
Abstract
Methylenetetrahydrofolate reductase (MTHFR) has been linked with the etiopathogenesis of psoriasis with inconsistent results. Methylenetetrahydrofolate reductase C677T polymorphism was evaluated in 106 Saudi psoriasis vulgaris patients and 280 matched healthy controls using PCR-RFLP (restriction fragment length plymorphism) technique. The cardiovascular risk factors were also compared in cases and controls. Allele T and genotypes CT and TT were found to be increased while allele C and genotype CC significantly decreased in psoriasis patients as compared with controls (P < .001). These results showed that the T-allele and T-containing genotypes (TT, CT) of MTHFR C677T are significantly linked with psoriasis susceptibility while C-allele and CC genotype are protective for it. Body mass index, fasting glucose, total cholesterol, low-density lipoprotein, triglycerides, and C-reactive protein, known markers for cardiovascular diseases, were found to be significantly elevated in the patient group as compared with the controls. It is concluded that the MTHFR C677T polymorphism increases psoriasis risk in Saudi patients.
Introduction
Psoriasis is a chronic inflammatory, immune-mediated disease which affects 120 to 180 million people worldwide. 1 It affects male and female patients equally.2,3 Globally 80% of psoriatic patients has psoriasis vulgaris, a subtype of psoriasis.4,5 Various factors including race, geographic location, genetics, infection, immunologic, biochemical, psychological, and environmental factors influence the prevalence of psoriasis. 6 Ethnic variations, ranging from 0% to 12% have been reported in the prevalence of psoriasis worldwide.7–11 According to World Health Organization (WHO), 11 psoriasis is a serious chronic non-communicable inflammatory skin disease with multifactorial cause.
The pathogenesis of psoriasis is very complex and several different etiological hypotheses including those of the genetic, environmental, and immunologic factors have been suggested.12,13 Available literature indicated that genetic variation contributes significantly to the risk of psoriasis and more than 40 genes/loci are associated with the susceptibility to psoriasis in different populations. 14
The methylenetetrahydrofolate reductase (MTHFR, NM-005957) has been linked with the etiopathogenesis of psoriasis. The MTHFR gene located at chromosome 1 (1p36.3) converts 5, 10-methylenetetrahydrofolate to 5-methylenetetra-hydrofolate leading to the remethylation of homocysteine to methionine.15,16 This process maintains the methyl donors for DNA methylation which is important for gene regulation and cellular differentiation.17,18
The polymorphism at position 677 in MTHFR gene substitutes nucleotide C with T changing Alanine to Valine. This change results into the reduction of MTHFR enzymatic activity and thermostability, leading to the increased homocysteine levels.19,20 The hyperhomocysteinaemia has deleterious effects on various systemic and inflammatory diseases.21–26 As the psoriasis is associated with multiple diseases and causes high psychological burden in patients, this association of the MTHFR gene polymorphism with psoriasis becomes quite significant.27–29
The role of MTHFR gene polymorphism in psoriasis has attracted much attention during last 2 decades due to inconsistent results reported in various studies from different regions of the world.17,24,30–32 Till date, no report on the association of MTHFR gene polymorphism with psoriasis is documented for the Middle Eastern population. In this study, a possible association of MTHFR C677T polymorphism with psoriasis vulgaris in Saudi patients has been investigated.
Subjects and Methods
Subjects
Three hundred eighty-six Saudi subjects (106 psoriasis patients and 280 healthy controls matched for age and sex) visiting Dermatology Clinic of Prince Sultan Military Medical City (PSMMC) Riyadh, Saudi Arabia, were recruited. The diagnosis of psoriasis was based on dermatological changes, the location, and condition of plaques. All cases and controls were examined by dermatologists. Patient information including demographic features was collected using a questionnaire. All patients must be diagnosed with plaque psoriasis for at least 1 year. Exclusion criteria were coexisting inflammatory skin disease, diabetes mellitus, hypothyroidism, systemic lupus erythematosus, rheumatoid arthritis, history of hyperlipidemia, and renal and liver failure. The severity and extend of disease was assessed by Psoriasis Area and Severity Index (PASI) score. 33
Written informed consent from the patients/parent was obtained before their enrolment. We recruited 106 confirmed cases of psoriasis including 42 female and 62 male patients. The patients with mean age of 37 ± 15.5 years (age ranging from 9 to 65 years) and the mean duration of disease 9 ± 4.5 years were recruited. All the cases were adults except 3 children with 9, 12, and 16 years of age. The male to female ratio in patient group was 1.76:1, while the age of onset of disease varied from 8 to 55 years. For control, healthy women (n = 100) and men (n = 180) with mean age of 36 ± 10 years were included. The control subjects were also screened using the same questionnaire about the health status and those with the history of autoimmune or inflammatory disorders were excluded. The controls having first or second degree relative with psoriasis or any autoimmune disorders were also excluded from the study to minimize genetic heterogeneity. The protocol of this study was approved by the research and ethical committee of the PSMMC, Riyadh, via No. A/2015-10D.
Venous blood was collected from all selected subjects following 12 hour fasting. Lipid profile of all the subjects was determined following standard procedures in central pathological laboratory of PSMMC.
Genotyping
For genotyping, venous blood samples were collected in the tubes containing ethylenediaminetetraacetic acid (EDTA). Genomic DNA was extracted using DNA extraction kits from Qiagen (USA). Methylenetetrahydrofolate reductase C677T genotyping was performed by PCR-RFLP technique following the protocol as described elsewhere. 34 We included positive and negative controls in the PCR and repeated genotyping for 25% of the randomly selected samples for quality control.
Statistical analysis
The statistical significance was determined by comparing allele and genotype frequencies in patients and controls using the Fisher’s exact test. 35 P values ≤ .05 were considered significant. Hardy-Weinberg Equilibrium (HWE) was calculated using Hardy-Weinberg Equilibrium Calculator for 2 Alleles (https://www.easycalculation.com/health/hardy-weinberg-equilibrium-calculator.php).
The strength of the association of disease with respect to a particular genotype/allele are reported with the odds ratio interpreted as relative risk (RR) following the method of Woolf as described by Schallreuter et al. 36 RR indicates how many times more frequent a disease is in the positive subjects compared with allele/genotype-negative subjects. The etiologic fraction (EF) and preventive fraction (PF) were calculated following Svejgaard et al, 37 as mentioned elsewhere. 38
Results
The basic characteristics of the participants are summarized in Table 1. The fasting glucose, total cholesterol, low-density lipoprotein (LDL cholesterol), triglycerides, and systemic inflammation indicated as C-reactive protein (CRP) were found significantly higher in the patients than the controls. Similarly data for body mass index (BMI) was higher for psoriasis patients than the controls. The PASI scores of patients ranged from 10 to 35 indicating that the patients were with moderate to severe psoriasis.
Basic clinical and laboratory parameters of participants.

Values are indicated as mean ± standard deviation. Abbreviations: BMI, body mass index; CRP, C-reactive protein; HDL, high-density lipoprotein; LDL, low-density lipoprotein; TC/HC, total cholesterol/HDL cholesterol.
P < .05; **P < .01
The frequencies of alleles and genotypes of MTHFR C677T polymorphism differed in cases and controls (Tables 2 to 4). The MTHFR C677T polymorphism (rs1801133) was in HWE in patients. Contrarily this polymorphism was not in HWE in control group. The frequency of genotype CT was higher (43.40% vs 25%) while that of genotype CC was lower (51.89% vs 75%) in patients than controls. Genotype TT was found in 5 (4.71%) patients while totally absent in the controls (P = .001). Higher allele T and lower allele C frequencies were found in psoriasis patients than controls (P < .001). Sex stratification of genotyping results within the group (in cases or controls) showed no significant difference. However, when compared across the group (cases vs controls), significant differences were noticed (Table 3). The comparison of results obtained after repeating genotyping for 25% of the random blind samples with the earlier results showed 100% similarity.
Comparison of frequencies of MTHFR (C677T) variants in patients and controls.
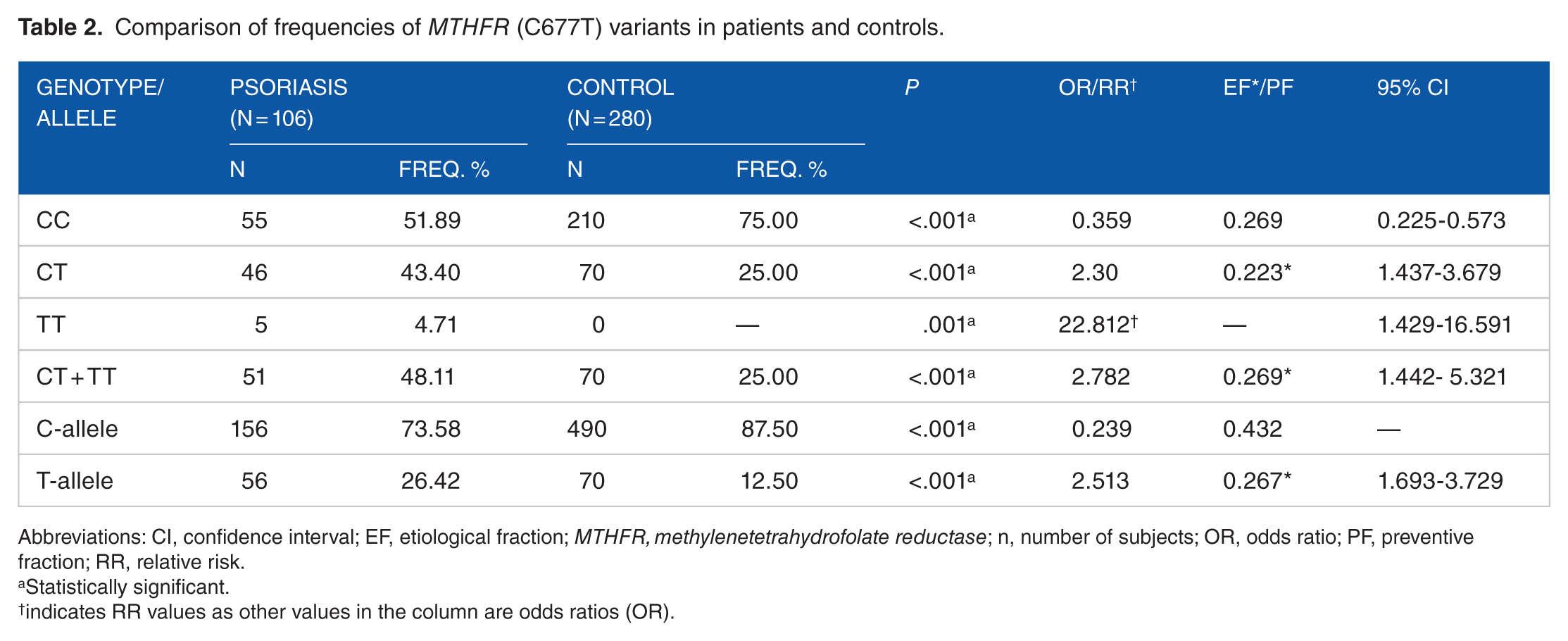
Abbreviations: CI, confidence interval; EF, etiological fraction; MTHFR, methylenetetrahydrofolate reductase; n, number of subjects; OR, odds ratio; PF, preventive fraction; RR, relative risk.
Statistically significant.
indicates RR values as other values in the column are odds ratios (OR).
Distribution of MTHFR (C677T) variants in male and female psoriasis patients.
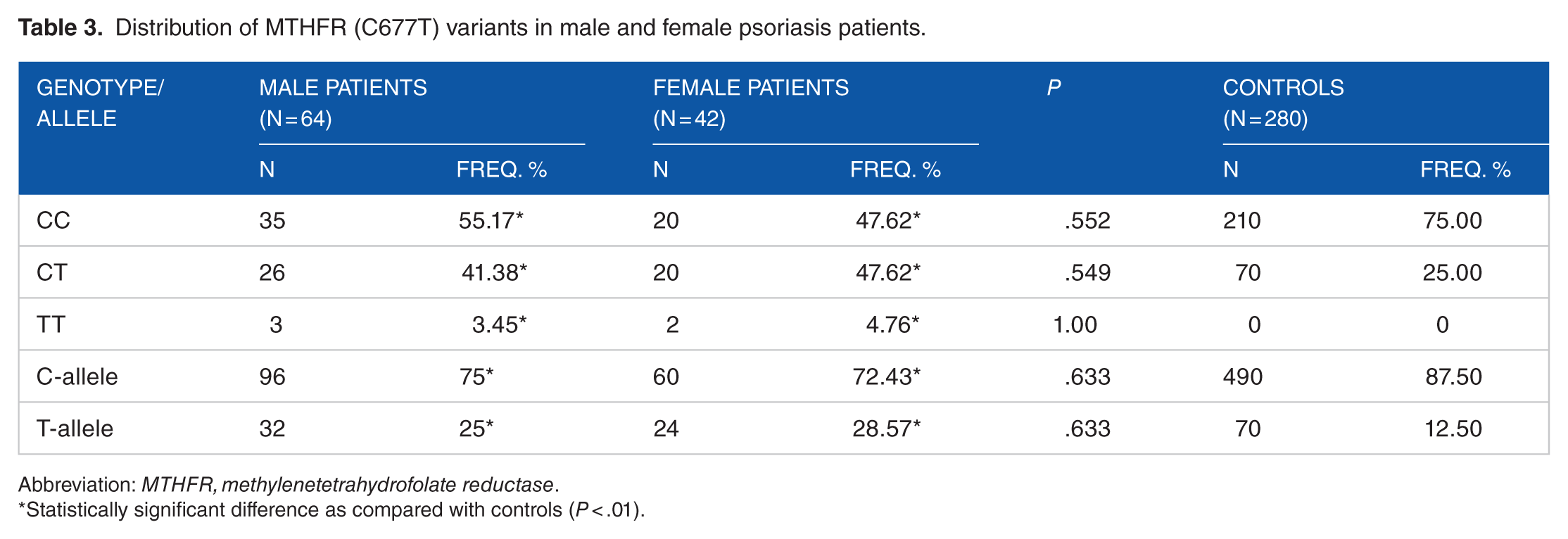
Abbreviation: MTHFR, methylenetetrahydrofolate reductase.
Statistically significant difference as compared with controls (P < .01).
Lipid profile with genotype of the patients.

All values are in mmol/L. Abbreviations: HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Higher than other groups (P < .0001, using MedCalc software).
The lipid profile of psoriasis patients with respect to genotypes of MTHFR polymorphism are shown in Table 4. The significant differences were noticed in the levels of HDL cholesterol, LDL cholesterol, total cholesterol, and triglycerides in the carriers of different genotypes of MTHFR polymorphism. Carriers of CC genotype had lower LDL cholesterol, total cholesterol, and triglycerides but higher HDL cholesterol. Subjects with TT genotype had significantly elevated triglycerides, LDL cholesterol, and total cholesterol but lower HDL cholesterol concentrations.
Discussion
The polymorphism data in controls were not in HWE. This deviation from HWE can be due to genotyping error or genetic factors which include a heterozygous advantage, population admixture/substructure, inbreeding, or copy number variants. 39 However, genotyping error was ruled out by repeating the genotyping for 25% of randomly selected samples and obtaining the same results. Therefore, this deviation could be due to consanguinity and/or an association with the functional locus as the consanguinity in Saudi population is quite high due to being a closed and isolated society with high rate of cousin marriages.
Higher frequencies of T-containing genotypes of MTHFR C677T polymorphism in patients as compared with controls indicated that MTHFR C677T polymorphism is associated with susceptibility to psoriasis. These results are in agreement with the earlier published reports from other ethnic groups (Chinese, Czech, Turkish, and Iranians) which consider MTHFR C677T polymorphism as a genetic risk factor for susceptibility and/or severity of psoriasis.17,31,32,40–42
Contrarily, the lack of association between MTHFR C677T polymorphism and psoriasis was reported in Australian and Malaysian patients.24,30 Recent meta-analysis also showed absence of association of this polymorphism with psoriasis susceptibility43,44; however, it was suggested that MTHFR C677T polymorphism may affect the severity of psoriasis. 44
These variations in association reports can be attributed to the ethnic variations as the prevalence of MTHFR C677T polymorphism varies among different healthy populations.34,45 The frequency of CC genotype varies from 23% to 97%, that of TT genotype from 0% to 28%, except in Mexican population where it is quite high (52%), while heterozygous CT genotype varies from 2.4% to 53% in various healthy populations worldwide as reviewed by Al-Shahrani et al. 34 In Saudi healthy population, the frequencies of CC, CT, and TT were 75%, 25%, and 0%, respectively.
Enzyme MTHFR is involved in homocysteine and folic acid metabolism and it is responsible for the irreversible conversion to 5-methyl tetrahydrofolate, which is a methyl donor of 5, 10-methylenetetrahydrofolate. 46 The reduced MTHFR enzymatic activity and thermostability due to MTHFR C677T polymorphism leads to the increased homocysteine levels.19,20 Higher Hcy concentrations in plasma of psoriasis patients than controls have been found.17,47,48 Significant differences in Hcy levels have also been reported in carriers of CC, CT, and TT genotypes of MTHFR polymorphism.17,49,50 MTHFR 677TT genotype and resulting hyperhomocysteinemia are known risk factors for cardiovascular diseases, cancer, and chronic idiopathic acrocyanosis.24,31,46,51–56 The MTHFR C677T polymorphism also decreases folate level in the serum57–59 which further increases the risk of hyperhomocysteinemia. 60 The decrease in folate consumption also influences the production of keratinocytes, consequently affecting the severity of psoriasis as suggested by Baiqiu et al. 17
The elevated CRP levels in Saudi psoriasis patients are in accordance with the earlier repost.61–65 The increased BMI, fasting glucose, total cholesterol, LDL cholesterol, and triglycerides are similar to those reported in several studies.66,67 Various parameters of adiposity like BMI, waist circumference, waist-to-hip ratio, and weight gain have also been associated with increased risk of psoriasis. 68
Conclusions
It is concluded that C677T polymorphism in MTHFR gene increases the risk of psoriasis development in Saudis. Psoriasis patients with T-containing genotypes of MTHFR C677T should be followed up for progression of any comorbidity as several comorbidities have been associated with psoriasis.
Footnotes
Acknowledgements
The authors extend sincere thanks to the administration of MSD for providing facilities.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MA conceived and designed the experiment. GBH, FAH, and AAK performed clinical examinations and collected demographic data. SR extracted DNA and performed genotyping. MA analyzed the data, interpreted the results, and drafted the manuscript. GBH, FAH, AAK, and AA-A agree with the manuscript results and conclusions. AA-A and MA revised, supervised, and approved the final version. All authors read and approved the final manuscript.