
Abstract
This study examined rates of heavy drinking and alcohol problems in relation to drinking motives and protective behavioral strategies in university students with a documented current diagnosis of attention-deficit/hyperactivity disorder (ADHD; n = 31) compared with students with no history of ADHD (n = 146). Participants completed a Web-based questionnaire, and logistic regression models tested interactions between ADHD/comparison group membership and motives and protective strategies. Group differences in rates of heavy drinking and alcohol problems were not statistically significant, but medium-sized risk ratios showed that students without ADHD reported heavy drinking at a rate 1.44 times higher than students with ADHD and met screening criteria for problematic alcohol use at a rate of 1.54 times higher than students with ADHD. Other key findings were, first, that drinking to enhance positive affect (e.g., drinking because it is exciting), but not to cope with negative affect (e.g., drinking to forget your worries), predicted both heavy drinking and alcohol problems. Second, only protective behavioral strategies that emphasize alcohol avoidance predicted both heavy drinking and alcohol problems. Contrary to expectations, we found no ADHD-related moderation of effects of motives or protective strategies on our alcohol outcomes. Results of this study are limited by the small sample of students with ADHD but highlight tentative similarities and differences in effects of motives and strategies on drinking behaviors and alcohol problems reported by students with and without ADHD.
Alcohol is a centerpiece of student social life on university campuses. As many as 76% of students drink alcohol, and 37% to 60% of students report heavy drinking (5 or more drinks in a row),1,2 rates that far exceed their nonstudent, same-aged peers. 3 Students actively encourage each other to drink,4,5 and students see drinking as an important way to meet new people, make friends, and have fun. 6 However, the social functions of drinking for some students carry negative consequences. Students who report heavy drinking miss more classes, earn lower grades, and are more likely to drop out of university.7,8 More severely, alcohol-related injuries and assaults are common, 9 and students are more likely than their nonstudent, same-aged peers to develop an alcohol use disorder. 10
Heavy drinking is an understudied concern for students with attention-deficit/hyperactivity disorder (ADHD), who comprise between 2% and 8% of the university population by self-report. 11 Attention-deficit/hyperactivity disorder is a common childhood neurodevelopmental disorder, with core symptoms of inattention (eg, difficulty sustaining attention on tasks such as schoolwork) and hyperactivity/impulsivity (eg, difficulty sitting still, taking turns during activities or conversation). Attention-deficit/hyperactivity disorder continues into adulthood12,13 with many of the same childhood symptoms but with diminished hyperactivity. 14 Students with ADHD have poorer grade point averages, report more academic concerns, and withdraw from more courses.15,16 They are also less likely to complete their degrees than students without ADHD.17,18 Social skills and adjustment to university life are also poorer for students with ADHD compared with non-ADHD peers. 19 However, the few studies examining alcohol use in students with ADHD have yielded inconsistent results. Students who self-reported a current ADHD diagnosis consumed alcohol more frequently than students without ADHD in one study 16 but in another study reported similar rates of consumption. 20 Another study showed that students meeting symptom criteria for current ADHD did not use more alcohol than students without ADHD but were more likely to experience alcohol problems (e.g., driving while intoxicated, risky sex). 21 Inattention symptoms in a general population sample of university students also predicted more alcohol problems but not more alcohol use. 22 One study that assessed student ADHD through their formal registration with a campus disability services office found that consumption rates were lower in students with ADHD compared with students without ADHD. 23 These conflicting findings are difficult to resolve because no studies have yet investigated potential mechanisms linking student ADHD to patterns of alcohol use or problems. In this study, we test whether drinking motives and protective behavioral strategies, consistent predictors of typical student drinking, are differently related to heavy drinking and alcohol problems in students with and without ADHD.
Drinking to Enhance and to Cope
In motivational models of alcohol use, a desire to regulate emotional experiences governs the strategic use of alcohol to either increase positive affect or reduce negative affect.24,25 Motives are viewed as powerful, proximal predictors of alcohol use. Indeed, students endorsing more drinking motives consume more alcohol per week and spend more hours drinking in a given week.26,27 Alcohol consumption and associated problems have been consistently associated with 2 internal sources of motivation: positively reinforcing enhancement motives (e.g., drinking for fun or to get high) and negatively reinforcing coping motives (e.g., drinking to forget your worries).28–30 Enhancement motives for drinking are among the most commonly endorsed drinking motives,31,32 aligning with the predominantly social environment for student drinking. For example, only enhancement motives were associated with heavy drinking on Friday and Saturday nights in one study, 33 suggesting that students intentionally drink to excess on weekends for fun, excitement, and to feel intoxicated. 34 Coping motives for drinking are less commonly endorsed by students, despite high rates of depression on university campuses. 35 However, coping motives are endorsed at high rates by students who report heavy drinking and who meet screening criteria for alcohol problems. 32
Coping motives align poorly with the heavily social context typical of university drinking. In samples of student drinkers, just 15% endorsed any recent solitary heavy drinking,36,37 and rates are low even among moderate to heavy student drinkers (24%). 38 A possible mechanism explaining the link between coping motives and heavy drinking for the subset of students fitting this profile may be poor impulse control—a common challenge among people with ADHD. Problems such as poor delay of gratification predict more alcohol use and more alcohol-related problems, 39 and poor impulse control and emotion dysregulation consistently predict drinking to cope, which in turn predicts alcohol problems in college and non-college samples.40–44 Executive function deficits typical of ADHD such as difficulty delaying gratification and heightened sensitivity to immediate rewards are related to more impaired functioning in students with ADHD. 45 These deficits may similarly strengthen the link between enhancement motives and heavy drinking for students with ADHD. No studies have yet examined associations between drinking motives in university students with and without ADHD.
Protective Behavioral Strategies
Another key factor in understanding student drinking—and a common emphasis of campus drinking intervention programs—is students’ use of protective behavioral strategies to reduce negative alcohol-related consequences, such as limiting drinks and alternating alcoholic with nonalcoholic drinks. 26 Protective behavioral strategies leverage students’ impulse-control and self-control skills and have been successful in reducing high-risk drinking and alcohol problems in students.46,47 Students who use protective behavioral strategies generally consume less alcohol 26 and report fewer negative alcohol-related consequences such as injury and unprotected sex.27,48–50 As typically measured, protective behavioral strategies comprise conscious, intentional cognitive-behavioral strategies to reduce high-risk drinking in social situations. Strategies include planning to stop drinking at a predetermined time or limiting drinks consumed, eating before drinking, and spacing out drinks (limiting/stopping; strategies while drinking), and avoiding mixing different types of alcohol and avoiding drinking games (manner of drinking; selective avoidance), among others.51,52 In general, studies show that effects of risk factors such as coping motives and poor impulse control are weakened or eliminated for students who use protective strategies, reducing their alcohol consumption, consequences, and problems to levels comparable with students who do not possess the same risk factors. 53 At the same time, risk factors make it more difficult for students to implement protective strategies, and not all students are equally successful.
Motives for drinking conflict with motives for implementing protective strategies under certain circumstances. Students who plan to become intoxicated may intentionally drink quickly or mix types of alcohol to achieve that state. Indeed, students who report greater enhancement motives for drinking also report using fewer protective strategies.26,27,54 Such intentions are thought to account in part for excessive drinking that occurs at special events such as spring break 55 and 21st birthdays. 56 For students who drink to cope, negative emotions such as depressive symptoms may present a barrier to activating the cognitive resources needed to implement consequence-reduction strategies that require substantial planning in advance of drinking episodes.57,58 However, coping motives for drinking are generally unrelated to protective strategies.26,27,59 An exception is one study that found first-year students who endorsed fewer protective strategies reported more abuse and dependence consequences after drinking only if they also reported high levels of coping motives. 60
Poor impulse control is a resource limitation that may also make it difficult for students to implement protective strategies, and these deficits are prominent in students with ADHD. 61 Students with poor self-regulation abilities and who used few protective strategies reported the most alcohol-related negative consequences in one study. 62 No studies have yet examined whether students with ADHD endorse fewer protective strategies nor whether endorsing protective strategies is related to heavy drinking or alcohol problems in students with ADHD.
This Study
The aim of this study is to explore drinking motives and protective behavioral strategies as potential sources of similarities and differences in heavy drinking and alcohol problems for students with and without a diagnosis of ADHD. We asked (1) whether there are differences in rates of heavy drinking and alcohol problems, endorsement of coping and enhancement motives, and endorsement of protective behavioral strategies between students with and without a current diagnosis of ADHD; (2) whether ADHD group differences in heavy drinking and alcohol problems depend on students’ motives and strategy use; and (3) whether effects of strategy use on heavy drinking and alcohol problems depend on students’ motives.
Method
Participants and procedure
Participants were (N = 208) undergraduate students at a mid-sized, eastern Canadian university, recruited from 2 settings. First, n = 43 students with a current ADHD diagnosis (the ADHD group) were recruited from an on-campus center for students with disabilities. Students seeking access to academic accommodations such as extra time to complete tests and exams or note-taking services register for a disability assessment. Students with ADHD must present a diagnostic statement and evaluation from a registered psychologist, neuropsychologist, psychiatrist, or physician with relevant training. Students with such documentation were eligible to participate. Second, a comparison and convenience sample of n = 165 students without a current or past ADHD diagnosis (the comparison group) was recruited from a participant pool of students enrolled in introductory psychology courses. Students responded to the following question: “In your lifetime, have you ever received a diagnosis by a doctor or mental health professional (eg, psychologist) for Attention Deficit/Hyperactivity Disorder (ADHD)?” Any student who reported no lifetime history of ADHD was eligible to participate.
Participants provided informed consent and completed a 30-minute, Web-based survey between December 2014 and February 2015. Attention-deficit/hyperactivity disorder group students were compensated by entry into a draw to win a $100 deposit of funds onto their student card (redeemable for on-campus food, goods, and services). Comparison group students were compensated with 0.5% course credit.
Measures
Heavy drinking and alcohol problems
Students were asked whether they had ever consumed any alcoholic beverage (“more than just a few sips”). Students who responded negatively (n = 25) were excluded from further assessment. Students with any history of alcohol use viewed a reference image for a “standard drink” developed by the University of Virginia’s Gordie Center for Substance Use Prevention (http://gordiecenter.studenthealth.virginia.edu/basics) with the following definition: “A ‘drink’ is a bottle of beer, a glass of wine, a wine cooler, a shot glass of liquor, a mixed drink, etc. Here is an image to describe how much alcohol is in a standard drink.” Heavy drinking was assessed by asking students how many times in the past 2 weeks they consumed 5 or more drinks on a single occasion. Students were coded 1 if they reported heavy drinking at least once in the past 2 weeks and coded 0 if they did not. Alcohol problems were assessed using the Alcohol Use Disorders Identification Test (AUDIT), 63 a 10-item tool to screen for high-risk drinking patterns that perform well in college student samples. 64 Items assess drinking quantity and frequency and drinking behaviors that suggest problematic patterns of alcohol use (e.g., morning drinking to “get going,” feelings of guilt/remorse, unable to stop drinking once started). Responses to all items were summed, giving scores that ranged from 0 to 40, with higher scores indicating more alcohol problems. A score of 8 or higher was considered evidence of alcohol problems. Students were coded 1 if they reached or exceeded this threshold and coded 0 if they did not.
Drinking motives
Students responded to 20 items assessing motives for drinking alcohol from the Drinking Motives Questionnaire-Revised (DMQ-R). 28 In this study, we focused on 2 subscales of the DMQ-R that assessed coping motives (e.g., “you drink to forget your worries”) and enhancement motives (e.g., “you drink because it’s exciting”). For each subscale, higher mean scores indicate stronger motives for drinking. Coefficient α was 0.86 for coping motives and 0.88 for enhancement motives.
Protective behavioral strategies
Students reported their use of 15 different strategies for limiting the negative and harmful effects of alcohol use from the Protective Behavioral Strategies Scale (PBSS). 51 Responses were on a scale ranging from 1 (never) to 6 (always). Three subscales of the PBSS assessed strategies for limiting/stopping (7 items, e.g., “alternate alcoholic and nonalcoholic drinks”), manner of drinking (4 items, e.g., “avoid mixing different types of alcohol”), and serious harm reduction (3 items, e.g., “know where your drink has been at all times”). A fifth item from the manner of drinking subscale (“drink shots of liquor”) was dropped due to its contribution to scale unreliability. For each subscale, higher mean scores indicate greater use of protective strategies to limit negative effects of alcohol. Coefficient α was 0.83 for limiting/stopping and 0.77 for manner of drinking. We excluded serious harm reduction from further analyses due to its low internal consistency (α = 0.51).
Depressive symptoms
Depressive symptoms were not a central measure of interest in this study, but given the relevance of this construct to coping motives and the high prevalence of depression in university populations, we included it as a descriptive measure. Students reported their depressive feelings over the past week by responding to the 20-item Center for Epidemiologic Studies Depression Scale (CES-D). 65 Responses were on a scale ranging from 0 (rarely or none of the time; less than 1 day) to 3 (most or all of the time; 5-7 days). The mean of 20 items, such as “I felt depressed,” “I had crying spells,” and “I felt hopeful about the future” (reverse-coded), assessed students’ symptoms. Higher mean scores indicate more depressive symptoms. Coefficient α for the scale was 0.92.
Missing data and analysis strategy
Of the original sample, 5 students (4 ADHD, 1 comparison) exited the survey before completing any measures relevant to this study. Of the remaining 38 participants in the ADHD group, 28 provided complete data on predictor variables (72%). Of the remaining 164 comparison participants, 144 provided complete data (87%). Most missing data came from participants who reported never consuming alcohol (an exclusion criterion in this study—7 students from the ADHD group; 18 students from the comparison group) and consequently were not shown follow-up questions on alcohol use, including measures of motives and protective strategies. These exclusions reduced our final analytic sample to n = 177 (n = 31 ADHD and n = 146 comparison participants). There were 5 additional participants missing data for unknown reasons such as fatigue or loss of interest, but given the small sample in the ADHD group, we retained all 177 cases with multiple imputation. We created 100 data sets using SAS PROC MI software and integrated logistic regression results across data sets using SAS PROC MIANALYZE.
Descriptive statistics summarized differences between students with and without ADHD in rates of heavy drinking, drinking problems, depressive symptoms, motives for drinking, and protective behavioral strategies. We followed this analysis with logistic regression analyses predicting (1) heavy drinking and (2) alcohol problems (AUDIT score ⩾8) from ADHD versus comparison group, coping and enhancement motives, limiting/stopping strategies, and manner of drinking strategies. We limited tests involving ADHD versus comparison group membership to 2-way interactions with every other predictor variable due to the small number of students with ADHD in the sample. We tested all 2-way interactions between motives and protective strategies. We trimmed nonsignificant interactions one at a time, beginning with the highest-order terms and in order of largest to smallest P values (see recommendations of Aiken and West, pp. 111–113 66 ). All interaction terms were retained if P < .10 to control for Type II error associated with dropping nonsignificant terms and to minimize bias to lower-order terms in our regressions.
Results
Our first aim concerned differences between students with and without ADHD in our suite of alcohol involvement measures. Table 1 shows descriptive statistics and pairwise tests of differences between students with and without ADHD on all study measures, and correlations are presented in Table 2. Distributions of data for each measure are presented in Figure 1, separately for each type of drinking and contrasting ADHD and comparison students. Descriptively, students with ADHD endorsed fewer coping and enhancement motives compared with students without ADHD. Students with ADHD endorsed not only higher levels of limiting/stopping and manner of drinking strategies but also higher levels of depressive symptoms compared with students without ADHD. Rates of heavy drinking and alcohol problems were higher in comparison group students without ADHD. None of these group differences were statistically significant using the Benjamini-Hochberg false discovery rate P value correction. However, the mean differences in enhancement motives and depressive symptoms were small-sized to medium-sized effects (Cohen’s d = 0.37−0.42), and the risk ratios for heavy drinking and alcohol problems were medium sized. Given nonsignificant P values for pairwise tests, however, group differences in this study were inconclusive.
Mean values, standard deviations, proportions, and effect sizes of study variable differences between ADHD and comparison students.
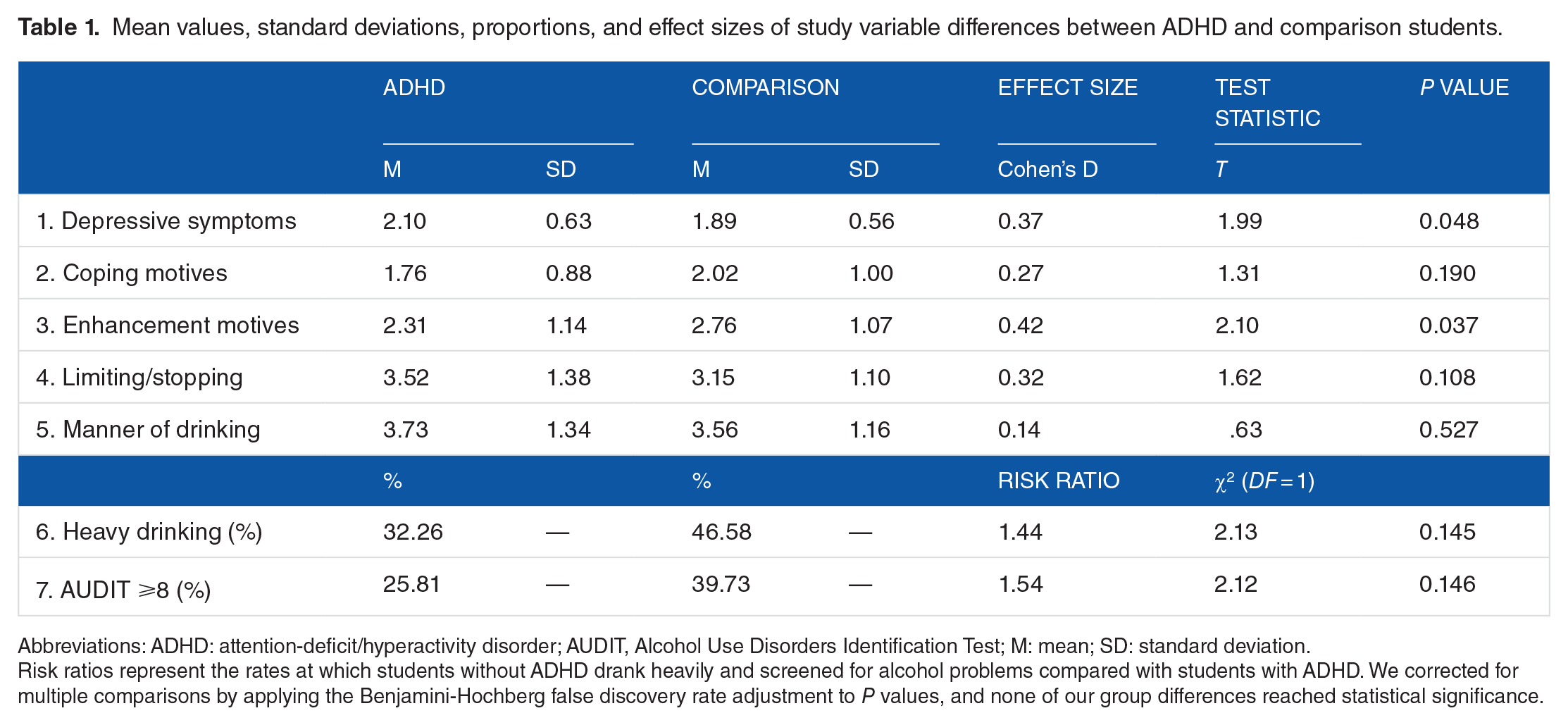
Abbreviations: ADHD: attention-deficit/hyperactivity disorder; AUDIT, Alcohol Use Disorders Identification Test; M: mean; SD: standard deviation.
Risk ratios represent the rates at which students without ADHD drank heavily and screened for alcohol problems compared with students with ADHD. We corrected for multiple comparisons by applying the Benjamini-Hochberg false discovery rate adjustment to P values, and none of our group differences reached statistical significance.
Intercorrelations among study variables for ADHD and comparison students.
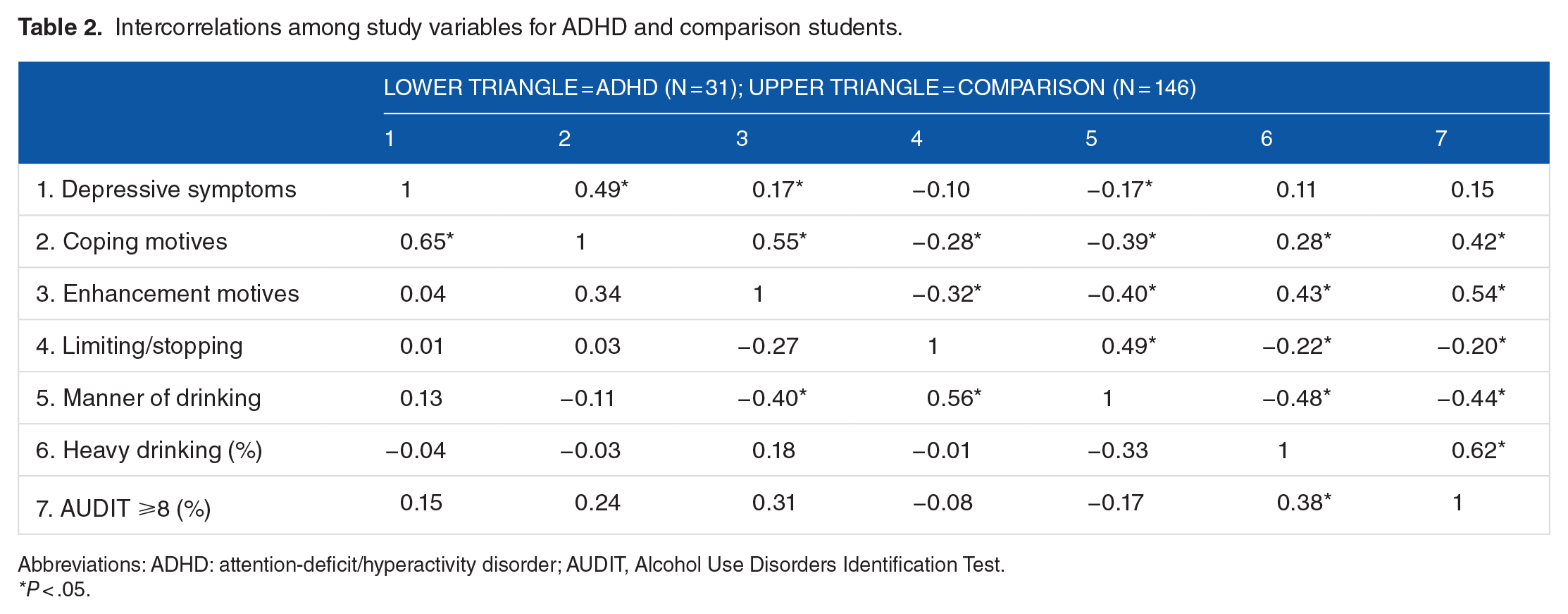
Abbreviations: ADHD: attention-deficit/hyperactivity disorder; AUDIT, Alcohol Use Disorders Identification Test.
P < .05.

Point and box plots showing distributions of data across ADHD and comparison groups for drinking motives, protective behavioral strategies, and depressive symptoms, presented separately for heavy drinking and alcohol problems. ADHD indicates attention-deficit/hyperactivity disorder; AUDIT, Alcohol Use Disorders Identification Test.
Our second and third aims targeted predictive tests of heavy drinking and alcohol problems in ADHD versus comparison students and whether effects of drinking motives and protective strategies differed in each group. Table 3 shows logistic regression results predicting the log odds of heavy drinking. Enhancement motives predicted an increased odds of heavy drinking, and manner of drinking strategies predicted a decreased odds of heavy drinking. There were no significant differences between students with and without ADHD, no significant effects of limiting/stopping strategies or coping motives, and no 2-way interactions between study variables.
Logistic regression results predicting heavy drinking.
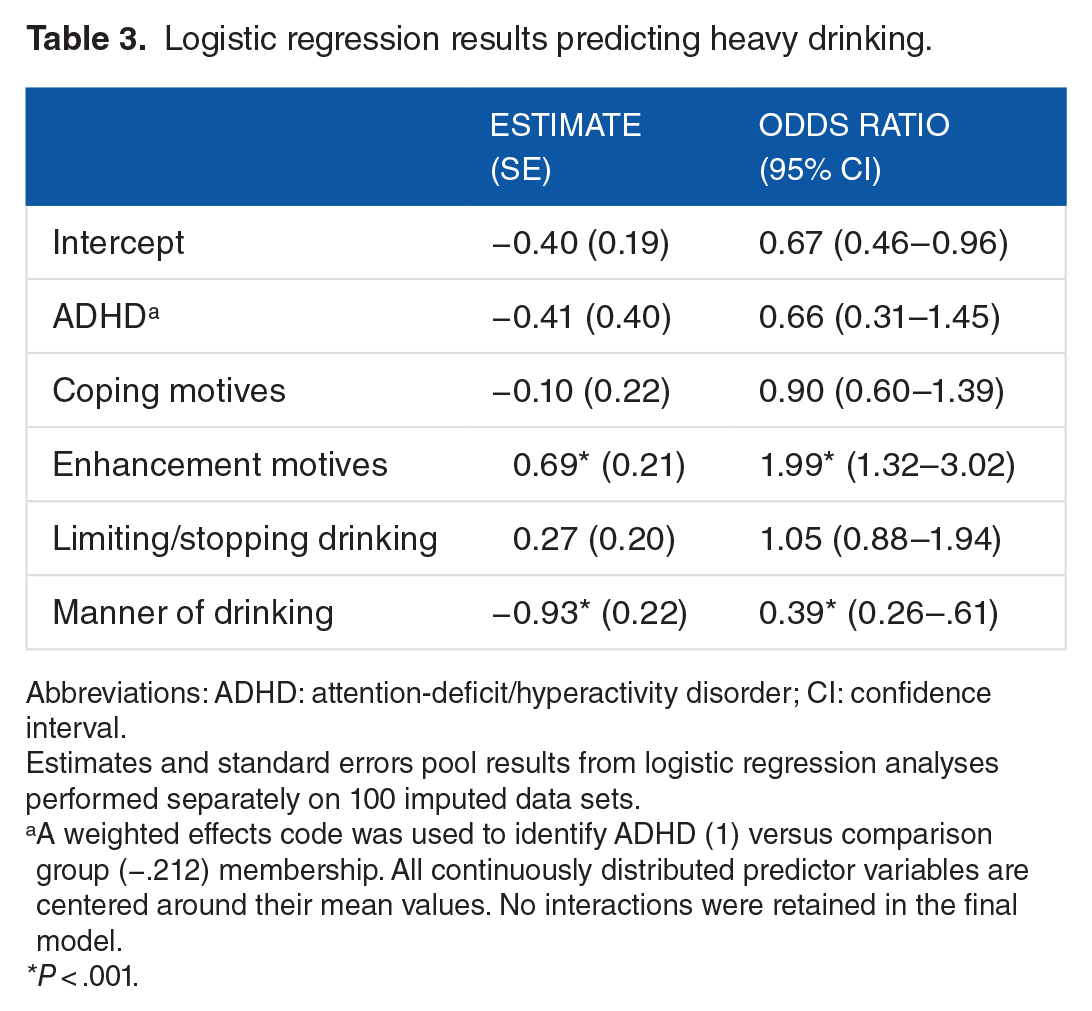
Abbreviations: ADHD: attention-deficit/hyperactivity disorder; CI: confidence interval.
Estimates and standard errors pool results from logistic regression analyses performed separately on 100 imputed data sets.
A weighted effects code was used to identify ADHD (1) versus comparison group (−.212) membership. All continuously distributed predictor variables are centered around their mean values. No interactions were retained in the final model.
P < .001.
Table 4 shows logistic regression results predicting the log odds of meeting criteria for alcohol problems (AUDIT score ⩾8). Similar to results for heavy drinking, enhancement motives were associated with an increase and manner of drinking strategies was associated with a decrease in the odds of problematic alcohol use. There were no significant differences between students with and without ADHD nor any differences due to limiting/stopping strategies.
Logistic regression results predicting alcohol problems (AUDIT score ⩾8).

Abbreviations: ADHD: attention-deficit/hyperactivity disorder; AUDIT, Alcohol Use Disorders Identification Test; CI: confidence interval.
Estimates and standard errors pool results from logistic regression analyses performed separately on 100 imputed data sets.
A weighted effects code was used to identify ADHD (1) versus comparison group (−.212) membership. All continuously distributed predictor variables are centered around their means. The interaction is the product of centered variables.
P < .005; †P = .079.
Discussion
This study examined heavy drinking and problematic alcohol use in university students with and without a current diagnosis of ADHD. We tested moderating influences of students’ drinking motives and use of protective behavioral strategies, and in our discussion, we emphasize 3 key points. (1) No statistically significant differences emerged between drinking rates of students with and without ADHD, but effect sizes suggest less heavy drinking and fewer alcohol problems in students with ADHD. (2) Enhancement motives broadly predicted heavy drinking and alcohol problems, and coping motives were rarely endorsed (particularly among drinkers with ADHD). We anticipated but did not find ADHD-related moderation of the effects of motives on our alcohol outcomes. (3) Manner of drinking strategies, but not limiting/stopping strategies, predicted heavy drinking and alcohol problems. Contrary to expectations, effects of strategies were similar irrespective of drinking motives or presence of a current ADHD diagnosis.
Heavy drinking and alcohol problems in students with and without ADHD
Table 1 and Figure 1 show that rates of heavy drinking, and alcohol problems appeared to be lower in students with ADHD compared with non-ADHD peers. Although tests of pairwise differences between groups showed meaningful effect sizes, these differences were inconclusive for failing to reach statistical significance. Our findings are inconsistent with results of several other studies showing more conclusively that alcohol consumption is similar between students with and without ADHD.20–22 Alcohol use disorders are also prevalent at similar rates in young adults with and without ADHD histories. 67 Instead, our results are consistent with findings of one other study that, like us, assessed student ADHD through their formal registration with campus disability services 23 —a process that requires considerable effort and may be more typical of academically conscientious students. In both cases, consumption rates by students with a current ADHD diagnosis were lower than students without ADHD. In our study, the largest difference (although nonsignificant) was found for alcohol problems, which numbered fewer in the ADHD group.
If the apparent differences in heavy drinking and alcohol problems in this study do reflect a pattern in the population of less severe drinking among university students with current ADHD, one reason may be social impairment in students with ADHD, 19 who tend to have fewer close friends and more social problems. 68 Adolescent social impairment was in one study associated with a reduced risk of heavy drinking in young adulthood, mediating the link between childhood ADHD and young adult heavy drinking. 69 Other drugs such as marijuana appear to be used at much higher rates by adolescents and young adults with childhood histories of ADHD. 70 Marijuana, rather than alcohol, may be sought out by young adults with ADHD for its anxiolytic properties and potential to lessen symptoms.71,72 In university students, current and childhood ADHD symptoms were associated with more frequent and severe cannabis use in one study, 73 but in another study were not. 21 Research on motives, cognitive processes, and differences in perceived consequences of alcohol, marijuana, and other illicit drug use may illuminate differences in alcohol and other substance use mechanisms for students with and without ADHD.69,74,75
Drinking to enhance, but not to cope, predicts heavy drinking and alcohol problems
Prior research shows that coping motives are consistently linked to problematic alcohol use, 76 but not typical alcohol use.29,30,60 Our study was the first to test associations between drinking motives and alcohol outcomes in university students with ADHD. Coping motives were unrelated to heavy drinking and alcohol problems, although Figure 1 shows that the distribution of coping motives appears more severe for students with alcohol problems. Instead, enhancement motives consistently predicted increases in rates of heavy drinking and alcohol problems for students with and without ADHD. We anticipated, but did not find, ADHD-related moderation of the effect of enhancement motives on alcohol outcomes. On the contrary, Figure 1 shows considerable variability in endorsement of enhancement motives among students with ADHD coded as drinkers or as meeting criteria for alcohol problems. For students with ADHD (at least those taking advantage of social opportunities for drinking), alcohol may serve a similar, predominantly social function as observed in the general student population.4,6 This interpretation is consistent with results of a recent meta-analysis showing that people with childhood histories of ADHD report similar rates of alcohol use experience by late adolescence to early adulthood. 70
Our preliminary evidence suggests that students with ADHD drink less and endorse few coping motives (see Figure 1), but we did not find evidence that coping motives were related to alcohol outcomes in a different manner compared with students without ADHD. One observation from Figure 1, however, is that coping motives were virtually absent among students with ADHD who were coded as heavy drinkers and/or as meeting criteria for alcohol problems. Just one person—a heavy drinker with an AUDIT score ⩾8 who also had an ADHD diagnosis—scored above the midpoint of the coping measure, compared with 21 of 77 students without ADHD (27%) who were coded as heavy drinkers and/or as meeting criteria for alcohol problems.
There were no significant interactions between motives, ruling out the possibility that students endorsing both high coping and high enhancement motives might be most likely to exhibit either heavy drinking or alcohol problems. In other words, enhancement motives predict alcohol problems irrespective of students’ coping motives. Students low on both types of motives are relatively unlikely to drink or to endorse alcohol problems, suggesting an overall lack of motivation to drink, less interest in drinking, and less actual consumption.
Manner of drinking, but not limiting/stopping, predicts heavy drinking and alcohol problems
In this study, manner of drinking strategies (e.g., avoiding mixing types of alcohol) predicted lower odds of heavy drinking and alcohol problems. Limiting/stopping strategies (e.g., stopping drinking at a predetermined time) were not related to either alcohol measure after controlling for manner of drinking strategies. This finding aligns with results of several other studies showing that manner of drinking strategies consistently predict alcohol outcomes while limiting/stopping strategies either do not predict39,77 or predict alcohol-related harms. 78 A limitation of protective strategy measurement is that students’ goals or expected outcomes following their use of protective strategies is not typically measured, 79 and students may not necessarily implement protective strategies for the sole purpose of reducing negative effects of alcohol. One perspective is that students may engage in certain protective strategies to deliberately become intoxicated. Heavy drinking provides social rewards, 80 particularly in college, and limiting/stopping strategies such as alternating alcoholic and nonalcoholic drinks might serve to extend and control students’ participation in alcohol-saturated events. 52 Manner of drinking strategies, however, explicitly reference avoidance behaviors and not taking part in the kinds of alcohol use likely to lead to negative consequences (e.g., mixing alcohols, drinking games).
We anticipated that poorer self-regulation and greater impulsivity typical in ADHD would impair students’ ability to implement protective strategies to limit their consumption, but it may be that the kinds of explicit, controlled processes measured by a typical PBSS are not well aligned with how students with ADHD make decisions about alcohol in practice. In other research, alcohol expectancies, or beliefs about the positive and negative effects of alcohol on mood and behavior, were lower in adolescents with childhood ADHD compared with adolescents without ADHD. 81 Students with ADHD may view protective strategies differently from students without ADHD, and their alcohol-related decision making may be driven by implicit, automatic processes not measured in this study. Such a possibility is a fertile area for future research and may have implications for on-campus interventions, many of which feature strategies for moderating drinking behavior.47,82
Study limitations
The principal limitation of this study was its small sample (n = 31) of currently diagnosed students with ADHD—a consistent limitation in this literature to date, with sample sizes ranging from n = 24 to 92—compared against a convenience sample of students drawn from introductory psychology courses. Parent reports and measures of impairment may be useful in increasing ADHD sample sizes in future research, as studies show that young adults dramatically underestimate their symptoms and impairment.12,83 Indeed, many young adults, including college students, with childhood ADHD histories no longer classify for a current diagnosis based on symptom criteria but are still impaired, 84 and these students were not captured in this study nor in prior studies comparing alcohol use in students with and without ADHD.
However, our findings (albeit inconclusive) that rates of heavy drinking and alcohol problems appeared to be lower in students with ADHD are consistent with results reported by Janusis and Weyandt, 23 who suggested that prescription medication use by students with ADHD may have lowered impulsivity and improved self-regulation. A limitation of our study was that stimulant medication use was not assessed, so we are not able to rule out its possible impact on reducing some of the deficits associated with ADHD that might be linked to alcohol use and decision making.
A final limitation of this study was that participant demographics could not be linked to key study variables due to data entry error. This precluded us from including biological sex in our analyses, an important omission given recent data showing a persistent gender gap over time in college student heavy drinking. 85
Conclusions
Overall, results of this study provide an encouraging direction for future study of the roles of drinking motives and protective strategies in explaining drinking patterns of students with and without ADHD. An important general finding was that enhancement motives are a potent predictor of alcohol problems for all students. The relative absence of coping motives, compared with considerable variability in enhancement motives among student drinkers with ADHD, tentatively suggests that students with ADHD are motivated to drink for similar reasons as students in the general population: frequently to enhance, but rarely to cope.
Students with ADHD also did not meaningfully differ from their non-ADHD counterparts in endorsement of protective behavioral strategies. Future research may benefit from a critical examination of protective strategies as a mechanism for changing alcohol behaviors in students. 79 For students with ADHD, in particular, protective strategies may not be an appropriate proxy measure of self-control or executive function. For example, underage drinkers in one study who set personal daily consumption limits and failed to drink within self-imposed limits felt more distressed and drank more on subsequent days. 86 Intentions for limiting drinking, in this case, worked against in vivo strategy implementation. In the absence of more conclusive evidence, it appears prudent at this time to recommend similar drinking prevention and intervention strategies for students with and without ADHD. In a larger sample, direct assessments of self-control or drinking-specific self-control and its relations to motives and depressive symptoms may help to clarify circumstances under which students with ADHD are differently vulnerable versus resilient to problematic alcohol use.
Footnotes
Acknowledgements
The authors are grateful to the staff at the Paul Menton Centre, Carleton University, for their assistance in reaching out to students with ADHD during our study recruitment.
Peer Review:
Six peer reviewers contributed to the peer review report. Reviewers’ reports totaled 4009 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
ALH designed the study, collected data, performed analyses, and wrote the manuscript. TRP assisted in writing the introduction and discussion sections.