
Abstract
Many previous studies have discussed an association between alcohol use disorder (AUD) and seizure incidents. There are also case reports of seizures during opioid withdrawals. Therefore, it is possible that AUD patients may have a higher risk of seizures if they also have opioid use disorder (OUD). However, it remains unproven whether AUD patients with a dual diagnosis of OUD have higher seizure incidents, to our knowledge. This study explored seizure incidents among the patients with a dual diagnosis of AUD and OUD as well as seizures among AUD only or OUD only patients. This study utilized de-identified data from 30 777 928 hospital inpatient encounters at 948 healthcare systems over 4 years (9/1/2018-8/31/2022) from the Vizient® Clinical Database for this study. Applying the International Classification of Diseases 10th Revision (ICD-10) diagnostic codes, AUD (1 953 575), OUD (768 982), and seizure (1 209 471) encounters were retrieved from the database to examine the effects of OUD on seizure incidence among AUD patients. This study also stratified patient encounters for demographic factors such as gender, age, and race, as well as the Vizient-categorized primary payer. Greatest gender differences were identified among AUD followed by OUD, and seizure patient groups. The mean age for seizure incidents was 57.6 years, while that of AUD was 54.7 years, and OUD 48.9 years. The greatest proportion of patients in all 3 groups were White, followed by Black, with Medicare being the most common primary payer in all 3 categories. Seizure incidents were statistically more common (P < .001, chi-square) in patients with a dual diagnosis of AUD and OUD (8.07%) compared to those with AUD only (7.55%). The patients with the dual diagnosis had a higher odd ratio than those with AUD only or OUD only. These findings across more than 900 health systems provide a greater understanding of seizure risks. Consequently, this information may help in triaging AUD and OUD patients in certain higher-risk demographic groups.
Introduction
Several previous studies have discussed an association between alcohol use disorder (AUD) and seizure incidents.1 -5 Although alcohol consumption in general is not proven to be associated with a higher risk of seizures, previous studies have examined an association between AUD and seizures. 2 For example, Hillbom et al2 argued that seizure prevalence among AUD patients is more than 3 times higher than those of the general population. However, reported prevalence rates of seizures among AUD patients have been varied; 9.9% in a study done by Tartara et al, 6 9% to 25% by Hillbom et al, 2 and 9.2% by Mattoo et al. 7 In particular, seizures and alcohol withdrawal appear to be correlated. The incidence of seizures is reported to be greater than 5% among patients with untreated acute alcohol withdrawal. 8
Opioid use disorder (OUD) may be associated with seizure activity as well. For example, tramadol was found to lower the threshold for seizures.9,10 However, there are also many case reports of seizures during heroin withdrawals.11 -13 Another study found that the odds ratio of unprovoked seizures due to opioid withdrawal was 2.58. 14 Mattoo et al 7 reported the prevalence of seizures was 12.5% in OUD patients.
Given the independent associations of AUD and OUD with seizures, it is possible that AUD and OUD may synergistically further increase seizure incidence. However, to our knowledge, no study has been conducted to make a connection between OUD and seizure incidents among patients with AUD. This study, therefore, was aimed at exploring seizure incidents among AUD and OUD patients. Namely, this study compared the frequency of seizures in patients with AUD and OUD to those with AUD or OUD alone. These findings can permit better seizure risk identification for patients with AUD and OUD as well as those with other demographic factors. This information can provide a greater understanding of seizure risks and, consequently, improve patient care in triaging AUD and OUD patients within certain higher-risk demographic groups.
Methods
Data collection
This research analyzed de-identified source data from the Vizient® Clinical Database. The data range was 4 years (9/1/2018-8/31/2022), representing 30 777 928 hospital inpatient encounters from 948 health systems in the United States. The International Classification of Diseases 10th Revision (ICD-10) diagnostic codes were employed to retrieve all encounters for seizures (G40 codes), AUD (F10 codes), and OUD (F11 codes). The duplicate diagnostic codes/encounters were removed, and thus the first visit codes/encounters were counted for this study. This is published data and does not deal with human subjects, and therefore, an Institutional Board Review approval was exempted; the study was approved by Vizient, Inc.
We examined 3 groups of encounters (seizures, AUD, and OUD) to evaluate possible associations between OUD and seizure incidents among AUD patients. The description of the data summary is listed in Table 1. In addition, the data sets were analyzed, stratifying the patient groups by demographic (sex, age, and race) and payer factors.
Data summary.
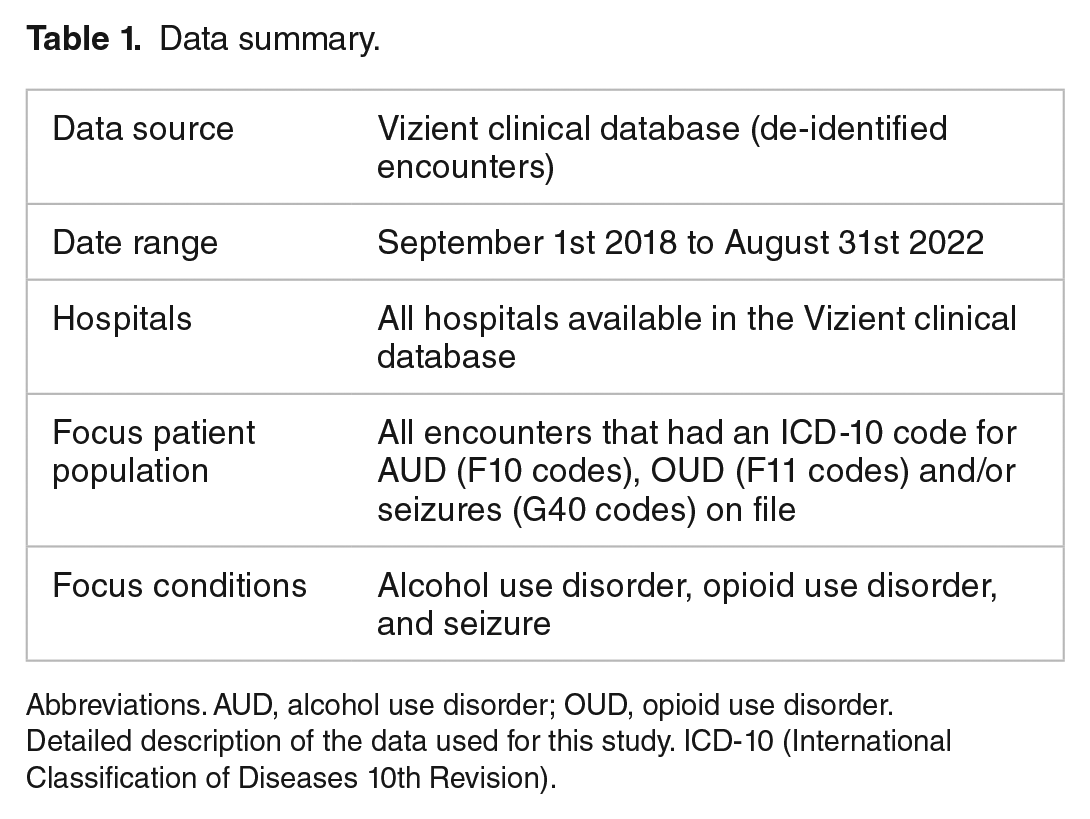
Abbreviations. AUD, alcohol use disorder; OUD, opioid use disorder.
Detailed description of the data used for this study. ICD-10 (International Classification of Diseases 10th Revision).
Statistical analyses
Associations between the 3 diagnostic code groups of AUD, OUD, and seizures were examined using Chi Square analysis and odd ratio analysis, with which alpha was set as .005 (α = .005). In addition, the diagnosis groups were stratified by demographic factors (age, gender, and race) as well as the Vizient-categorized primary payer. Microsoft SQL Server Management Studio 18 (SSMS 18) was used to retrieve the data sets, which were stored in Microsoft Excel (Microsoft 365 Version 2210). Tableau (Version 2021.4) was employed for chart images and IBM SPSS (Version 28.0.0.0) for statistical analyses.
Results
A descriptive analysis of the data was conducted first. Out of the 30 777 928 total encounters, utilizing the ICD-10 codes, 3 groups of encounters (seizures, AUD, and OUD) were retrieved. The most common diagnostic ICD-10 codes were AUD, followed by seizure, and lastly OUD (1 953 575; 1 209 471; and 768 982, respectively). Then, these data sets were reviewed to include demographic information, specifically age, gender, race, and primary payer.
This study extracted patient group demographic and payer information for (1) all-group total encounters, (2) seizure group, (3) AUD group, and the (4) OUD group (Table 2).
Summary of Demographic Analyses.

Age, sex, race, and insurance information for seizure, alcohol use disorder (AUD) and opioid use disorder (OUD) encounters, compared to all encounters from September 2018 to August 2022.
Demographic analyses
Total encounters
The majority of total encounters were female (55.2%) with the mean age of 58.7 years. Most patients were White (66.6%), followed by Black (18.8%). Most of the encounters were classified as Medicare (44.1%), followed by Commercial/ Private (27.9%), and Medicaid (20.6%).
AUD encounters
Males had a much higher frequency of AUD diagnosis (71.7%) than females (28.3%). The mean age for AUD was 54.7 years; most AUD patients were White (68.1%), followed by Black (18.7%). The most common primary payer for AUD encounters was Medicare (36.8%), followed by Commercial/ Private (28.5%), and Medicaid (21.0%).
OUD encounters
The mean age of OUD patients was 48.9 years. Males more often carried an OUD diagnosis (54.2%) than females (45.8%). The majority of OUD encounters were White (71.3%), followed by Black (18.4%), and most encounters were covered by Medicare (50.2%), followed by Commercial/ Private (27.8%), and Medicaid (12.4%).
Overall, gender differences were greatest for patients with AUD (71.7% male vs 28.3% female), followed by OUD (54.2% male vs 45.8% female), and seizure incidents (50.3% male vs 49.7% female), although females had a higher rate in total encounters (male 44.9% vs. female 55.2%). This indicates AUD and OUD are more common in men, but with negligible gender difference for seizures. The mean age of seizure incidents was 57.6 years, while AUD and OUD had a mean age of 54.7 and 48.9, respectively, indicating that seizures tend to take place later in life compared with AUD and OUD. The most common primary payer overall for each group was Medicare, followed by Commercial/Private, and Medicaid. OUD encounters had a much lower rate of Medicaid utilization (12.4%), compared to AUD (20.6%), seizure (16.9%), or all encounters (20.6%). AUD had the highest utilization of self-pay (8.2%), compared to OUD (5.2%) and seizures (2.7%).
OUD influence on seizures among AUD patients
Employing Boolean logic (Figure 1), this study quantified patient diagnostic codes in each category (Table 3).
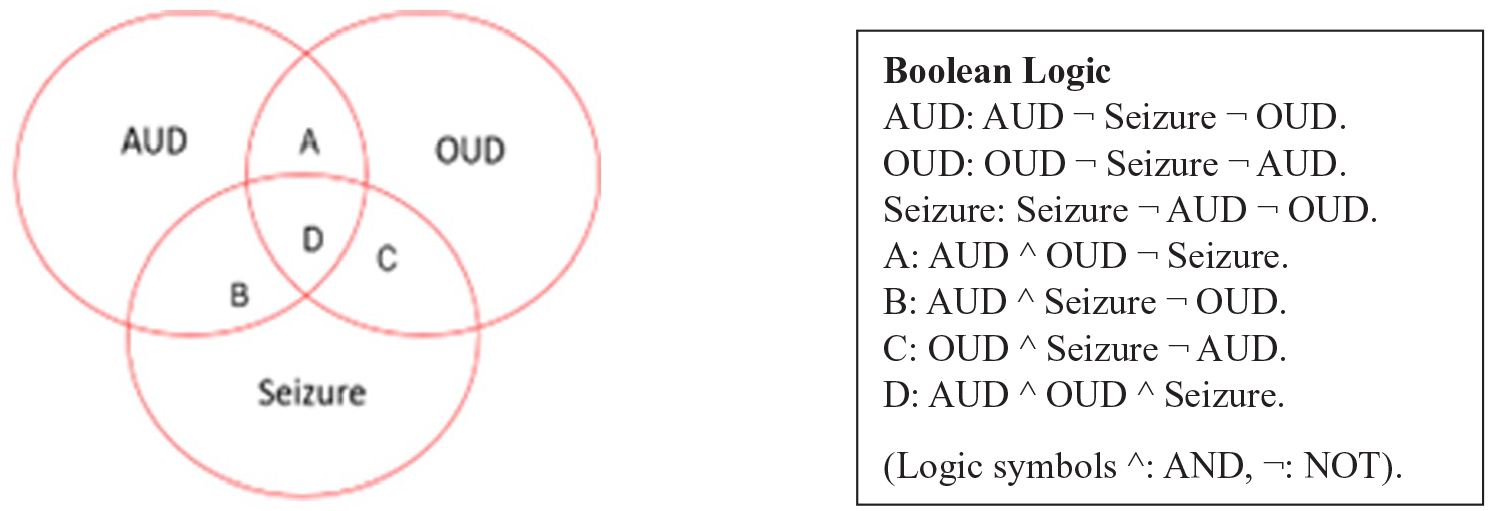
Boolean logic for AUD, OUD, and seizure incidents. 9 Visual description of alcohol use disorder (AUD), opioid use disorder (OUD), and seizure interface and Boolean logic codes for each section.
Summary results of associations among seizure, AUD, and OUD.
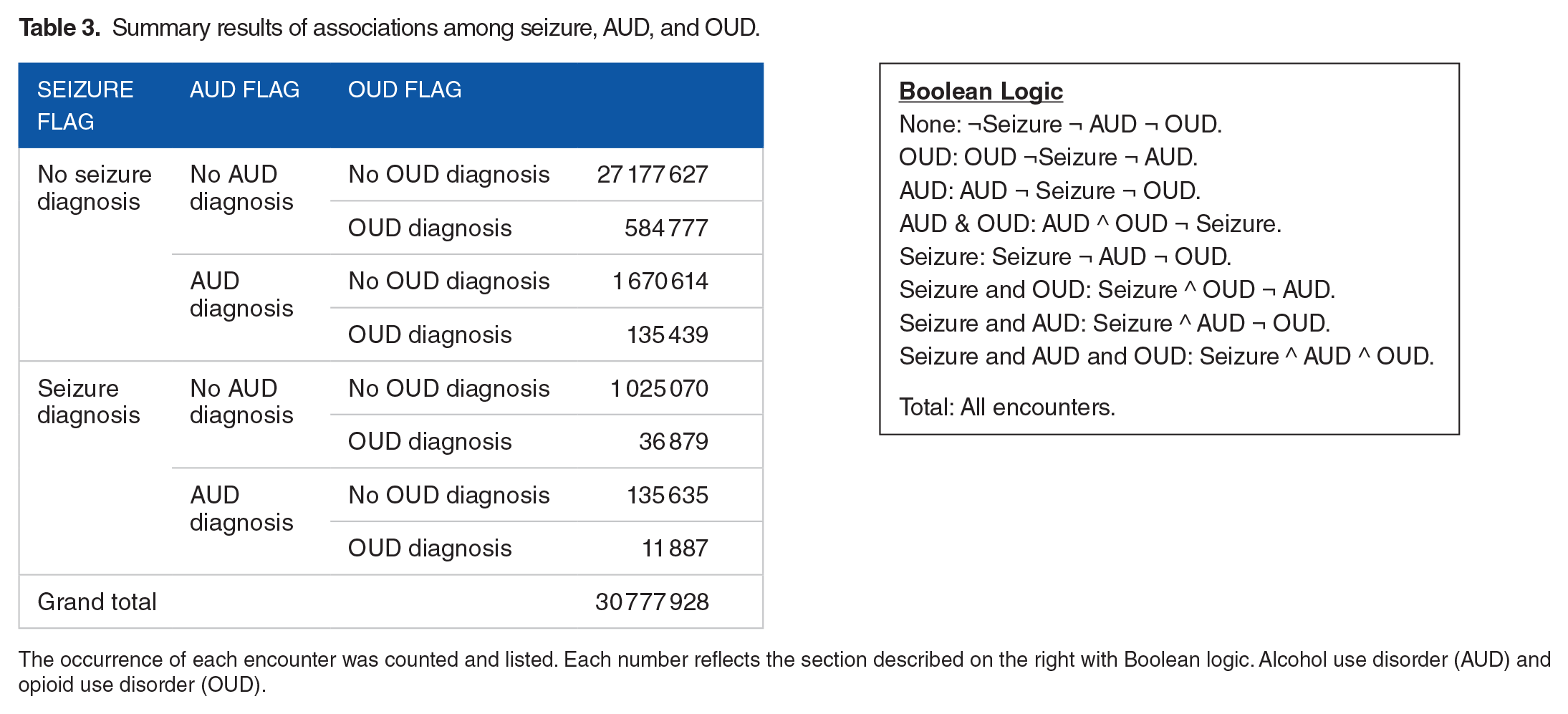
The occurrence of each encounter was counted and listed. Each number reflects the section described on the right with Boolean logic. Alcohol use disorder (AUD) and opioid use disorder (OUD).
Of the total encounters (N = 30 777 928), AUD without OUD nor seizure (1 670 614) was more common than OUD without AUD nor seizure (584 777). To identify the incident percentages of seizure, each group of incidents (OUD, AUD, seizure and AUD, seizure and OUD, AUD and OUD, and seizure and AUD and OUD) were examined. The percentage of each category was calculated and listed in Table 4.
Incident percentages of seizure, AUD, and OUD encounters. 9

The total counts and percentages for each category are listed. Alcohol use disorder (AUD), and opioid use disorder (OUD).
Almost 4% of total encounters included a diagnostic code for seizure while 6.35% and 2.50% of all encounters included codes for AUD and OUD, respectively. Because the data came from hospital inpatient encounters, these percentages should be lower compared to those of the general US population. For example, the percentage of health care professional visits of the general population in 2021 was reported to be 82.3% in the US. 15 This study found the percentages of the 3 groups were as follows; seizure was recorded for 7.55% of AUD encounters, 6.34% of OUD encounters, and 8.07% with both AUD and OUD encounters. Seizure incidents among patients with AUD took place at a significantly higher rate when OUD was present (8.07%) than when OUD was not present (7.55%), with a statistical significance, χ2 (1, N = 30 777 928) = 6716.968, P < .0001); chi-square test of independence). The odd ratio of seizure incidents was higher for patients with a dual diagnosis of OUD and AUD (OR = 2.200, 95% CI [2.160, 2.240]), compared to those with AUD only (OR = 2.163, 95% CI [2.153, 2.175]) or OUD only (OR = 1.708, 95% CI [1.694, 1.725]). Therefore, those with a dual diagnosis of AUD and OUD as documented in their charts are more likely to present with a seizure.
Discussion
Demographics
Gender
This study found that AUD and OUD incident rates vary by gender. AUD was much more common among males (71.7%) than females (28.3%). It is reported that even though alcohol-related injuries are more common among males than females, increasing numbers of women have started drinking in recent years, narrowing the gender gap of AUD patients. 16 Regarding gender differences among those with OUD, men have higher opioid overdose-related death rates especially, however women have a higher rate of emergency department consultation for opioid misuse.17,18 Our study found a negligible gender difference in seizure incidents, 50.3% male and 49.7% female encounters. This data agrees with a Danish study, finding no gender difference related to localization-related epilepsy yet differences depending on seizure subtypes. 19
Age
The mean age of the 3 diagnostic code groups was lower than that of total encounters; the mean age of the total encounters was 58.7 while seizure 57.6, AUD 54.7 and OUD 48.9. Regarding AUD, alcohol is the most common drug of abuse among older adults. 20 For example, White et al 21 found an increase in alcohol consumption among people aged 55 to 64 years. On the other hand, the mean age of OUD patients was 48.9, approximately 10 years younger than that of the total encounters. This might be due to the fact that opioid related overdose death rates have been increasing drastically, especially in the age group of 55 to 64 years old.18,22 In addition, this result indicates OUD may be more common in younger age groups, compared to AUD and seizure. However, the onset of AUD and OUD are reportedly similar; the mean age of AUD onset as 27.6, but the mean age of initial alcohol use was 21.39, 23 while that of opioid use onset was 25.6 years old. 24
Insurance
This study identified Medicare as the most common insurance payer for seizures, AUD, and OUD, as well as all encounters. This study found that the average age of all encounters was 58.7 years old and that of seizure 57.6, and AUD 54.7 years old. Therefore, many of the encounters may have included patients older than 65 years of age who were covered by Medicare. 25 Medicare includes coverage for substance disorder treatment in inpatient settings, which can also increase the number of encounters covered by Medicare. 26 Commercial or private insurance was the second most common insurance payer for all groups. This type of insurance covers those who are employed since it is typically paid for by their employers. Medicaid was the third most common payer in all encounter groups. Medicaid covers substance use disorder patients, except for the 10 states, where Medicaid expansion covers low-income patients. 27 However, more frequent coverage of OUD among older Medicare beneficiaries is thought to be largely due to social isolation and instability of housing conditions. 28 Additionally, AUD had the highest proportion of self-paid encounters (8.2%), compared to seizure encounters (2.7%) and OUD encounters (5.2%). More AUD patients may be able to afford to pay out-of-pocket without using insurance coverage, possibly to avoid having the diagnosis included in their personal health-insurance record.
Race
Race is an important determinant of health outcome among those with OUD and AUD. Based on Centers for Disease Control and Prevention (CDC) opioid-involved overdose death rates reported in 2015 to 2017, 15 in metropolitan areas of the United States, there is an increase in opioid overdose death rates mainly due to synthetic opioid use. Whites between 25 and 34 years of age were more involved in synthetic opioid drug usage in the illicit drug markets compared to other races and age group populations. 22 In this study, a similar result was obtained in OUD encounters among White patients, which were higher (71.3%) compared with other groups (Black 18.4%, Asian 0.4%, and other 7.9%). Siddiqui and Urman 29 demonstrated that White patients have a higher risk in developing OUD because they receive more pain management in surgical and clinical settings compared to other races. A meta-analysis study discovered that Black patients were less likely to receive opioid treatments for the same pain complaints as compared to those of Whites. 30 Another study argued that minorities were less likely to be treated for OUD. 31 Ransome et al 32 demonstrated that Black women with AUD have more adverse health effects than White women with AUD, with much of the difference due to socioeconomic status, healthcare factors, and psychosocial stressors. This study found that White patients have a higher incidence of seizure, AUD, and OUD. This might be due to a higher incidence of alcohol and opioid use as well as their treatments, which could lead to AUD, OUD, and correlated increasing seizure incidents among White populations.
OUD and seizure among patients with AUD
Although a dual diagnosis of AUD and OUD is not uncommon, there has been little research conducted on the combined impact of AUD and OUD on seizure development.33,34 This study demonstrated the first large-scale comparison between the interaction between AUD and OUD and on the incidence of seizure events. While the correlation between seizures and AUD or OUD individually have been previously discussed, the analysis in this paper exhibited a statistically significant increase in seizure incidents among patients with combined AUD and OUD compared to those with AUD or OUD alone.
While the mechanism for alcohol lowering the seizure threshold is well-documented, the mechanism for opioid related seizures seems to be more diverse and complicated by variation of both opioid type and opioid dosage. Alcohol’s primary action at high concentrations potentiates inhibitory effects of gamma-aminobutyric acid (GABA) receptors. Chronic use of alcohol results in tolerance development with down regulation of GABA and up regulation of N-methyl-d-aspartate (NMDA) glutamate receptors. 35 Sudden cessation of chronic alcohol consumption results in unmasking of central nervous system excitation involving GABA receptors that often takes the form of generalized tonic-clonic seizures. 36 One study reported that greater than 90% of all seizures resulting from alcohol withdrawal occur between 6 and 48 hours of cessation of chronic alcohol use. 37
In contrast, opioids act on the opioid receptors with the majority of the analgesic properties attributed to action on the mu-opioid (MOP) receptor; however, some opioids have additional activity at other opioid receptors or non-opioid receptors. 38 The kappa-opioid (KOP) receptor is an opioid receptor that has implications in analgesia, stress, depression, sedation, and diuresis. 39 In a study involving mice, KOP receptor antagonism caused increase seizure-like activity while receptor agonism caused a reduction in seizure-like activity. 40 In addition, inhibition of the serotonin and norepinephrine reuptake pathway has been postulated as a mechanism behind tramadol’s adverse effect of lowering the seizure threshold. 41 Furthermore, inhibition of GABA and histamine H1-receptor activation has also been suggested as a mechanism for tramadol increasing seizure risk.42 -44 Thus, the greater incidence of seizures among patients with concurrent AUD and OUD is likely the result of a direct additive effect of reducing the seizure threshold through alcohol and opiate action upon the same or similar signaling pathways. Other unknown potentiating effects may also be involved. One recent case study reports development of seizure in a patient who has been taking tapentadol, an opioid not known to cause seizures. 9 This case report posits that there may be an interaction with another drug that the patient might have been taking concurrently such as heroin. Another study examining seizure development in patients concurrently taking cocaine and alcohol concludes that cocaine use did not have an independent effect on risk of seizure but may accelerate alcohol-related seizures in predisposed patients. 45 Regardless of the mechanism, studies have shown that the combination of alcohol, opioids and/or other drugs results in more serious emergency department visits and longer hospital length of stay requiring greater vigilance in patient triage.46,47 This study adds support to previous findings, indicating that AUD and OUD patients have further increased risk of seizure and thus require a higher level of care.
Limitations
One of the key strengths of this study is the large sample size. However, the incidence rates of AUD, OUD, and seizures in this analysis were done using individual inpatient encounters, not individual patients. Since it is likely that patients included in this analysis had readmissions, the actual individual patient number may be lower than the figures presented. Additionally, this study examined hospital inpatient encounters and excluded outpatient encounters. So, the actual rates of the 3 ICD-10 encounters of seizure, AUD, and OUD are most likely higher than presented in this study. Given the scale of data for this study, the presence of seizures, AUD, and OUD was determined through diagnostic coding, rather than more detailed chart review. In addition, temporal information is not accounted for regarding the frequency of seizures, duration, or history because this study focused on the ICD-10 diagnostic encounters instead of longer-term prevalence. Furthermore, this study did not include other demographics factors such as socioeconomic status of the patients, patients’ co-morbidity, co-taking medications and psychosocial factors that may have affected the diagnosis of seizure, AUD, and OUD. The increase in seizure incidence among patients with underlying AUD and/or OUD, when compared to patients who do not have 1 or the other of these diagnoses, suggested a connection to AUD and OUD to seizures; however, the causality between seizure incidents and AUD and/or OUD cannot be concluded from the findings and is beyond the scope of this study.
Conclusions
This study found that the frequency of seizure incidents was higher for patients with a dual diagnosis of OUD and AUD, compared to those with AUD only or OUD only. In addition, certain demographic populations also have a higher risk of seizures among these groups. This information may help in triaging AUD and OUD patients in these population groups. Therefore, patients in high-risk populations for seizures might require a higher level of care with closer monitoring than other groups.
Footnotes
Author Contributions
Concept and design: Furo; Acquisition of the data: Podichetty, Whitted, and Brimhall; Retrieval of the data: Podichetty; Analyses and interpretation of the data: Furo; Drafting of the manuscript: Furo, Zhou, and Torres; Critical revision of the manuscript for important intellectual content: Brimhall and Whitted; Statistical analysis: Furo; Administrative, technical, or material support: Whitted and Brimhall; Supervision: Furo and Brimhall.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Hiroko Furo has the following functions: 2022 to Present PleoPharma Clinical Trial Sub-Investigator: Marijuana use disorder medication 2022 to Present. AelisFarma Clinical Trial Co-Principal Investigator: Marijuana use disorder treatment 2023 to Present Curb Stimulant Clinical Trial Medical Clinician: Cocaine use disorder treatment.
Data Availability Statement
Data Sharing
Vizient states that data from Vizient’s Clinical Data Base is considered proprietary and is only shared with subscribing members.