
Abstract
Introduction:
Drug overdose is the leading cause of injury-related death in the United States. It has been linked to respiratory depression and cardiac toxicity, both of which can lead to cardiac arrest. Despite this potential association, few studies have examined this relationship, particularly in transport to the hospital. The purpose of this research was to determine if there was a relationship between opioid overdose and cardiac arrest in transport.
Methods:
A sample (n = 1 000 000) was utilized from the National EMS Information System (NEMSIS) from the year 2019. A logistic regression model was used to predict cardiac arrest from dispatch reason with gender, race, and age included as controls.
Results:
Overdose-related dispatch reason was associated with an increased likelihood of cardiac arrest in transport (Odds Ratio = 1.65, 95% Confidence Interval: [1.22, 2.22]).
Conclusions:
Opioid overdose is associated with an increased incidence of cardiac arrest in transport in the United States.
Introduction
In 2017, the Centers for Disease Control and Prevention (CDC) declared drug overdose the leading cause of injury-related death in the United States. 1 Of these deaths, 68% were due to prescription or illicit opioids, making opioids the largest drug contributor to overdose deaths. 1 Opioids are often considered an essential tool for managing pain for those with chronic conditions, moderate to severe traumatic injury, post-operative pain, or terminal health conditions such as cancer. 2 However, long-term use of opioids can cause a wide-range of side effects from nausea to dependence, and even respiratory depression leading to cardiac arrest. Recent studies have demonstrated that even in a hospital setting, opioid administration leads to respiratory depression in 1.5% of cases. 3 It rationally follows that these rates are even higher among people who use illicit drugs where medical personnel and technology are not present, and the drugs may be laced with other potentially toxic substances, including fentanyl.
Additionally, the rate of both prescription and illicit drug use has increased rapidly in the last 20 years. Between 1999 and 2011 in the United States, consumption of prescription hydrocodone increased by 200% and prescription oxycodone increased by 500%. 4 Within this time frame, the death rate due to prescription opioids quadrupled. 5 Since 2011 the opioid consumption rate has been almost cut in half, still not returning to the consumption rate at the turn of the century. 6 Overall opioid overdoses continue to rise, however, likely due to a decrease in the availability of prescription opioids and their subsequent replacement with drugs like heroin and fentanyl. Alarmingly, death rates due to prescription opioids have remained relatively constant since 2011, still almost 4 times higher than the rate in 1999. 7 If anything, the consumption and death rates due to heroin portray an even more alarming trend. National drug overdose deaths involving heroin are almost 15 times higher than they were in 1999. 7 This is likely due to that fact that illicit heroin is often laced with fentanyl, which is 50 to 100 times more potent than morphine, making it more deadly than any other opioid. 8 It has been hypothesized that this is the reason for the continued rise in opioid death rates, even after increased awareness by the CDC and NIH, as well as law enforcement organizations such as the DEA. 7
Treatment of cardiac arrest has also evolved since the turn of the century. From 1999 to 2010 cardiac arrest outcomes did not improve significantly, leading to new guidelines that emphasized CPR quality, minimization of interruptions, and standardized post-resuscitative care. 9 These guidelines—including the Resuscitation Outcomes Consortium (ROC), cardiac arrest registry (Epistry), and randomized clinical trials (RCTs)—led to a higher discharge rate for cardiac arrest patients than had been seen previously. Yet, even within hospitals, the likelihood of surviving a cardiac arrest event has only increased to about 20%. 10 Out-of-hospital cardiac arrest has an even lower survival rate of approximately 12%. 11
Opioids can cause cardiac arrest through both respiratory depression and cardiac toxicity. 2 As mentioned above, a common side effect of opioid use is respiratory depression which can lead to respiratory arrest and subsequent cardiac arrest. Additionally, opioids have been proven to inhibit sodium and potassium channels involved in the pacemaker potential. 12 This prolongs various phases of the action potential, prevents repolarization, and lengthens various cardiac intervals, potentially leading to cardiac arrest. This is known as cardiac (opioid) toxicity. Therefore, it is known that long-term substance use increases the risk of cardiac arrest, however it has not been determined if there is a relationship between opioid overdose and cardiac arrest in transport. Thus, the aim of this research is to determine if opioid overdose is related to an increased incidence of cardiac arrest for patients in transport compared to the incidence of cardiac arrest for those who did not overdose.
Methods
Sample
The National EMS Information System (NEMSIS) from the year 2019 was used for this study. 13 The NEMSIS is the national database that is used to store EMS data from states and territories within the United States. It includes data from 47 states and territories, 10 062 reporting agencies, and 34 203 087 events. Information regarding the EMS Agency, dispatch reason, ambulance crew, times to and from the destination, gender, race, age, payment information, scene information, situation, injury, cardiac arrest information, patient history, vital signs, laboratory results, examination results, medications, procedures, patient outcome, and location. Since this was a retrospective study, institutional review board approval was not required. All 34 203 087 events were included in this analysis originally. A random sample of 1 million subjects was used for the final analysis.
Data
A complete list of variables used for this analysis can be found in the table below. The variables dispatch reason, cardiac arrest etiology, reason CPR was discontinued, end of arrest event, gender, age, race, region, division, and urbanity were originally chosen to be controlled for in this logistic regression, based on variables controlled for in similar epidemiology research. 14 Using these variables, a dataset was created that contained cardiac arrest, dispatch reason, gender, race, and age. The primary outcome variable was cardiac arrest. NEMSIS defined cardiac arrest using the guidelines proposed by the Utstein Cardiac Arrest Criteria. 15 The primary explanatory variable was dispatch reason. Dispatch reason consisted of 44 reasons why EMS was dispatched. For purposes of this analysis, dispatch reason was transformed into a 3 factor categorical variable consisting of the groups overdose-related, cardiac-related, and other. The cardiac-related category consisted of the dispatch reasons cardiac arrest, non-traumatic chest pain, and breathing problems, as these are known to result in cardiac arrest. Gender (male or female), race (American Indian, Asian, African American, Hispanic, Hawaiian, or White), and age were extracted to serve as covariates in the analytical model.
Data analysis
A logistic regression model was used to predict cardiac arrest from dispatch reason. Gender, race, and age were included as covariates. Dispatch reason was analyzed as a factor, comparing the groups overdose-related and cardiac-related to the reference group other. Race was also analyzed as a factor, comparing American Indian, Asian, African American, Hispanic, and Hawaiian to the reference group White. Gender was analyzed as a binary variable and age was analyzed as a numeric. The primary explanatory variable of interest was overdose. The analysis was done using RStudio version 4.0.2. 16
Results
Descriptive statistics for the full sample can be found in Table 1. Overall, 0.74% of patients experienced cardiac arrest. The sample consisted of 45.5% females and 41.6% males. 37.9% of the sample was White, 15.2% was African American, 0.64% was American Indian, 0.36% was Asian, 0.15% was Hawaiian, and 2.9% was Hispanic. The median age of this sample was 61.00 years.
Sample descriptive statistics. NEMSIS 2019. n = 1 000 000.

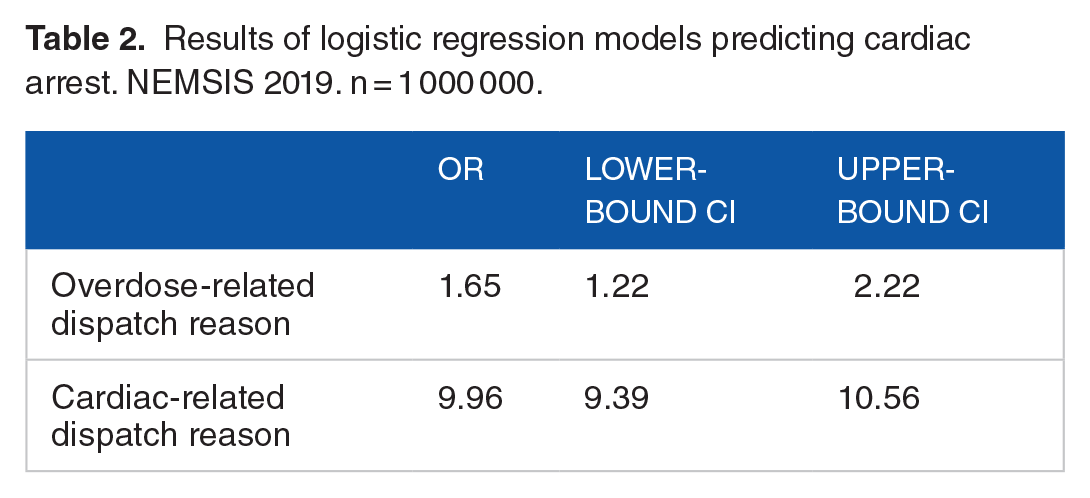
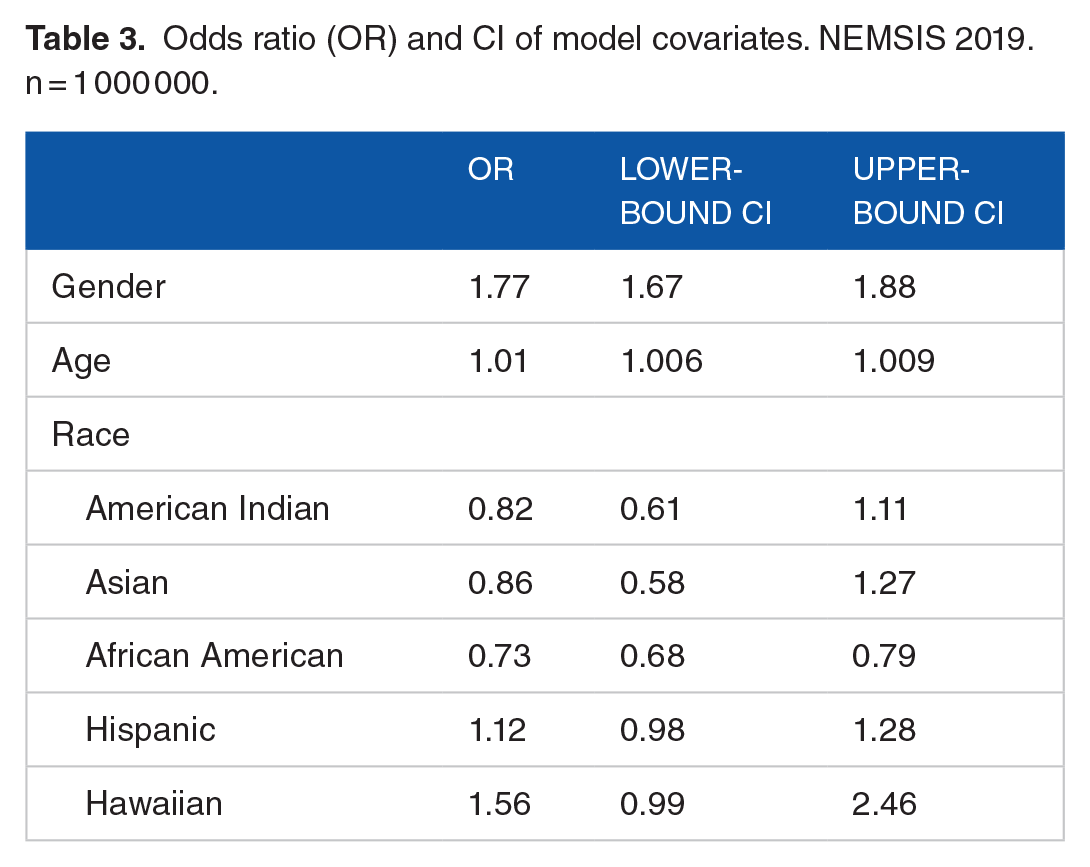
The results of the logistic regression model for the primary explanatory variable can be found in Table 2. Overdose-related (Odds Ratio = 1.65, 95% Confidence Interval: [1.22, 2.22]) and cardiac-related (OR = 9.96, 95% CI: [9.39, 10.56]) dispatch reasons were associated with an increased odds of cardiac arrest, when compared to the reference category other. Males were significantly more likely to experience a cardiac arrest (OR = 1.77, 95% CI: [1.67, 1.88]) compared to females (Table 3). Compared to the reference group, White, African Americans were significantly less likely to experience cardiac arrest (OR = 0.73, 95% CI: [0.61, 1.11]). No other race was significantly associated with cardiac arrest, although Hawaiian was trending toward an association with increased odds of cardiac arrest (OR = 1.56, 95% CI: [0.99, 2.46]). Additionally, an increase in a year of age was associated with an increased likelihood of cardiac arrest (OR = 1.01, 95% CI: [1.006, 1.009]).
Results of logistic regression models predicting cardiac arrest. NEMSIS 2019. n = 1 000 000.
Odds ratio (OR) and CI of model covariates. NEMSIS 2019. n = 1 000 000.
Discussion
Opioid overdose was significantly associated with cardiac arrest in this sample. While no known research has been done on the association between cardiac arrest and opioid overdose in transport, this result does reflect other research that found an association between cardiac arrest and opioid use during in-hospital care.14,17 Most recently, Sakhuja et al 14 found that cardiac arrest was much more common in patients with opioid overdoses and that opioid overdoses were independent risk factors for cardiac arrest. This study reflected the findings of Hörburger et al 17 who found that, within his emergency department, opiates were the leading cause of intoxication-related death. These findings—including those from this study—are all consistent with the known pathophysiology of overdose, including cardiac toxicity and respiratory arrest. Therefore, the findings of this study are congruent with prior research and the pathophysiology of opioid overdose, which suggests an association between cardiac arrest and opioid overdose in hospital, out of hospital, and in transport.
As mentioned above, there is limited epidemiological research on the relationship between opioid overdose and cardiac arrest, particularly in transport. Any research related to this topic appears to support the correlation between these 2 variables. Thus, there is currently no data that refute the association established in this and the other aforementioned studies. However, there are some limitations that must be considered when evaluating these results. To begin, the data obtained by NEMSIS relies on the reporting of first responders. 13 EMS workers face significant stressors in their careers, including pressures for efficiency, as well as trauma. 18 The CDC has proven that stress decreases workplace productivity. 19 This may mean rushing through paper work, or even pushing it aside. This can be seen in the NEMSIS data where only 58% of all reports included whether a patient experienced a cardiac arrest outcome, even though it is required to be reported as a “yes” or “no” in the reporting system. 13 In addition, there is evidence to suggest that this pressure and other factors result in very low to low accuracy within EMS systems. 20 This means that diagnoses of overdose and cardiac arrest may be incorrect, resulting in bias within the dataset.
In addition, much of the information obtained by first responders is given by patients. Thus, biases due to self-reporting are likely a limitation of this research as people try to hide behaviors they fear would be stigmatized. This means that the true incidence of opioid overdose within the EMS system is likely much higher than the reported incidence. Furthermore, first responders may be susceptible to bribery by patients who do not wish for their opioid use to be reported. A recent law review suggests that these healthcare workers are vulnerable to this kind of bribery. 21 EMS personnel may also lie for the benefit of themselves or their EMS organization, to avoid a lawsuit for example. 22 Therefore, there are many reasons why opioid overdose and cardiac arrest may be underreported, skewing the results of this study. However, this would likely make the results of this research more significant with an even higher odds of cardiac arrest due to overdose. This means that the results of this study are likely still applicable and useful.
Furthermore, there is no information provided by NEMSIS about other factors that contribute to the likelihood of cardiac arrest due to overdose. Most notably, information on the duration of overdose would likely be useful in evaluating the relationship between opioid use and cardiac arrest, as there is significant evidence to suggest that an increased duration of use would contribute to a higher incidence of cardiac arrest due to overdose. 23 These data may be found elsewhere and are a potential future direction of this research. In addition, the NEMSIS dataset did not differentiate between the types of opioid overdose. There is significant evidence that heroin overdose is much more likely to cause cardiac arrest than prescription opioids. 14 Again, these data may be found elsewhere and could be used to further this research. Also, data from the CDC and NIH suggest that opioid overdose and subsequent cardiac arrest varies by region.6,7 Thus, including region as a controlled variable in another logistic regression could provide more information about trends throughout the nation and around the world.
Finally, this study focused on only 2019 data. Comparing the 2019 incidence of cardiac arrest due to overdose to other years would allow researchers to evaluate trends in these data throughout time. This is important because there is evidence that opioid use disorder is increasing in the United States. 6 Therefore, future research could compare 2019 NEMSIS data to other years to evaluate this association in transport throughout the last decade.
This research may have several implications for EMS practice. Since opioid overdose has an association with cardiac arrest and the likelihood of surviving a cardiac arrest event outside of the hospital is 12%, it is essential that patients who are suspected to have overdosed on opioids receive Naloxone promptly. This medication reverses the effects of opioids and would likely reduce the chance of patients experiencing a cardiac arrest event due to opioid overdose. Thus, proper training for first responders on prompt recognition and treatment of opioid overdose would decrease the likelihood of these patients experiencing cardiac arrest. More research could be conducted in this area to evaluate the relationship between first responder training and cardiac arrest events, as well as the best ways to train first responders to recognize opioid overdose. Furthermore, EMS practice could also focus on preventing opioid overdose altogether through patient education. By preventing opioid overdose, they would prevent the risk of cardiac arrest from overdose. Again, this is a potential area for future research to determine how best to educate patients on opioid safety and the impact of such patient education on outcomes.
To conclude, opioid overdose is associated with an increased likelihood of cardiac arrest in transport. While a few studies have examined the relationship between opioid overdose and cardiac arrest, few to none have analyzed this association in transport. Therefore, this research contributes to our understanding of the relationship between these 2 variables by analyzing their association in a unique setting. This is significant for many first responders and emergency care workers, as this is a problem they will likely come across sometime in their careers. Furthermore, as the opioid public health crisis reaches epidemic proportions in the United States, this issue will likely become more and more prevalent in the lives of researchers, first responders, and emergency health workers. Further research in this area may have significant impacts in addressing this issue.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Marissa L Ritter and Matthew B McQueen contributed to the design and implementation of the research. Marissa L Ritter and Adam D Bohr contributed to the analysis of the results. All authors contributed to the writing of the manuscript.