
Abstract
Sleep problems are common among children and adolescents. Sleep quality plays a significant role in their mental health. We aimed to determine the prevalence of poor sleep quality (PSQ) among secondary school students, identify sociodemographic factors associated with PSQ in this group, and examine the independent associations of psychological distress, stimulant use, and internet use with PSQ. Data were collected from 420 secondary school students from four different schools who were selected using a mixture of convenience and random sampling. A set of questionnaires was administered to collect data, and it consisted of 5 sections measuring: the sociodemographic, drug use, psychological distress, internet use, and sleep quality. A total of 378 questionnaires were analyzed. The participants comprised 174 (46.2%) males and 203 (53.8%) females who were between 10 and 21 years. The mean age was 14.78 years. The prevalence of those who had PSQ was 12.2%. A logistic regression model showed that anxiety (AOR = 1.20, 95% CI: 1.10-1.32), depression (AOR = 1.12, 95% CI: 1.00-1.25), and internet use (AOR = 1.02, 95% CI: 1.00-1.03) were significantly associated with PSQ. PSQ commonly exists among students and has a relationship with their psychological state and potentially addictive behavior, such as internet use. We prescribed the optimal treatment of psychological disorders and addictive behavior, of which sleep problems are a typical fallout.
Background
The National Sleep Foundation described good sleep quality as total sleep time of 85% or more of the total time in bed, commencing sleep not later than half an hour while attempting sleep, waking up not more than once during the night and being able to recommence sleep within 15 minutes of an initial awakening across all age groups. 1 While sleep quantity (number of hours of sleep during the night) is an essential determinant of how “good sleep” could be defined, sleep quality is a more important determinant of optimal sleep as the range of sleep quantity varies widely from one individual to the other. 2
Sleep problems are common among children and adolescents in Nigeria,3,4 and beyond,5-7 and they are associated with physical and mental health indices. For example, while poor sleep quality is associated with obesity, impaired blood lipids in adolescents, 8 reduced learning capacity, and academic performance, 9 it is associated with psychological symptoms such as depression, anxiety disorders, and behavioral disorders in studies among adolescents.9-11 Nonetheless, the relationship between sleep dimensions and psychological disorders could be non-linear, especially when the sleep duration is considered. 12
The association between sleep problems and drug use is also important to mention. Drug use has varying effects on sleep, depending on the type, amount, and stage of use. The association between sleep quality and stimulating drugs has been established, though it remains complex. 13 Stimulants such as methylphenidate have been shown to improve both quantity and quality of sleep in a population of individuals with attention deficit hyperactivity disorder, but this finding is not so among those without the disorder.14,15 Another survey involving 166 participants revealed that dependence on stimulants such as caffeine and nicotine was associated with poor quality of sleep and increased psychological distress. 16
Sleep problems have also been associated with internet use, another potentially addictive behavior among adolescents and young adults.7,17 It was observed in a study of 1212 adolescents, using the Young Internet Addiction Scale, that the participants who had higher scores reported more problematic sleep habits and sleep problems. 18
In Nigeria, the relationship of sleep quality with these domains of interest: psychological distress, stimulant use, and internet use have not been adequately studied, even though there are some reports on the prevalence of poor sleep quality (PSQ) among children and adolescents.3,4,19 Undoubtedly, there is growing evidence that the rate of drug (stimulant) use is increasing among adolescents in Nigeria 20 who use stimulants to stay alert and fend off sleep. 21 Similarly, the number of internet users and abusers among adolescents in Nigeria has continued to rise, 22 and the figure of adolescents suffering from psychological problems has equally increased. 23 In a locale where data is grossly insufficient, it is apt to fill in gaps in information by conducting studies of this nature, which may be useful for other researchers, clinicians, and policymakers. With the increasing concern about students’ mental health in recent years, it is, therefore, necessary to update the prevalence of PSQ among secondary school students, identify sociodemographic factors associated with it in this group, and to examine the independent associations of psychological distress, stimulant use, and internet use with PSQ. We thus hypothesize based on the literature from other climes, that there will be an independent relationship of PSQ with stimulant use, psychological distress, and problematic internet use.
Methods
Study location and population
This cross-sectional study was carried out in Benin City, which is the capital city of Edo State, located in the South-South geopolitical zone of Nigeria. The city is the residence of diverse ethnic groups, and it has a population of more than a million persons. Within the city are schools either owned by the government (public) or individuals (private). The privately-owned schools obtain approval from the government to operate, and they far outnumber the public schools. In Nigeria, the educational system is divided into three major stages. The stages include primary education, which lasts for six years, the secondary or post-primary, which also lasts for six years and the tertiary with a minimum of four years, depending on the field of study. The secondary or post-primary school education is divided into junior and senior, and each is a three-year program. The study population consisted of students from both junior and senior secondary schools.
Procedure
Before the collection of data, approval was obtained from the research and ethics department, Edo State Ministry of Education (STT1465T/188), and the authorities of the schools involved. Written informed consent was obtained from the participants and their parents if below the age of 18 years. Only the students who gave consent or assent were selected.
A total of 420 questionnaires were distributed even though a sample size of 195 was calculated using a Nigerian study in which 15.5% of children and adolescents had sleep problems. 19 Sampling was based on convenience; four gender-mixed schools were picked from the numerous schools in the city. The selection was purposefully made to include two schools each from the public (government-owned) and privately owned schools. Students were thereafter randomly selected from both the junior and senior secondary levels from the chosen schools.
Two graduates’ research assistants who were adequately trained were employed for the collection of data. The training entailed understanding the content of the questionnaire enough to assist the students when necessary. The training lasted for 90 minutes, during which the queries they had were resolved, and possible concerns that students could raise were addressed. The administration of the questionnaire was done in the classroom, mostly during the break period. Data were collected between January 22 and February 2, 2018.
Measures
A set of questionnaires consisting of 5 sections was used to collect data, and all were designed in the English language, which is the official language of instruction at this stage of education.
Socio-demography
The first section, which is the sociodemographic characteristics, was used to collect information such as the gender (male or female), age (in years), family structure (polygamous or monogamous), school type (public or private), religion (Christianity or others), ethnicity (Bini which is the dominant ethnic group or others), parental figure (single parent, both parents, or guardian), and academic performance (above average, average or below) of the students. It was purposefully designed and structured to meet the objectives of the study.
Sleep quality
The Sleep Quality Questionnaire (SQQ) 24 was used to assess sleep quality in the participants. It is a 9-item scale that is scored on a 5-point scale from 0 to 4 and added together. Possible scores range from 0 to 27; the lower the score, the more severe the sleep problem, while high scores indicate better sleep quality. A score of 18 and below is highly suggestive of problems with sleep using SQQ, and this was adopted as the cut-off in this study. The scale has a strong correlation (r = 0.925) with another sleep scale, the Sleep Condition Indicator, which has been validated and found to have good psychometric properties. 24 The reliability score of the SQQ in the current study was 0.71.
Internet addiction
The Internet Addiction Test 25 is a 20-item scale that assesses the general pattern of internet use and its impact on the respondent’s life at work, school, home, and social. Responses are made on a 6-point Likert measure (0-5); thus, the possible score ranges between 0 and 100. A score of 50 and above indicates a potential internet addiction, which was chosen in this study. 26 It has been widely used among students, and the scale recorded a Cronbach alpha of 0.93 in the current study.
Psychological distress
The Hospital Anxiety Depression Scale (HADS) 27 was used to screen for the presence of anxiety and depression in the participants. HADS can be used in clinical and non-clinical populations, and it consists of seven depression and anxiety items. It has been validated for use in Nigeria. 28 A higher score on each scale indicates higher psychological distress. A cut-off point of eight and above on either of the two components is regarded as a probable case diagnosis.
Drug use
The World Health Organization Questionnaire for Student Drug Use Surveys was developed from different parts of the world, including Nigeria. 29 For this research, only the tobacco and caffeine sections of the instrument were used to obtain information on the commonly used stimulants. Respondents were required to indicate whether they had used them in the past 30 days (current use) and the frequency of use within this period. The instrument has been used in different cultures and countries, including Nigeria.
Data analyzes
Data collected were analyzed using the Statistical Package for Social Sciences (SPSS), version 22 (IBM Corporation, Armonk NY, USA) for Windows. Uni-variate analysis, such as frequencies, was determined and displayed in tables. Some variables, such as religion, current stimulant use, were dichotomized to enable a sufficient number of participants for analysis. Cut-off points were utilized to determine the prevalence of cases of depression, anxiety, problematic internet use, and PSQ. However, the continuous scores of some of these variables were employed in further bivariate and multivariates analyzes.
The Chi-square tests were used to determine the association between sleep quality and categorical variables such as gender, family structure, school type, academic performance, current use of stimulants (caffeine and cigarette). The sleep quality score was tested for normality using the one-sample Kolmogorov-Smirnov tests and was found to be non-normally distributed. Hence, the non-parametric Mann-Whitney U (MWU) test was applied to examine the differences in the rank mean scores of age, depression, anxiety, and internet use between the normal and poor group of sleep qualities. Variables such as current tobacco use, internet use, depression, and anxiety, which were significant on bivariates analyzes were included in a logistic regression model. A P-value of less than .05 was accepted as the level of statistical significance.
Results
Sociodemographic characteristics
A total of 378 (90%) out of the 420 questionnaires distributed were analyzed. The remaining questionnaires were discarded because of inconsistent responses or unfilled data. The participants comprised of 174 (46.2%) male and 203 (53.8%) female students. Age ranged between 10 and 21 years with a mean and median of 14.78 and 15.00 years, respectively. The sample included 189 students from the public schools, while 183 (49.2%) were from private. Other characteristics of the participants are summarized in Table 1.
Participants’ characteristics.

Missing data.
Prevalence of PSQ and associated variables
The prevalence of those with PSQ was 12.2%, and those with problematic internet use measured 23.3%. Current uses of caffeine and tobacco were 39.4% and 6.1%, respectively. One hundred and twelve (29.6%) and 48.4% of the participants scored respectively above the cut-off point for the Hospital Anxiety and Depression Scale to merit cases of depression and anxiety.
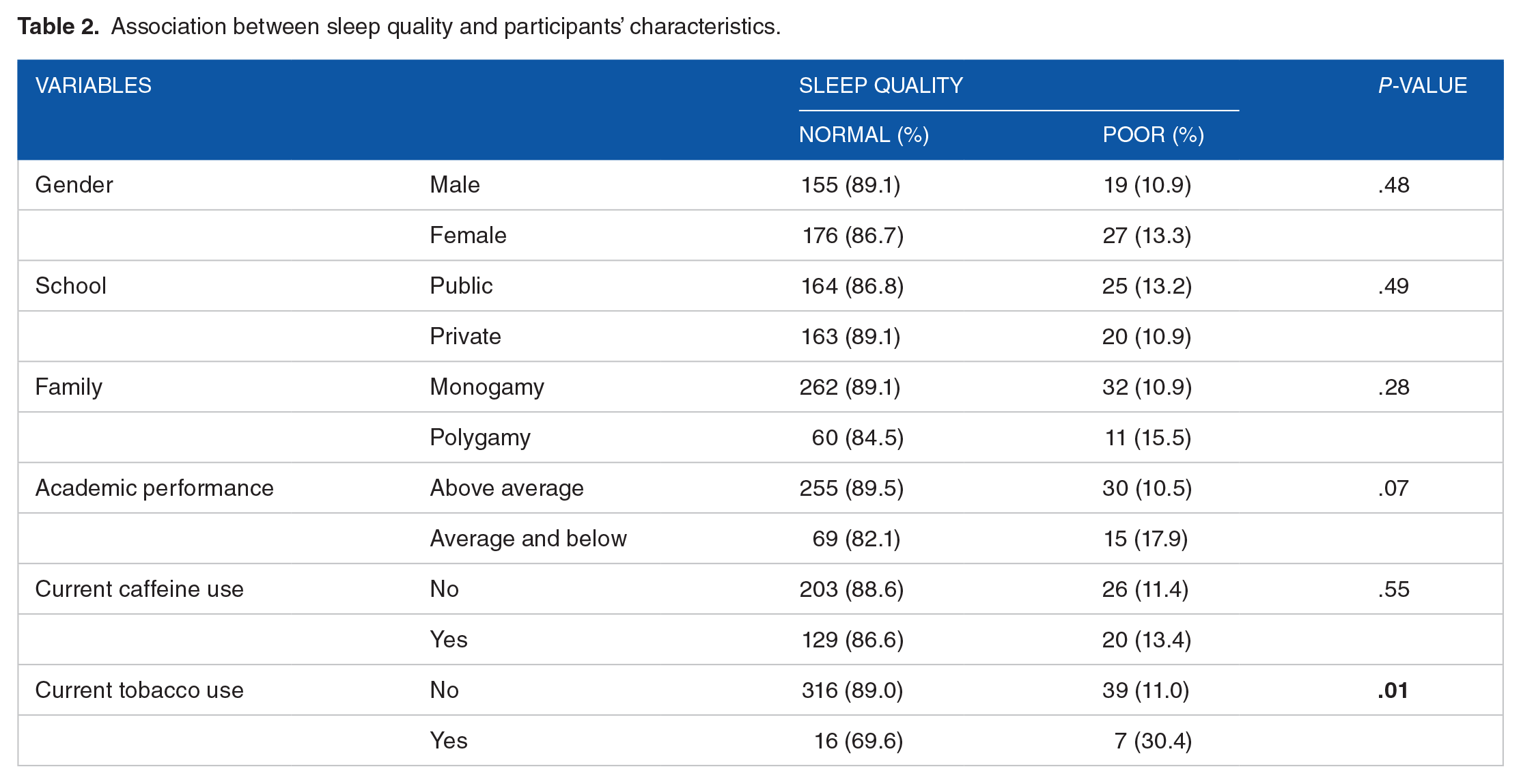
There was a significant association between PSQ and current tobacco use (X2 = 7.64, P = .01) (Table 2). Furthermore, participants with PSQ had significantly higher scores on anxiety scale (MWU = 4417.50, P = .00), depression scale (MWU = 5305.00, P = .00), and internet use (MWU = 5918.50, P = .01) when compared with those without sleep problems (Table 3).
Association between sleep quality and participants’ characteristics.
Relationships of age, anxiety, depression and internet use, with sleep quality.

Note: normal (n = 332), poor use (n = 46), MWU, Man-Whitney U.
A binary logistic regression of the current use of tobacco, internet use, depression, and anxiety was carried out on PSQ. The result showed that anxiety, depression, and internet use were significantly associated with PSQ (Table 4).
Logistic regression of tobacco use, internet use, depression and anxiety on sleep quality.

Discussion
We investigated the prevalence of PSQ and its interaction with some identified risk factors, including sociodemographics and clinical correlates. Our findings revealed that 12.2% of the participants rated themselves to have PSQ. Evidence from previous studies among adolescents, such as in the USA, 5 Taiwan, 7 Turkey, 30 and Nigeria,3,4 revealed higher rates than the current report, while a study from India recorded a lower prevalence. 31 The disparity in rates may be related to the differences in research tools utilized to assess sleep quality, the definition of terms, and, most notably, the participants’ age. For example, while the mean age of the participant in the current study is lower than those from the USA, 5 Taiwan, 7 Turkey, 30 and Nigeria,3,4 it is slightly higher than the study from India. 31
An earlier study has reported a different rate of sleep-related problems at different stages of adolescent development, with a lower rate at the early adolescence compared to late adolescence. 4 While the ranked mean age of those who reported poor quality of sleep in the present study was higher than those who did not, the difference was not statistically significant. This is similar to the report by Şimşek and Tekgül, 30 who examined the effect of age on sleep quality, even though they applied a different screening tool in their study. The effect of the biological changes that accompanies aging has been acknowledged and said to account for the changes in sleep pattern in adolescents. Notwithstanding, evidence pointing to the role of environmental elements, especially the modern-day technology, and those of the psychological disorders, is now evolving.7,30 Some authors have linked the reduced need for sleep and an increasing adolescent stage with increasing school and social demands.31,32 Hence, the lack of association of age with sleep quality may simply suggest that environmental and psychosocial factors that are related to maturity are more likely to account for the increasing rate of poor sleep in older age groups rather than the effect of biological development. When we explored the association between PSQ and potential social and environmental factors in our sample using chi-square tests, four factors emerged. These include the current use of tobacco, internet use, depression, and anxiety disorders.
Tobacco use has been shown to reduce the quality of sleep,33,34 and high levels of withdrawal, and craving, have also been associated with PSQ. 34 The present study revealed an association between tobacco use and PSQ. However, when we included this variable in the logistic regression model, the association fizzled out. This suggests that some mediatory factors which explain the association between the two domains exist. Whilst it is necessary to further explore the relationship between tobacco use and sleep quality in a carefully selected sample, smokers should be well informed on the possible implication of smoking on sleep quality.
The rates of anxiety and depression among our participants are very high, as other reports from studies conducted among adolescents elsewhere.23,35 Our study also revealed that the participants’ sleep quality was significantly associated with these health conditions, as in other studies.10,11 The composite relationship between sleep and psychological disorder, such as anxiety and depression in adolescents, has attracted much attention over time.10,36 Although there has been mixed evidence regarding the bidirectional relationship between sleep and anxiety disorder, 10 evidence supporting early sleep problems as a precursor to anxiety in adolescence is receiving a lot of attention.37-39 Regulation of mood and emotion is contingent on adequate sleep. This is because the key neural regions and circuitry involved in emotional processing and regulation are highly active during sleep than during wakefulness. 40 In an experiment where adolescents were subjected to a mild sleep restriction protocol of 6.5 hours in bed per night for five consecutive nights, the participants were more irritable, oppositional, tense, and prone to emotional outbursts than those with healthy sleep duration plan. 41 Furthermore, a gradual sleep extension in adolescents experiencing a chronic reduced sleep duration was reported to significantly reduce depressive symptom severity in these individuals. 42 Therefore, early identification of sleep problems and effective interventions may be potential preventive measures for psychological disorders later in life. Conversely in the relationship, poor sleep is one of the common symptoms of psychological disorders such as anxiety, depressive, and psychotic disorders. 43 Improved sleep quality is one of the earliest signs of remission of most psychological disorders, while poor quality of sleep is an early feature of relapse. 43
Our logistic model revealed a strong influence of internet use on sleep quality, as reported in previous studies.7,17 Internet access has contributed significantly to African growth in terms of economic and health promotion, but its excessive use has been associated with unwanted health outcomes, mainly psychological, and most notably, in the youth. The scientific explanations behind the link between internet use and poor sleep are poorly understood, and the details are beyond the scope of this study. However, one study has implicated the stimulating effect of the central nervous system, through participating in internet games and mind activating program at bedtime, on prolonged sleep latency. 44 Another possible theory is the suppressing effect of the blue light emission on the secretion of melatonin from the pineal gland, which comes from internet-enabled devices, and may prolong sleep latency. 45 Alternatively, adolescents with sleeping difficulty may use the internet to engage themselves or cope with this problem rather than seeking professional help until they develop a medical or psychological disorder. However, the link between poor sleep and internet use should be further elucidated in African samples. In Africa, factors that encourage excessive and late-night internet use should be studied and addressed. Foremost among these factors is the availability of cheaper internet in the night, commonly called “midnight internet package.” The typical sales advert “trading sleep for data,” which encourages excessive midnight internet use should be discouraged. Perhaps, warning regarding the psychological effect of internet use at night should be attached to the advert as in tobacco use.
Our study has some limitations, which highlight the need to interpret our findings cautiously. It is limited in terms of generalizability to other regions in Nigeria. The convenience sampling method applied, and the broad age range sampled in which there can be diversity in behaviors also limit the interpretation of our findings. Another limitation is the failure to control for sleep quantity, which can mediate the relationship between sleep quality and psychological outcomes. Finally, the analysis cannot determine the causal relationship between our outcome and the dependent variables due to its cross-sectional nature. A longitudinal study will be more applicable.
Conclusions
Our findings revealed PSQ in 12.2% of the adolescents sampled, which falls towards the lower limit of the range reported elsewhere. Age, and use of stimulating drugs, were both not found to predict the poor quality of sleep in our sample. Our study rather suggested the possible influence of psychological and environmental factors such as depression, anxiety, and internet use. We hypothesized that environmental and psychosocial factors that are age-related to maturity are more likely to account for the increasing rate of poor sleep quality rather than the age effect of biological development. Thus, we recommended a more in-depth investigation of the interaction among these factors and sleep quality in a more carefully selected sample of adolescents. Importantly, we suggest further exploration of PSQ as a precursor of psychological disorders, as it may be one of the potential ways of preventing psychiatric disorders from developing later in life. We also prescribed the optimal management of psychological disorders and addictive behavior, of which sleep problems are a consequence.
Footnotes
Acknowledgements
The authors gratefully acknowledge the teachers and those who participated in this study.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ contributions
OAA and AOO (1st) conceptualized the study. AOO collected the data and carried out the analysis. OAA and AOO (3rd) wrote the initial draft. All the authors made significant intellectual input in the writing of the manuscript and agreed to the final draft.