
Abstract
Background:
The quality of caregiving in mothers with substance abuse problems appears to be compromised. However, divergent findings, methodological variability, and sample characteristics point to the need for research synthesis.
Methods:
A comprehensive systematic search was undertaken. Studies were eligible if they (1) compared substance-misusing mothers with non–substance-misusing mothers, (2) involved children from birth to 3 years, and (3) maternal sensitivity and child responsiveness were measured using observational methodology.
Results:
A global meta-analysis for maternal sensitivity (n = 24 studies) and child responsiveness (n = 16 studies) on 3433 mother-infant dyads yielded significant population effect sizes and significant heterogeneity. Subgroup analyses found reduced heterogeneity when the meta-analysis was conducted on studies where groups were matched on key demographic characteristics; although the effect size was small, it was still significant for maternal sensitivity but not child responsiveness.
Conclusions:
Compromised quality of caregiving is found in high-risk, substance-misusing mothers, emphasising the importance of early intervention that draws from attachment-based interventions.
Introduction
The developmental outcomes of children living in families with illicit parental substance use are significantly compromised with difficulties initially identified in early infancy extending throughout childhood and into adolescence. 1 Many areas of children’s functioning are compromised, including early interaction with caregivers resulting in elevated rates of insecure and disorganised attachment,2,3 and performance on tests of cognitive functioning4–6 and language.7,8 The compromised caregiving seen in mother-infant dyads 9 has been implicated in poor outcome and high rates of disorganised and insecure attachment. 10 These difficulties extend into childhood with evidence of difficulties in a range of executive functions 11 and higher-than-normal rates of internalising and externalising disorders.12–14
Extensive research indicates that many of these difficulties are influenced by exposure to an early caregiving environment that lacks sensitive, contingent, and responsive maternal caregiving behaviour. 15 For example, maternal insensitivity is associated with long-term difficulties,16,17 including conflict within parent-child relationships18,19 and internalising and externalising disorders at 5 years of age 20 and beyond. 21
There has been considerable investigation of the quality of caregiving in substance-misusing mothers, although there is also wide variability in the way in which the quality of caregiving has been measured across studies. Substantial variability in sample size, populations studied, and quality of the study design has contributed to mixed findings. An early narrative review of research studies published between 1990 and 1999 by Johnson 9 provided an integrative synthesis of 23 studies in which mother-infant interaction had been measured. Fifteen of these studies were longitudinal or cross-sectional in design and focused on correlational associations between maternal characteristics and quality of caregiving. Notably, only 8 studies were included where there had been a direct comparison of mother-infant interaction in substance-misusing and non–substance-misusing mothers. Although 6 of these studies found poorer quality caregiving in the substance-misusing mothers, 2 found that substance-misusing mothers did not differ from a nonsubstance comparison group in their interactional style,22,23 with both studies using a comparison group that was matched on demographic characteristics.
Since Johnson’s 9 review, studies have continued to show differences in the quality of caregiving.24,25 LaGasse and colleagues 24 found that cocaine-using mothers were significantly poorer on 3 of 5 measures of maternal behaviour during feeding with their 1-month-old infant compared with non–substance-using mothers. Prenatal cocaine exposure was associated with poorer ratings of mother-child interactions measured at 3 years of age. 26 Mother-child interactions were poorest for children with prenatal cocaine exposure whose mothers continued cocaine use postnatally, compared with children whose mothers did not use cocaine during pregnancy or at a 3-year follow-up visit. Poorer emotional availability was observed in a study of opioid-dependent mothers and their 7-month-old children compared with non–substance using mothers. 27 Women who were polydrug and cocaine users during pregnancy have also shown greater dyadic conflict during feeding interactions. 28 Contrary findings by Ukeje and colleagues 29 found compromised care in both substance-misusing mothers and a matched comparison group. Thus, it is possible that the poor-quality caregiving relationship found in some studies may be more related to the accumulation of adverse environmental risk than maternal substance use per se.30,31
In summary, there is inconsistency in the results of studies addressing the quality of caregiving in mothers who have used illicit substances. One methodological issue that emerges from our reading of the literature that may potentially help explain discrepant results relates to study design. Studies with greatest methodological rigour have compared substance-misusing mothers with mothers facing similar environmental adversity, whereas those that are less methodologically robust have drawn the comparison group from a general population of mothers. However, studies also varied on other factors, such as the age of children, when the quality of caregiving was assessed. Finally, mothers who are engaged in treatment, and particularly residential treatment, may show less compromised caregiving as many treatment services, particularly residential programmes, may have addressed parenting as part of the treatment process. Thus, associated improvements in well-being32,33 and parenting practices 34 may influence the quality of caregiving.
The aim of this study is to assess the extent to which mothers with substance misuse have compromised caregiving. This builds on existing narrative reviews and extends this literature by providing a comprehensive systematic review and meta-analysis of studies that have compared the quality of parent-child interactions (maternal sensitivity and child responsiveness) in illicit substance-misusing and nonmisusing groups. Illicit substance use was the focus of this review as there is a range of legal, environmental, and lifestyle risks accompanying illicit substance use in women which makes them qualitatively different from women with tobacco or alcohol problems. 35 The primary aim of this study was to investigate the quality of caregiving relationship in mothers with substance use problems (including those on opioid replacement therapy) by comparing measures of maternal sensitivity and child responsiveness with mothers who did not have a substance misuse problem. The second aim was to examine factors (moderators) that could influence the quality of the caregiving relationship.
Methods
Studies
Studies were included in the review if they included all of the following elements: mothers of children aged birth to 3 years, mothers who were current illicit substance misusers and/or were on opioid replacement therapy due to a history of opioid dependence and/or were in residential treatment due to a history of illicit substance use, and a comparison group of non–substance-using mothers; there was an assessment of maternal-child interactions using an observational method that was videotaped and subsequently coded to assess the quality of maternal caregiving.
Outcomes
The primary outcome measure was maternal sensitivity. This was operationalised as a maternal response to infant or child cues related to maternal warmth in situations of low frustration rather than during situations of frustration or negative affect. 36 The measure of maternal sensitivity was extracted from a range of observational tasks that included free play, structured play, and infant feeding observations. Thus, we selected scores on observational coding systems that explicitly measured maternal behaviour and affect using terms such as ‘talks to infant’, ‘shows pleasure towards infant’ and ‘appears cheerful’,37(p4) ‘responding to the child’s activity and interests (sensitivity/pacing), positive feelings shown to the child’.38(p557) The secondary outcome measure was child responsiveness. This was also required to have been explicitly included as a scale or construct measured in the observational system that rated infant or child responsiveness directly, such as ‘involvement with the mother, positive feelings shown to mother’,38(p557) and ‘child responsiveness indicates how well infant responds to maternal bids and expressions’.27(p250)
Given the diversity of study populations, we identified 3 potential sources of heterogeneity across studies to test in subgroup analyses: (1) study design (groups matched on key demographic variables vs studies comparing substance-misusing mothers with a general population group), (2) age of child (less than 12 months vs more than 12 months and up to 40 months), and (3) treatment (not in treatment vs currently in outpatient treatment, including opioid replacement therapy and/or residential treatment).
Search strategy
Search terms were identified by (1) an examination of indexing terms in relevant databases, and (2) a preliminary scoping of eligible studies prior to the systematic search. Search terms were combined together with Boolean OR and each set of search terms was then combined with Boolean AND to search across title, abstract, and keywords in each search location. There were no restrictions placed on document type. Search terms were (‘maternal substance use’ OR ‘maternal drug use’ OR ‘substance-using mothers’ OR ‘drug-using mothers’) AND (‘caregiving’ OR ‘care giving’ OR ‘interaction’). Studies were included if they were in English-language publications and the date range was from 1995 to 2015 (updated April 2016; see Figure 1) as this 20-year period reflects the steady increase in the use of cannabis and the growing use of crack cocaine and heroin that began in the early 1990s. 39 Studies were identified by searching the following electronic databases: Scopus, MEDLINE, ScienceDirect, PsycINFO, SpringerLink, and Google Scholar. The reference lists of existing reviews and eligible studies were harvested after completion of systematic screening to ensure capture of all eligible studies.
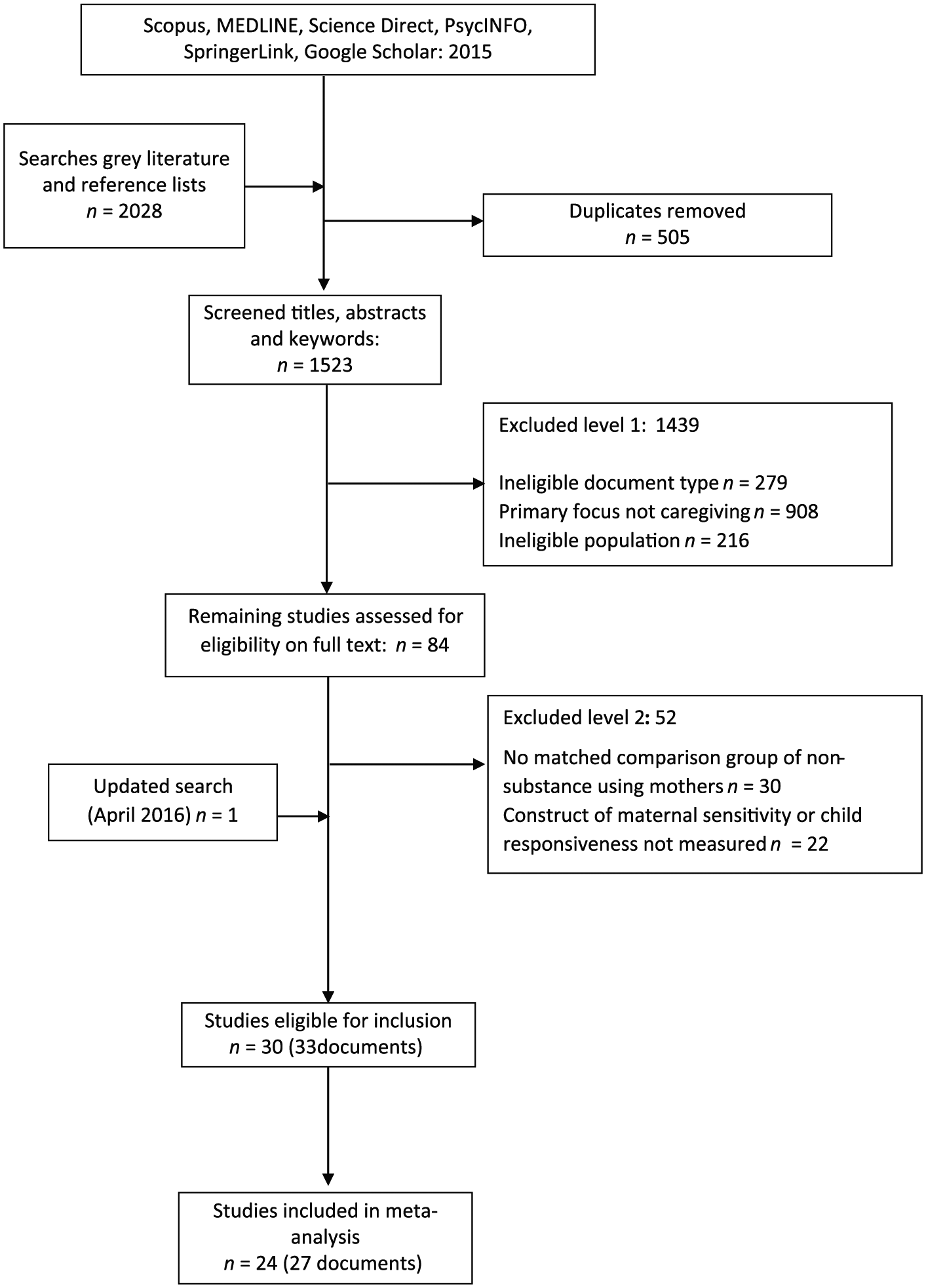
Selection process for eligible papers for systematic review and meta-analysis (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) 2009 flow diagram.
Study selection and data extraction
The literature search identified 2028 studies. Figure 1 provides a description of the complete selection and exclusion process using Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 40 guidelines. The PRISMA Statement was developed to enhance clarity and transparency of reporting in systematic reviews. It includes a detailed 27-item checklist that provides explanations of the key components that need to be determined in a systematic review and an additional 4-phase flow diagram that documents the decision-making process in the selection of studies for the review. 41 Search results were exported into EndNote Version X7 for Windows, and duplicates and ineligible document types (eg, books) were removed. The remaining records were imported into systematic review management software, SysReview, 42 for initial eligibility screening. Titles/abstracts/keywords were screened and the record was excluded if the title and/or abstract and/or keyword indicated that the document was not an eligible document type. Following the completion of title and abstract screening, a full-text review was undertaken and data were extracted in a standardised format following the PRISMA guidelines. 40 Of the remaining 84 articles, a further 52 documents were eliminated (level 2 exclusion), reducing the pool to 32 documents. One further study was identified during an updated literature search (April 2016) and included (see Figure 1).
These 33 documents reported the results of 30 unique research studies as 3 studies had reported on maternal sensitivity across different research reports. Finally, 6 studies were not included in the meta-analysis as data were not reported or not available from authors due to the passage of time (descriptive characteristics are included in Table 1). Therefore, data from 24 studies were included in the final analysis.
Participant characteristics including primary drug used, age, race, recruitment site, and description of maternal sensitivity and child responsiveness measures.

Abbreviations: ASI, Addiction Severity Index; BSID, The Bayley Scales of Infant Development–Revised; EAS, Emotional Availability Scale; FFSF, Face-to Face Still-Face; MIFS, Mother Infant Feeding Scale; MISU, Maternal Inventory of Substance Use; MLS, Maternal Lifestyle Study; NCAFS, Nursing Child Assessment Feeding Scale; NICHD, National Institute Child Health and Human Development Network; NICU, Neonatal Intensive Care Unit; OMT, Opioid Maintenance Therapy; ORT, Opioid Replacement Therapy; PC-ERA, Parent-Child Early Relational Assessment; PCOG, Parent-Child Observation Guides for Program Planning; RSIS, Rating Scale of Interaction Style; SES, socioeconomic status; THC, Marijuana; TLFB, Timeline Follow Back; VLBW, Very low birth weight.
Data synthesis, study quality appraisal, and analyses
Study quality was assessed using 9 items from the 14-item Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies (National Institute of Health). 65 The excluded items related to aspects of study quality that required a follow-up component (eg, attrition, number of follow-up points). The retained items are listed in Supplementary Table 1. All meta-analytical calculations were performed using Review Manager 5. 66 Standardised effect sizes (d) were calculated for the included studies. When data on maternal sensitivity were reported at 2 time points in the same document, data from the second time point were used (ie, 3 and 6 months 54 ; 3 and 12 months 59 ). On both occasions, the second time point was used as this was closer to the mean age of children across all studies. Two studies24,25 divided their sample into ‘heavy’ and ‘some use’, and we selected data from the heavy group as this reflected substance use patterns reported in other papers.
A random-effects model was used to calculate effect size due to expected heterogeneity in the studies. 67 Three potential sources of heterogeneity were identified a priori and 2 were subsequently investigated. The latter were as follows: (1) study design (groups matched on key demographic variables vs studies comparing substance-misusing mothers with general population) and (2) age of child (less than 12 vs more than 12 months and up to 40 months) in accordance with recommendations regarding subgroup analyses (Cochrane Handbook; Chapter 9.6.6). 68 It was not possible to test whether treatment was a moderator as most of the studies that were classified as ‘in treatment’ were also included in the subgroup ‘unmatched’.
A forest plot was calculated in Review Manager 5 (version: 5.3.5), and the heterogeneity between studies was assessed using the Q statistic and I2 index. Subgroup analyses were conducted to investigate sources of heterogeneity. Finally, sensitivity analyses using a priori weight functions were conducted to determine whether the estimates of effect size were likely to be influenced by publication bias.69,70
Results
Study characteristics and quality appraisal
Twenty-four studies that included a total of 3433 mother-child dyads met final inclusion for the meta-analysis. Of these, 15 studies reported that the mother’s primary drug of use was cocaine or a combination of cocaine and other drugs, whereas 9 studies reported that the primary drug was an opioid. Studies did not typically use diagnostic nomenclature to describe the study population. Thirteen studies provided information on quantity and frequency plus urine toxicology, hair analysis, and/or meconium testing; 1 study used clinical assessment to arrive at a diagnosis; 9 studies reported that mothers were being prescribed opioid replacement therapy as either an outpatient or were currently in a residential treatment facility; and 1 study used prenatal maternal urine toxicology reports to verify substance use. Of all the 17 studies reporting maternal substance use conducted in the United States, only 3 studies had a focus on mothers in treatment. Conversely, all studies conducted outside the United States were conducted in either residential treatment or outpatient opioid replacement clinics (ie, Finland, 4 studies; Norway, 2 studies; Australia, 1 study). The timing, identification, and assessment of substance use also differed between studies. Twelve studies identified and assessed mothers for substance misuse antenatally, 2 studies reported assessment of substance use both antenatally and postnatally, and the remaining (n = 10) assessed substance use postnatally. Studies were divided relatively equally between infants less than 1 year (n = 13) and infants more than 1 year (n = 11). The observational measures all included a measure of the construct of maternal sensitivity and consisted of Ainsworth’s Maternal Sensitivity Measure (n = 2), 71 the Parent-Child Early Relational Assessment (n = 6) (PC-ERA), 72 the Emotional Availability Scales (n = 4) (EAS), 73 and Still-Face Paradigm (n = 1), 25 and 11 studies used purposely designed measures of maternal sensitivity (see Table 1 for a description of studies).
There was relatively little variability in study quality, with all studies scoring a YES on key elements of design (eg, clearly stated research question, clearly defined population, and clearly defined independent and dependent variables (see Supplementary Table 1). The 1 item that showed variability related to study design, namely, were participants recruited from the same or similar populations. Fourteen studies scored a YES indicating that the samples have been drawn from the same population. However, 10 of the studies reported variations in sample characteristics and thus scored NO. This item was subsequently used to classify studies on the basis of matched or unmatched samples for later subgroup analyses.
Global analyses of maternal sensitivity and child responsiveness
A global meta-analysis of the 24 studies reporting maternal sensitivity yielded an overall population effect size of 0.46 (95% confidence interval [CI]: 0.31-0.61, Z = 5.99, P < .00001), indicating that maternal sensitivity was higher in non–substance-using mothers compared with substance-misusing mothers. Notably, however, the proportion of total variability explained by heterogeneity was high (Q(23) = 73.53, P < .00001; I2 = 69%).
Similar findings were obtained for a second global meta-analysis of the 16 studies reporting child responsiveness. The overall population effect size was 0.32 (95% CI: 0.06-0.59, Z = 2.37, P = .02), once again indicating that child responsiveness was higher in non–substance-using mothers compared with substance-misusing mothers. There was also significant heterogeneity across studies (Q(15) = 65.05), P < .00001), and the proportion of total variability explained by heterogeneity was high (I2 = 77%).
Moderation analyses to identify sources of heterogeneity
The significant heterogeneity did not allow any meaningful interpretation of the distribution of effect sizes across studies. 77 To investigate potential sources of heterogeneity, subgroup analyses were undertaken. The first of these was design, as the precision of effect sizes is related to methodological quality, including the matching of study groups. 78 Subgroup analysis for study design found that the overall effect size of maternal sensitivity for the matched subgroup was statistically significant (Z = 5.60, P < .00001) but small (0.28, 95% CI: 0.18-0.38; see Figure 2), whereas for the nonmatched subgroups, the overall effect size remained large (0.85, 95% CI: 0.48-1.22) and also statistically significant (Z = 4.47, P < .00001). A test for subgroup differences found that the lower estimate of effect size within the matched subgroup was statistically significant (Q(1) = 8.27, P = .004), and heterogeneity within the matched subgroup was significantly reduced and no longer statistically significant (Q(13) = 13.88, P = .38; I2 = 6%), whereas heterogeneity within the nonmatched subgroup remained high and statistically significant (Q(9) = 53.54, P < .00001; I2 = 83%).

Forest plot of maternal sensitivity for total sample (n = 24) grouped by study design (matched and nonmatched).
A similar but nonsignificant pattern was found for child responsiveness. The overall effect size of child responsiveness for the matched subgroup was not statistically significant (Z = 1.59, P = .11) and small (0.13, 95% CI: –0.03–0.29; see Figure 3), whereas for the nonmatched subgroup, the overall effect size remained large (0.79, 95% CI: 0.00-1.58) and statistically significant (Z = 1.96, P = .05). A test for subgroup differences found that the lower estimate of effect size within the matched subgroup was not statistically significant (Q(1) = 2.57, P = .11). Although heterogeneity within the matched subgroup was reduced, it was not statistically significant (Q(9) = 12.19(9), P = .20; I2 = 26%) and heterogeneity within the nonmatched subgroup remained high and statistically significant (Q(5) = 36.82(5), P < .00001; I2 = 86%).

Forest plot of child responsiveness for total sample (n = 16) grouped by study design (matched and nonmatched).
Overall, these results show significantly reduced levels of heterogeneity for estimates of effect size for both maternal sensitivity and child responsiveness when samples of substance-misusing mothers were compared with mothers matched on factors such as socioeconomic status, level of education, and (for US studies) eligibility for Medicaid. However, when substance-misusing mothers were compared with mothers drawn from the general population, the differences between the groups on maternal sensitivity and child responsiveness were observed to be significantly larger.
There were no effects of age on heterogeneity. Furthermore, consideration of the variable treatment (mothers in treatment vs not in treatment) was not pursued as the studies of mothers in treatment were also those with nonmatched design, indicating that any finding relating to heterogeneity would be confounded by design.
Publication bias
The existence of publication bias was evaluated by inspection of the funnel plots for maternal sensitivity and child responsiveness. A funnel plot is a scatterplot of effect size (x-axis) graphed against sample size (y-axis) centred on the true population effect size. In the absence of publication bias, studies with larger sample sizes would be expected to be closer to the true population effect size with greater variability of effect size estimates in studies with smaller sample sizes. Thus, when the values of effect size estimates are plotted, the values will be symmetrically distributed around the population effect size in the shape of a funnel. Visual inspection of the funnel plot for maternal sensitivity showed that 3 studies did not fall within the expected funnel shape. The Kendall τ, a test to detect the presence of publication bias, was found to be significant τ(N = 24) = .38, P = .01, suggesting publication bias. To assess whether the publication bias would differ when adjusted for publication bias, we used the procedure by Vevea and Woods 70 as described in Field and Gillett. 69 This procedure assesses how effect size estimates would change if selection bias was present using several models of possible selection bias. Adjusted parameter estimates ranged from .52 to .58, suggesting slightly lower overall effect size for maternal sensitivity after adjusting for publication bias.
Discussion
This systematic review and meta-analysis examined 24 studies with a combined total of 3433 mother-child dyads to compare quality of caregiving in mothers who were using illicit substances or were currently in treatment and/or prescribed opioid replacement therapy with the quality of caregiving in non–substance-using women. These findings provide a synthesis of the literature on the quality of caregiving in substance-misusing mothers and is the first quantitative analysis of caregiving quality in substance-misusing mothers. 9
Overall, the composite effect size based on the meta-analysis of all 24 studies indicated that maternal sensitivity and child responsiveness were higher in mothers who had not used illicit substances. However, we found considerable heterogeneity that limited meaningful interpretation of the results. 79 Therefore, we undertook an examination of potential moderators that might be influencing the variability in effect sizes between studies using subgroup analyses. The first moderator to be tested was design. Smaller effect size values were observed for maternal sensitivity but not for child responsiveness in studies in which substance-misusing mothers were drawn from the same population and thus shared similar demographic characteristics such as socioeconomic status, single parenthood, level of education, and eligibility for Medicaid compared with those studies that were not matched groups. This finding raises important questions about the interplay between environmental risk and maternal substance use on a key moderator of child outcome: the quality of the caregiving relationship. 80 It is clear that the participants in the matched group of studies were recruited from high-risk populations: they were all of low income, drawn from geographical areas associated with severe financial disadvantage, had low levels of education, and in the case of the US studies, were predominantly from ethnic minority groups who were in receipt of Medicaid. All of these are well-recognised risk factors that have a cumulative rather than additive effect on child outcome.81,82 Thus, these families are at high risk of poor child outcome. The addition of maternal illicit substance use appeared to increase risk; there was still a significant, albeit small, difference in the quality of caregiving that favoured the non–substance-using group for maternal sensitivity. Thus, the additional risk of maternal substance use is likely to confer even greater vulnerability for these children who are already exposed to a significant number of socioenvironmental risks.83,84
We also tested age of child as a potential moderator. Typically, maternal sensitivity and associated constructs are relatively stable across time. 85 However, family stress and adversity have been found to influence a range of maternal behaviours, including sensitivity. 86 Thus, it is plausible that for families with maternal substance use, and at least for those matched in sociodemographic features, age of the child may be associated with poorer sensitivity and child responsiveness. The third moderator that we had aimed to assess was whether mothers who were currently in treatment for opioid replacement therapy and/or residential treatment differed from mothers who were not in treatment. However, it is notable that most of the studies that met this criterion were also nonmatched. As design took precedence over testing treatment as a moderator, we are unable to answer the question. Thus, the question remains one for further research.
Implications for research, practice, and policy
These results have important research, practice, and policy implications. First, the quality of the caregiving relationship in substance-misusing mothers is poorer than for mothers facing similar environmental adversity. Although these differences are not large, they underscore the potential impact substance misuse has on a mother’s capacity to provide sensitive and nurturing caregiving.
What is also striking, however, is the number of risk factors present in the matched non–substance-using group of mothers. The extensive literature linking multiple risk exposure to poor child outcomes dates from the seminal work of Rutter and colleagues. 81 More contemporary models of socioenvironmental risk emphasise the importance of cumulative risk rather than the identification of specific risk factors. 87 Thus, within this model, maternal substance misuse should be viewed as one further risk that, in combination with a range of other risk factors such as poverty, 88 will be associated with compromised child outcome. This leads us to question whether there is a disproportionate focus on maternal substance use as a risk factor independent of the broader contextual environment of impoverished families. Substance use is one of the key reasons families are referred to child protection services in both pregnancy and the postnatal period. 89 Although women with substance use problems have complex lives and histories, making them a high-risk group, these meta-analysis results raise issues about the potential failure to identify families where the quality of caregiving is poor, but maternal substance misuse is not necessarily present. 90
Second, results highlight the importance of providing parenting support to substance-misusing mothers that focuses on enhancing maternal sensitivity and responsivity to maximise child outcomes. This is an area of growing research and clinical focus, and a number of studies have shown the benefits of providing attachment-based interventions for high-risk mothers and their children.91–93 However, improving maternal sensitivity will also require a focus on helping mothers develop emotional regulation skills and additional support to address real-world problems such as housing and access to material resources. Contemporary parenting programmes, such as the Parents Under Pressure,91,94 draw from conceptual models of affect regulation and integrate these within a parenting framework.
Third, it is notable that most of the studies identified have focused on cocaine (sometimes in combination with other drugs of abuse), with only a few focusing on opioids but in the context of replacement therapy. Drug use patterns across much of Europe, Australia, and North America are changing with a growing use of psychomotor stimulants such as ‘ice’ and ‘crystal meth’. 95 These substances may influence the quality of caregiving in qualitatively different ways. For example, amphetamine abuse is more likely to be associated with a pattern of interaction with the child that may be hostile and/or unpredictable, given that these are both behaviours associated with ongoing amphetamine abuse. 96 This environment may be qualitatively different due to the direct effects of the substance, compared, for example, with cannabis and could result in poorer outcomes, including insecure/disorganised attachment strategies that occur in the context of hostile and unpredictable parent-child relationships, 15 leading to even greater risk of psychopathology. 12 Thus, future research should be conducted that investigates the relationship between the type of substances, combination of substances, and child outcome, ensuring that adverse environmental risk is controlled for by careful matching of comparison groups.
Conclusions
This meta-analysis is the first study to bring together literature spanning 20 years to assess both the impact of maternal substance use on quality of caregiving and factors that might moderate this relationship. The clear operationalisation of maternal sensitivity and child responsiveness enabled us to systematically identify and meta-analyse data from 24 studies and undertake subgroup analyses that enabled us to look at the potential impact of study design and infant age. The results show that maternal illicit substance use is significantly related to caregiving quality in the first 3 years of a child’s life. The subgroup analyses have highlighted that this difference, although significant, is nonetheless a small effect. These findings highlight the importance of addressing the quality of caregiving for substance-using mothers and draw attention to the need for future studies to ensure that substance-using mothers are compared with mothers who also face a range of environmental adversity.
Footnotes
Acknowledgements
All contributions to the authorship of this paper have been acknowledged.
Peer review:
Eight peer reviewers contributed to the peer review report. Reviewers’ reports totalled 2725 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author Denise Hatzis gratefully acknowledges receiving a Griffith University Postgraduate Research Scholarship awarded to her during the period 2011-2014 (CRICOS provider number: 00233E), which was provided to support candidature in the Doctor of Philosophy in Clinical Psychology (062206F) in the Applied School of Psychology.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
The systematic review as presented was designed and conducted by the first author DH who produced the first draft of the manuscript. DH, SD, and JB coded identified articles for inclusion into the meta-analysis. The second author SD provided constructive critical feedback and revision of the manuscript. PH contributed by assisting with analysing the data for the meta-analysis. JB made critical revisions and approved the final version. All authors reviewed and approved the final manuscript.
Disclosures and Ethics
As a requirement of publication, author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including, but not limited to, the following: authorship and contributorship, conflicts of interest, privacy and confidentiality, and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.