
Abstract
Little has been written about the living experiences of Māori caregivers who parent children living with Foetal Alcohol Spectrum Disorder, Te Iho Tātai-ā-Rongo (FASD) in Aotearoa. This study, of 14 Māori caregivers, focused on health and wellbeing and parenting strategies. Eight of the caregivers were whānau caregivers who were parenting children from extended family, and six other Māori caregivers were parenting children not known to them. Semi-structured interviews identified themes of hauora or wellbeing impacts, financial and employment issues, cultural practices, systems’ harms, FASD-informed parenting and systems’ changes needed. The findings show that Māori caregivers face great adversity in providing the best possible care for their children living with Foetal Alcohol Spectrum Disorder, and that they sacrifice a great deal in terms of their health or finances, alongside battling for basic supports and resources for their children. They are also active advocates for systemic change for increased resources to help their families.
Keywords
The reality and context of FASD (Te Iho Tātai-ā-Rongo) in Aotearoa New Zealand
In Aotearoa New Zealand, 24% of the population has a disability, and rates for Māori are higher, ranging from 26% to 32% (Ministry of Social Development [MSD], 2020). Rates for childhood disability are around 15% for Māori children, compared to 9% of non-Māori children (MSD, 2020). However, for neurodevelopmental disabilities or neurodivergent conditions, including Attention Deficit Hyperactivity Disorder (ADHD), Autism and Foetal Alcohol Spectrum Disorder (FASD), we do not have precise data. For autism, we have a prevalence rate of around 1% of children (Bowden et al., 2020). For ADHD, prevalence rates of childhood ADHD of over 5% are suggested (ADHD New Zealand, n.d.; Young et al., 2016). For FASD, it is estimated that rates for Aotearoa are 1.1–3.9% of the general population (Romeo et al., 2023), which equates to 58,646–207,928 people in Aotearoa of the current estimated population (Romeo et al., 2023; Statistics New Zealand, 2024). Romeo et al. estimated the Māori prevalence to be 1.7%–6.3%. However, these numbers are likely to be underreported as no system exists to capture robust data (Crawford et al., 2020; Romeo et al., 2023).
While specific data does not exist for Māori, researchers within Aotearoa and spokespeople point to disproportionately high numbers of whānau Māori likely to be living with FASD. We know that higher rates of Māori are in the youth justice system, among the homeless, in the prison system, among those taken into care, among those who cannot maintain continuous employment or housing, and those who are being misunderstood and excluded from schools. The Māori population is overall a younger population with a higher birthrate. Important Māori data, however, has been published by one diagnostic centre. In the Hawkes Bay District CDS (Child Development Services), between 2010 and 2015 out of the children assessed for FASD 77% were boys and 82% were Māori (Crawford et al., 2020).
FASD, known in te reo Māori (Māori language) as Te Iho Tātai-ā-Rongo, can be caused by any level of exposure to alcohol and is a lifelong neurodevelopmental – brain-based – disability that impacts a person’s central nervous system, alongside their physical health which means they can have significant primary challenges in areas of executive, social, emotional, motor and adaptive functioning, and secondary challenges or disabilities (Popova et al., 2023). Secondary challenges are likely to be harms caused by systemic ableism and intolerance from education, health, mental health, justice and welfare systems. Children with FASD can live good lives, and they have many strengths and qualities; they stand the best chance of positive outcomes if they have a stable, loving family or placement, do not experience violence and are assessed and diagnosed before they are too old, less than 8 years old ideally (Streissguth et al., 2004). Unfortunately, most children in Aotearoa New Zealand go undiagnosed (Crawford et al., 2023; Gibbs & Sherwood, 2017).
A particularly pressing issue for Aotearoa is the disproportionate numbers of Māori in institutional settings, alongside a high chance of not being diagnosed with any neurodivergent condition. There are some estimates that up to 50% of children in care might live with FASD but few will be identified as such (Gibbs & Sherwood, 2017). International and local studies suggest that rates of diagnosis for Indigenous children and adults are much higher than for non-Indigenous and that this represents a complex picture of racism, inadequate or poor quality assessment and diagnosis capacity and practices, multiple and intersecting forms of oppression, and impacts from the intergenerational harm of colonisation (Crawford et al., 2020, 2023; Espiner et al., 2022; Gibbs & Sherwood, 2017; Gonzales et al., 2021; Oldani, 2009; Rockhold et al., 2024; Williams & Badry, 2023).
Rockhold et al. (2024) and Gonzales et al. (2021) refer in detail to the results of colonisation being a key causal factor for Indigenous intergenerational cycles of risk across generations which perpetuate cycles of vulnerability to FASD throughout Indigenous populations globally. The colonising factors they list include: racism, displacement, spiritual and cultural harms, State-sanctioned violence against Indigenous peoples, institutionalisation practices and the lack of representation of Indigenous people and perspectives in health and social services. New Zealand has many of these same ‘risk’ factors – see next section. Gonzales et al. (2021) and Rockhold et al. (2024) consider preventive and strategic interventions to reduce the risks and harms of FASD, including actions towards prevention, diagnosis and intervention, but also things like preserving and keeping Indigenous children with FASD in their birth or extended families, keeping culture and language alive, and the ‘indigenization and decolonization of our health care, social services, public health and educational and economic systems’ (Gonzales et al., 2021: 292). Māori have fought to advance and sustain many of these prevention and protective factors already alongside new initiatives – see below – which can facilitate better, brighter and more culturally strong futures for Māori whānau where FASD is concerned.
Shameful history
Aotearoa’s shameful history of colonisation includes the use and misuse of alcohol in the establishment of colonial governments, right up to the present day and of failing to address the health impacts of the most damaging teratogen on babies’ health in the country. While Māori populations in contact with Europeans did not initially like or take to alcohol (Hutt, 1999), it was not long before Māori were greatly impacted, and it was noted in a petition in 1874 that Māori children were not born healthy because their parents were ‘drinking to excess’ (Haimona Te Aoterangi & 167 others, 1874).
The current cost to Aotearoa of alcohol harm is estimated to be 9.1 billion dollars, with around a staggering 4.8 billion attributed to FASD (New Zealand Institute of Economic Research [NZIER], 2024). The legacy of over 200 years of colonisation and alcohol harm has seen disproportionate numbers of Māori being placed into institutions of surveillance and so-called ‘care’, but in reality, these institutions have ensured Māori children have been abused, ripped apart from their cultural heritage, not had their disabilities or needs recognised, and in high numbers gone to prison, died young, or experienced lifelong mental health difficulties and trauma (Whanaketia, 2024). Our recent Abuse in Care enquiry exploring abuse in State and Faith-based care between 1950 and 1999 revealed that 624 or 27% of survivors of abuse who registered with the enquiry described themselves as disabled, and of those disabled survivors, 303 or 49% described themselves as neurodivergent (Abuse in Care, 2024). In this group of now adult survivors, there would undoubtedly be a large number of suspected people with FASD because historically we have had no capacity to diagnose FASD, only starting around 2008 in New Zealand (Gibbs & Sherwood, 2017).
Recent initiatives
Gibbs and Sherwood (2017) noted the slow speed at which FASD became noticed by several governments as a disability worthy of action, and since an initial national FASD Action Plan in 2016, few resources have been focused on helping families struggling to manage the challenges of caring for a child with FASD. However, recently, in 2024, the former Minister of Health, the Honourable Dr Shane Reti, has committed new project-based resources to support Te Tiriti-informed FASD diagnostic guidelines and training to increase clinician capacity to assess and diagnose FASD. The initiatives supported by the Ministry of Health have enabled some caregiver training and interventions for Māori caregivers, funding to support a screening prevalence study, ongoing support for the Te Kāhui Taurikura, the national Māori FASD advisory body, and funding to support the Māori Coalition made up of whānau and professionals with living experience of Te Iho Tātai-ā-Rongo, as well as much consultation with Māori and non-Māori, before a refreshed version of the FASD Action Plan is launched in late 2025 (Reti, 2024).
New language
The term used for impairments caused by prenatal alcohol exposure to the child before they are born is highly stigmatising. Prior to European colonising activities, neither Aboriginal nor Māori used the concept of disability to mean impairment or deficit (Hickey & Wilson, 2017; Williams & Badry, 2023). Instead, Aboriginal and Māori cultures often viewed disability as a gift or special status and accepted disability as part of human diversity. Prenatal alcohol exposure is an injury that can have a wide range of disability outcomes. In New Zealand, we have seen some reframing of neurodisabilities, and new names, based on strengths’ perspectives are emerging, for example, takiwātanga for autism, meaning in their own time and space, and aroreretini for ADHD, meaning attention goes to many things. The name Te Iho Tātai-ā-Rongo has been created by the Māori Coalition to support whānau with FASD, to ensure a new strengths-based definition of FASD. Māori are only too aware of the experience of stigma, judgement and overrepresentation and do not need to be placed in deficit-based boxes anymore. Colonisation processes have served to reinforce the deficit approach and invisibility of Māori and their whānau (Hickey & Wilson, 2017), and that is one of the reasons their voices must be prioritised in research.
Indigenous caregivers and FASD
Domeij et al. (2018) completed a systematic review of the experiences of caregivers alongside the experiences of people living with FASD noting that parenting was viewed as a lifelong commitment and that the whole family can become isolated and burdened because of FASD. In Australian studies, researchers have noted significant impacts for Indigenous caregivers of children living with disabilities generally, and also specifically, FASD (DiGiacomo et al., 2017; Williams & Badry, 2023). Impacts included difficulties getting financial resources and support for themselves or their children, experiencing health issues and other costs like stress, grief, isolation, financial costs, and having to advocate constantly to have the needs of their family heard.
Recently, Crawford et al. (2023) undertook a kaupapa Māori-led interview study with 14 Māori caregivers in New Zealand, focusing on diagnosis pathways, experiences of assessment and diagnosis, and access to FASD services and other supports that helped them in their journeys. Findings from the research noted that the current provision of FASD services, supports and pathways in New Zealand were inadequate and unnavigable. Crawford et al. (2023: 15) state that: ‘The lack of systemic support for whānau caring for tamariki was devastating for many whānau, with the impacts being felt continuously’, and that families often only gain limited support once they are at their wits end, completely exhausted and burnt out. Also, in New Zealand, Gibbs (2024) published a study with 56 caregivers, including Māori caregiver participants, where caregivers talked about the violence and abuse they experienced from their children with FASD. The impacts of aggression and violence were significant, with caregivers noting sustained health, stress and shame issues as a consequence, as well as frustrations with caring professionals not understanding the issues or impacts. Both the Crawford et al. and Gibbs studies highlight the tenacity and courage of caregivers and remarkable resilience in parenting children with complex needs.
There have not been enough studies in Aotearoa to gauge the lifelong challenges of parenting a child or young person with FASD. This study does this while also focusing on the positive strategies and practices that Māori caregivers use to help their children live their best lives, despite the harsh reality that FASD, until recently, has attracted no specific funding for supports. Gonzales et al. (2021) note a protective factor for future FASD is honouring Indigenous stories and ensuring representation in data collection, analysis and reporting.
The study
Methods and analysis
Semi-structured interviews were undertaken by Anita Gibbs as part of a larger study of 56 caregivers of children and young people living with FASD at locations all over New Zealand. A semi-structured interview schedule was used, and three main questions were posed:
What are some of the impacts of parenting a person with FASD on caregiver health and wellbeing?
What positive strategies are used by caregivers to survive and thrive?
What can be done to improve and support the health and wellbeing of those parenting persons with FASD?
The study was approved by the University of Otago Ethics committee, and consultation was undertaken with the Kai Tahu Māori advisers for research at Otago. A Māori colleague advised the main researcher to ensure that Māori caregiver voices were heard and included in the interviews and reports of the research. Participants were recruited through purposive and convenience sampling, hence, by word of mouth, direct requests to caregiver support groups, and in response to an information post from FASD-CAN on their Facebook pages. The participants were volunteers, and sampling was purposive and not matched to controls. The group of caregivers may or may not represent higher needs. However, FASD is viewed as a complex or high need disability by clinical experts and within international guidelines for assessment and diagnosis.
Informed consent was gained and interviews were undertaken in person at the location of the caregivers choosing or via Zoom as caregivers could also choose this option. Eight face-to-face interviews occurred, and six zoom interviews occurred. Interviews were recorded and transcribed, and each interview lasted between 45 and 90 minutes. Participants were sent their transcripts to amend as desired.
Analysis was undertaken using an iterative process of reading and re-reading transcripts. All transcripts were read multiple times, with a deep familiarisation of the narratives being the first outcome, then the drawing up of codes to build up sub-themes and themes, drawing on the work of Braun and Clarke (2006: 79) who describe qualitative thematic analysis as ‘a method for identifying, analysing and reporting patterns (themes) within data’. Also, applying the work of Thomas (2006), who describes processes of inductive and deductive reasoning. This meant that the themes linked to the main research questions were also being asked, and enabled new topics to be explored. The themes are reported in the next section.
Demographics
Fourteen Māori caregivers were interviewed, and basic demographics are shown in Table 1.
Caregiver demographics.
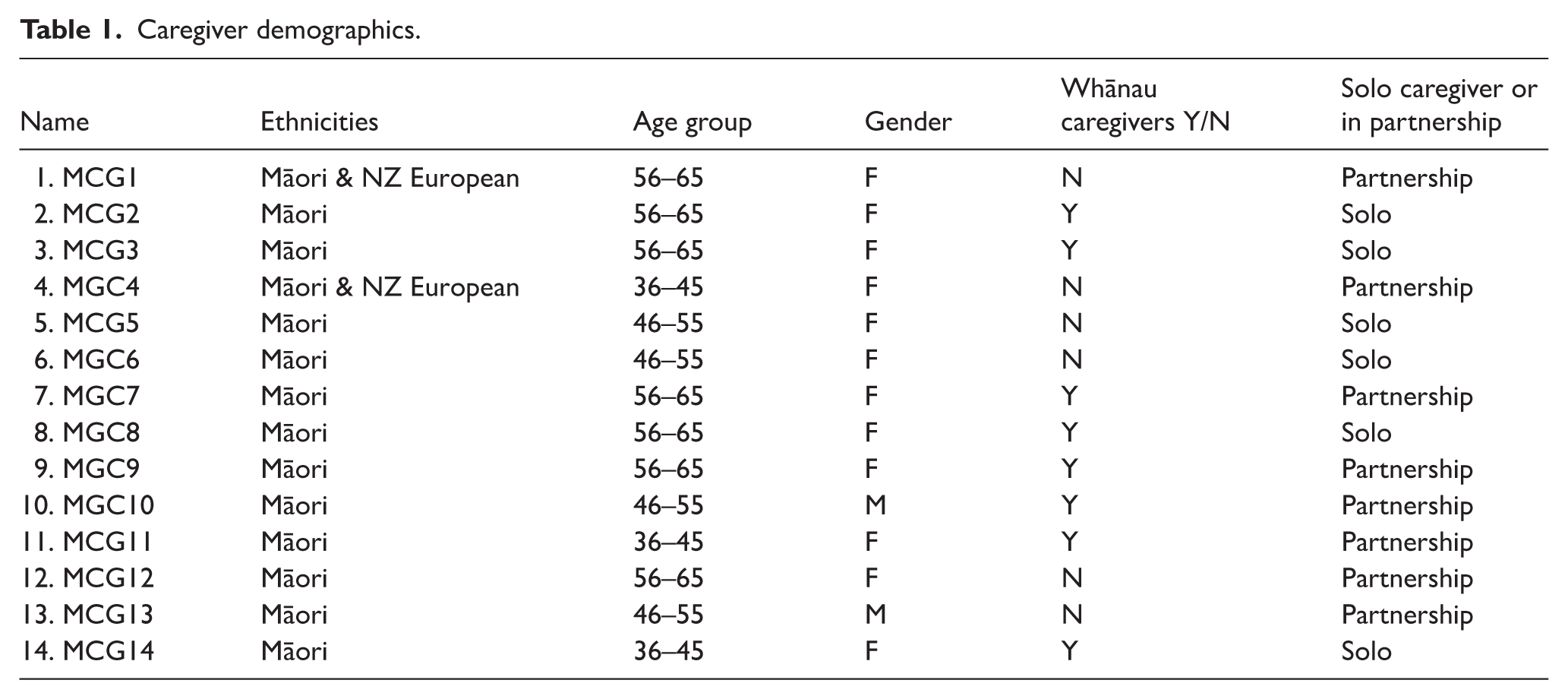
In summary, 12 females and two males were interviewed; they were an older population with seven in the age range 56–65 years, four in the age range 45–55 years, and three in the age range 36–45 years. Caregivers were predominantly female and older in age, and six out of the 14 were solo caregivers. All participants had their caregiving arrangements formalised with the State, but for 8 of the 14 caregivers, the children had come into their care specifically as whānau arrangements, where the child or children had a whakapapa or genealogical connection to them. Hence, some were aunties, grandmas, cousins, or other extended whānau relatives.
Positionality of researchers
The interviews were undertaken by Anita Gibbs, a non-Indigenous English-born New Zealander, alongside Māori co-authors, Cherryl Smith and Deb Cole, who assisted in the analysis and the writing of the article. All three identify as caregivers of children or grandchildren living with FASD, and all three are active in disability advocacy in their communities. Cherryl Smith and Deb Cole are grandmothers and both kaupapa Māori researchers who have written and presented on the needs of whānau Māori with Te Iho Tātai-ā-Rongo. Both are members of the Māori Coalition on Te Iho Tātai-ā-Rongo, who are running wānanga and developing training targeting Māori based on a whānau ora approach. The findings of this research present the living experiences of Māori caregivers and the authors are committed to ensuring caregiver voices are heard.
Limits of research
Gibbs notes that, while as an interviewer we shared common experiences in raising rangatahi with FASD, as a non-Indigenous New Zealander and non-fluent te reo speaker, the interviewees may have chosen not to reference specific cultural knowledge and may have tailored responses to the interviewer’s understanding. A te reo Māori interviewer was offered in the research information approved by Otago University ethics committee and none of the participants took up the offer. The number of Māori participants at 14 might be deemed a small study, though 14/56 is 25% of the total of caregivers interviewed for the larger study (Gibbs, 2024). In the general population, 18% are Māori. While 14 is not representative of all Māori caregivers, the themes highlighted are consistent with themes outlined from other small studies of Indigenous caregivers (Crawford et al., 2023; DiGiacomo et al., 2017; Williams & Badry, 2023).
Findings
The main themes arising from the caregiver interviews were the impacts on hauora or wellbeing across the four dimensions of Te Whare Tapa Whā (Durie, 1994), financial and employment impacts, systems’ harms, strategies and supports, use of cultural knowledge and practices in parenting and gaining supports, and systems’ changes required to help whānau flourish.
Theme 1: impacts on the wellbeing of caregivers
We are using the four dimensions of Te Whare Tapa Whā (Durie, 1994), taha wairua—spiritual wellbeing, taha hinengaro—emotional and mental wellbeing, taha whānau—social and family wellbeing, taha tinana—physical and health wellbeing, as a scaffolding concept to convey wellbeing from a Māori worldview. Durie’s wellbeing model represents the whole person through the analogy of a wharenui or meeting house with four dimensions. Caregivers were impacted in every area—with impacts on emotional and mental wellbeing alongside health being the most significant.
There were days where I really just wanted to end it, and end it for both of us, not just me. I was going to take him with me. . .. So that he wasn’t alone. But, luckily, I have had a good counsellor that has brought me out the other side of that, and I think I am doing okay. MCG14 Of course that just erodes your whole sense of immunity and self-care, you know, your whole sense of self-worth, you just think oh god, just so useless. MCG1 It does take a toll on you emotionally. I think the hardest thing is you become very isolated. MCG6
Twelve of the 14 caregivers noted significant and ongoing challenging behaviour, aggression, violence and verbal abuse and damage to property as a big impact on their mental health and emotional wellbeing:
Oh, I’ve still got all that. All my holes in my walls are still there. Yep. Skateboards through the walls, feet through the walls, punching the walls. . ..That’s where the depression came from. . . he doesn’t know any better but I can’t deal with it. It’s too much. MCG5
Caregivers were acutely aware of the toll that sustained violence took on the whole family and MCG13 described at great length how he retrained himself to take a step-back, or withdraw to make sure he was regulated himself, and then to try and calmly help his children dysregulate before he could chat with them about the outbursts or damage.
Taha tinana
Physical wellbeing was mentioned by all caregivers, down to humourous quips like ‘wrinkles, can’t you see them’, to more serious statements like ‘the body keeps the score’. Caregivers experienced significant health issues, like chronic immunity problems or constant sickness, heart issues from stress, becoming overweight due to being unable to have breaks from the children or undertake exercise, and high blood pressure. Some caregivers were able to address their physical health issues with medications and self-care, like taking walks and little respite breaks but overall, caregivers noted there were not many supports in place for them to be able to look after their health and general wellbeing:
Yeah, they were exhausting, and it started to show on my health..it was direct. . . .it was real. . . .My blood pressure went up yeah and I had no history of it. It was just the—you could see why. It was the long hours with little sleep, working plus baby. MCG3 So, as a family, we have been working towards better health, because it’s just killing me. My blood pressure was huge, and dangerous. So, my health was really bad, but I didn’t have any energy to do anything else. MCG4
Taha whānau
There were numerous impacts described by caregivers on their social and familial wellbeing. These included becoming isolated, not being able to have partners, loss of marriages/partners, loss of friends, not able to go places or to events or have people visit, difficulties getting good respite, limits on activities and going on holiday, and negative impacts on siblings and other extended family members. Sometimes, there were positive impacts on siblings, with older siblings maturing and taking care of their disabled brother or sister:
Partners, well, I made [my son] my priority when I got him, so I know what it was like to have men in and out of our lives, so I chose not to do that. MCG14. It’s a big job, it’s affected me, it’s affected our relationship and I think it’s affected the other kids in the family. MCG10.
Taha wairua
Out of the 14 Māori caregivers, spiritual wellbeing was noted as important by 13, especially as a source of strength and support, with only one caregiver noting no spiritual wellbeing and just a few caregivers describing that their spiritual wellbeing had been negatively impacted as a consequence of being caregivers:
I call my daughter my spiritual guru, because she’s just driven me into a meditation practice. . .. she sort of drove me into a daily practice, so that’s positive. I meditate twice a day. . .. I try and keep that up, and I teach my daughter.. MCG1 I am a Christian. . . . a swearing one. And, we have a church group, we are involved. . . .like I have had some messages like “could we request, I am sitting on top of my son right now, can you please pray”. MCG4 I think for me, yeah, I just have a strong sense of spirituality with what I am. I don’t really—it’s not necessarily attached to a church for me. For me it’s being in nature or being outside or just being in a quiet space. MCG3 I think from a spiritual perspective, I think it also hits your wairua about feeling settled that you’re doing a good job as a parent. MCG10
In addition to impacts on the personal and familial lives of caregivers there were two further areas that were significantly impacted, those of financial and employment impacts, and systems harms.
Theme 2: financial and employment impacts
There are high financial costs to caring for children with FASD and most of the 14 caregivers in this study had more than one child in their households. Children with FASD have additional health and social needs which caregivers often need to fund. There are few FASD specific services or supports. Caregivers tend to try and ‘fight’ for the same – and often inadequate – resources that everyone else is trying to access. Then there are the endless repairs for damage, additional education or school supports, funding activities that provide respite breaks for all, funding some medications, and funding FASD or other assessments:
MCG12 noted: Financial. Yes. We’ve had to do that [pay money out] many times because [son was] stealing other people’s money, as well as misusing her credit card.
MCG9 noted that the child welfare service involved with her whānau paid for some supports and other caregivers noted they got a foster care allowance, and some funded training from a permanency care agency.
Many caregivers reported having to reduce or give up their paid work and the subsequent loss of income but this meant they could give better care to their complex needs’ children. Several caregivers described employment as a ‘lifeline’ or ‘respite’, or ‘place of safety’, as well as a FASD-friendly place, where they got support to care for their children or work flexibly. Hence, as well as necessary income generation, employment could be a protective factor against isolation:
No, that’s been huge. Capacity to work and to be employed is the biggest thing for me. MCG2 [Employer] is FASD-friendly, it’s caregiver friendly. Yeah, absolutely. They were very, very accommodating, supportive of making sure that our young men in care, were being looked after. MCG9 Work is really important because it keeps me in contact with other people and think about other stuff. MCG3
Theme 3: systems’ harms
Around seven caregivers noted a few ‘big issues’ that led to them feeling stressed and stigmatised but the issues did not come from their children; rather professionals and judgement from society at large made their life all the worse. Notably, parent-blaming and ignorance about FASD from professionals really hit hard. Having to constantly advocate for resources or assessments also made caregivers feel like their children were not important. Delayed diagnosis and gatekeeping from professionals were noted as particularly distressing:
MCG1 Where you get blamed and shamed for not being or doing enough. MCG6 The stress levels are through the roof, as well as judgement. You get judged from every aspect of society, doctors, schools. There’s not one area you don’t get judged. . ..has been hard to get a diagnosis for FASD because she is academically brilliant. I think that’s one of the things that’s very exhausting is when you’re constantly being questioned on parenting. MCG3 People just don’t understand FASD—Oh, they just don’t understand it. MCG5
Another area where parents felt ‘harmed’ by the system was their experience of the education system, and caregivers described much trauma when teachers misunderstood their children, or, tried to exclude the children when no efforts had been made to upskill themselves in FASD knowledge:
If you go to a mainstream school. . ..you are going to be out—zero tolerance. MCG14 [Teachers] are so ingrained in [the standard educational system], that it’s very difficult for them to turn that on their head and to see the behaviour as being a symptom of a poor fit. MCG1
Theme 4: FASD-informed strategies and supports
Caregivers were adept at implementing strategies of FASD-informed parenting and accessing whatever supports they could.
FASD-informed strategies
Caregivers implemented many changes in order to help their children flourish. These included well-known FASD-informed strategies: ‘making accommodations’, ‘acceptance’, ‘reframing’, ‘repetition’, ‘modelling’, using ‘simple concrete language’, implementing ‘structure and routine’, ‘supervision’ of the child, use of ‘visual reminders’ and a ‘focus on strengths’:
I need really firm boundaries I need him—there’s no leeway and that’s what I did. . .consistency is your key..yep..very firm structure. Very clear communication. Very short, sharp communication with him. . . .Very, J do this, J do that. Good boundaries, consistency. All those sorts of things. Repeat, repeat, repeat as they say. MCG5 It is just what it is, I can’t change it, I just have to work with what I have got, to make the best of what I have got. MCG14 There are times that it’s been terrible, but you try and focus on the good times rather than the negative. MCG6
Survival parenting
Caregivers noted that sometimes just ‘surviving’ was enough to get through a day of parenting their children. In order to survive at times they might find themselves swearing – stress relief strategy – or using ‘cutting humour’, or ‘lowering their expectations’ of what they or their child could achieve. MGC14 said ‘I just take each day as it comes’. Caregivers also used words like ‘grit’, ‘bloody-mindness’, ‘determination’ and ‘hope’, to convey they were often doggedly hanging in through the tough times, in the hope that things would get better over the lifecourse:
There are times that I say “fuck”. Mother living with FASD [kids]. I mean, I am not a swearer, but I mean, by the end of it, you are like “for fuck’s sake”, because you are really. . ..will ask 20-25 times politely, and will you PLEASE go and do this, would you PLEASE do this, and then. . ..Why didn’t I just start with “go and fucking do it”, straight away, and I wouldn’t have had to waste my 2,000 words before 8 o’clock this morning. [Laughter] MCG4 And I’ve had to lower my expectations on myself and the kids really. MCG11
Rural living, environmental changes
In a few cases, caregivers noted that they had to move out of bigger towns or cities to rural areas to change the environment and keep their child safer or gain better schooling experiences, in smaller rural schools:
Into a new school. School worked well. [And] We found a lovely caregiver who was able to support me for absolutely nothing. So, she was just gold. MCG5 Definitely, definitely in terms of play for the kids. You know, there are walks, forest walks and that, but. . ..Because these children, you couldn’t take them to town before. MCG8
Helpful others
Caregivers acknowledged that they relied on and appreciated assistance from professionals, family supports, other caregivers and friends, whether for practical support or therapeutic assistance or respite. They especially noted the importance of connecting with FASD peers and groups for mutual support, often through the formal peak body for FASD, FASD-CAN:
We live in an area with all of my husband’s cousins as well, so we got far more extra help. MCG9. A brilliant teacher—she’s got all the rooms very subdued. . .it is all muted, she’s really into rhythm, she’s really into consistency, she’s really into structure, she’s really into kindness, she’s really into embracing diversity, and unique learning needs. MCG1 So, when we finally got to do respite, that worked well. We have a regular family that he goes to. MCG12 Your safest bet is talking to people that have FASD kids because they understand and there’s no judgement when you talk. MCG6
Self-care
All caregivers were able to understand the need to look after themselves, but only a few were able to implement the self-care strategies that they knew would help them recuperate and have enough energy for their needy children. Self-care included mindfulness, exercise, trips away, gardening, employment, voluntary work, eating healthier, and actively seeking help:
Self-care is so important because if you are not replenished you can’t give out. MCG1
Advocacy and activism
Several caregivers talked of the importance of being advocates to get the right help for their children but also having to work with others to become vocal in raising awareness of FASD. MCG3 talked about how she met with other Māori caregivers and professionals to strategise and advocate specifically for Māori solutions and supports:
Particularly Let’s fight for them, so that they can be acknowledged. So, I am that parent that will talk to anyone about it. MCG5
Theme 5: use of cultural knowledge and practices in parenting and gaining supports. (Taha Whānau)
In theme 1 on impacts we noted from the Te Whare Tapa Whā model taha whānau, family and social wellbeing impacts, and this next theme links to this in terms of the importance of using cultural knowledge and practices in parenting and gaining supports. For some caregivers, it was vital to both practice and integrate Māori language (te reo Māori) at home, and undertake a range of cultural practices that helped enhance the cultural connections for their whole whānau. These practices might include karakia, participation at regular `marae events, singing waiata, and other important tikanga to ensure Māori culture was upheld and integrated into their lives. Caregivers also ensured they drew on their Māori culture to get the right supports for their children, such as ensuring their children connected to their cultural knowledge and maintained links to Iwi and Hapū. A few caregivers noted the importance of having wider Māori networks to help keep their children safe or offer respite:
I definitely engage a lot in terms of Māori Atua—Atua Māori. . .I still use that—so, all of that is there. That cultural connection. Maintaining those cultural connections. I’m just fortunate that I have a level of knowledge to—just to help and guide him with that. MCG2 We integrate quite a lot of the Te Ao Māori world view stuff, so I think that keeps us actually well, and grounded, and teaching that to the kids and certainly with our daughter, she responds well to that. MCG1 Keeping the connection. Keeping the connection with the wider whānau, and we’re not there to be better than anybody, we’re there to share that and to give it back to them, to maintain that. Maintain who they are, that’s all we can do. MCG7
Theme 6: systems changes required to help whānau flourish
The caregivers were united in their calls for FASD to be funded and recognised much earlier so that their children got the early assessment, diagnosis and services much earlier than they did. They wanted ‘bespoke FASD navigators’ or ‘case managers’, ‘one-stop shops’ or ‘dedicated 24/7 help lines’ where they could get specific FASD advice, rather than having to constantly ‘shop around’ for generic assistance. They wanted ‘good quality respite care with neuro-informed carers’ who had been trained and were paid properly. They wanted all professional groups to have deeper training and knowledge and skill development around FASD. MCG1 noted the need for system-wide change to enable children with FASD to participate and flourish in all areas of society:
At the end of the day is it about FASD? Is it just about recognising that that is—oh, yeah, it’s a biggie. It’s a huge one. . . .We’re going through the autism—again, autism gets a lot of support. We need the same level of support. That’s it at the end of the day. Same objective. It’s the same impacts on children. MCG2 I don’t know how many times I’ve talked to people from government and that. FASD needs funding, the funding is just non-existent. MCG6 We need a “one-stop shop” for people with FASD children that you could ring and they say “okay, well you need to ring this organisation for that”. MCG6 Being able to tap into somebody who knows and who knows it well. . . .a paid person to be there to come and help and support these families to find hope because it’s the hope that goes when you get that diagnosis. MCG5
Discussion
Caregivers are tenacious, resilient and determined, and they sacrifice and suffer, with little recognition of the impacts on their health and wellbeing (Crawford et al., 2023; DiGiacomo et al., 2017; Domeij et al., 2018). Our study of Indigenous caregivers in Aotearoa New Zealand confirms similar costs and impacts, especially in terms of health, emotional, social and financial issues, and similar sacrifices and levels of commitment. Delayed supports, whether diagnosis or help provided at home or school meant Māori caregivers had to leave or change their employment, and bear the brunt of providing additional, extensive and costly care for their children with FASD. They had to become advocates and activists to get money and services, and they often educated professionals about FASD. Crawford et al. (2023) and DiGiacomo et al. (2017) confirm the challenges to get any resources for children with FASD in Australia and New Zealand. Māori caregivers were particularly adept at implementing accommodations and strategies that took account of their child’s different brain functioning; indeed, they were experts in FASD-informed parenting. They also utilised peer support extensively, appreciating the skills of other caregivers and the tolerance and understanding from their peers, which they often did not feel they had from uninformed professionals, friends and sometimes other family members. The expertise of this caregiver group needs to be acknowledged and appreciated, and consulted in the development of new FASD initiatives to help families.
Some studies have noted that connections to culture are just as protective and important as placement or home stability (Williams & Badry, 2023). In this study, a number of Māori caregivers strove to ensure their children were familiar with their whakapapa and important practices that linked them to their birth families and extended whānau and gave them an appreciation of the Indigenous language and prayers, songs or stories. The importance of spiritual practices for 13 of the 14 caregivers in this study is reflective of the significance of spiritual connections alongside a holistic viewing of the person in a Māori worldview (Te Ao Māori). In fact, the collective is seen as bigger than the individual and therefore wellbeing or hauora is viewed as an extended family concept, not just about the individual. In Te Ao Māori worldview if one individual is troubled then all are impacted; if one is joyful, then all will share the joy. It is vital to ensure that both culturally important practices and spirituality are encouraged and supported as part of the support to families where FASD is an issue. If Māori families discuss the importance of spiritual and cultural practices for themselves and their children, then these need to be welcomed by professionals, whether those professionals are familiar with them or not. Cultural and spiritual hauora lead to better outcomes for families (Gonzales et al., 2021; Rockhold et al., 2024).
Māori caregivers were very clear in their hopes for changed systems in many areas; they noted the need for recognition of FASD as a disability at all levels of society. With that came a call for funding to ensure better diagnosis or assessment services, alongside well-trained professionals including FASD navigators or FASD specialists who could offer best FASD-informed supports. Caregivers also wanted much more tailored support for their whole whānau which included all family members, not just the individual with FASD. Caregivers wanted to move away from ‘just survival parenting’ and the only way that would ever happen is when a proper change in systems’ funding of health, welfare, justice, disability and mental health occurred. As other researchers have noted (Crawford et al., 2023; Gonzales et al., 2021; Rockhold et al., 2024) to enable Indigenous children and youth and adults with FASD to flourish, the barriers to their participation and inclusion must be demolished, and their voices heard. We do see some emerging bespoke programmes in the form of FASD-CAN’s Life with FASD, a specialised group-based and peer-led caregiver programme (Foetal Alcohol Spectrum Disorder Care Action Network [FASD-CAN], n.d.) and McLachlan et al. (2023) have developed Te Whare o Oro, an Indigenous model and associated workshops, both designed to educate and empower caregivers. But FASD has not yet been formally accepted as a fundable disability in its own right, in the same way that autism has been funded in New Zealand for over a decade now. The Ministry of Health’s funding has been mostly for short-term, one-off projects, rather than ongoing, accessible funding for all families where FASD is an issue. Until that changes, families will continue to be burnt out and exhausted and having to draw on their own resources to get by, with no guarantees their whānau will flourish.
In addition, we need a robust research agenda exploring interventions and strategies for whānau with Te Iho Tātai-ā-Rongo, as we have a paucity of well-tested programmes. The emerging models that have been created by caregivers for caregivers need to show their effectiveness, and yet funding has been minimal, relying mostly on the willingness of expert, unfunded caregivers to develop and deliver training. We already know what caregivers and stakeholders want; we just need the government and research funders to fund the initiatives already developed (Chu et al., 2023).
Conclusion
This study has sought to illuminate the everyday struggles of being a caregiver of children living with FASD in Aotearoa, New Zealand. While the state struggles to fully acknowledge FASD as a disability or the subsequent need for funded supports to individuals and caregivers, the impact on caregivers, many of whom are ageing and in challenging circumstances, is dire. Caregivers have shared that the burdens and costs can be lifelong, but also that they have tenacious love and determination for their children. They reveal remarkable efforts to enable good lives for their children and families. It is hoped their stories will provide further evidence and momentum for FASD to be duly recognised and funded as a disability in Aotearoa and end the homelessness, imprisonment, victimisation, addiction and institutionalisation track that is so commonly part of their experience when they are not understood and when they are not given adequate housing, resources and supports. It is hoped these stories will work to enable those living with FASD, Te Iho Tātai-ā-Rongo, and their whānau caregivers, to live and be treated with the dignity they deserve.
Footnotes
Authors’ note
Anita Gibbs teaches criminal justice and disability studies at Ōtākou Whakaihu Waka, University of Otago. She has caregiving experience of Te Iho Tatai-ā-Rongo, FASD, and has developed training and support for caregivers in both Australia and New Zealand. She has published extensively in the field of FASD and advocates for better outcomes for all those living with FASD.
Cherryl Smith, Ngā Wairiki, Ngāti Apa, Ngāti Kahungunu, Ngāi Tahu, Te Aitanga a Hauiti. Based in Whanganui, she has over 30 years of experience in Kaupapa Māori research across the environment, health and education sectors. She has three mokopuna with Te Iho Tātai-ā-Rongo, and is part of the Māori coalition for Te Iho Tātai-ā-Rongo. This coalition brings its lived experience of caring for tamariki with Te Iho Tātai-ā-Rongo and their professional expertise to deliver training for whānau and professionals around the motu.
Deb Cole, Ngāti Kahu, Ngāti Hine, Te Rarawa, Ngāi Takoto, is also part of the Māori coalition for Te Iho Tātai-ā-Rongo and has lived experience of caring for mokopuna with Te Iho Tātai-ā-Rongo. Deb is also a member of the Kāhui Taurikura, a national advisory rōpū that advises government on alcohol harm. Deb is currently completing a Masters of Applied Practice that focuses on giving voice to kuia who have raised or are raising mokopuna who live with FASD. She is also a reverend in the Māori Anglican Church.
Funding
The authors received no financial support for the research, authorship and publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and publication of this article.
Glossary
aroreretini Attention Deficit Hyperactivity Disorder (ADHD)
hapū cluster of extended families, descended from an eponymous ancestor
hauora health and wellbeing
iwi tribe, nation
Kai Tahu [Ngāi Tahu] tribe within the South Island of Aotearoa
karakia ritual chants; invocations
kaupapa Māori Māori focused
marae traditional Māori place of gathering
rangatahi youth; teenager
taha hinengaro emotional and mental wellbeing
taha tinana physical and health wellbeing
taha wairua spiritual wellbeing
taha whānau social and family wellbeing
takiwātanga autism
tamariki child; children
Te Ao Māori Māori worldview
Te Iho Tātai-ā-Rongo Foetal Alcohol Spectrum Disorder (FASD)
Te Kāhui Taurikura Māori FASD advisory body
te reo Māori Māori language
Te Tiriti [o Waitangi] The Treaty [of Waitangi]
Te Whare o Oro Indigenous model and associated workshops designed to educate and empower caregivers with FASD tamariki
Te Whare Tapa Whā health philosophy, based on a holistic health and wellbeing model, developed by Dr Mason Durie in 1982.
tikanga customary practices and protocols
waiata song
whakapapa genealogy
whānau family
whānau Māori Māori family
wharenui meeting house