
Abstract
Purpose:
Employment and family/social relationships are 2 of the highest priorities among those in substance use recovery. This study examined the relationship of work status with couple adjustment and other recovery capital treatment outcomes among symptomatic alcohol, substance use, and gambling participants (N = 38) using data collected in a randomized trial comparing a systemic Congruence Couple Therapy (CCT) and individual-based Treatment-as-Usual (TAU).
Method:
Change scores and associations between work status and couple adjustment together with 8 other recovery outcome variables at post-treatment (5 months from baseline) and follow-up (8 months from baseline) in TAU (n = 17) and CCT (n = 21) were analyzed.
Results:
Number of those working increased with both CCT and TAU but without reaching significance in either CCT (Cochran’s Q = 5.429, P = .066) or TAU (Cochran’s Q = 2.800, P = .247). Relative to those not working in the combined sample, those working showed significantly improved scores in post-treatment and follow-up in addictive symptoms, couple adjustment, psychiatric symptoms, depression, and life stress. Separating the CCT and TAU groups, similar trend was found in the CCT group but was inconsistent in the TAU group.
Conclusion:
Significantly greater improvement in addictive symptoms and recovery capital of couple adjustment, mental health, and life stress was found in the working vs not-working group. Compared to individual-based TAU, exploratory findings indicate that the systemic treatment of CCT showed a clearer and more consistent difference in improved working days, addictive symptoms and recovery capital. Replication with larger samples is needed to generalize these results.
Keywords
Defining alcohol and substance use recovery and treatment success as abstinence has been criticized as too narrow a criterion.1,2 A broader frame advanced to view recovery is that of recovery capital (RC), described as a building up of internal and external resources for a lifestyle characterized by productivity, supportive relationships, employment, physical and mental health, purpose, and citizenship.3-5 Various RC categories have been formulated to define the domains of protective and resilient factors in substance use recovery. 6 A recent RC conceptualization was also proposed for gambling disorder consisting of human, community, social and financial domains based on the reports of recovered gamblers. 7 The gambling RC identified are largely similar to the RC for substance use disorder, but physical health was not mentioned among problem gamblers and financial resources were more salient to gamblers. 7
Possession of a wide range of RCs aided recovery in its various stages and different RCs were deemed to work in concert with one another.7,8 Employment and family and social relationships are highly prioritized areas by those in recovery 9 and employment itself has consistently been identified as a top recovery goal. 10 Notably, family/social support6,7,11 and emotional regulation12,13 are both recognized as dominant recovery resources but their relationship to employment has been under-studied. Given these top recovery priorities, domains of RC that correlate with and are predictive of successful employment are important to map out to inform the effective structuring of treatment and recovery programs.
Employment as a key recovery capital
Employment is a key index of recovery, 10 strongly predictive of successful treatment completion and long-term recovery. 14 Job-related engagement during treatment is associated with higher post-treatment quality of life, more prolonged treatment and abstinence, 15 lower stress, and happiness. 16 Giving life stability in providing income and benefits, employment is also a path for career progression, and acts as a social deterrent for substance use. 8 It opens up access to social networks and support. 8 Conversely, unemployment has consistently been shown to impair mental health such as depression, anxiety, psychosomatic symptoms, subjective well-being, and self-esteem.17,18
Among polysubstance use individuals in recovery, those with a history of chronic physical and mental conditions have lower odds of being employed. 10 In one qualitative study, socially “integrated” and “marginalized” groups in treatment recovery demonstrated marked differences in work functioning, family connections, social network, and mental health. 19 Consistent with the above literature, employment has an association with the personal and social domains of RC 20 and less substance use dependence severity. 21
Intersections of different recovery capitals
Assessing substance use and gambling recovery using the framework of recovery capital is a compelling proposition, but empirical support for the inter-relationships among different RC domains is still in its infancy. Recovery capital items identified in the Assessment of Recovery Capital, 22 a predominant measure of RC, require more evidence for their correlations with each other to determine their interrelationships.23,24 One recent study found that improvement in gambling symptoms was positively associated with internal and external recovery capital and spirituality and negatively associated with anxiety, depression, and stressful life events. 25 Better delineations of the interconnections of different types of RC can help identify specific RC resources an individual lacks or possesses to target treatment goals and increase understanding of how each RC contributes to overall recovery. These delineations and empirical correlations would also serve to fortify the recovery capital construct and expand our understanding of contributing factors in recovery.
Couple and family capital in employment
The recovery capital literature points to social support, which includes group and family supports, as an important influence on employment and other recovery areas. 26 Employment can also improve couple relationships by reducing stress, pessimism, conflict, and increasing satisfaction with life.27,28 Job-related self-efficacy of one partner in a couple influences the other in enhancing work functioning through verbal persuasion and vicarious learning. 29 Family members can be a source of strength or detriment in recovery and work functioning.30,31 The indications that a connection exists between family support and employment invites further exploration.
To date, predominant employment interventions for recovering substance abusers have focused specifically on employment search and skills development 32 and less so as an integrated part of treatment with other areas of recovery such as improving couple and family relationships. A recent Norwegian study of employment-specific programs found improved work functioning among substance abusers enrolled in couple and family therapy. 33 In this study, improved work functioning correlated with decreased depression and couple distress levels and improved levels of family functioning. In a qualitative study of counselors case notes from a randomized controlled trial of a systemic treatment model, Congruence Couple Therapy, employment problems, and employment-related stress featured as central concerns to addicted clients in a large majority of CCT couple cases. 34 Tight linkages were found between employment stress with couple distress and addiction issues. The family-work interface has been studied for two decades in disciplines such as occupational psychology,35,36 but has not been exploited for treatment and recovery in the addiction field.
Treatment groups: Congruence couple therapy and treatment as usual conditions
This study examined the relationship between work status and couple adjustment and treatment outcomes among symptomatic alcohol, substance use, and gambling participants (N = 38) using data collected in a randomized controlled trial (RCT) comparing a systemic Congruence Couple Therapy (CCT) and individual-based Treatment-as-Usual (TAU).
CCT is a manualized, structured, systemic intervention that privileges the reciprocal interaction of primary client with addictive symptoms and their partner and the linkages among 4 dimensions: intrapsychic, interpersonal, intergenerational, and universal-spiritual to effect change.37,38 Addiction is conceptualized as an outcome of repeated problematic processes among and within the 4 dimensions. CCT offers a conceptual shift away from focusing solely on the individual and symptom reduction to addressing the complex underlying individual and relational processes related to addiction. Targets of intervention encompass the 4 dimensions of: (1) intrapsychic awareness and emotion regulation; (2) interpersonal awareness and acknowledgment in couple communication skills; (3) intergenerational awareness and acknowledgment of family of origin influences; and (4) universal-spiritual awareness and acknowledgement of the universal human needs for connection, safety, and worth. Descriptions of the CCT framework can be found in earlier publications.37,39,40 The comparison TAU condition reflects services couples normally received separately on an individual basis consisting of motivational interviewing, solution-focused therapy, cognitive-behavioral therapy, and relapse prevention.
CCT participants attended an average of 13 couple treatment sessions. TAU primary clients and partners attended individual-based counseling counselor, family support groups, and psychoeducation programs for an average of 8 sessions. TAU participants further received an average of 9 additional sessions between post-treatment and follow-up while CCT participants did not receive additional treatment during the follow-up period.
Purpose of study and research questions
There are 4 questions we sought to answer in this study: (1) Is there a change in work status (working in past 30 days) within the CCT and TAU groups over time? (2) Is there a difference in the change in work status between the CCT and TAU groups? (3) Is there improvement in couple adjustment and other RC areas in working versus non-working groups? and (4) Do couple adjustment and other RC areas improve significantly for CCT and TAU groups separately?
Methods
Assessment instruments
Work status
Work status in the last 30 days was assessed based on respondents indicating that they: (1) did not work, (2) worked 1 to 10 hours a week, (3) worked 11 to 30 hours a week, and (4) worked more than 30 hours a week. Those with one or more working hours per week were categorized as “working” versus “not working at all.”
DSM-5 alcohol use disorder (APA, 2013 41 )
Twelve binary items indicate symptoms of alcohol use disorder (AUD) in the last 12 months. Individuals endorsing 2 or 3 items indicate mild AUD, 4 to 5 items for moderate AUD, and 6 or more symptoms for severe AUD. The DSM-5 items were only administered at baseline for diagnostic purposes.
DSM-5 gambling disorder (APA, 2013)
This measure consists of 10 items scored in a binary fashion to indicate symptoms of gambling disorder (GD) in the last 12 months. A minimum score of 4 indicates positive for GD: 4 or 5 is mild; 6 or 7 is moderate; and 8 or 9 is severe. The DSM-5 for GD was only administered at baseline for diagnostic purposes.
Operationalization of recovery capital
Recovery capital as operationalized in this analysis consists of employment, couple adjustment, mental health, emotion dysregulation, and reduced life stress. These together with substance use and gambling were measured in 9 variables using standardized instruments. DSM-5 diagnostic criteria were used at baseline for AUD and GD for inclusion into the study.
Study participants
Main RCT sample
In the main RCT, inclusion criteria were one or both partners meeting DSM-5 criteria for AUD or GD, 18 years or older and couples were committed to their relationship by self-definition. Exclusion criteria were those with serious suicidal ideation or attempted suicide in the past year, reporting psychotic symptoms in the past month or recurring intimate partner violence, or were involved with loan sharks increasing risks.
Secondary sample
Drawing from the sample of the main RCT, data were analyzed for a sub-sample of 38 individuals, including both primary clients and partners with addictive symptoms meeting DSM-5 criteria for AUD or GD or who scored in the moderate to high risk categories in other types of substance use based on ASSIST, including cannabis, cocaine, sedatives, amphetamine, sleeping pills, and opioids. Of the sub-sample, 26 individuals met the DSM-5 criteria for AUD (45%) with a mean score in the severe range (M = 8.1, SD = 2.5) corroborating with the mean score on AUDIT (M = 20.6, SD = 7.1). Those meeting DSM-5 criteria for GD (3%) had a mean score in the moderate to severe range (M = 7.4, SD = 2.3) corroborating with their PGSI mean score of 12.6 (SD = 8.5). Those meeting both AUD and GD constituted 21% of the current sample. The sample reporting only other substance use (n = 12) had a mean score of 14.6 (SD = 9.9) on the ASSIST indicating moderate risk of health and other problems.
Statistical analysis
Data analysis was performed using SPSS version 26.0, and statistical significance for all analyses was determined at 95% CI (2-tailed test). The proportions of participants who reported not working versus those working in the last 30 days were described in percentages at O1 (baseline), O2 (5-month post-treatment), and O3 (8-month follow-up). The mean scores on substance use, gambling and RC measures using continuous data were calculated at each time point (as shown in Table 2). Within-treatment group changes in the percentages of participants who reported working in the last 30 days were examined using Cochran’s Q test across 3 time-points and McNemar test across 2 time-points.
Additionally, within-treatment group changes in mean scores on substance use, gambling and RC areas (psychiatric symptoms, couple adjustment, depression, PTSD, emotion dysregulation, and life stress) were assessed at 2-time points using Wilcoxon test because problem gambling and substance use measures did not meet normality requirements for parametric test. For between-group comparison, CCT and TAU difference in changes in the proportions of participants who reported working in the last 30 days were estimated at 2 and 3-time points using the z test.
Results
Baseline information of participants
Baseline demographic differences between the experimental (CCT) and control (TAU) groups were insignificant (see Table 1). Participants were majority males (55%), with a mean age of 46 years, 50% had post-secondary education, and an annual household income of $100 000 or higher (55.3%). The mean scores for the combined CCT and TAU groups for both working and not working status (N = 38) for the RC outcomes at O1, O2, and O3 are displayed in Table 2.
Demographics of sample with addictive symptoms.

Group equivalence in baseline characteristics with categorical responses were assessed with a Chi-square test. Group equivalence in age was assessed with a t-test.
Mean substance use, gambling and recovery capital scores for the combined CCT and TAU groups (N = 38) at baseline (O1), post-treatment (O2), and follow-up (O3).

Note. The sample comprises both working and not working groups.
Question 1: Change in work status in CCT and TAU
CCT participants who reported working in the last 30 days were 71.4% at baseline, 90.5% post-treatment, and 71.4% at follow-up. TAU participants who reported working in the last 30 days were 41.2% at baseline, 47.1% post-treatment, and 58.8% at follow-up. The within-group analysis of changes in the percentage of participants who reported working across the 3-time points (O1, O2, O3) was not statistically significant in either group: CCT (Cochran’s Q = 2.556, P = .169) and TAU (Cochran’s Q = 2.800, P = .247). The results of within-group changes at O2 and O3 from O1 are as follows: at O2, the percentage of participants who reported working increased by 19.1% in CCT (P = .219) and by 5.9% in TAU (P = 1.000) from O1, but both increases did not reach statistical significance. At O3, the percentage of participants who reported working remained the same as O1 in CCT (P = .125) and increased non-significantly by 17.6% in TAU (P = .625) from O1.
Question 2: CCT and TAU group difference in changes in work status
CCT and TAU between-group difference in changes in work status reported across the 3-time points (O1, O2, O3) was not statistically significant (z = 1.938, P = .052). The group difference in work status reported from O1 to O2 was significant (z = 2.934, P = .003), but their difference in work status reported from O1 to O3 was not significant (z = 0.814, P = .418). Note that higher z scores indicate a better improvement in RC; this interpretation also applies to all reported results with z scores in all the analyses.
Question 3: Changes in recovery capital among working versus not-working participants for both CCT and TAU treatment groups
The working and not-working groups were created based on changes in work status from O1 to O2 (Table 3) and from O1 to O3 (Table 4). For example, the working group comprises those who reported working at O1 and continued working following treatment as well as those whose work status changed from not working to working after treatment, reflecting positive changes. A similar approach was used to create the not-working group, reflecting any negative changes.
Post-treatment (O1-O2) improved treatment outcomes with work status for combined TAU and CCT groups (N = 38).

Wilcoxon rank-sum test estimated change scores from baseline (O1) to 5 months post-treatment (O2).
P < .05.
Follow-up (O1-O3) improved treatment outcomes with work status for combined TAU and CCT groups (N = 38).
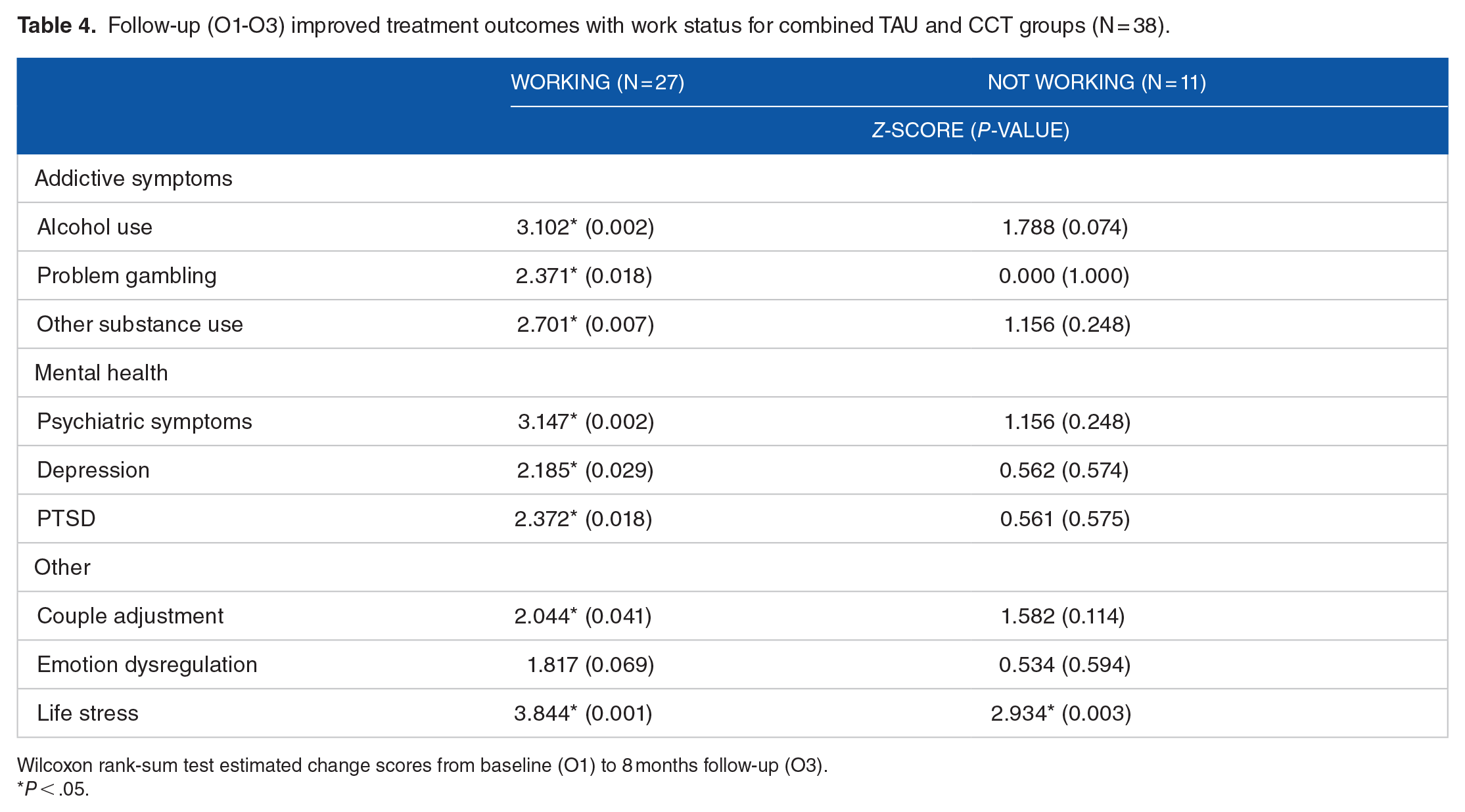
Wilcoxon rank-sum test estimated change scores from baseline (O1) to 8 months follow-up (O3).
P < .05.
At both O2 (Table 3) and O3 (Table 4), working group RC changes (all z-scores ⩾ 1.160) surpassed those of not-working group in alcohol use, problem gambling, other substance use, depression, psychiatric symptoms, emotion dysregulation, couple adjustment distress, and life stress (all z-scores ⩾ 0.001) based on the entire TAU and CCT sample. At O2, all RC improvements were statistically significant for those working except for problem gambling (P = .246), PTSD (P = .077), and emotion dysregulation (P = .100); only life stress improved significantly among those not-working at O2 (P = .003). At O3, all RCs except emotion dysregulation (P = .069) improved significantly among those working; again, only life stress was significantly improved among those not-working (P = .003).
Question 4: Changes in recovery capital in working versus not-working group for CCT and TAU groups separately
For TAU at O2, (Table 5), only life stress improved significantly in those working (z = 2.521, P = .012) and not-working (z = 2.666, P = .008). For TAU at O3 (Table 6), only substance use (z = 2.380, P = .017) improved significantly in those working, while those not-working improved significantly in depression (z = 2.207, P = .027), psychiatric symptoms (z = 2.366, P = .018), couple adjustment distress (z = 2.371, P = .018), and life stress (z = 2.366, P = .018).
Post-treatment (O1-O2) improved treatment outcomes by work status TAU versus CCT.
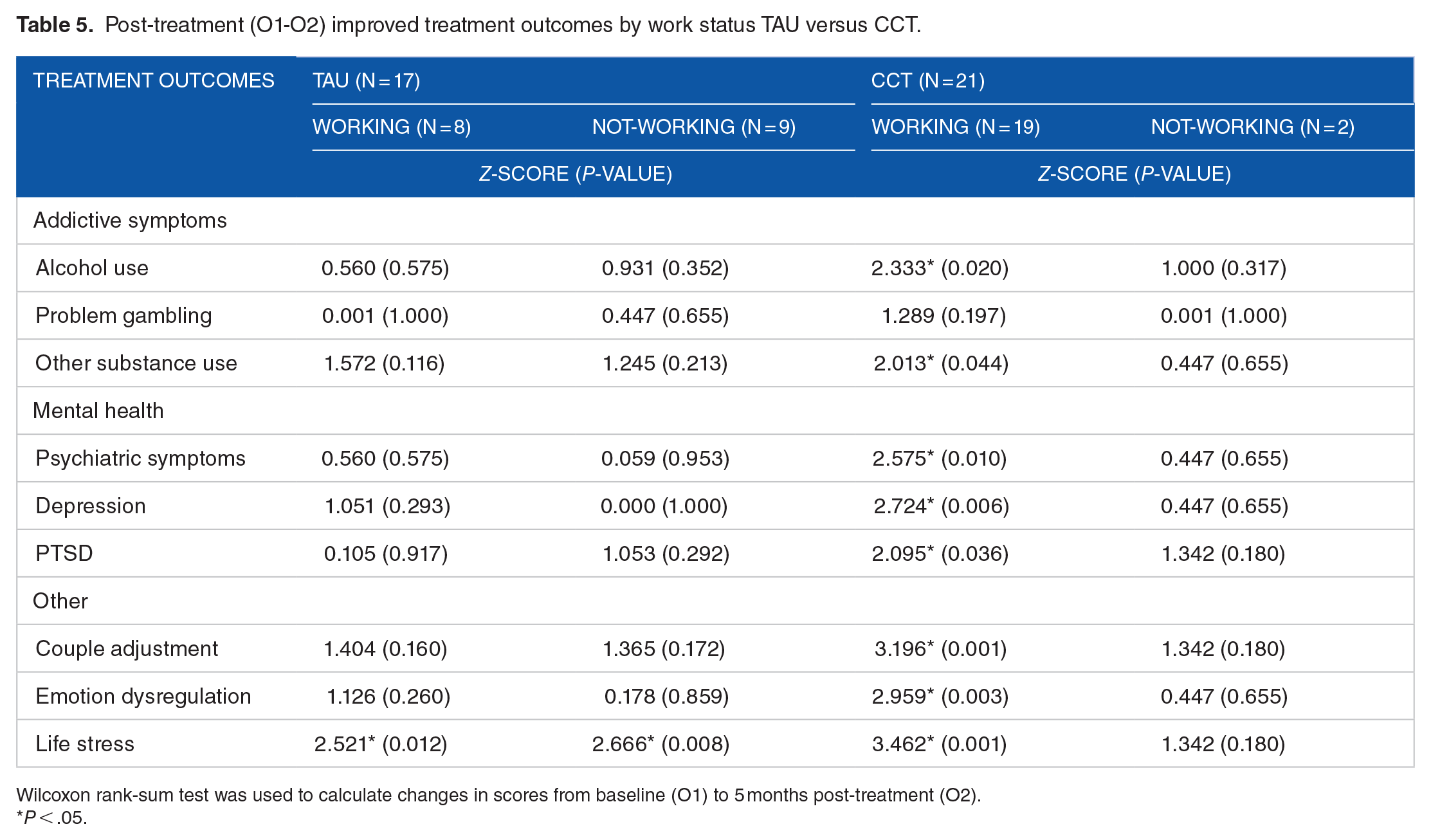
Wilcoxon rank-sum test was used to calculate changes in scores from baseline (O1) to 5 months post-treatment (O2).
P < .05.
In contrast, for CCT at O2, (Table 5), all RC areas improved significantly (all P < .05) for those working except for problem gambling with its small sample (n = 3) (P = .197). No RC area improved significantly for those not working (all P > .05). For CCT at O3 (Table 6), those working improved significantly in alcohol use (z = 2.158, P = .031), other substance use (z = 2.046 and P = .041), psychiatric symptoms (z = 2.783, P = .005), PTSD (z = 2.199, P = .028), and life stress (z = 3.351, P < .001). With CCT, those not working also showed significant improvement in alcohol use (z = 2.032, P = .042), depression (z = 2.014, P = 0.044), and life stress (z = 1.992, P = .046).
Follow-up (O1-O3) improved treatment outcomes by work status TAU versus CCT.

Wilcoxon rank-sum test was used to calculate changes in scores from baseline (O1) to 8 months follow-up (O3).
P < .05.
Power analysis
A G-Power analysis (based on Pearson r correlation test) with the sample of 38 using a 2-tailed alpha of .05 yielded a calculated power of 0.91. When the sample of N = 38 was split disproportionally between the working (n = 21) and not-working (n = 11) groups, the analysis was underpowered at 0.63.
Discussion
The concept of recovery capital broadens a view of recovery from abstinence to that of well-being in multiple areas that are important to overall functioning. In particular, employment, social and together with family support, mental health, and effective coping are considered important recovery assets.6,55 Improved functioning in these RC areas buffer stress and improve the quality of life during treatment recovery. 56 However, empirical evidence that supports the importance of this broader set of recovery capital and their relationship to each other is still limited. In this study, focusing on work status, we sought to determine whether those working made more improvement in addictive symptoms, couple adjustment, and other RC treatment outcomes compared to those not working. In addition to improved symptoms in alcohol and other substance use, the working group indicated more numerous and more significant changes in couple adjustment, depression and psychiatric symptoms, and life stress at post-treatment and follow-up. Majority of these improvements were significant and consistent in the CCT treatment group with its systemic interventions relative to the individually-based TAU group but these results need to be taken tentatively and cannot be generalized because of the small split samples. As a systemic model, CCT works on self and other awareness, couple communication, interrupting dysfunctional intergenerational patterns from adverse childhood experiences, and fostering higher self-worth. In doing so, it holds the potential to elevate concomitant outcomes in a positive direction that could spill over from couple adjustment and related RC into the work domain as suggested by findings from a parallel qualitative study that offered corroboration with the results of the present quantitative study. 34
Association between work status and RC domains
Positively significant changes in all RC areas were found in the working group but were limited in the not-working group. One earlier study showed positive correlations of improved employment functioning with improvement in other life areas including alcohol and drug use, medical, family, social, legal, and psychiatric outcomes. 57 However, clinical observations from other studies also showed that treatment outcomes including abstinence, quality of life, health, coping, happiness, and social and family relationships often do not progress smoothly in clients during recovery.58,59 Manifestations of such symptomatic changes tend to be uneven and dynamic, varying from one person to another and over the course of time. Enhanced coping has been proposed as a core component to a conceptualization of RC 60 to be made a process goal in treatment and recovery. In this present study, improvement in addiction symptoms and other RC areas among those working suggests that employment is interwoven with addiction recovery and multiple changes in other areas of life. However, the sequence and mechanism of this relationship remain to be determined.
Various studies have emphasized employment assistance and training for those in substance use recovery,28,32 and employment problems persist even for those in post-recovery. 61 According to a recent systematic review on the effectiveness of employment interventions that target primarily employment skills for substance use disorder, the magnitude of the outcomes of employment-specific programs is small and the findings are inconsistent. 32 Findings in the present study suggest that employment programs would best benefit from targeting recovery areas of couple adjustment, emotion regulation, mental health, and addiction in combination with employment in an integrated approach rather than just working on employment alone as an adjunct or separate after-care program.
Work and couple satisfaction interface
The reciprocal nature of work-family interaction has been the subject of research in other disciplines since the early 21st century.35,62 However, this salient connection has not been explored or exploited in the realm of addiction recovery and treatment. A secondary qualitative study from the same CCT RCT drawing on CCT addiction counselors’ case notes revealed that employment problems featured in 88% of couples, negatively impacting addictive behaviors, couple distress, and well-being of partners and clients in a systemic fashion that are intricately related. 34 With CCT’s systemic intervention, interacting themes of increased awareness of self and one’s family of origin influences, congruent communication, and the enlisting of spousal support are conducive to reducing employment stress and enhancing employment functioning. 33
These qualitative findings converge with our quantitative findings in showing the inter-relatedness of work and couple adjustment as well as other recovery variables of emotion regulation, mental health, and life stress. Rather than viewing work and couple functioning as existing in separate compartments, these findings invite us to regard improvement or strain in either domain as a potential to enhance or tax the other domain, similar to that reported in the work-family interface literature.35,63 Hence innovative interventions that aim for simultaneously improvement of addiction symptoms, couple satisfaction, employment, and other RC domains in a concerted holistic fashion should be further explored and studied.
Supporting the recovery capital paradigm
To gain the adoption of the recovery capital paradigm and advance its promises, we require strong research evidence acceptable to all stakeholders both within treatment institutions and in community settings. 64 This study supports this agenda in demonstrating improvement in couple and mental health functioning alongside an index of employment outcome based on working days, thus adding to the empirical base of the inter-relationships among RCs.
Limitations and future directions
Several limitations accompany this study. Although the results of improvement of RCs for those working are adequately powered, the analyses comparing the split groups of TAU and CCT are under-powered. Therefore findings comparing TAU and CCT should be interpreted as exploratory requiring future replication with larger samples. Another limitation of this study is that we only used work status measured in number of working days in the past month as an index of employment. Future studies on employment would be strengthened with a greater number of employment variables such as new employment, length of employment/unemployment, earnings, job loss, and frequency of work-related conflict. In light of the many employment-related problems found among problem and pathological gamblers,65,66 an important contribution of the present study is that it extends the substance use literature on work and recovery capital to include those with gambling disorder, but the gambling sample is small. Replication of the findings of this study with a larger sample would allow the use of inferential analysis to differentiate the effects of a systemic versus individual-based intervention to map out more precise pathways of interactions among a multiple set of recovery capital with employment.
Footnotes
Acknowledgements
The authors would like to thank Dr. Kamrul Islam and Dr. Andrew Greenshaw for their consultation in the development of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The data reported in this manuscript are part of a larger randomized controlled trial on Congruence Couple Therapy versus Treatment-as-Usual funded by a major grant from the Alberta Gambling Research Institute (Grant No. 43 649), and sub-grants from CIHR Canadian Research Initiative in Substance Misuse (CRISM Prairie Node) and the Canadian Depression Research and Intervention Network, Regional Depression Research Hub.
Declaration of Conflicting Interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Bonnie Lee is the developer of Congruence Couple Therapy and has received fees for workshops conducted on this model.
Author contributions
Bonnie Lee and Samuel Ofori Dei both contributed to the conceptualization, analysis and writing of this article.