
Abstract
Background:
Cancer is the second leading cause of death in the United States. Lifestyle choices such as substance abuse can impact a survivor’s health and overall quality of life.
Methods:
We used longitudinal data from the Wave 1-3 Population Assessment of Tobacco and Health data to examine sociodemographic characteristics and substance use behaviors (current cigarette, e-cigarette, alcohol, and marijuana use) by cancer diagnosis status. A generalized estimating equation model was used to examine the population-averaged effects of sociodemographic factors on substance use.
Results:
Among 1527 participants diagnosed with cancer, 14.5% used cigarettes, 3.8% used e-cigarettes, 49.1% used alcohol, and 4.2% used marijuana in the prior 30 days in Wave 1. While the prevalence of cigarette use among those with no cancer history decreased significantly between Wave 1 (21.9%) and Wave 3 (20.2%), it increased significantly among participants diagnosed with cancer from 14.5% to 16.0%. E-cigarette use decreased for both groups, whereas alcohol and marijuana use increased. Results showed that substance use among people diagnosed with cancer significantly varied by sociodemographic characteristics. Age, sex, race-ethnicity, education, income, and region of residence were significantly associated with substance use among patients diagnosed with cancer.
Conclusion:
Overall, substance use is lower among participants diagnosed with cancer than those with no cancer history. Substance use varies by sociodemographic characteristics among people diagnosed with cancer. More focus on substance use prevention among patients diagnosed with cancer could be beneficial in terms of improving the overall well-being of this population.
Introduction
Cancer is the second leading cause of death in the United States. 1 In 2018, an estimated 609 640 U.S. residents died of cancer. 2 Each year in the United States, 1.7 million new cancer cases are diagnosed, with $147.3 billion in cancer expenditures. 2 However, the 5-year relative survival rate for all cancers has risen by more than 20% over the past 3 decades.2-4 As a result, the number of cancer survivors in the United States is expected to increase from 15.5 million in 2016 to 20.3 million by 2026. 2 Cancer survivors often face subsequent health challenges caused by cancer treatment or recurrence. Lifestyle choices, including substance abuse, can impact the health and overall quality of life of survivors. For instance, survivors of small-cell lung cancer who continue to smoke have an increased risk of developing a second lung cancer.5-7
Substance abuse can impact cancer prognosis, and exacerbates other health conditions, mental health, and overall quality of life. Several studies have found a positive association between continued cigarette smoking and risk of mortality among cancer patients.8-11 Research also indicates that cancer patients who smoke are at higher risk for emotional problems and poor mental health, as well as reduced physical quality of life.12,13 Though e-cigarettes (vapors) are commonly considered less harmful than cigarettes, some ingredients in these products are known to cause harm. 14 E-cigarette vapor has been found to contain nicotine, heavy metals, volatile organic compounds, and carcinogens. 14 Interestingly, a study by Charlet and Heinz reported improved mental health, physical function, and overall quality of life among participants with reduced alcohol intake. 18 Although some cancer patients use recreational marijuana to help mitigate cancer-related pain and nausea,15,16 marijuana use has been shown to have negative physical, mental, and cognitive health outcomes. 17
Several prior studies have estimated the prevalence of cancer survivors who use cigarettes, e-cigarettes, alcohol, and marijuana. Evidence from a study among 142 5-year disease-free survivors of non-small cell lung cancer (NSCL) indicated that 57.7% self-reported as current drinkers. 19 In 2013, about 5.1% and 8.3% of U.S. adult cancer survivors reported heavy and binge drinking, respectively, though both rates were significantly lower than their cancer-free counterparts. 20 Regarding cigarette use, Westmaas et al. 21 found that 9.3% were current smokers approximately 9 years after diagnosis, and smoking status was significantly associated with younger age, lower education and income, and greater alcohol consumption. Prior studies reported that after cancer diagnosis, smoking-related cancer survivors have a higher risk of continued cigarette smoking than non-smoking-related cancer survivors. 22 Likewise, another study found that the smoking rate was higher in young cancer survivors (age ⩽40) than in young individuals who had never been diagnosed with cancer. 23 Among samples of cancer patients who smoked cigarettes, about 6.5% to 19% reported current e-cigarette use.24,25 Moreover, a cross-sectional U.S. study among cancer patients at the Seattle Cancer Care Alliance found that 2.8% of those with a history of cancer reported current e-cigarette use, which was lower than among the general population. 26 For marijuana use, Pergam et al. 27 found that in a state where recreational marijuana use was legal, past-year and past-month prevalences were 24% and 21%, respectively.
There are limited studies on sociodemographic characteristics associated with substance use among cancer survivors. Previous studies have shown that education was significantly negatively associated with cigarette use among cancer survivors, as well as the general population.23,28,29 In addition, Asfar et al. and Emmons et al. found non-Hispanic white and low-income cancer survivors had higher odds of cigarette use.23,28 Evidence suggests that e-cigarette use was more prevalent among cancer survivors younger than 50 years. 30 Most prior studies of substance use among cancer survivors are focused on specific types of cancer (childhood cancer28,31,32 and lung cancer, 19 and retinoblastoma 29 ), with studies using small or non-generalizable samples.19,20,24,25,29,30 In this study, we assessed the prevalence of current cigarette, e-cigarette, alcohol, and marijuana use among adults with a history of cancer and those without a cancer history using nationally representative data. Additionally, this study examined the sociodemographic characteristics associated with substance use among patients diagnosed with cancer.
Methods
Data
The Population Assessment of Tobacco and Health (PATH) is a nationally representative longitudinal cohort study. It is the first large joint research effort administered by the National Institutes of Health (NIH) and the Food and Drug Administration’s (FDA’s) Center for Tobacco Products to assess tobacco use and how it impacts the health of civilians throughout the country. 33 The target demographic is the civilian household population at least 9 years of age in all 50 states and the District of Columbia. Active-duty members of the military and all persons living in institutional and non-institutional groups other than college dormitories were excluded. The survey assesses tobacco-use patterns, risk perceptions, and attitudes regarding harmful constituents, new and emerging tobacco products, as well as tobacco initiation, cessation, and relapse behaviors. PATH study used a 4-stage stratified area probability sample design in Wave 1, which included a stratified sample of geographical primary sampling units (PSUs), smaller geographical segments, residential addresses, and households. As part of the complex survey design, survey weight was designed to compensate for variable probabilities of selection, differential non-response rates, and possible deficiencies in the sampling frame and account for sampling design factors such as the stratification and sampling of PSUs and area segments, and the use of oversampling and non-response adjustment factors. Weights for the following waves were based on Wave 1 survey weights and further adjusted for non-response to interview questions in the previous survey. The first wave of the PATH study was conducted in 2013/2014, Wave 2 was conducted in 2014/2015, and Wave 3 was in 2015/2016. A total of 32 320 adults, 13 651 youth, and 13 588 parents of youth were interviewed. 33 All Wave 1 respondents were eligible to be interviewed in the later waves, as long as they were still living in the United States and were not incarcerated. This analysis included all 32320 adults at baseline, Wave 1, and those who turned 18 between Waves 2 and 3: 1915 participants for Wave 2 and 1907 participants for Wave 3. Additionally, participants who refused, did not know, or requested to remove the response to the cancer diagnosis question were treated as missing.
Measures
The dependent variables were 4 substance use behaviors: cigarettes, e-cigarettes, alcohol, and marijuana. Four dichotomized variables were created to measure the current use of each substance use behavior at each wave independently. The current use of cigarettes and e-cigarettes was defined as adult respondents who had ever used those tobacco products and had used some days or every day at the time of the survey. Current alcohol use was defined as adult respondents who used alcohol within the past 30 days of the survey. It was assessed by the question: “How long since you last used alcohol,” which was addressed to those who had ever used alcohol. The possible responses were “Within the past 30 days,” “More than 30 days, but within the past year,” and “More than a year ago” in Wave 1. Respondents in Waves 2 and 3 were asked: “Have you used alcohol within the past 30 days?” with the possible responses of “Yes” or “No.” Respondents who had never used alcohol were grouped with those who did not use alcohol in the past 30 days. Similar questions were used to define current marijuana use.
The main independent variable of interest was cancer diagnosis at each wave. The cancer diagnosis was assessed by the survey question, “Have you ever been told by a doctor, nurse or other health professionals that you had cancer” for the Wave 1 adults and aged-up adults at Waves 2 and 3 (who were younger than 18 years old at previous wave). In addition, adults who were successfully followed up with in Wave 2 and Wave 3 were asked, “In the past 12 months, have you been told by a doctor, nurse, or other health professionals that you had cancer?” Respondents without cancer history in previous waves but that responded “Yes” to the cancer diagnosis question in the current wave were reclassified as respondents with cancer history during the follow up wave.
The following demographic characteristics were included in the analysis: age (18-34, 35-54, and 55 years old or older), sex (male or female), race/ethnicity (non-Hispanic white, non-Hispanic black, Hispanic, or non-Hispanic other races), poverty status (<100% of poverty guideline, 100%-199% of poverty guideline, and ⩾200% of poverty guideline), education level (less than high school, high school graduate or equivalent, some college [no degree] or associate degree, bachelor’s degree, or advanced degree), residential region (Northeast, Midwest, South, West), and other tobacco product use (“Yes” or “No”). The poverty income guideline was based on the 2015 poverty guidelines for the 48 contiguous states and the District of Columbia. It was calculated by multiplying $4160 by the number of people in the household and adding $7610 to the total. Other tobacco product use was defined as adult respondents who had ever used tobacco products and used some days or every day at the time of the survey, with other tobacco products including dissolvable tobacco, filtered cigars, cigarillos, traditional cigars, hookah, pipes, smokeless tobacco, and snus. Other tobacco product use was assessed at each wave, while other demographic characteristics were collected at baseline.
Statistical analysis
Wave 1 sociodemographic characteristics and substance use behaviors were calculated by cancer diagnosis status (participants with cancer history vs no cancer history). The weighted frequency and 95% confidence interval (CI) were reported for all categorical variables, and Chi-square tests were used to compare characteristics between participants with and without a history of cancer. Prevalence was estimated for each substance use behavior (cigarette, e-cigarette, alcohol, and marijuana) for participants with and without a history of cancer in each wave independently. Single-wave sampling weights were included in estimating the prevalence to increase estimate stability and account for complex survey design. 33 Pearson Chi-square tests were used in examining the change in prevalence and the difference between participants with and without a history of cancer. Stratified analyses were conducted in male and female subgroups.
To examine the population-averaged (marginal) effects of socioeconomic and demographic characteristics on the risk of substance use among participants diagnosed with cancer, generalized estimating equation (GEE) models were used for each substance use behaviors (cigarettes, e-cigarettes, alcohol, and marijuana) independently. We used the GEE framework because the population-averaged response for the specific behavior “is directly estimable from observations without assumptions about the heterogeneity across individuals in the parameters.” 34 All models adjusted for time-invariant covariance, including age, sex, race, poverty status, education level, residential region, and time-variant variables, including other tobacco product use, and survey wave (time). GEE models were estimated by SAS Genmod procedure and used the exchangeable covariance structure. All tests were 2-sided, and a P-value <.05 was considered significant. All analyses were conducted using SAS 9.4 (SAS Institute, Inc. Cary, NC) or R 3.5.
Results
Table 1 presents the sociodemographic characteristics and substance use behaviors among participants with and without a history of cancer at Wave 1. Among 32 320 participants, about 47.8% were between 18 and 34 years old, 50% were male, approximately 60.6% were non-Hispanic white, and 21.2% had at least a bachelor’s degree. Sample demographic characteristics differed significantly between participants with cancer history and participants without a history of cancer. Participants diagnosed with cancer tended to be older, female, non-Hispanic white, and have a family income at, above, or twice the poverty level.
Sample demographic, socioeconomic characteristics, and substance use by cancer diagnosis from Wave 1 (2013/2014) of the PATH study.
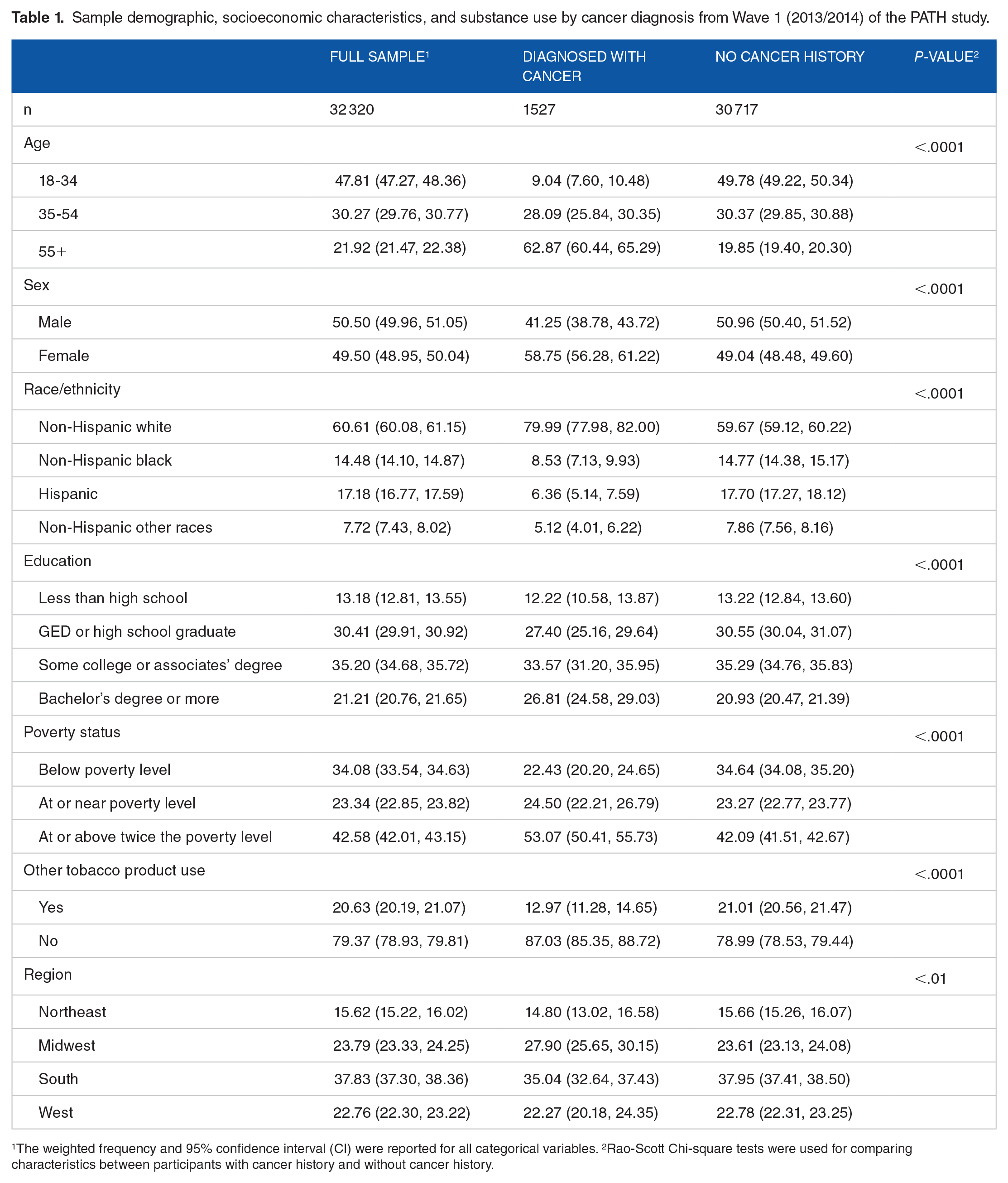
1The weighted frequency and 95% confidence interval (CI) were reported for all categorical variables. 2Rao-Scott Chi-square tests were used for comparing characteristics between participants with cancer history and without cancer history.
Table 2 presents the association between sociodemographic characteristics and substance use behaviors among PATH study participants diagnosed with cancer from Wave 1 to Wave 3 from the GEE models. Participants diagnosed with cancer who were Hispanic (Figure 1; aOR: 0.58, 95% CI: 0.37-0.92), those with higher education (Figure 1; GED or high school graduate: aOR: 0.53, 95% CI: 0.37-0.75; some college or associate degree: aOR: 0.39, 95% CI: 0.28-0.56; bachelor’s degree or more: aOR: 0.13, 95% CI: 0.08-0.20) and had a higher income (at or near poverty level: aOR: 0.60, 95% CI: 0.45-0.81; at or above twice the poverty level: aOR: 0.33, 95% CI, 0.24-0.44) had lower odds of current cigarette use compared to the reference categories. For e-cigarette use, male participants diagnosed with cancer (Figure 1; aOR: 0.43, 95% CI: 0.30-0.61), non-Hispanic black (Figure 1; aOR: 0.35, 95% CI, 0.19-0.65), and those with at least bachelor’s degree (aOR: 0.48, 95% CI: 0.24-0.95) had significantly lower odds of current e-cigarette use compared to male participants without a cancer history in the corresponding reference groups. For alcohol use, significantly higher odds were found among participants diagnosed with cancer who were younger than those who were 55 years of age or older (Figure 1), had at least a bachelor’s degree, and had a family income at or above the poverty level (Figure 1). Hispanic and non-Hispanic other race participants diagnosed with cancer had lower odds of alcohol use (Figure 1). Similar results were found for marijuana use, with younger participants diagnosed with cancer having significantly higher odds of marijuana use (Figure 1). Participants diagnosed with cancer with a family income at or above twice the poverty level (Figure 1; aOR: 0.37, 95% CI: 0.24-0.59) had significantly lower odds of marijuana use.
The association of demographic characteristics and substance use behaviors among participants diagnosed with cancer from Wave 1 (2013/2014) to Wave 3 (2015/2016) of the PATH study.

Four generalized estimating equation (GEE) models were used to estimate the marginal effects of demographic characteristics on each substance use behavior independently. Significance (p<0.05) and odds ratios (95% confidence interval (CI)) are presented in

The association between demographic characteristics and substance use behaviors among participants diagnosed with cancer from Wave 1 (2013/2014) to Wave 3 (2015/2016) of the PATH study.
The prevalence of substance use among participants with and without a cancer history is presented in Figure 2. Over the 3 waves, the prevalence of cigarette use among participants with no history of cancer decreased from 21.9% to 20.2%, decreasing among both males (from 25.5% to 22.9%) and females (from 18.5% to 17.6%). However, among participants diagnosed with cancer, prevalence increased overall (from 14.5% to 16.0%) and among males as well (from 12.8% to 16.2%). The prevalence of e-cigarette use overall and among females showed a decreasing pattern. Among male participants diagnosed with cancer, the prevalence increased between Wave 1 (2.1%) and Wave 2 (3.2%), followed by a decrease between Wave 2 and 3 (2.3%). An increase from Wave 1 to Wave 3 was found for alcohol use among most subgroups. Though, among female participants diagnosed with cancer, the prevalence decreased from 47.9% in Wave 1 to 46.9% in Wave 3. Across the study period, the prevalence of marijuana use increased from 4.2% to 4.8% among participants with a history of cancer, and from 7.4% to 9.9% among participants with no history of cancer. The increasing trend was consistent among male and female participants with no history of cancer and male participants diagnosed with cancer. Among female participants diagnosed with cancer, the prevalence of marijuana use decreased from 5.2% in Wave 1 to 4.0% in Wave 3.

Prevalence of substance use among participants with and without cancer history from Wave 1 (2013/2014) to Wave 3 (2015/2016) of the PATH study, stratified by sex.
Discussion
Cigarettes
The current study assessed the prevalence of current cigarette, e-cigarette, alcohol, and marijuana use among adults with a history of cancer versus those without a history of cancer. We also examined sociodemographic characteristics associated with substance use among participants diagnosed with cancer. Cigarette smoking was less prevalent among participants with cancer history than those without but increased over time. Similarly, Emmons et al. and Carswell et al. found that cancer survivors were less likely to smoke cigarettes compared to control groups. However, Asfar et al. 28 reported that survivors initiated smoking earlier and had higher odds of smoking more than controls. These studies found that cancer survivors are less likely to smoke, but smoke more than those without a history of cancer. From Wave 1 to Wave 3, the prevalence of cigarette use decreased among participants with no cancer history but increased among those with a cancer history. A national trend analysis of adult survivors of childhood cancer from 1997 to 2010 found that the prevalence of cigarette use gradually declined among those without a cancer history. 28 The prevalence of cigarette use among cancer survivors was not consistent across study periods. 28 Asfar et al. 28 suggest that cancer survivors are more sensitive to cigarette price changes, which may have influenced the differences in temporal trends of smoking prevalence between the two groups. In addition, some cancer survivors may quit smoking at diagnosis following a doctor’s advice only to have relapsed later. The National Comprehensive Cancer Network published (NCCN) Guidelines for Smoking Cessation recommends including smoking cessation as part of the treatment plans for all smokers with cancer. 35
Consistent with the general population, we found lower socioeconomic status was associated with higher odds of smoking. Specifically, we found that participants diagnosed with cancer with more education were less likely to be current cigarette users compared to those with less than a high school education. This finding agrees with prior studies, which reported that cancer survivors with less education were more likely to use cigarettes than those with more education.28,29,31 Participants diagnosed with cancer in the current study with an income at or above the poverty level were less likely to be current cigarette users. Two prior studies also reported that survivors from low-income households were more likely to use cigarettes.28,31 In addition, our findings showed that Hispanic participants diagnosed with cancer had lower odds of current cigarette use than non-Hispanic white participants, which is consistent with prior studies.28,31
E-cigarettes
Participants diagnosed with cancer had a lower prevalence of current e-cigarette use than those without a history of cancer, with findings showing a decreasing pattern between Wave 1 and Wave 3. A prior study reported a lower prevalence of e-cigarette use among those with a history of cancer than among the general population. 26 Non-Hispanic black participants diagnosed with cancer were significantly less likely to be current e-cigarettes users compared to non-Hispanic whites. In a 2014/2015 study among the general U.S. population, black persons had lower odds of ever, current, and regular e-cigarette use, compared to white persons, indicating that our finding reflects a larger trend. 36 Consistent with the social gradient in substance use, our findings showed that participants diagnosed with cancer who had at least a bachelor’s degree were less likely to be current e-cigarette users compared to those with less than a high school education. In terms of sex differences, male participants diagnosed with cancer were less likely to use an e-cigarette. Similarly, Kalkhoran et al. 25 reported that among current smokers with a recent cancer diagnosis, current e-cigarette users were more likely to be female than never e-cigarette users.
Quitting cigarettes was the most commonly stated reason for using e-cigarettes in a study of current smokers with a recent cancer diagnosis. 25 From a harm reduction perspective, e-cigarettes may be beneficial for cancer survivors to the extent they can switch from combustible cigarettes to e-cigarettes. However, dual-users of both cigarettes and e-cigarettes may have higher difficulty quitting and more nicotine dependence. 24 In a study among head and neck cancer patients who wanted to quit smoking, those who used e-cigarettes to reduce cigarette use were less likely to quit smoking than those who stopped smoking cold turkey. 37 The study also found that e-cigarette users did not decrease the number of cigarettes smoked compared to cigarette-only smokers. 37
Alcohol
The current study found that participants diagnosed with cancer who had a lower prevalence of alcohol use than those with no cancer history. A prior cross-sectional study found that cancer survivors were less likely to binge drink.19,20 Overall, alcohol use increased in our study from Wave 1 to Wave 3. In terms of race/ethnicity, Hispanic and non-Hispanic other race were less likely to use alcohol compared to non-hispanic white participants diagnosed with cancer. These findings align with previous studies that Hispanics and those in the other race category have a lower prevalence of binge drinking than those who are non-Hispanic white in the general U.S. population. 38 Contrary to cigarette, e-cigarette, and marijuana use, cancer survivors who had at least a bachelor’s degree and higher income were more likely to drink alcohol. Cremeens et al. 38 suggest that alcohol has a different association with sociodemographic status because drinking has not been as widely recognized as risky and may not carry the same social stigma as other substances.
Marijuana
The prevalence of marijuana use was higher among those with no cancer history than those with a cancer history in the present study. Over the study period, the prevalence of marijuana use increased among all groups except for female participants diagnosed with cancer. A previous study using the 2016 and 2017 Behavioral Risk Factor Surveillance System found adults with medical conditions had higher odds of reporting current marijuana use than those without medical conditions. 39 However, our results align with their findings on the inverse association between age and current marijuana use. 39 Additionally, though outside of the scope of our study, it remains unclear how the changing marijuana policy environment may impact use among cancer survivors. Pergam et al. 27 found that marijuana legalization significantly increased the likelihood of use in more than half of the participating patients with cancer.
The results of this study should be interpreted considering its limitations. Our analyses were limited to variables that were included in each wave of the PATH interviews. Another limitation of this study is that the interviews rely on self-reported substance use without biological confirmation of substance use. We could not differentiate between those currently receiving cancer treatment and those in remission for our definition of a cancer diagnosis. Additionally, the results may not be generalizable to individuals who are institutionalized or active members of the military. It is also important to note that we could not determine the effect of time since cancer diagnosis and cancer type on substance use behaviors and reasons behind these behavioral changes and their proximity to the cancer diagnosis. For example, the effect of cancer diagnosis could differ significantly for participants diagnosed with cancer, and participants who had childhood cancer. Despite these limitations, the current study documents the prevalence and potential trends in substance use among those diagnosed with cancer.
Conclusion
Overall, substance use was lower among people diagnosed with cancer than those with no cancer history. However, female participants diagnosed with cancer had a higher prevalence of e-cigarette use than those with no cancer history. Among people diagnosed with cancer, substance use varied by sociodemographic characteristics and use was more prevalent among those who were younger and of lower socioeconomic status. Hence, more focus on substance use prevention among people diagnosed with cancer could be beneficial in terms of improving the overall well-being of this population.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors made substantive contributions to the manuscript.