
Abstract
Alcohol consumption increases longer-term health risks, including cancer. Many adults at midlife in Aotearoa New Zealand drink frequently but may not be aware of such risks. This study examined midlife adults’ awareness of alcohol and health risks and their knowledge of government low-risk drinking guidelines. A convenience sample of 502 adults (aged 40–65 years; 70% female) completed an online questionnaire. Almost all respondents reported they were aware of health risks associated with alcohol consumption. When unprompted, 41% of the sample named cancer as a health risk; when asked if they knew that alcohol use was associated with cancer, 61% agreed. For one-third of these respondents, this awareness did not motivate them to drink less. Most knew government drinking guidelines existed although did not know what they were. To support midlife adults to drink less, we need more insight into how they make sense of the long-term health risks of alcohol.
Introduction
Drinking alcohol is a leading risk factor for the global burden of disease (Murray et al., 2020; Rehm et al., 2017) yet it continues to be socially embedded in Western societies. Evidence demonstrates a link between alcohol consumption and increased risk for many health conditions including cancer. In 2020 an estimated 4.1% of all new cases of cancer globally were attributable to alcohol consumption (Rumgay et al., 2021), and it has been associated with mouth, throat, oesophagus, liver, colon, rectum and breast cancers (Connor, 2017; Connor et al., 2017; Rumgay et al., 2021). These risks increase with rising consumption levels and recent evidence suggests that there are no safe drinking levels in terms of cancer and heart health (Paradis et al., 2023; Rumgay et al., 2021). In Aotearoa New Zealand (NZ), approximately 4% (236) of all cancer deaths in 2012 among those younger than 80 years were attributable to alcohol consumption, with a higher loss of potential years of life for Māori, NZ’s indigenous people (Connor et al., 2017). Half of these deaths were attributable to consuming less than four standard drinks per day (Connor et al., 2017). More recent research using 2018 data found that 3.5% of all cancer deaths in NZ were attributable to alcohol, and of the overall 901 deaths attributable to alcohol in this study, 42% were from cancer (Chambers et al., 2024). Reducing alcohol consumption, even by a few standard drinks per day, would therefore reduce the number of deaths attributable to cancer (Connor et al., 2017; Rumgay et al., 2021).
Governments seek to encourage lower risk drinking through publication of official guidelines. To reduce the long-term health risks of drinking, NZ guidelines recommend that women drink no more than two, and men no more than three, standard drinks per week, with a total weekly limit of 10 standard drinks or women and 15 for men. To reduce risk of acute injury, the guidelines recommend no more than four standard drinks on a single occasion for women, and 5 for men. Despite these guidelines, there is evidence of high rates of consumption in older adults in NZ (Towers et al., 2017, 2018), with approximately one-fifth of past-year drinkers aged 45–64 years drinking hazardously in the 2022/23 year (assessed using the 10-item AUDIT scale; Ministry of Health/Manatū Hauora, 2023). Males, and Māori and Pacific people, were more likely to drink hazardously than others (Ministry of Health/Manatū Hauora, 2023). In Australia, approximately one-fifth of adults aged 45–64 years have been found to exceed long-term risk drinking guidelines and also engage in risky single episode drinking (Australian Bureau of Statistics, 2023).
Survey research conducted with adults (18+) in NZ in 2001 and 2015 showed that there was an increase in awareness of the alcohol-cancer link, from 7.6% to 13.8% of the sample (Richards et al., 2017). In a 2023 NZ survey, 18% of respondents stated that alcohol is related to cancer risk when unprompted and 64% when prompted (Peniamina et al., 2023). Similarly, only one in five Australian adults mentioned cancer when asked about the health risks of alcohol (Tabbakh et al., 2021). When prompted about specific health conditions, however, 26% agreed that alcohol was a risk factor for throat and mouth cancer and 18% for breast cancer; 85% believed that alcohol could cause liver cancer. A UK survey conducted in 2023 found that 45% of adults had a spontaneous recall of the alcohol-cancer link (Whitelock, 2023). While these studies indicate increasing awareness of the alcohol-cancer link, they also suggest that alcohol is often not immediately perceived as a long-term risk factor for cancer.
It is unclear whether improving public awareness of the alcohol-related risks for cancer is effective in changing people’s drinking behaviour. In a 2020 Australian alcohol poll, 51% of respondents reported they were aware that alcohol consumption caused cancer, although only 57% of these people said that this motivated them to drink less (Foundation for Alcohol Research and Education, n.d.). Further, fewer of the midlife and older drinkers (49% of those aged 35–50+) said it motivated them to drink less compared to younger drinkers (67% of those aged 25–34).
There is a paucity of knowledge about midlife adults’ knowledge of NZ government low-risk drinking guidelines, their awareness of the health risks of drinking alcohol, including cancer and how such awareness may inform their decisions about drinking alcohol. The current study was designed to address this knowledge gap and provide insights that could support midlife adults to reduce their consumption and therefore longer-term health harms. We examined midlife adults’ drinking practices, their unprompted views about alcohol and health risks (including cancer), their knowledge of government guidelines for safer alcohol consumption, and explored whether their knowledge about the risks motivated them to consume less alcohol.
Methods
This questionnaire-based, cross-sectional, self report study received ethical approval from Victoria University of Wellington’s Human Ethics Committee.
Questionnaire: An online questionnaire was developed in Qualtrics, piloted with 6 midlife adults for sense and understanding, and refined. The final questionnaire included the following sections:
Demographics: Age, gender, ethnicity, sexuality, work status, qualifications, household composition, relationship status, parental status, caregiver status, household income.
Drinking practices: The 3-item AUDIT-C scale (comprising the first three questions of the 10-item AUDIT scale) asked about frequency and amount of drinking. AUDIT-C scores greater or equal to 3 are considered to warrant additional screening for alcohol problems in women and greater or equal to 4 in men (Reinert and Allen, 2007). Six additional items asked about when and where respondents drank alcohol, who they drank with and what they drank.
Drinking motivations: 7 items asked respondents for open-text responses about why they drink alcohol, their drinking preferences, what makes them feel/not like drinking, what makes it easy/not easy to drink.
Perceptions of alcohol and health risks: 6 items asked participants if there were health risks associated with alcohol, what these were (unprompted, open text response), how often they think about health risks and if they were aware that alcohol causes cancer. Those who stated there were aware were then asked which cancers have been linked to alcohol consumption (5 listed, open text to provide others) and whether this knowledge motivates them to drink less. All participants were asked if they were aware of the Ministry of Health guidelines to reduce health risks from alcohol use.
Changes in drinking: Participants were asked if they had thought about reducing their drinking, why, what would help/make it difficult, if they had reduced their drinking in the past and why.
Recruitment & procedure: We recruited a convenience sample of adults at midlife, which we defined as those aged between 40 and 65 years, through social media and personal and professional networks during 2022. The landing page outlined the purpose of the study and eligibility for participation (aged between 40 and 65 years). Willing participants indicated their consent. All responses were anonymous. 555 people responded to the questionnaire. Data were screened and 53 respondents were excluded (4 whose IP addresses were identified as spam, 3 who indicated never drinking alcohol, 32 who completed the survey in under 1 minute, 14 who had incomplete responses on over 90% of the questions).
Sample: The final sample consisted of 502 midlife adults aged between 40 and 65 years, with the majority between the ages of 40–55 years (mean = 50.3; SD = 6.9). There were more women (70.1%) than men (28.1%) or other genders (1.4%). Most respondents identified as New Zealand European/Pākehā (81.5%), with others identifying as Māori (9.2%), or another ethnicity (8.2%). Almost 80% of the sample reported having children, and of these, 73.1% reported that one or more of their children lived with them at least some of the time. An overview of the sample demographics is provided in Table 1.
Respondents’ demographic information.
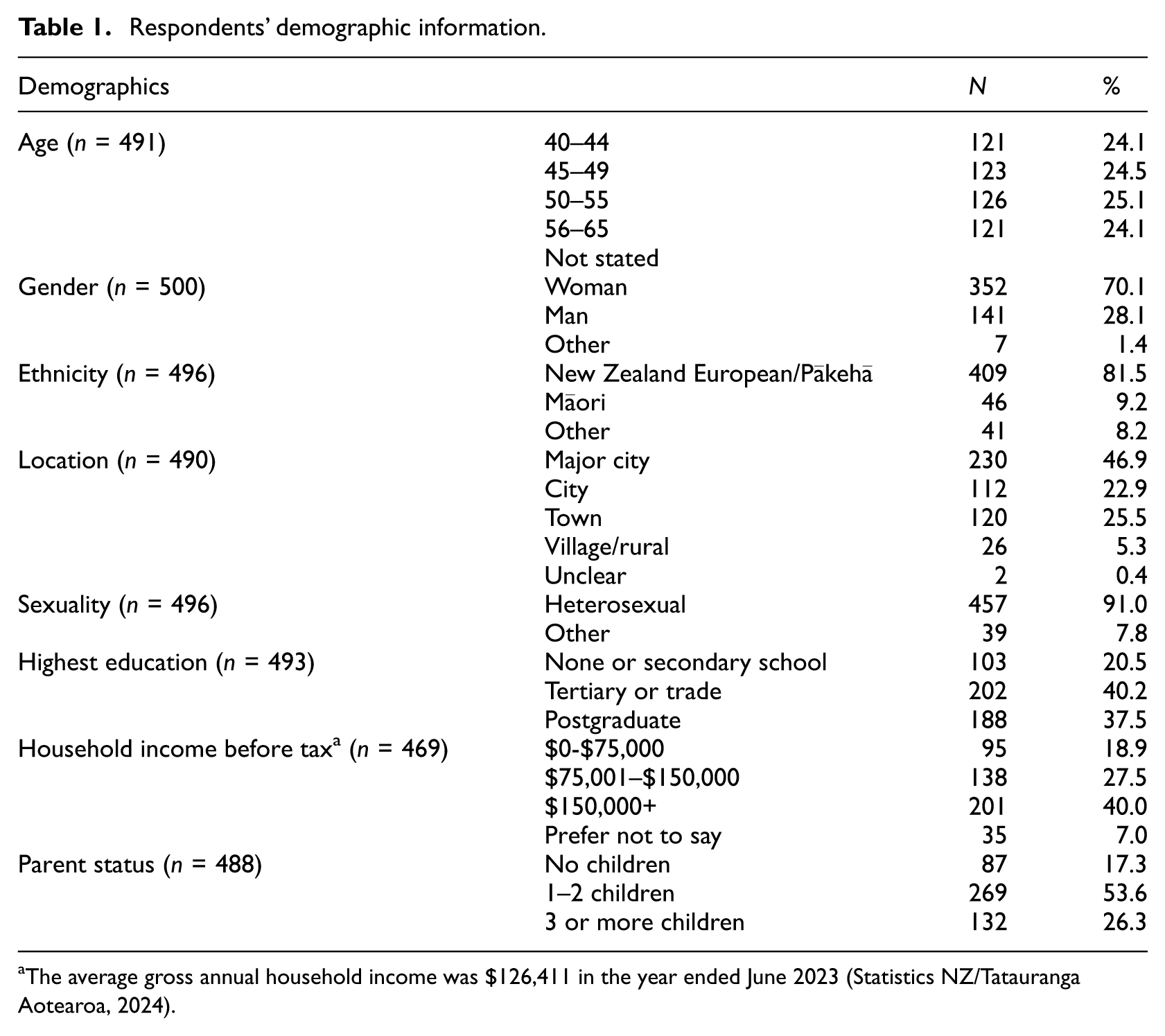
The average gross annual household income was $126,411 in the year ended June 2023 (Statistics NZ/Tatauranga Aotearoa, 2024).
Analyses: Questionnaire data were exported to STATA for screening and analysis. A series of descriptive analyses were undertaken to describe drinking practices, views about alcohol and health risks, knowledge of guidelines and motivations to consume less alcohol.
Results
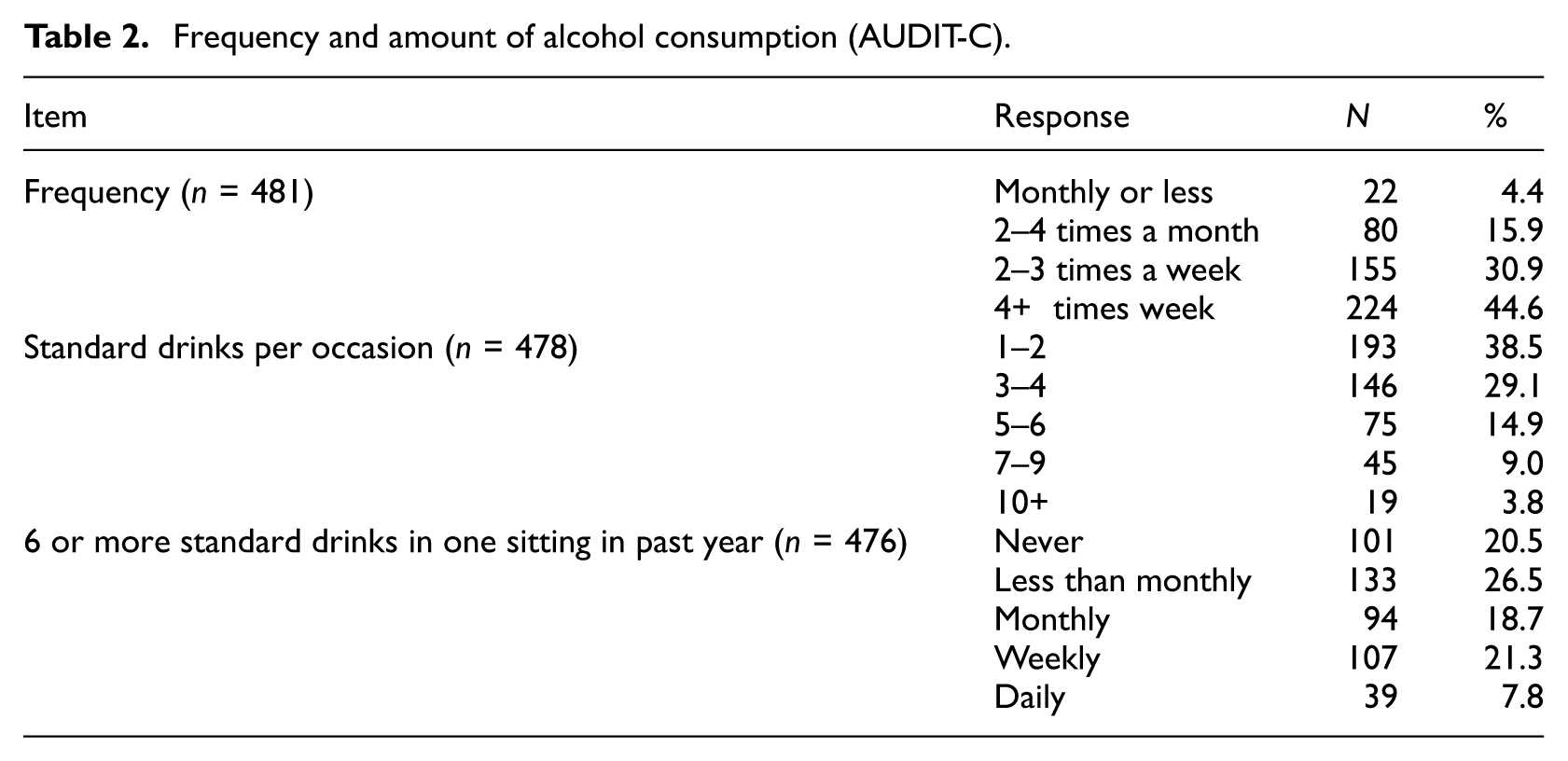
Patterns of alcohol consumption within this convenience sample are displayed in Table 2. Almost half (44.6%) reported drinking more than 4 times per week, and 61.5% reported that they drank three or more drinks per occasion. Almost a third of respondents indicated that they drank six or more standard drinks in one sitting either weekly or daily in the past year. The three AUDIT-C questions were summed and scores ranged between 1 and 12 (mean = 6.0, sd = 2.6), with higher scores in men (mean = 6.5; sd = 2.74) than women (mean = 5.8; sd = 2.5) and other genders (mean = 5.3; sd = 3.4). Eighty-five percent of women, and 76% of men, had scores that were at or above the AUDIT-C cut-off for hazardous drinking.
Frequency and amount of alcohol consumption (AUDIT-C).
Almost all participants (96.8%) responded that there were health risks associated with drinking alcohol (2.3% said there weren’t; 0.9% said they did not know). These respondents were then asked to provide a list of the health risks associated with drinking alcohol (unprompted, open text response). Almost a quarter of respondents listed five or more health risk outcomes; these are shown in Figure 1. Most commonly mentioned was cancer (by 41% of respondents) followed by cardiovascular disease (40% of respondents). Participants who listed health risks were also asked how often they had thought about these risks in the past month; almost half (46.5%) reported they had never thought about them, or only thought about them once. A small group of respondents (5.5%) stated they thought about the health risks every day.
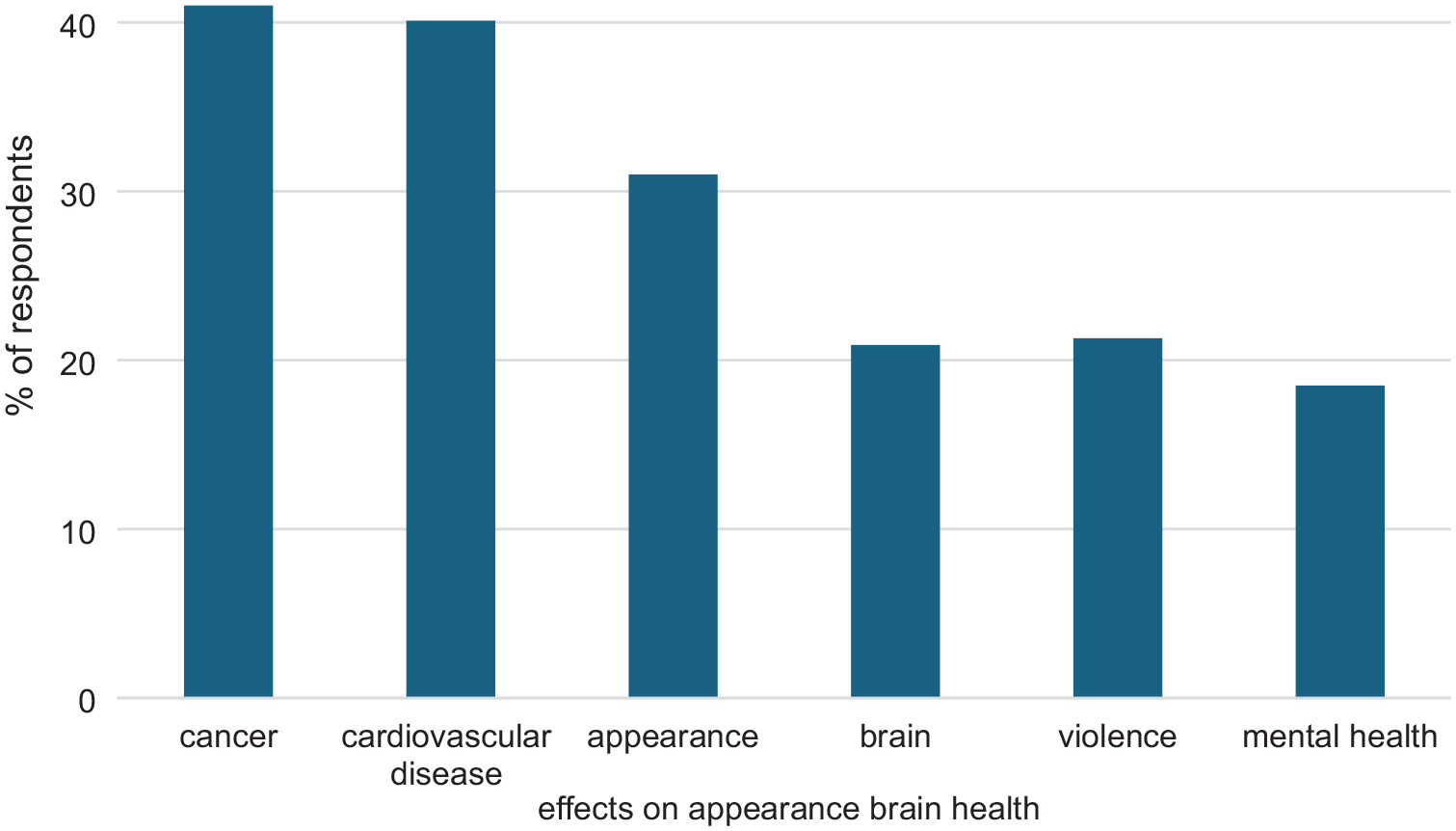
Common health risks that respondents associate with alcohol consumption (open text, unprompted; N = 436).
When asked directly if they were aware that alcohol causes cancer, 61% of respondents (265/432) stated that they were aware; 16.4% responded maybe; a fifth stated they were not aware (19.9%); and 2.3% said they did not know. Respondents who responded yes and maybe were then given a list of seven cancers and asked which had been linked to alcohol consumption. Responses are shown in Figure 2. Half stated that all of the cancers listed were linked to alcohol. Liver cancer was identified most often.
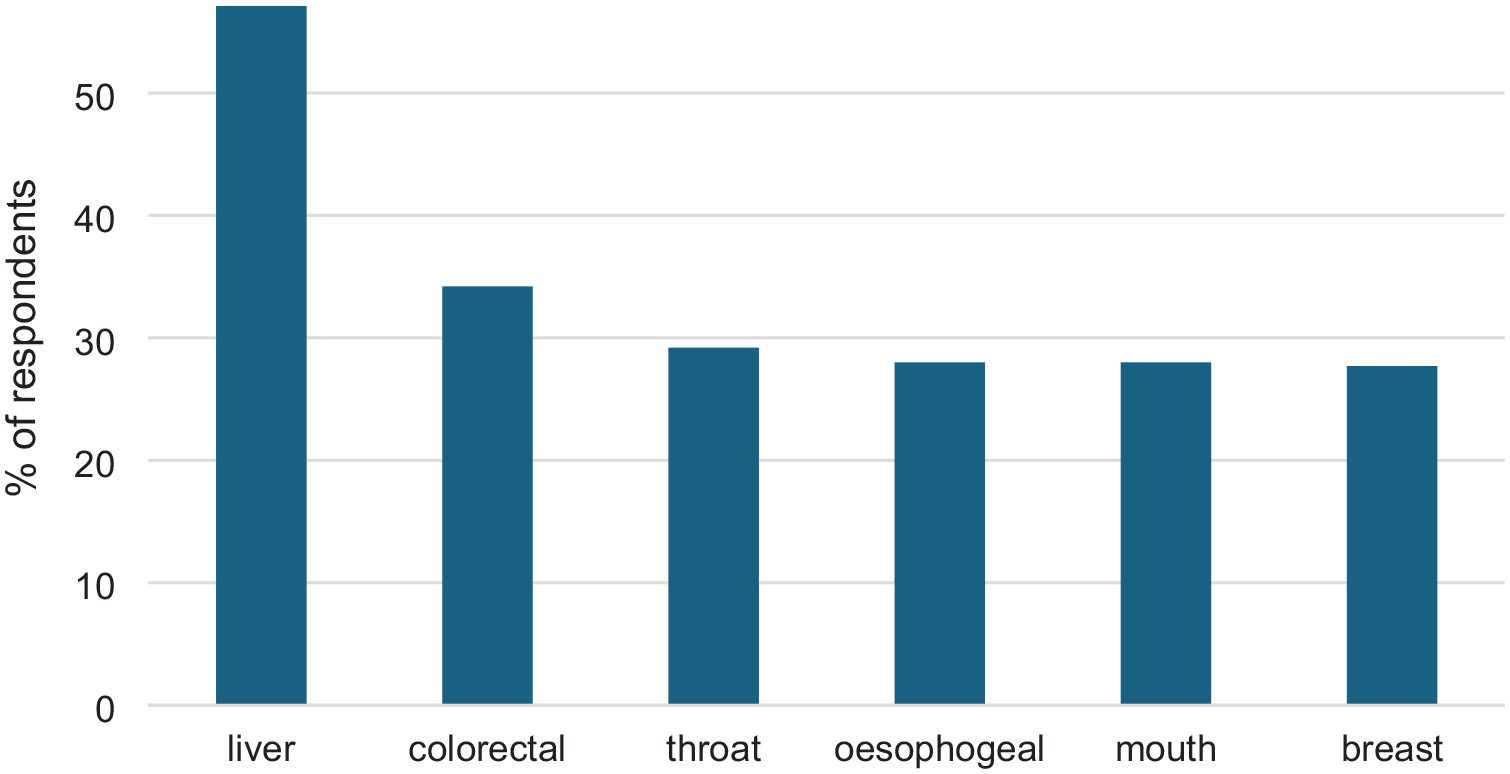
Respondents’ views on cancers linked to alcohol consumption (N = 336).
Respondents were asked if their knowledge about cancer risks motivated them to drink less alcohol and findings are shown in Figure 3. Almost 40% of respondents stated their knowledge about cancer risk and alcohol did not motivate them to drink less.
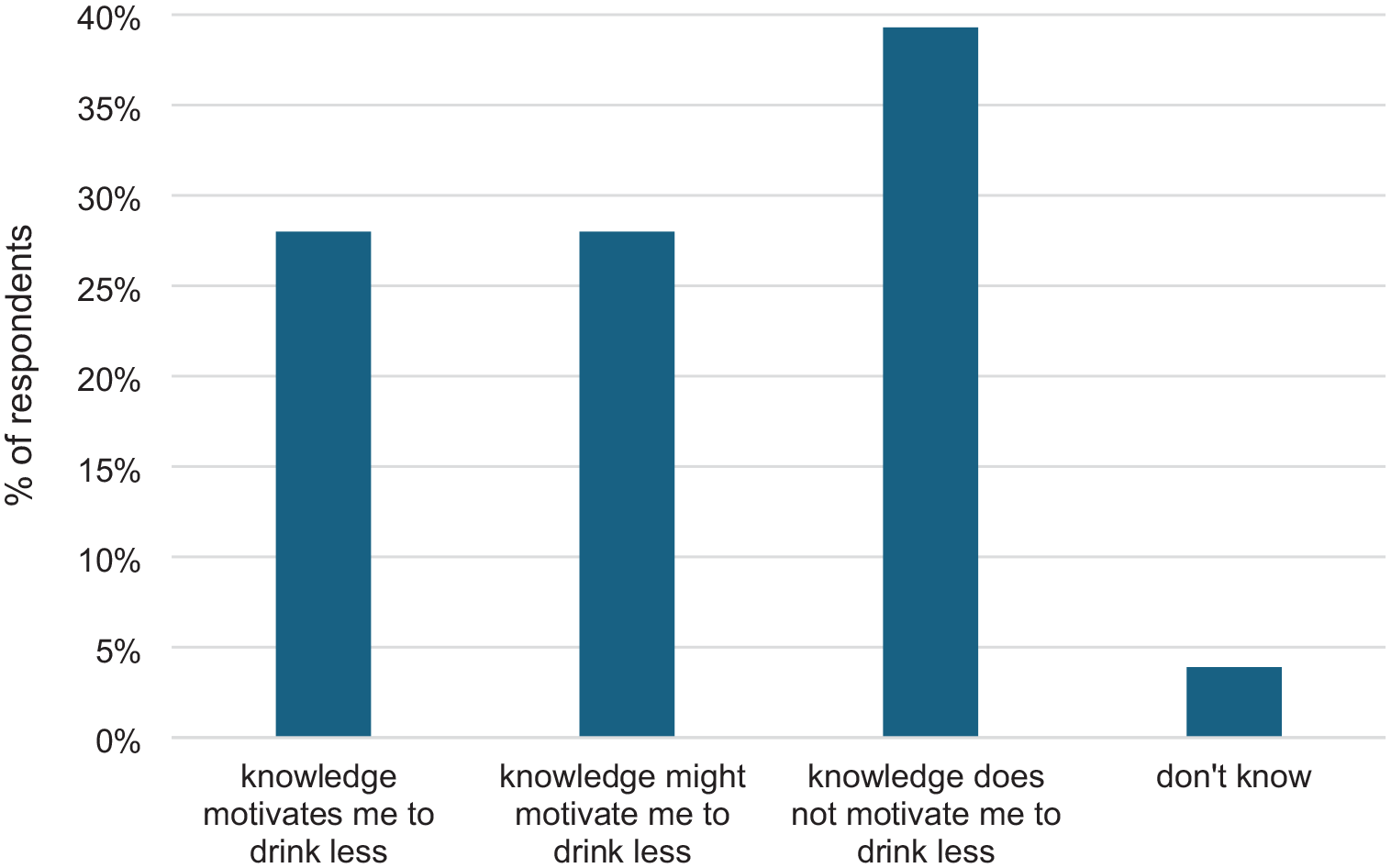
Knowledge of cancer risks of drinking alcohol motivating respondents to drink less (N = 335).
All participants were asked about their awareness of the Ministry of Health guidelines to reduce health risks from drinking alcohol. Responses are shown in Figure 4. Almost a quarter were not aware of the guidelines, while a quarter said that they were aware and familiar with the content. Half were aware of the guidelines but not the specific recommendations.
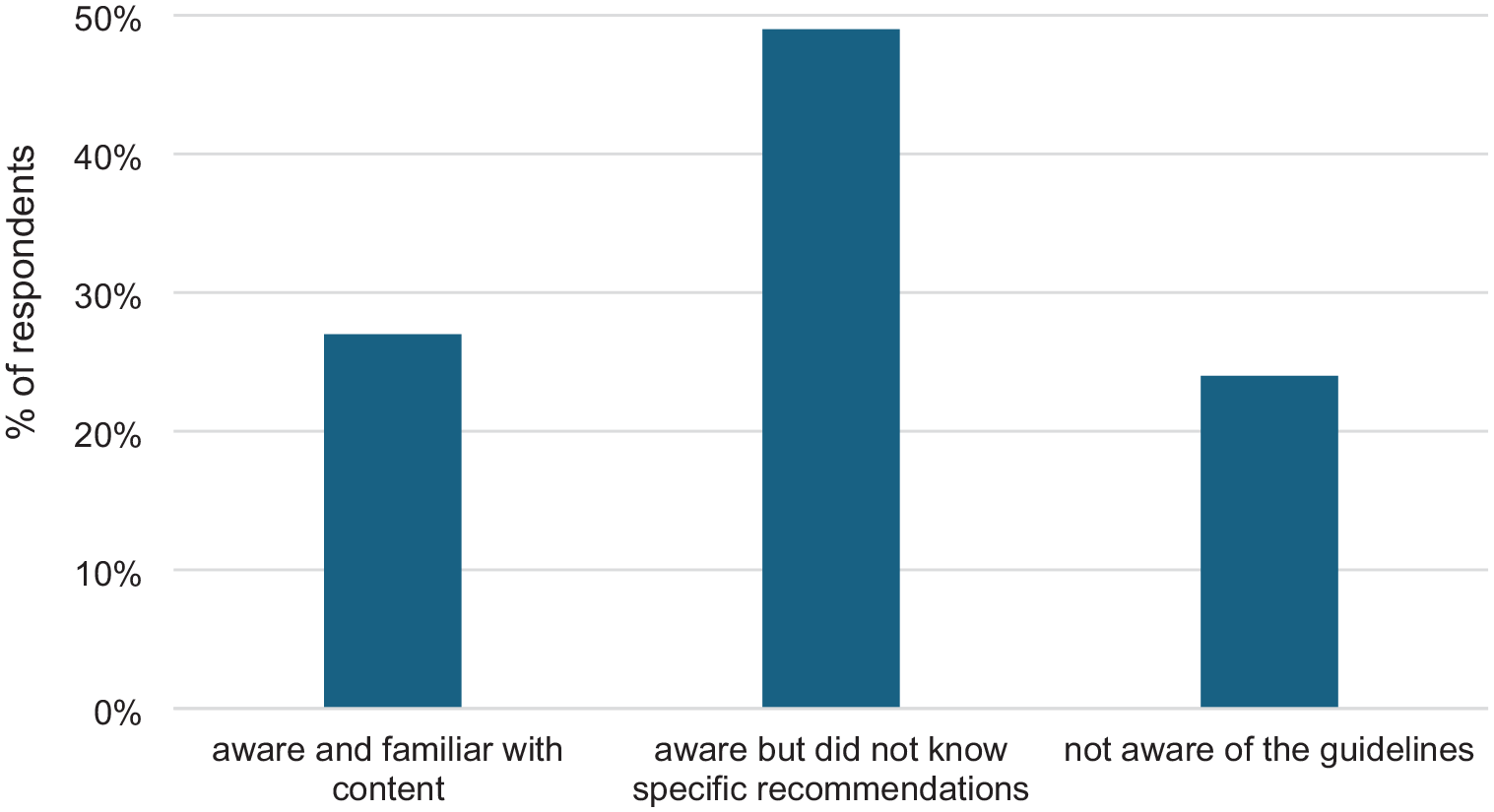
Respondents’ awareness of government low-risk drinking guidelines (N = 432).
Respondents were also asked if they would like to drink less than they currently do, and 56% reported they would (19.4% would like to drink a lot less, and 36.9% would like to drink slightly less), while 41.2% reported they did not want to change the amount they currently drink.
Discussion
Midlife adults in this convenience sample (with a high proportion of tertiary-educated respondents) reported relatively high levels of alcohol consumption. Their AUDIT-scores showed that over 75% were drinking at levels that warranted further screening for problematic alcohol consumption (Reinert and Allen, 2007. Almost three-quarters of respondents drank at least twice a week; almost a third reported they drank more than 6 standard drinks in a sitting, at least once a week. Over half of this sample (56%) reported they would like to drink less alcohol than they do currently, with one-fifth stating they would like to drink a lot less.
Almost all respondents stated there were health risks associated with drinking alcohol. Cancer was the most frequently unprompted named risk, although it was named by less than half of respondents. While this is higher than previous findings in NZ, the UK and Australia, a 2023 survey with 1425 NZ adults found that that only 18% of respondents identified alcohol with a risk of cancer. These differences may be attributable to differences in the age and education levels within the samples. However, other findings were similar to this previous study with 60% of participants being aware of the cancer and alcohol risk when prompted. How this knowledge relates to drinking behaviours, and intentions to reduce consumption, is important. We asked our respondents directly about whether this knowledge motivated them to drink less. For many (almost 40%) it did not, although it did for over a quarter of the sample (28%). Research from Australia has also found that knowledge about health risks does not have an impact on many people’s drinking practices (Foundation for Alcohol Research and Education, n.d.).
The current study does not tell us why many of the midlife adults were not motivated to reduce their alcohol consumption when they were aware of the longer-term health risks. Research shows that considering the risks of drinking competes with drinking as a socially embedded and culturally valued activity in Western societies. For adults at midlife, alcohol is linked positively with relaxing, coping, celebrating, socialising, connecting and having fun (Emslie et al., 2012, 2013; Foley et al., 2021; Jackson et al., 2018; Kersey et al., 2022; Lunnay et al., 2023; Lyons et al., 2023). Despite increases in consumption of no- and low-alcohol products and declining trends in young people’s consumption (Vashishtha et al., 2020), adults at midlife report finding it very difficult to not drink alcohol due to social and peer pressure (Bartram et al., 2017; Katainen et al., 2022). Research also shows that drinking alcohol is a social practice that is habitual and routinised within the lives of many adults at midlife (Lyons et al., 2023). More research is required to explore how people understand and negotiate risks around alcohol, particularly cancer and other long-term risks.
Furthermore, people may be unclear about what levels of alcohol consumption are linked with increases in cancer and other risks (Foley et al., 2024). While government drinking guidelines incorporate understandings of long-term risks (with an overall limit on number of drinks per week), many drinkers are unaware of the thresholds (Bowden et al., 2014; Buykx et al., 2018; Chapman et al., 2020; Rosenberg et al., 2017). In the current study, three-quarters of respondents were aware that the guidelines existed, but only a quarter knew what they said. A recent Australian survey similarly found that 65% of Australians knew that low-risk drinking guidelines existed, but only 26% were aware of their content (Foundation for Alcohol Research and Education, n.d.).
Government drinking guidelines to reduce harm from alcohol use vary across countries and have implications for health promotion. Many government guidelines state a recommended maximum number of drinks per week or occasion to reduce risk, which implies that that there is a level of drinking without risk (Davies et al., 2023; Mugavin et al., 2023). Drinking guidelines are currently set at levels higher than that understood to increase cancer risk, which is one of the reasons that the Canadian government has changed to a traffic light system, where drinking 1–2 drinks per week is categorised as low risk (Paradis et al., 2023). As governments around the world update their low-risk drinking advice based on recent evidence, we simultaneously need research that examines how people learn about – and make sense of – governmental guidelines on low-risk drinking.
The current study had a number of limitations, including its use of a convenience sample that was well-educated with relatively high-income levels, and more females than other genders. Findings cannot be generalised to the NZ population of midlife adults. The self-report nature of the data raise issues around the social desirability of responses; while many participants shared frequent and heavy levels of alcohol use, they may potentially be under-reporting. Additionally, some participants may not have wanted to state that even though they are aware of the alcohol-cancer link, they do not wish to reduce their drinking. Nevertheless it did capture midlife adults who are drinking frequently and at times heavily, and provides insight into their views on alcohol consumption, perceptions of health and cancer risks and motivations around reducing consumption.
To support adults at midlife to reduce their alcohol consumption, we need greater insights into their drinking practices, their own conceptualisations of the longer-term risks of alcohol consumption and their views on government guidelines. Health promotion would benefit greatly from knowing why it is so difficult for many midlife adults to reduce their drinking, even when they would like to drink less. Government policy could support health professionals to discuss drinking with midlife adults (Agabio et al., 2021; Donat-Vargas et al., 2021). We also need to be implementing evidence-based policy shown to reduce alcohol consumption through regulating the availability, accessibility, affordability and marketing of alcohol to negate the normalised role of alcohol in everyday lives. International evidence demonstrates the success of such policies (Public Health Scotland, 2023; Rehm et al., 2023).
Footnotes
Acknowledgements
We would like to thank Dr Timea Partos for her analytic work in earlier stages of this project.
Author contributions
All authors contributed to study design, conduct, analysis and drafting revisions. It was not pre-registered.
Data sharing statement
Data is not available for sharing from this study as participants only gave consent for the named researchers to have access to their data.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a research grant from Cancer Society New Zealand.
Ethics approval
The study received ethical approval from the Victoria University of Wellington Human Ethics Committee reference number 0000029785.
Informed consent
Willing participants indicated their consent online prior to completing the survey.