
Abstract
Evidence indicates that substance use and mental health treatment is often associated with reduced criminal activity. The present systematic review examined this association among military veterans, and aimed to provide a comprehensive summary of needed research to further contribute to reduced criminal activity among veterans. This systematic review was derived from a scoping review that mapped existing research on justice-involved veterans’ health. For the current systematic review, a subset of 20 publications was selected that addressed the question of whether criminal activity declines among veterans treated for substance use and mental health disorders. Generally, veterans improved on criminal outcomes from pre- to post-treatment for opioid use, other substance use, or mental health conditions, and more sustained treatment was associated with better outcomes. This occurred despite high rates of criminal involvement among veterans prior to entering treatment. Needed are substance use and mental health treatment studies that include women justice-involved veterans, follow criminally-active veterans for longer periods of time, and use validated and reliable measures of criminal activity with fully transparent statistical procedures. Future randomized trials should evaluate new treatments against evidence-based treatments (versus no-treatment control conditions). Subsequent studies should examine how to link veterans to effective treatments, facilitate sustained treatment engagement, and ensure the availability of effective treatments, and examine mechanisms (mediators and moderators) that explain the association of treatment with reduced criminal activity among veterans. Best practices are needed for reducing criminal activity among the minority of justice-involved veterans who do not have diagnosed substance use and/or mental health disorders.
Introduction
After members of the military are discharged or released from service, some engage in criminal activity and become involved with the criminal justice system. Involvement with the criminal justice system occurs for a number of reasons, including police contact due to homelessness and mental health crises, substance use consequences, and property and violent offenses.1–3 Of national concern is reducing criminal activity and resulting legal difficulties among veterans to prevent adverse consequences for them and their family, friends, and communities. This concern is shared by the varied agencies in which justice-involved veterans are seen, including jails and prisons, and health care settings in the community and, in the US, the Veterans Health Administration (VA), as well as by society at large. 4
About 1 81 500 veterans are in jails and prisons, representing 8% of the total incarcerated population in the US. 5 Because nearly 70% of the US correctional population is supervised in the community on parole or probation, 6 incarcerated veterans are a fraction of the total number of veterans involved in the criminal justice system. Involvement in the criminal justice system includes having been arrested, arrested and charged, convicted, and incarcerated. Nationally representative surveys in the US found that almost one-third of veteran respondents (31.1%) had ever been arrested and booked, a rate significantly higher than among civilians (18.0%). 7 Another study found that although military service during wartime was inversely related to subsequent incarceration, veterans of the post-1973 All Volunteer Force were more likely to be incarcerated than civilians and veterans who served during the draft era. 1
Among veterans in treatment for substance use or mental health problems, a history of criminal justice involvement is the norm rather than the exception. 8 For instance, one study investigated the prevalence of specific types of criminal arrests among a large, nationally representative sample of male patients in VA addiction treatment programs, all of whom served in the military before September 11, 2001. 9 Among these patients, 85% had at least one lifetime criminal charge, and 58% had at least three such charges. In addition, 46% of patients had at least one lifetime conviction, and 17% had at least three such convictions. Another study investigated veterans in addiction or mental health treatment who reported any lifetime history of military or non-military trauma exposure. 10 Overall, 46% reported a history of having a violent or non-violent legal charge.
Among criminal offenders generally, just over two-thirds will recidivate (ie, be rearrested, reconvicted, or reincarcerated for a new crime or violation of their parole or probation) within three years of prison release, and just over three-fourths will recidivate within five years of prison release. 11 Many veterans are caught in a cycle of contact with the criminal justice system such that recidivism is also common among veterans who are justice-involved. Specifically, the majority of incarcerated veterans in US jails and prisons had at least one prior incarceration, and 43% had four or more prior lifetime arrests. 5 In fiscal year 2012, justice-involved veterans who were in contact with the VA’s Veterans Justice Programs (VJP) reported a mean of eight prior arrests in their lifetime. 8 These findings highlight why reducing justice-involved veterans’ criminal activity and recidivism is a top priority for a number of national organizations, including the VA and the Substance Abuse and Mental Health Services Administration.12–14
There is evidence spanning decades that substance use and mental health treatment is associated with reductions in criminal activity among non-veteran adults.15,16 Treatment for an individual with a severe substance use disorder typically involves three to seven days in a medically managed withdrawal (detoxification) program, followed by one to three months of residential care, followed by continuing outpatient care, first in an intensive program (2-5 days per week) and subsequently in a traditional program (1-2 times per month). 17 Patients with serious substance use disorders should stay engaged for at least one year in the treatment process. 17 Effective treatment requires identifying and treating any other mental health conditions. 17 A national study of US adults in recovery found that the mean number of recovery attempts was 5.35 (SD = 13.41), with each episode involving varying degrees of the use of particular clinical approaches, including mental health treatment components. 18
Analyses of the US population have determined that increases in admissions to substance use treatment are associated with reductions in crime and incarceration rates. 19 An analysis of 78 studies conducted from 1965 to 1996 found that drug treatment had a statistically significant and clinically meaningful effect in reducing crime. 20 The National Treatment Improvement Evaluation Study found that drug treatment significantly reduced respondents’ self-reported criminal activity, yielding a 64% reduction in arrests, and a 48% reduction in financial support through illegal activities. 13 More recently, in a sample of 4847 adults with alcohol use disorders, serious mental illness, and criminal justice involvement who received substance use or mental health treatment, number of days incarcerated decreased from pre- to post-treatment, although the likelihood of being arrested did not change. 21 Similarly, in a study in Sweden, among offenders with self-reported mental health and substance use problems who were followed for three years, those with at least three specialized outpatient substance use clinic visits had a substantially reduced risk of reoffending compared to those with fewer than three such visits. 22 In addition, for those with at least three visits, criminal recidivism was reduced by 75% during periods of outpatient treatment participation in comparison to periods of non-participation. 22
Despite such evidence that substance use and mental health treatment is associated with reduced criminal activity among non-veterans, there is a need to examine this association among veterans specifically because of their unique characteristics. Veterans engaged in criminal activity are a special population with distinct needs compared with other veterans or other criminally-involved adults. 23 Veterans are likely to have completed specialized training in tactics, weapons, and use of deadly force. 24 Veterans are more likely to have experienced multiple traumatic events than the general population. 24 Justice-involved veterans have higher rates of mental health disorders than other veterans and other justice-involved adults, with PTSD, substance use disorders, and depression among the most prevalent conditions.8,23,25 Justice-involved veterans with co-morbid substance use and mental health disorders in particular are at increased risk of violent behavior. 23
Veterans may have difficulty readjusting to civilian life, and more difficulty with reintegration may be associated with more criminal justice system involvement.26,27 The most difficult elements of readjusting to civilian life are having had an emotionally traumatic experience while serving, having suffered a serious service-related injury, having served in a combat zone, and knowing someone who was killed or injured. Combat stressors, in particular, may weaken veterans’ ability to face challenges posed by the return home.27,28 The inability to sustain meaningful relationships and control frustrations once home may increase the likelihood that veterans will experience criminal justice-related difficulties. 29 Frustration is due in part to veterans’ observations that while the military does an effective job of training them to operate within the military, it does a poor job of preparing them for civilian life. 30 Frustration among veterans in everyday situations is also traced to their traumatic events from past military experience, such as combat, injury, or the loss of a peer. This is because some of the coping resources that helped during military service are missing in civilian life, such as the structure, routine (food, clothing, and housing are dictated and provided without personal choice), chain of command, clarity, and sense of purpose in daily work that military life provides. Veterans may feel frustrated because civilians don’t understand the experience of serving. For example, employees in civilian life may appear less committed and less interested in teamwork than veterans are accustomed to. Veterans may become frustrated that they often need to translate military skills and jargon they know well into civilian duties and “civilian English.” 31 It is often difficult for veterans to reconnect with and reestablish a role in their family. Due to unrealized expectations and goals about returning home, and an environment with more ambiguity, veterans may feel disappointed, angry, and alienated from their own families and from civilian society, which leads to maladaptive coping that heightens the risk of criminal behaviors.28,32
The current systematic review was derived from a scoping review that mapped the nature, characteristics and volume of existing research on justice-involved veterans and their health and health care. 33 For the current systematic review, a subset of publications gathered for the scoping review was selected to address the question of whether criminal activity declines among veterans treated for substance use and mental health disorders. This review is intended to fill a critical gap in the literature in that identification of treatments that reduce criminal activity will be useful to providers of clinical and social services to justice-involved veterans. In addition to reviewing the relevant studies, a second aim of this paper is to provide, given the findings of the systematic review, a road map for future research aiming to reduce the likelihood of criminal activity among military veterans seeking treatment. In light of the recent upsurge in research to better address the criminal and legal difficulties of veterans, 34 this systematic review offers an ideal opportunity to comprehensively summarize potentially useful future directions.
Method
The method of study selection is presented in Figure 1 which contains the PRISMA flow diagram. The initial scoping review used a variety of search mechanisms to find articles related to justice-involved veterans. Mainly, five databases were searched: MEDLINE/PubMed, Scopus, Web of Science, CINAHL, and PsychInfo. Keywords included veterans or former military, and criminal justice-related terms such as prisoners, jail, court, or probation, with no restrictions on dates searched (for a full listing of keywords, see Finlay et al). 33 The initial scoping review search was implemented on June 2, 2017. Alerts were also created in the selected search engines and articles were added until May 1, 2018. The initial scoping review excluded studies that did not include justice-involved veterans, were not relevant to health or health care, were limited to active duty military, or did not include any results specific to justice-involved veterans. Excluded were case reports, editorials, meeting abstracts, law articles or briefs, letters, protocols, narrative or systematic reviews, unpublished articles, brief news articles that did not report original results, and articles that were not in English or without a published English translation. Included were non-peer-reviewed publications if they were publicly available in a published form (eg, government reports).
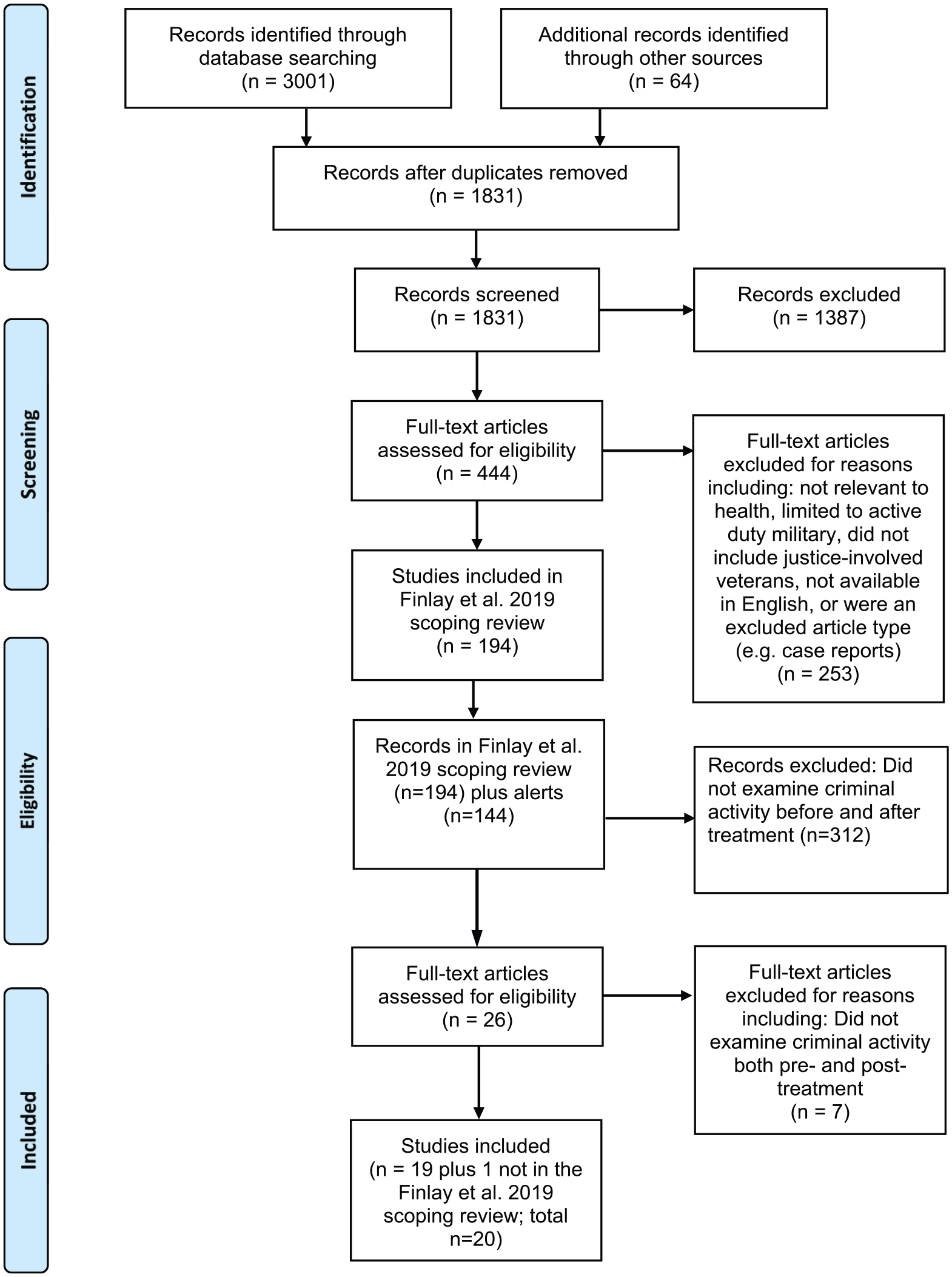
PRISMA flow diagram of study selection.
In the scoping review, prior to abstract review, duplicates were removed. Two authors reviewed all abstracts using Rayyan, 35 and any differences in agreement were discussed and resolved. Full-text articles were obtained for the selected abstracts, and each article was independently reviewed by an author of the scoping review. A 10% random sample of full-text articles were independently reviewed by two authors. Any studies that raised questions were discussed among the research team to reach agreement. For studies selected for inclusion, authors extracted 14 study characteristics that were based on prior studies such as study design, sample size, and reporting of gender, race and age.33,36 In total, the scoping review reviewed 1831 abstracts of which 1387 were excluded. Full-text reviews were conducted for 444 articles of which 250 were excluded. These methods left 194 studies included in the scoping review.
For the current systematic review, the abstract of each of the 194 studies in the scoping review, as well as the abstract of each of the 144 studies to which authors were alerted until May 2018, was reviewed again by two authors to determine whether the study examined criminal activity before and after treatment. This review yielded 26 studies that potentially met this criterion. Of these, seven studies were excluded after a full-article review indicated that they did not examine criminal activity both pre- and post-treatment. In addition, one study was identified that had not been included in the initial scoping review. Thus 20 studies were reviewed.
When the study provided the information needed to compute the effect size (ie, means, standard deviations, and samples sizes to compute Cohen’s d), it was computed and reported. The quality of each study was evaluated using the checklist by Downs and Black, 37 which applies across study designs (eg, observational studies and randomized controlled trials). The checklist has 10 items assessing quality with possible scores ranging from 0 to 11. Each study was rated by two authors on this checklist. Of 200 ratings, the authors initially disagreed on 9 (4%); these disagreements were then resolved between the authors.
Results
Studies included in the review are listed in chronological order in Table 1. All studies took place in the US. All of the study samples were 100% male veterans unless noted in the study description below. In the following sections, we describe studies in three naturally occurring and logical domains: those that focused on opioid use disorder treatment, studies that examined alcohol and other substance use treatment, and studies on mental health treatment. We summarize findings for each type of study treatment briefly in the results section, but mainly in the discussion section.
Summary of published studies on criminal activities before and after treatment among veterans (n = 20 studies).

Note: RCT, randomized controlled trial; yo, years old; MM, Methadone Maintenance; ASI, Addiction Severity Index; CS, composite score; M, Mean, SD, Standard deviation; NR, not reported; LT, lifetime; VHA, Veterans Health Administration; DMH, Department of Mental Health; JSI-M, Justice System Involved-Mandated to treatment; JSI-NM, Not Mandated; COD, Co-occurring disorders; MH, Mental health disorders.
Opioid Use Disorder Treatment
In the earliest study in the review, Bale et al studied 585 veterans entering VA’s detoxification for opioid (heroin) use disorder, 38 80% of whom had at least one lifetime criminal conviction. Groups were compared according to treatment received during the follow-up year. Specifically, treatment received at 1-year follow-up by the 545 veterans followed was none (41%), non-VA (20%), VA short-term (14%) or long-term (14%) residential, and methadone maintenance (MM, 11%). At follow-up, compared to the no-treatment group, patients in long-term VA residential treatment were significantly less likely to have been arrested (37.3% versus 54.5%), and to have been convicted (21.3% versus 38.0%), during the previous year. Also compared to the no-treatment group, patients in MM were significantly less likely to have been convicted (22.0% versus 38.0%). Further, compared to the no-treatment group (21.1%), patients in long-term treatment (4.0%) or in MM (10.2%) were less likely to be in jail. Veterans in the treatment (short- and long-term combined) and MM groups did not differ from each other at the 1-year follow-up on arrests, convictions, or jail status.
Later, Bale et al 39 followed 347 of the same veterans in the first study by Bale et al 38 for a total of a 2-year follow-up. In the follow-up study, 39 analyses compared veterans who had been residentially treated in a professionally-staffed program, a peer-staffed and confrontational program, or an eclectic program, to a single combined group of veterans in MM or no treatment. Results were that veterans in the professionally- and peer-led programs were less likely to have a criminal conviction over the 2-year follow-up than veterans in the combined MM/no-treatment group (percent convicted was 40.5%, 56.0%, and 68.7%, respectively). Veterans in the eclectic program did not differ on convictions at follow-up (67.5%) from the combined group.
McLellan et al conducted a six-month follow-up of veterans admitted to a VA MM treatment program. 40 Participants were grouped according to whether the majority of their pretreatment income was from employment, public assistance, or criminal activity. Legal status was assessed with the Addiction Severity Index’s (ASI) legal composite score, 58 which assesses severity of legal problems in the past 30 days and ranges from 0 (least severe) to 1 (most severe); it was also assessed with an ASI item assessing amount of income from illegal activity in the past 30 days. Significant improvements in legal status were found in the employed group. However, the group initially supported by criminal activity showed the greatest improvement on legal status, whereas the group receiving public assistance showed no significant improvement. In another seven-month study of veterans in VA MM treatment who either stayed in treatment (n = 116) or did not (n = 41) during the follow-up period, both groups improved at follow-up on ASI legal severity scores and number of days of illegal activity in the past 30 days. 45 Veterans who stayed in treatment had better outcomes (ASI legal severity score, number of days of illegal activity) than veterans who discontinued treatment, at both baseline and follow-up. Finally, Rothbard et al studied 126 veterans receiving treatment from a VA (79%) or community (21%) MM clinic. 46 From the two years before to the two years after treatment admission, the mean number of arrests per person, and the number of people arrested, did not significantly change. Analysis of crime categories revealed that property crime (burglary, theft, and receipt of stolen goods) increased significantly, whereas the number of crimes associated with drug and other offenses was similar, for the pre- and post-treatment periods. A longer length of treatment was significantly associated with a lower number of post-treatment arrests.
In summary, the studies that examined opioid use disorder treatment found that veterans who received treatment had better criminal justice outcomes than veterans who were untreated,38,39 that legal problem severity and days of illegal activity decreased from treatment admission to follow-up,40,45 and that longer treatment was associated with a lower likelihood of post-treatment arrest.45,46
Alcohol and Other Substance Use Treatment
McLellan and colleagues conducted a six-month follow-up among veterans admitted to VA residential alcohol treatment. 41 In this study, participants were grouped according to whether they had low, mid, or high mental health symptom severity at treatment admission. Residential alcohol treatment was based on the principles of Alcoholics Anonymous and the structured therapeutic community, with group and individual psychotherapy and social work, educational, and vocational assistance arranged as needed. At baseline, the mean number of lifetime arrests (M = 2, 5, and 5 respectively) and the mean number of months incarcerated (M = 1, 5, and 5, respectively) did not differ among groups (standard deviations were not reported). For veterans with high psychiatric severity, ASI legal severity composite scores, and income from illegal sources, in the past 30 days declined from baseline to follow-up. For veterans with mid severity, legal problems decreased. For veterans with low severity, legal problems and illegal income were quite low at baseline, and did not decrease at follow-up.
In a subsequent study, McLellan and colleagues examined a sample of 742 VA-treated (residential, outpatient, or MM programs) alcohol or drug patients at admission and six-month follow-up. 42 Upon treatment admission, drug patients had more criminal activity (convictions and months incarcerated) than alcohol patients. Accordingly, ASI legal severity composite scores, number of crime days, and illegal income declined for patients in drug treatment at follow-up, but stayed the same for patients in alcohol treatment. However, additional analyses found that alcohol patients in longer-term treatment (>15 days) improved on legal severity scores more than alcohol patients in shorter-term treatment. Drug patients in longer-term treatment improved more than drug patients in shorter-term treatment on legal severity scores, number of crime days, and illegal income. Consistent with these findings, McLellan and colleagues found that, among veterans in drug treatment, number of crime days and illegal income declined between treatment admission and six-month follow-up. 43
McKay et al followed patients with cocaine use disorders 18 months after entrance to VA continuing care, which was initiated after an episode of VA residential treatment. 47 ASI legal severity scores, and the percentage of veterans with legal severity scores of >0, did not change significantly during follow-up. Groppenbacher et al followed veterans admitted to community-based residential substance use treatment for two years after program discharge. 50 The number of arrests declined from 58 in the two years before treatment, to 40 in the two years after treatment, representing a reduction in arrests of 30%. Wallace and Weeks found that veterans who completed a VA substance use intensive outpatient treatment program were significantly less likely to be incarcerated at six-month follow-up than veterans who did not complete the program (1% versus 10%). 51 Kelly et al reported that reductions in arrests from the year prior to VA residential substance use treatment through the five years following treatment were substantial. 52 Patients who were justice system-involved and mandated to treatment, and patients who were justice system-involved but not mandated to treatment, had arrest reductions of 73% and 53%, respectively, during the year following treatment. These reduced rates of arrest were sustained at the 5-year follow-up.
Using another approach, Schultz et al found that veterans (98% male) admitted to VA outpatient substance use treatment clustered into three profiles based on their criminal history: mild (low numbers of criminal offenses, convictions, and months incarcerated; 79% of patients); moderate (high number of public order offenses, repeated convictions, and >3 years incarcerated; 14% of patients); and severe (violent criminal offenses, repeated convictions, and >10 years incarcerated; 7% of patients). 55 All groups improved on ASI legal severity scores from baseline to 1-year follow-up: mild (M = .094 [SD = .169] baseline, to M = .056 [SD = .124] follow-up; moderate (M = .184 [SD = .242] baseline, to M = .050 [SD = .125] follow-up); and severe (M = .182 [SD = .198] baseline, to M = .034 [SD = .120] follow-up); Cohen’s d was .26, .70, and .90, respectively. All groups also improved on percent reporting trouble controlling violent behavior in the past 30 days: mild (13-9%), moderate (27-15%), and severe (25-12%).
In one of only two randomized controlled trials (RCTs) in this review, Siegal et al randomly assigned 453 veterans (98.7% men) who received VA substance use treatment (residential and outpatient treatment followed by continuing outpatient care) to case management or no case management. 49 In the whole sample, ASI legal severity scores declined from baseline to 1-year follow-up (Ms = .17 [SD = .21] and M = .08 [SD = .16], respectively; Cohen’s d = .48), but a significance test was not reported; 31.1% had a new arrest during the 1-year follow-up. Case management was associated with participation in continuing care (β = .425, p < .001), and longer continuing care was associated with lower ASI legal severity scores at follow-up (β = –.112, p < .05). In the second of the two RCTs, Kashner et al randomly assigned homeless veterans with substance use disorders receiving residential services to a supported employment program or a control condition without supported employment; all veterans in the study had access to VA health care. 48 At the 1-year follow-up, veterans receiving supported employment services were 30% less likely to have been incarcerated than controls (p = .01), but specific rates of incarceration were not reported.
To summarize studies that examined substance use treatment other than for opioid use, most reported that legal and criminal problem severity declined among veteran patients, including those with co-occurring mental health problems,41–43,50,52,55 or that longer treatment was associated with better legal and criminal outcomes.42,49
Mental Health Treatment
Relatively few studies of mental health treatment reported criminal activity among veteran participants. In Johnson et al’s study, 44 Vietnam veterans who completed a PTSD residential 3-phase treatment program (prepare for examination of traumatic experiences; review and restructure trauma through therapy; engage with community and family to plan for the future) showed a significant decrease in violent actions and thoughts using a measure from the National Vietnam Veterans Readjustment Study that ranged from 0 to 32. Specifically, from admission to 18-month follow-up, scores changed from M = 14.0 (SD = 6.4) to M = 10.2 (SD = 5.5); Cohen’s d = .64. ASI legal severity scores also decreased significantly from admission to follow-up (M = .21 [SD = .32] and M = .11 [SD = .24], respectively). Buchanan et al constructed a measure of violence (eg, destroyed property, physically fought someone) from the National Vietnam Veterans Readjustment Study that ranged from 0 to 4. 57 Among 35 330 combat Veterans treated in specialized intensive PTSD treatment programs (provided in day hospitals, short-term acute care admission units, specialized intensive inpatient units, and extended-stay residential treatment facilities) between 1993 and 2011, violence decreased between treatment entry and four months post-discharge; Ms = 1.49 (SD = 1.34) and .91 (SD = 1.42); Cohen’s d = .42.
Pandiani et al examined the criminal justice involvement of veterans in the year before and the year after receiving outpatient services from behavioral health programs of VA or a state Department of Mental Health (DMH). 53 Women made up 8% of the VHA sample, and 11% of the DMH sample. More than two-thirds of veterans in both groups received mental health services, and the remainder received substance use services. Veterans who received DMH services experienced a greater reduction in the rate of criminal charging than veterans who received VA services (43% and 17% reductions). However, for veterans with co-occurring mental health and substance use disorders, the rate was reduced 33% among VA service recipients, whereas the rate increased 48% among DMH service recipients.
In Mohamed’s investigation of 661 veterans with co-occurring mental health and substance use disorders (90.6% male), and 2761 veterans who had mental health disorders only (86.8% male), all were enrolled in VA’s intensive case management programs. 54 Programs used the assertive community treatment model which involves a multidisciplinary team approach, direct provision of most services, and 24-hour team coverage of emergency services. At treatment entry, number of nights in jail in the past six months did not differ between groups (Ms [SDs] = 1.9 (9.4) and 1.2 [9.2] for the co-occurring and non-co-occurring groups, respectively) but number of arrests in the past six months was significantly higher for the co-occurring (M = 0.2, SD = 0.7) than the non-co-occurring (M = 0.1, SD = 0.5) group. The change in violent ideation and behavior from baseline to six-month follow-up was described as showing significant improvement (decrease) in the sample as a whole; Ms, SDs, and the statistical test were not reported, however.
In a study of veterans with co-occurring mental health and substance use disorders entering VA outpatient integrated mental health-substance use treatment, Timko et al reported that at treatment intake, 9.2% had no arrest history (of these, 93% were male), 56.3% had been arrested for non-violent offenses only (of these, 92% were male), and 34.5% had been arrested for violent offenses (of these, 91% were male). 56 All three groups improved from baseline to 2-year follow-up on ASI legal severity scores: no arrests (M = .008 [SD = .038] baseline, M = .006 [SD = .001] follow-up; non-violent arrests (M = .108 [SD = .174] baseline, M = .014 [SD = .069] follow-up; violent arrests M = .113 [SD = .180] baseline, M = .047 [SD = .136]. Significance tests from baseline to follow-up were not conducted, but Cohen’s d was .07, .71, and .41, respectively. All three groups improved from baseline to 2-year follow-up on percent reporting trouble controlling violent behavior in the past 30 days: no arrests (50.0% at baseline to 9.5% at follow-up), non-violent arrests (50.3-11.3%), and violent arrests (71.4-16.3%).
Among studies that examined mental health treatment, all reported a decrease in legal problem severity and/or violent ideation from pre- to post-treatment.44,53,54,56 We summarize and interpret findings pertaining to opioid, alcohol and other substance use, and mental health treatment more fully in the discussion section.
Discussion
We systematically reviewed 20 studies that reported criminal behavior outcomes of veterans treated for substance use and mental health disorders. Generally, treated veterans improved on criminal behavior outcomes from pre- to post-treatment, and more sustained treatment was associated with better outcomes. Effect sizes indicating the strength of associations of substance use or mental health treatment with reduced legal or violence severity scores were generally in the medium to large range and were larger for patients with scores that were more severe at baseline.44,49,55–57 Improvement occurred despite the high rates of criminal involvement prior to entering opioid use, other substance use, or mental health treatment. For example, Timko et al’s study found that 91% of veterans entering mental health treatment had a history of violent or non-violent offenses. 56
More specifically, of the four studies (counting the two Bale publications as one study) that examined opioid use disorder treatment, one found that veterans who received treatment (residential, MM) had better outcomes than veterans who were untreated on criminal justice outcomes assessed by arrests, convictions, and incarceration. 38 Two others found that legal problem severity and days of illegal activity decreased from treatment admission to follow-up;40,45 one of these also found that veterans who stayed in treatment had better outcomes than those who discontinued treatment. 45 Rothbard et al found that property crime increased post-treatment, 46 but also found, consistent with findings of Cacciola et al, 45 that longer treatment was associated with a lower likelihood of post-treatment arrest. Rothbard et al’s study was the only one in which some veterans received treatment at a non-VA program, which may have been related to poorer treatment effectiveness. 46
Of eight studies that examined other substance use treatment, seven reported that legal and criminal problem severity declined among veterans with alcohol or drug use disorders and among veterans with co-occurring mental health problems.41–43,50,52,55 In addition, longer treatment was associated with better outcomes among alcohol and drug patients,42,49 and treatment completion (which cannot be achieved if patients are detained or reincarcerated during treatment) was related to a lower likelihood of incarceration than was non-completion. 51 All of these studies examined veterans entering a new episode of substance use treatment. In contrast, the study that reported no change in legal problem severity followed patients who had completed an episode of residential treatment and then transitioned to continuing care, 47 which was the treatment setting studied.
Of four studies that examined mental health treatment, all reported a decrease in legal problem severity and/or violent ideation from pre- to post-treatment.44,53,54,56 Pandiani et al found that, for veterans with co-occurring mental health and substance use disorders, rates of criminal charging decreased when treatment was provided by VA, but increased when treatment was provided by state services. 53 Together with Rothbard et al’s study, 46 findings suggest that VA may provide the organization and culture that veterans need to enhance treatment effectiveness. 53
Limitations of Studies Reviewed
Limitations of the studies reviewed are that study quality varied (see Table 1), and only two studies, both of substance use patients,49,58 used a randomized controlled trial (RCT) design, which is considered by many to be the gold standard for studies examining treatment effectiveness. We also note that the great majority of veterans studied were male, samples varied in terms of size and follow-up rates, and none of the studies reviewed selected research participants based on their having a criminal justice or criminal activity history. Indeed, none of the study interventions was intended to address criminal justice involvement as a primary treatment outcome. Accordingly, although studies often used the ASI legal composite score as an indicator of criminal activity (finding generally that legal severity decreased from treatment admission to post-treatment follow-up among substance use and mental health patients41,42,55,49,56), there was not consistency as to how criminal activity was measured, some studies did not adequately report statistical analyses on criminal outcomes, and the great majority of studies relied on veterans’ self-reports of criminal involvement without corroboration. Even aspects of criminal involvement measured at study baseline or as indicators of recidivism at follow-up that can be corroborated through documentation, such as arrests, have limitations. Using re-arrest as an indicator of recidivism may be inaccurate because arrest patterns often reflect shifting police tactics such that areas where law enforcement operates with alternatives to arrest may have lower arrest rates overall. 59 Further, the majority of studies (n = 12) followed participants for only one year or less which does not adequately capture likely recidivism. Thus, particularly needed are substance use and mental health treatment studies that include women justice-involved veterans, follow women and men justice-involved veterans for longer periods of time, and use validated and reliable measures of criminal activity with fully transparent statistical procedures.
Building a Research Agenda
Having reviewed the state of the literature on associations of substance use and mental health treatment with criminal justice-related outcomes among veterans, another purpose of this study is to describe next steps needed in this research area to better serve the veteran population. Future studies of veterans with substance use and mental health disorders that address reduced criminal activity as a treatment goal should be designed in keeping with the evidence provided here, even with its noted limitations. That is, well-delivered substance use and mental health treatment is generally associated with better criminal and legal outcomes. Although causal assertions with regard to the effects of treatment on criminal activity cannot be made, reductions in arrests and incarcerations are important because they result in concomitant reductions in law enforcement and judicial expenses, as well as reductions in broader societal costs. 52 Future investigations should also be designed with the knowledge that many treatment approaches for substance use and mental health disorders are supported as effective for their primary goals of reducing substance use and mental health symptoms. 60 Therefore, it is unlikely that a no-treatment control condition should be considered in future trials to reduce criminal activity among veterans, because withholding or delaying treatment would be unethical. Rather, any new interventions must be tested against control conditions with supported effectiveness. This will “raise the bar” for studies attempting to show a relative benefit for a newly-developed or untested treatment approach in terms of improving criminal activity and other outcomes.
Given the evidence that substance use and mental health treatment is likely to be associated with reduced criminal activity, in addition to developing and evaluating new intervention approaches, forthcoming research should focus on practices to link veterans to treatment, and on ensuring that effective treatments are available. With regard to linkage, the VA’s VJP offices connect justice-involved veterans to health care services through two nationwide programs, Veterans Justice Outreach (VJO) and Health Care for Reentry Veterans (HCRV), with demonstrated effectiveness.12,61 The VJP offices also work closely with Veterans Treatment Courts, which provide rehabilitation rather than incarceration for criminal justice involvement, in part by linking veteran participants to mental health, substance use, and medical care, as well as housing and employment services. 62 There is little research on the effectiveness of the VTC model and this research is needed, along with investigation of other means by which the legal system could leverage effective treatment modalities for veterans to reduce criminal justice involvement. VTC participants describe treatment and recovery services as well as the high level of structure associated with the VTC as vital to their desistance from criminal activity. 62 In addition to linkage through VTCs, research has shown that substance use patients and patients with co-occurring substance use and mental health disorders can be successfully linked to treatment and to 12-step groups, which in turn improves substance use and mental health as well as criminal justice-related outcomes.63–65 These linkage interventions are brief and practical to apply on a routine basis in health care settings and could be investigated in selected samples of veterans with a history of criminal activity.
To ensure that effective treatments are available to justice-involved veterans, research is needed on how best to implement these treatments in settings that provide services to this target population. Implementation of an effective treatment requires action-oriented steps to change existing operations. 12 In a current implementation effort, Simmons et al are using Facilitation as an implementation strategy to promote adoption and use of a peer mentor program that provides reentry services to veterans leaving prison. 66 In this approach, implementation researchers (called “external facilitators”) are partnering with local staff (“internal facilitators”) to tailor adoption strategies to the local context. A hypothesis of this study is that improving the reentry process will contribute to improved substance use and mental health among veterans with criminal justice histories, which highlights the bidirectional associations between criminal activity and well-being. More generally, other efforts to implement effective substance use treatment strategies have used multifaceted academic detailing programs with components such as training local providers to serve as intervention champions, and a website for providers that offered educational materials, a case-finding dashboard, and contact information for clinical experts.67,68 These efforts serve as illustrations of how researchers might increase the availability of effective treatments for criminally-involved veterans.
In considering this review’s findings that longer or completed treatment was associated with better criminal outcomes,42,45,46,49,51 future studies could be aimed at determining the optimal treatment “doses” to improve outcomes—that is, the dose with the greatest value in terms of benefiting patients while conserving health system resources. As these optimal treatment doses are determined, studies could focus on how to ensure that justice-involved veterans stay in treatment for the needed dose or period of time. Most likely, the optimal treatment duration will depend on patient severity and other patient characteristics such that more severe patients (eg, patients who have committed major or violent crimes, or those with serious mental illness) need longer treatments to obtain benefits. 69
Both RCTs and observational studies of treated justice-involved veterans should also be designed to examine the mechanisms—moderators and mediators—that explain the associations of treatment with reduced criminal activity. Studies are needed to identify and evaluate moderators and mediators of criminal desistence in different subpopulations of veterans, including those having different cultural and socioeconomic milieus, life stage, housing and support networks, cognitive functioning, and medical disorders. Such studies would help service providers determine which veterans should be targeted for which treatments. Such investigations have the potential to generate new information about the processes of staying away from criminal activity and relapsing to criminality and would have a significant impact in advancing the field.
A final question related to needed research is how treatment should be conceptualized for veterans who have criminal justice and legal difficulties in the absence of diagnosed substance use and mental health conditions in order to reduce the likelihood of future criminal activity. This question may be of concern for the minority of justice-involved veterans, as at least one-half have an alcohol and/or drug use disorder (estimates are as high as 71% and 65%, respectively) and other mental health disorders, such as depression (estimates are as high as 51%). 23 For criminally-involved veterans without mental health conditions, the question is how best to address cognitive processes that may be potential risk factors for criminal activity and for recidivism following desistance. Cognitive-behavioral interventions such as Moral Reconation Therapy (MRT) have been developed to restructure antisocial cognitions and behaviors with the aim of reducing criminal recidivism. 4 MRT is relatively intensive in that it uses manualized exercises and lessons directed at groups of 10 to 15 offenders, and involves 12 to 16 face-to-face sessions, with each session lasting up to two hours. Although there is evidence of MRT’s effectiveness, 70 still needed are studies that compare MRT to an active intervention, rather than an untreated control condition. Accordingly, Blonigen et al are currently testing the effectiveness of MRT to reduce risk for criminal recidivism and improve health-related outcomes among justice-involved veterans in residential mental health treatment. 71 More generally, still needed are health system studies of interventions to deter criminal involvement and recidivism. Such studies could include treatment delivery by means of telephone and mobile app and web-based technology to increase reach to criminally-active veterans.
Limitations
In this systematic review, a second review was conducted of only a subset of the full-text articles. In addition, because researchers tend to publish studies that show a significant effect, the review’s reliance on published studies may not fully represent findings on criminal and legal involvement following substance use and mental health treatment among veterans.
Conclusion
Substance use and mental health disorders and criminal activities can be viewed as chronically relapsing conditions and behaviors that require ongoing support and management after a course of treatment in order to maintain treatment gains and prevent relapse or recidivism. These behaviors are not easy to study because, for example, law enforcement agencies have discretion on how to respond to potentially criminal behaviors, depending on who is engaging in them, where they are taking place, and whether the individual has an advocate to help with diversion from further criminal system involvement. 72 Despite their methodological weaknesses, the studies reviewed here consistently indicate that participation in substance use and mental health treatment can be beneficial in reducing criminal activities among veterans. Veterans who enter treatment often struggle with a host of factors in addition to any criminal involvement that take time to resolve (eg, housing, employment, and family problems) and place them at heightened risk for recidivism for considerable lengths of time. 23 This larger context of veterans’ experiences and needs must be considered as researchers design, evaluate, and implement interventions to prevent criminal activity and legal involvement.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the VA Health Services Research and Development (HSR&D) Service (CDA 13-279 to Dr. Finlay; RCS 00-001 to Dr. Timko) and VA Office of Academic Affiliations (TPH 61-000-20, Advanced Fellowship in HSR&D, to Dr. Owens). The views expressed are the authors’ and do not necessarily reflect those of the VA.
Declaration of Conflicting Interest:
The authors declare that there is no conflict of interest.
Authors’ Contributions
All authors made substantial contributions to the study’s conception and design, methods for data coding, and interpretation of findings. CT and AN drafted the manuscript, and all authors were involved in revising it critically for important intellectual content. All authors gave approval for the final version to be published.