential volunteers for future studies. No clinical syndromes were required to join the registry and the eligibility criteria were intentionally broad. Inclusion criteria were age 18 to 65 years old, willingness to be contacted for future studies, and use of a computer (including smartphone) more than once per week (for competency with electronic assessments). Exclusion criteria were unwillingness or inability to provide informed consent or complete study procedures, a medical condition that would preclude participation in future studies (e.g., terminal conditions), and lower than ninth grade education (for adequate literacy). The cohort comprised 1432 adults from the Hamilton, Ontario, area, but for the current study, only participants who reported cannabis use in the last month were included (N = 395; 27.5%). This study was approved by the local research ethics board (HiREB #4699).
Measures
Demographics
Participants completed a battery of demographic questions, including age, sex, education level, income, and ethnicity.
The Cannabis Use Disorder Identification Test – Revised (CUDIT-R). 27
The CUDIT-R is an 8-item measure of cannabis use problems. The measure includes 4 domains of misuse: cannabis problems (abuse), consumption, dependence, and psychological features. In our sample, the reliability was Cronbach α = .82.
Marijuana Motives Questionnaire (MMQ). 14
The MMQ is a 25-item scale, with each item rated on a 5-point Likert Scale ranging from “almost never/never” to “almost always/always.” The MMQ comprises of 5 subscales/motives: Enhancement (e.g., “to get high”); Coping (e.g., “because it helps me when I feel depressed or nervous”); Conformity (e.g., “to fit in with the group I like”); Expansion (e.g., “to expand my awareness”); and Social (e.g., “because it helps me enjoy a party”). In prior research, item 16 (“to celebrate a special occasion with friends”) failed to clearly load onto any factor,14,15 and as such, was removed in this study and a 24-item scale was employed. The reliability of the subscales in our sample were Cronbach α = .87, .90, .82, .94, and .90, respectively.
Patient Health Questionnaire (PHQ, depression, anxiety, and somatic subscales). 28
The depression subscale (PHQ-9) asks about various symptoms (e.g., “little interest or pleasure in doing things”) over the past 2 weeks on a 4-point Likert scale ranging from “not at all” to “nearly every day.” The reliability in this sample for this measure was Cronbach α = .90. The anxiety domain asks about various symptoms (e.g., “feeling nervous, anxious, on edge, or worrying about a lot of different things”) over the past 4 weeks on a 3-point Likert Scale from “not at all” to “more than half the days.” If participants answered “not at all” to the example item, no other items were administered, and their score was zero for this domain. The reliability for the anxiety domain in our sample was Cronbach α = .78. The somatic symptom domain asks about various somatic symptoms from back pain to chest pain over the past 4 weeks on a 3-point Likert Scale, from “not bothered” to “bothered a lot.” The reliability for this domain in this sample is Cronbach α = .76.
The PTSD Checklist for DSM-5 (PCL-5). 29
The PCL-5 is a measure of symptoms related to PTSD. It is a 20-item questionnaire, with 4 clusters of symptoms corresponding to DSM 5 criteria: Cluster B (intrusion symptoms); Cluster C (avoidance of stimuli); Cluster D (negative alterations in mood or cognition); and Cluster E (alterations in arousal and reactivity). Items are rated on a 4-point Likert Scale from “not at all” to “extremely.” The reliability for these clusters in our sample were Cronbach α = .90,.88, 91, and.82, respectively. A total PCL was computed by summing the cluster scores, with Cronbach α = .95.
Procedure
Eligibility was determined via telephone and web-based screening. Participants received a brief overview of participation and, for those enrolling, provided informed consent before completing an assessment session lasting approximately 3 hours. The focus of the current study is cannabis-related assessments and other pertinent mental health related measures (described above). Over the course of the assessment, participants received snacks and breaks to avoid fatigue. Participants were provided with $30 in gift cards as incentives for participation.
Data analysis
One participant was missing 2 data points from the MMQ and was thus excluded from analyses involving those subscales (Social and Expansion motives). There were no other missing data in this study. Five covariates of interest were included: age; sex; race; household income; number of years of education. Candidate covariates were examined in relation to CUDIT scores and were included if significantly associated (see Table 1). We first performed correlations between all measures of interest. Next, we examined the relationship between cannabis motives and cannabis misuse using hierarchical linear regressions. Specifically, we regressed CUDIT scores on the cannabis motives domains, incorporating relevant covariates (education, income) and evaluated collinearity based on a variance inflation factor of 2. Next, we regressed CUDIT on the psychiatric and somatic symptom scores (depression, anxiety, somatic symptoms, PCL total), incorporating relevant covariates (education and income). Finally, we performed parallel mediation analyses using the PROCESS macro 30 to investigate if motives partially accounted for the association between CUDIT scores and psychiatric and somatic symptoms. Only symptoms that were significant in the preceding hierarchical linear regressions were examined in the mediation analyses. Mediation analyses were conducted with psychiatric/somatic symptoms as the predictor, relevant cannabis motives subscales as the mediator, and CUDIT as the outcome variable. For indirect effect analyses, bootstrapping (5000 replicates) was used. Confidence intervals for indirect effects that do not contain zero imply a significant effect. All analyses were computed using IBM SPSS version 23. 31
Zero-order correlations and participant characteristics.


Abbreviations: MMQ, Marijuana Motives Questionnaire; PHQ, Patient Health Questionnaire; PCL-5, PTSD Checklist for DSM-5; CUDIT, Cannabis Use Disorder Identification Test.
Legend:
Percent Female. bMedian income. cPercent self identified as White or Caucasian. Bolded values are significant at P < .05 or less. Values on legend refer to Pearson R correlations, with strong negative correlations shaded dark blue, weak relationships not shaded, and strong positive correlations shaded dark red.
Results
Descriptive statistics and zero order correlations
See Table 1 for descriptive statistics and zero-order correlations. CUDIT was significantly and positively correlated with all the measures of psychiatric and somatic symptoms, with effects in the small to medium range (rs = 0.19−0.36, ps < 0.001). Additionally, CUDIT was significantly correlated to all cannabis motives, with effects generally in the medium range (rs = 0.12 − .63, P < .001).
Cannabis use motives and cannabis misuse severity
See Table 2 for regression results. In the first regression analysis, CUDIT scores were regressed onto motives to investigate whether motives remained associated with cannabis misuse. After incorporating the relevant covariates (income and education), cannabis motives collectively accounted for an additional 35% of the variance in CUDIT scores. Three motives (Coping, Enhancement, and Social motives), remained significantly related to cannabis misuse. Additionally, Coping motives was most robustly associated to CUDIT with an effect more than double the other significant cannabis motives (β = .48 compared to 0.13-0.15).
Hierarchical linear regression of cannabis misuse on cannabis use motives.
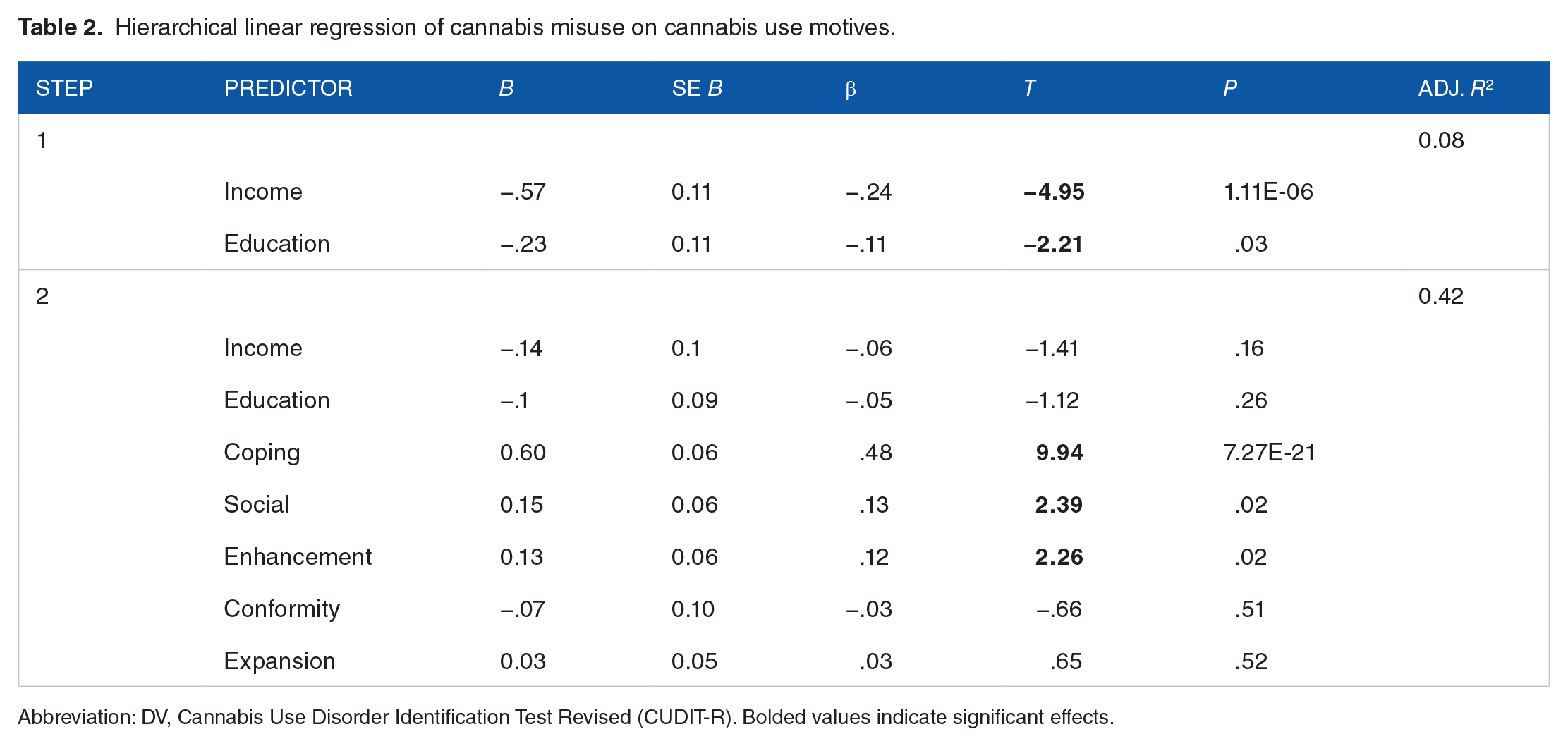
Abbreviation: DV, Cannabis Use Disorder Identification Test Revised (CUDIT-R). Bolded values indicate significant effects.
Comorbid symptoms and cannabis misuse
See Table 3 for regression results. In this step of analysis, 4 additional regressions were conducted to investigate whether the psychiatric symptom scores would remain associated with CUDIT scores. After incorporating the relevant covariates (income and education), all symptoms remained significantly associated to CUDIT scores (βs = .13−.30).
Hierarchical linear regressions of concurrent symptoms on cannabis misuse.

Abbreviation: PTSD, posttraumatic stress disorder. Bolded values indicate significant effects.
Given the significant associations between coping, social, and enhancement motives and CUDIT, we conducted 4 parallel mediation analyses to examine whether the relationships between psychiatric/somatic symptoms and CUDIT were associated through these motives (Table 4). The 2 mediation analyses for anxiety and somatic symptoms displayed the same pattern of results: a non-significant direct effect, and a significant indirect effect for coping motives but not social or enhancement motives. This pattern reflects that that the indirect pathway through coping motives was significant, the relationships between anxiety and somatic symptoms and CUDIT were rendered non-significant after accounting for coping motives, but the pathways through social and enhancement motives were not.
Indirect effect analyses of motives as a mediator of the relationship between CUDIT and somatic and psychiatric symptoms.

Bolded indirect effects are associated with LLCI and ULCIs that do not cross zero, and are thus considered significant.
In the mediation analyses with PTSD and depression, there were significant direct and indirect effects. For PTSD, only coping motives was a significant mediator, reflecting that coping motives accounted a significant portion of the variance associated with the relationship between PTSD and CUDIT, but that this relationship remained significant even after accounting for coping motives. For depression, both coping and enhancement motives were significant mediators, signaling that both coping and enhancement accounted for significant portions of the variance associated with the relationship between depression and CUDIT, but that this relationship remained significant even after accounting for these motives.
Discussion
The aims of this study were twofold: first, to identify cannabis motives associated with cannabis misuse in a sample of community adults, and second, to investigate whether those motives link the relationship between psychiatric/somatic symptoms and cannabis misuse. In the first aim, zero-order correlations demonstrated that all motives (coping, social, enhancement, conformity, and expansion) were significantly and positively associated with cannabis misuse. However, in consolidated models, only coping, social, and enhancement motives remained as significant unique indicators. Of these, coping motives was the strongest, with an effect size more than double that of social and enhancement motives. This implicates coping motives as a particularly strong correlate of cannabis misuse in adults.
To address the second aim, 4 parallel mediation analyses were conducted with coping, social, and enhancement motives as mediators. Analyses revealed that coping motives was a significant mediator for all tested symptoms (somatic, anxiety, PTSD, and depressive symptoms). This implication of coping motives as a significant mediator is consistent with prior research on cannabis use problems and social anxiety, PTSD, and OCD.24-26 While coping motives fully accounted for the relationship between anxiety/somatic symptoms and cannabis misuse, motives only partially accounted for the relationship between PTSD/depression and cannabis misuse. This finding suggests that other important variables may account for these relationships. One study found that depressive symptoms and cannabis use and consequences were positively and indirectly associated through both coping motives and ruminative thinking, while another study found that PTSD and depression were indirectly related to cannabis use disorder through coping motives and sleep motives.25,32
Interestingly, enhancement motives were also revealed as a significant mediator between depression and cannabis misuse, suggesting that those higher in depressive symptoms may also use cannabis to derive pleasure (items on enhancement subscale: “I like the feeling”; “it’s exciting”; “to get high”; “it gives me a pleasant feeling”; “it’s fun”). One study found a significant indirect effect of enhancement motives on depressive symptoms and cannabis use and consequences, although in the opposite direction as the results of this study. 32 Additional research is warranted to clarify the direction of the indirect effect of enhancement motives on depression and cannabis misuse.
Common across all mediations was the implication of coping motives as a significant mediator. This result can be understood within the context of a negative reinforcement model of addiction, which proposes that a substantial factor in developing substance use disorders (SUDs) is using substances to avoid negative or aversive states, such as stress, negative affect and/or withdrawal. 20 Indeed, this study found that a negative reinforcement motive (coping) was the most robust motivational indicator in relation to cannabis misuse in a community adult sample, providing clear support for the negative reinforcement model. The finding that coping motives accounted for a significant portion of the relationship between cannabis misuse and somatic, anxiety, PTSD and depressive symptoms provides even further support for this model, as it indicates that cannabis misuse is related to these symptoms through negative reinforcement motives. Additionally, results support for Koob’s hypothesis 33 that as substance use progresses into problematic substance use (ie, cannabis misuse), the relative contribution of positive reinforcement decreases and is replaced by negative reinforcement. Specifically, coping motives were the most robust motivational correlate of cannabis misuse, and positive reinforcing motives, such as enhancement, social, and expansion motives, were weakly associated or not associated at all. In younger samples, an age when cannabis use generally begins, these positive reinforcement motives for use are more predictive of cannabis use.17,34 Future research should investigate change in cannabis use motives longitudinally to characterize when and how cannabis users shift from positive to negative reinforcement motives for use.
Together, results of this study suggest that using to cope will likely serve as an important treatment target for those with a CUD and for those experiencing concurrent CUD and psychiatric disorders. Notably, CBT is among the best-supported treatments for CUD,35-38 and further, studies have shown that CBT was more effective for CUD compared to other SUDs.37,39 CBT for other SUDs have included modules that address coping with anger and negative affect, 39 and this study supports the added benefits of explicitly addressing coping with psychiatric symptoms. Additionally, findings regarding the associations between cannabis misuse and psychiatric symptoms highlights the importance of recognizing concurrent disorders. Some epidemiological research has found that almost half of those with an SUD have a co-occurring psychiatric disorder. 40 Treatment that addresses CUD in conjunction with other co-occurring disorders will likely prove more effective. Indeed, some researchers have found support for an integrated cannabis use and anxiety reduction treatment. 41 Future treatment studies investigating the added value of addressing cannabis misuse, coping skills, and psychiatric disorders concurrently have promise.
There are a number of considerations that bear on the current results. First, the study design was cross-sectional, so causality in the relationships among these variables cannot be definitively inferred. Longitudinal research on the relationships between cannabis misuse and psychiatric disorders suggest that cannabis use can both initiate symptoms, and exacerbate pre-existing symptoms,10,11 but it is possible that the presence of symptoms may increase risk of cannabis use and misuse. Understanding the direction of these relationships and the underlying mechanisms for these bi-directional relationships is an important avenue for future research. Despite being cross-sectional, this study suggests coping motives are a meaningful motivational mechanism. Second, while the participants in this study were assessed using psychometrically validated dimensional indicators of CUD, anxiety, depression, PTSD, and somatic symptoms, they were not treatment-seeking individuals and did not undergo diagnostic assessments. As a result, these findings may not generalize to clinical samples in treatment settings. A related limitation is the lack of racial and gender diversity. Of the sample, 81.3% identified as White/Caucasian and there was no representation of gender non-conforming individuals. As such, these findings may not generalize to ethnically diverse or gender diverse populations.
Acknowledging these considerations, this study nonetheless contributes to understanding the relationship between cannabis motives and cannabis misuse, and “connects the dots” between cannabis misuse, motives, and psychiatric symptoms. Specifically, results revealed unique associations between cannabis misuse and social, enhancement, and particularly, coping motives. Further, this study revealed that coping motives was a significant mediator between cannabis misuse and somatic, anxiety, PTSD, and depressive symptoms. Taken together, these results lend support for a predominant negative reinforcement pathway in adult cannabis users, especially with regard to concurrent cannabis use disorder and psychiatric disorders. These results suggest that targeting maladaptive coping with cannabis may prove an effective treatment target in addressing co-occurring cannabis misuse and psychiatric disorders.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by the Peter Boris Centre for Addictions Research. The Peter Boris Centre for Addictions Research had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
Declaration Of Conflicting Interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: James MacKillop is a principal in BEAM Diagnostics, Inc. and consultant to Clairvoyant Therapeutics; no other authors have potential conflicts of interest to disclose.
Author Contributions
M.L.S., C.M., and J.M. contributed to study design, M.L.S. conducted the statistical analyses and wrote the first draft of the manuscript. C.M. contributed to data curation. C.M., I.B. K.R. & J.M. contributed to research conceptualizations and manuscript revisions. All authors contributed to and have approved the final manuscript.