
Abstract
Background:
Severe acute alcoholic hepatitis (AAH) has an extremely poor prognosis with a high short term mortality rate. As a result, many centers, including our own, have allowed transplant patients to be listed for transplantation prior to achieving 6-months of sobriety. Several scoring systems, designed to target patients with a minimal period of sobriety, have been proposed to identify patients with alcohol use disorder (AUD), who would be predisposed to relapse after liver transplantation. We investigated whether these scoring systems corroborated the results of the non-structured selection criteria used by our center regarding decision to list for transplant.
Methods:
We conducted a retrospective case-control study of 11 patients who underwent early liver transplantation for AAH matched with 11 controls who were declined secondary to low insight into AUD. Blinded raters confirmed the severity of the diagnosis of DSM-5 and scored the patients on a variety of structured psychometric scales used to predict alcohol relapse. These included the High Risk for Alcohol Relapse Scale (HRAR), Stanford Integrated Psychosocial Assessment Tool (SIPAT), Alcohol Relapse Risk Assessment (ARRA), Hopkins Psychosocial Scale (HPSS), Michigan Alcoholism Prognosis Score (MAPS), Alcohol Use Disorders Identification Test -Consumption (AUDIT-C), and Sustained Alcohol Use Post-Liver Transplant (SALT) scales. All patients who underwent transplantation were followed for harmful and non-harmful drinking until the end of the study period.
Results:
The transplant recipients had significantly favorable MAPS, HRAR, SIPAT, ARRA, and HPSS scores with cutoffs that matched their previous research. The SALT and AUDIT-C scores were not predictive of our selection of patients for transplantation. Despite an expedited evaluation and no significant period of sobriety, our case cohort had a 30% relapse to harmful drinking after an average of 6.6 years (5-8.5 years) of follow-up.
Discussion:
Despite the rapid assessment and the short to no period of sobriety, the patient cohort demonstrated a 30% relapse to harmful drinking, consistent with the 20% to 30% relapse to drinking rate reported after liver transplantation for all forms of alcoholic liver disease. Average scores from MAPS, HRAR, SIPAT, ARRA, and HPSS corroborated our current stratification procedures, with lower mean risk scores found in the transplanted group.
Conclusion:
Patients with AUD and severe AAH who obtain new insight into their disease and posses other favorable psychosocial factors have low rates of AUD relapse post-liver-transplantation. The psychosocial selection criteria for patients with alcoholic hepatitis in our institution are consistent with 4 of the 5 scoring systems investigated in their prediction of sobriety post-transplant.
Keywords
Introduction
Risk factors associated with alcohol relapse after liver transplantation have been extensively studied.1 -4 Length of sobriety has been shown to be a significant protective factor in sustained abstinence, therefore, historically, patients who require liver transplantation for alcohol-associated liver disease (ALD) have been asked to complete 6 months of sobriety before being considered for liver transplantation. 5 Patients suffering from severe acute alcoholic hepatitis (AAH) unresponsive to medical therapy have a mortality rate of over 70% by 6 months. 6 In this subset of patients, the 6 months sobriety rule is there for a virtual death sentence.
In highly selected patients, early liver transplantation for AAH has been shown to achieve excellent clinical outcomes with low impact on the donor pool.7 -9 We previously studied mortality in a case-control study of patients selected for transplant after a first episode of AAH 9 applying the selection criteria as originally outlined by Mathurin et al. 7 The psychosocial team sought candidates with a first liver decompensating event, new information on alcohol use disorder (AUD), motivation for sobriety, and strong social support. Special emphasis was placed on having good insight in the face of new liver disease as a practical way to measure readiness for transplantation. These basic criteria have become standard protocol in further studies of patients presenting with AAH.10,11
In an attempt to predict alcohol relapse after LT for those with alcohol use disorder (AUD) and ALD multiple scoring systems have both been created 12 and assessed for validation. 13 Commonly used scales to assess AAH patients for appropriateness for liver transplant include the High Risk for Alcohol Relapse Scale (HRAR), Alcohol Relapse Risk Assessment (ARRA), Hopkins Psychosocial Scoring System (HPSS), Sustained Alcohol Use post-LT (SALT), Stanford Integrated Psychosocial Assessment Tool (SIPAT), Michigan Alcoholism Prognosis Scale (MAPS), and the Alcohol Use Disorder Identification Test – Concise (AUDIT-C).5,14,15
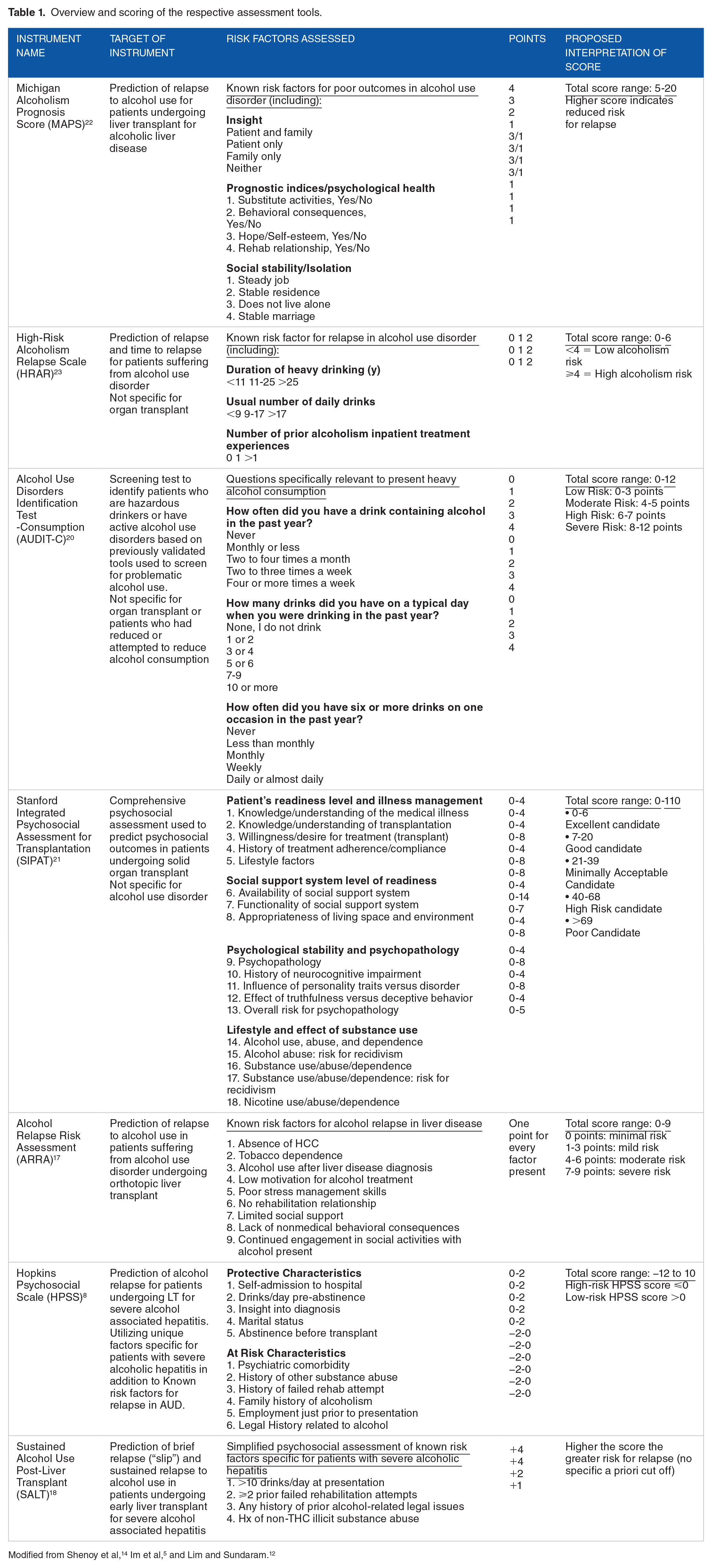
These scoring systems were each created to address disparate factors and clinical concerns. The MAPS was conceived through a conceptual review of the alcohol addiction literature; and was intended to help treatment planning in liver transplant candidates. 16 The ARRA was retrospectively created using a regression analysis of 25 risk factors. Nine were found to strongly correlate with post LT alcohol relapse; less than 6 months of sobriety was not associated with relapse rates in the multivariate model. 17 The HPSS and SALT were also created at transplant centers utilizing a retrospective review of risk factors, designed for the explicit purpose of assessing risk for relapse in LT recipients with alcohol-associated hepatitis (AH).8,18 The HRAR was originally proposed to predict relapse in a non-transplant population but was later adapted by Yates et al to help listing decisions when the patient was in early remission. 19 The AUDIT-C was designed as a screening tool for AUD by the World Health Organization. 20 The SIPAT is a general psychosocial assessment tool for transplant recipients. 21 Table 1 summarizes the factors and scores assessed by the respective assessment scales.
Overview and scoring of the respective assessment tools.
Multiple studies have examined the predictive value of the MAPS with mixed results.16,24,25 In one study, the HRAR was found to predict AUD relapse in liver transplant patients 26 but its predictive ability in subsequent studies has been uneven. The SIPAT has been shown to predict morbidity post-transplant 27 as well as AUD relapse. 13 The ARRA was designed to predict relapse in a retrospective review of AUD patients after liver transplant 17 but this has not been replicated. The HPSS helped to identify patients relapsed to harmful drinking after a median follow-up of 1.5 years in a cohort of 17 transplanted patients. 8 In a cohort of 138 patients a score greater than 7 on the SALT scale was associated with relapse to any alcohol use post liver transplant. 13 In one study the AUDIT-C was found to be predictive of excessive alcohol consumption post-liver transplant. 28 In one study the AUDIT-C was found to be predictive of excessive alcohol consumption post-liver transplant. 28 Table 2 summarizes prior studies that have been carried out to assess the validity of the respective assessment scales with regards to predicting outcomes post liver transplant for ALD.
Summary of validity studies of scoring systems used to assess patients with ALD for suitability for transplant listing.

In our initial study, we prospectively rated inpatient candidates as having good, developing, or poor insight as they presented to our center with severe AAH. No scales were used in selecting patients with the characteristic of good or developing insight. We hypothesize that the psychometric properties of the scales included here, will validate our process of selecting patients based on either good or developing insight about their alcohol misuse. Furthermore, we present the 6-year follow up outcomes along with the individual psychometric scores of the first transplanted patients at our center, as compared to patients not transplanted.
Methods
Between 1 January 2012 and 6 January 2015 the psychosocial team at the Recanati-Miller Transplantation Institute at Mount Sinai Hospital evaluated 81 AAH patients, with less than 3 months of sobriety, for early liver transplantation. Twenty-two (27%) were psychosocially cleared for expedited listing with 11 patients eventually transplanted. Both psychiatry and social work independently evaluated all potential candidates with this presentation in the hospital. In addition to the patient’s interview, the level of addiction was corroborated with family and friends. The control group (n = 11) were age, sex and year-matched patients from the cohort who were also evaluated as inpatients but declined for psychosocial reasons (n = 59). Two psychosomatic fellows (AD and KM) retrospectively reviewed the psychiatric and social work data that confirm the diagnosis of AUD DSM-5 and scored HRAR, ARRA, HPSS, and SIPAT. The assessors were blinded to the evaluation decision and transplant results. The MAPS, AUDIT-C and SALT were scored by one of the authors (AS) who had originally evaluated all patients. Scores of psychosocially accepted cases and declined controls were compared using 2-tailed t-tests with 95% confidence intervals. The sensitivity and specificity for the cutoff points used for these scoring systems was calculated. The mean psychometric scores of cases and controls were compared to patient populations in the reviewed literature.
The follow-up data of all patients who underwent AAH transplantation have been collected for harmful drinking for a minimum of 3 years. All patients were seen every 2 weeks in the first 3 months after transplantation, monthly for the next 6 months, and every 3 to 6 months depending on stability in the first 3 years. Regular post-transplant interviews, routine, and random urine ethyl glucuronide (uETG) tests, participation of social workers and corroboration from family and outpatient providers helped with the evaluation of relapse. IRB approval was obtained for a review of the chart of all patients evaluated for early LT at Mount Sinai Hospital.
Results
Of the 81 patients evaluated by the psychosocial team for alcoholic hepatitis, 11 (14%) were psychosocially cleared and transplanted. All cases (n = 11) and controls (n = 11) met the criteria for AUD and had similar durations of sobriety prior to evaluation (mean 35 vs 22 days, P = .08). Transplanted cases versus controls tended to present with their first liver decompensation (73% vs 27%) and with good or developing insight (91% vs 27%). Both groups had similar levels of acceptable social support (100% vs 73%). Three cases presented with their second liver decompensation and were transplanted due to overwhelming support from the recipient review committee. A case with poor insight was cleared and transplanted similarly. The number of drinks per day, years of drinking, failed rehabilitation history, and family history were not different between the groups (Table 3).
Characteristics of cases and controls with scoring systems.

The MAPS, HRAR, SIPAT, ARRA, and HPSS discriminated between cases and controls. The mean case score was a higher MAPS (m = 17.1), lower HRAR (m = 2.0), lower SIPAT (m = 23.5), lower ARRA (m = 2.3), and higher HPSS (m = 2.4). The AUDIT-C and SALT scores were not significantly different between the groups. The AUDIT-C mode was 12 (the maximum score) in both groups (Table 4).
Scoring system results.

Cut-off scores of: MAPS 14, HRAR 3, SIPAT 40, ARRA 4, and HPSS 0; suggested a classification of the cases and the controls in the expected direction. No single cut-off score on any of the tools would have selected transplanted patients in this cohort or declined patients in the control. A heat map was created to illustrate the wide range of color-coded scores with respect to the risk of relapse (Figure 1).

Heat map of cases and controls with 5+ year follow up.
One transplanted patient died in the first 6 months from postoperative complications. The surviving transplanted cohort (n = 10) had positive psychosocial characteristics with low HRAR (m = 2.0), low ARRA (m = 2.3), high HPSS (m = 2.4), low SALT (m = 3.8), and low SIPAT (m = 23.5). The cohort has been followed from 5 to 8.5 years (mean = 6.6 years). Three patients (#4, #5, and #11) relapsed to regular alcohol use, one dying of liver failure (Figure 1: Heat map).
Discussion
In prospective studies of risk factors for relapse in liver transplant patients, a diagnosis of alcohol dependence (severe or moderate AUD), a family history of alcoholism, low social support, and a shorter duration of pretransplant sobriety predicted relapse. 4 However, in cases of severe AAH in which there is limited time to wait for a longer period of sobriety or to refer to AUD treatment, a new paradigm must be sought. Our transplant cohort, like the control group, had a high burden of alcohol use, addictive behavior, and genetic load, as demonstrated by the high AUDIT-C score in both groups. Outpatient compliance with addiction treatment was not possible because many of these patients were too sick for discharge. Despite this, the primary criteria for selecting patients with new decompensated liver failure, good insight into their addiction, and strong social support helped identify a successful cohort with a 20% relapse rate after a mean of 5 years follow-up 9 and a 30% relapse rate after a mean follow-up of 6.6 years. This relapse rate is consistent with the reported 20% to 30% relapse to heavy drinking after liver transplantation for all forms of alcoholic liver disease. 35 We cannot comment on the potential relapse outcomes of patients who were not transplanted and did not survive.
Validated cut-off scores 14 of the HRAR < 3, ARRA < 4, HPSS > 0, and SIPAT < 40 would have corroborated the stratification process used in our center. However, given the recent findings from a large multicenter trial that SALT scores below 5 had a 95% NPV for sustained alcohol use post LT, 18 it is possible that our psychosocial clearance was too strict and 5 out of the 11 controls would have been deemed acceptable candidates by this score alone.
The MAPS was highly correlated with our institutional psychosocial assessment, possibly because its emphasis on insight as a protective factor 36 paralleled our use of emerging insight in the face of new liver disease. The use of new information has been a practical way to measure readiness for transplantation. This finding is consistent with previous studies that have identified self-awareness of choice behavior (insight) as a prediction of substance disorder related choices in addiction. 37 Similarly, SIPAT and HPSS, with their focus on readiness for transplant and social support,8,27 were correlated with our institutional assessment. This is comparable to previous research that identified social support as a protective factor against relapse to alcohol use disorder.38,39 Interestingly, there was a statistical difference in HRAR scores between the 2 groups, although it is composed of elements, 23 which are also risk factors for AAH. 6
For this study we utilized previously studied, numerically scored, psychosocial tools used to help selection of liver transplantation candidates with lower risk of relapse. As the study population was focused on patients undergoing expedited transplant listing, tools that utilized extended abstinence as a variable, such as a recently developed tool that required follow up time to observe if the patient followed up with an intensive outpatient program (IOP) 11 were not utilized in this study.
As the medical community has moved to view alcohol use disorder as a disease and not a vice, it has become universally accepted that patients with ALD should not be automatically excluded from receiving a liver transplant.40,41 While the assessment of patients with ALD has been criticized as somewhat subjective 42 and inconsistent,43,44 the use of numeric scoring systems partially alleviates these ethical challenges by introducing a numeric score that can be used consistently to portray a patient’s alcohol related behaviors and relapse risk. In our study, scores from the objective scales largely reflected the risk stratification that our institution employed in our initial AAH transplant population.
Limitations of the case-control include the retrospective nature of our data collection and our small sample size of patients cleared and transplanted. The small sample size was largely a function of the high mortality associated with severe AAH and that only 27% of all potential transplant candidates evaluated psychosocially were deemed acceptable by the methods used at our center. This clearance rate was similar to the Franco-Belgian study done by Mathurin et al 7 using similar criteria for clearance. Larger cohorts that include a wide range of risk scores will be necessary to validate the use of any of these tools, as well as to analyze which individual factors can prognosticate a favorable candidate in this unique population.
Conclusions
Patients with AUD and new information on their addiction, social support, and readiness for transplantation at the time of evaluation for transplantation have low rates of alcohol relapse after transplantation. Scoring systems may approximate and assist in directing this traditional selection process. Pre-existing scoring systems may have varying utility in their ability to assist in making this determination. Patients with ALD should instead be evaluated to stratify risk for selection for transplantation and should be referred for AUD treatment and post-LT follow-up. Centers that perform liver transplants for patients with alcoholic hepatitis should include a psychosocial team with addiction experience and consider known risk factors for AUD relapse in their initial assessments.
Footnotes
Author contributions
AD was involved in preparing the manuscript, as well as retrospectively reviewing the psychiatric and social work data confirming the DSM-5 diagnosis of AUD and scored the HRAR, ARRA, HPSS, and SIPAT. PD was involved in preparing the manuscript. KM was involved in retrospectively reviewing the psychiatric and social work data confirming the DSM-5 diagnosis of AUD and scored the HRAR, ARRA, HPSS, and SIPAT psychometric scales. OM was involved in preparing the manuscript. ES performed the initial pre-transplant psychosocial evaluation. LF performed the initial pre-transplant psychosocial evaluation. ME performed the initial pre-transplant psychosocial evaluation. GI performed the pre- and post-transplant medical evaluations. AS was involved in editing the manuscript, performed the initial pre-transplant psychiatric evaluations and retrospectively scored the MAPS, AUDIT-C and SALT psychometric scales.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.