
Abstract
In Aotearoa New Zealand, perinatal mental health outcomes and maternal suicide rates demonstrate that Māori (the Indigenous peoples of New Zealand) mothers and birthing parents have the worst outcomes relative to other ethnic groups. Little research exists exploring Indigenous approaches to perinatal mental health or the perspectives of Indigenous peoples on perinatal mental health interventions. This article explores a kaupapa Māori (Māori approach) perinatal mental health intervention, offering insights around its responsiveness to the needs of Māori birthing parents. This qualitative study was guided by kaupapa Māori research methodology and explores the experiences of 11 Māori mothers who had accessed a kaupapa Māori group intervention for perinatal mental illness. Results demonstrate that future service design of perinatal mental health services should consider the incorporation of whanaungatanga (relationship building) and tikanga (cultural customs, conventions) to improve mental health outcomes and elevate the mana (prestige, power) of Māori during the perinatal period.
Keywords
Ki te kotahi te kākaho ka whati, ki te kāpuia, e kore e whati (The single strand of kākaho breaks easily, not so a bunch)
Introduction
It is well established that the health of Indigenous peoples has been negatively impacted by the continual effects of colonisation (Reid et al., 2019). Māori (the Indigenous peoples of New Zealand) experience significant inequities across all areas of health, including the perinatal period. Perinatal health outcomes for all Indigenous parents are particularly concerning (Hickey et al., 2021). In Aotearoa New Zealand, perinatal mental health outcomes demonstrate that Māori mothers and birthing parents have the worst outcomes relative to other ethnic groups, with the Perinatal and Maternal Mortality Review Committee (PMMRC) (2022) of New Zealand repeatedly calling for urgent actions to address these inequities. Non-Indigenous mothers and birthing parents are more likely to be screened, assessed, and treated for perinatal mental illness compared to their Indigenous counterparts, perpetuating patterns of inequity for Indigenous parents already impacted by structural racism and discrimination (Miller et al., 2024). These patterns of inequity are echoed in the Aotearoa New Zealand context, with Māori mothers and birthing parents being significantly impacted by racism and discrimination within health care settings (Becares & Atatoa-Carr, 2016; Thayer et al., 2023). This issue is further emphasised by the most recent New Zealand report highlighting that suicide accounts for over 40% of direct maternal mortality events, with Māori being affected three times the rate of their New Zealand European counterparts (PMMRC, 2024).
In Aotearoa New Zealand, the health system privileges a western model of care, while failing to address the inequities that Māori face (Graham & Masters-Awatere, 2020; Reid et al., 2019). The design and delivery of kaupapa Māori (Māori approach) health services have been developed to address health inequities through improving access and providing culturally responsive health interventions (Rolleston et al., 2020). There is very little research exploring such Indigenous approaches during the perinatal period. Of the research that does exist, there is little that centres the voices of Indigenous parents (Meredith et al., 2023).
Disruptions to social identity and connection are known to increase the risk of mental and emotional distress for birthing parents in the perinatal period (Seymour-Smith et al., 2017). A lack of social connection has been associated with poor physical and mental health outcomes across a range of contexts and populations (Morina et al., 2021). Perinatal interventions that strengthen social support have been recommended for preventing and treating mental health distress (Meredith et al., 2023). Group interventions for parenting skills offer a supportive space and provide short-term positive impacts on the emotional health of parents (Lavender et al., 2016). While there is strong evidence of the efficacy of professionally facilitated, programme-based support groups for people living with mental illness outside of the perinatal context (Worrall et al., 2018), research is limited on effective modes of delivery of mental health interventions in the perinatal period (Surkan et al., 2024). Even less literature exists regarding such interventions for Indigenous parents (Meredith et al., 2023).
The aim of this article was to explore the perspectives of Māori mothers and birthing parents of a kaupapa Māori perinatal mental health group intervention, exploring the effectiveness and responsiveness of the group to the needs of Māori mothers and birthing parents. A secondary aim was to gain insight of the factors that support Māori engagement with a group perinatal mental health intervention.
Methods
Background of study
Māori mothers enrolled in community perinatal mental health services within the previous 12 months were interviewed in March to May, 2023, as part of a wider research study exploring Māori perspectives and experiences of perinatal mental health. Participants for the overall project were recruited from two community perinatal mental health services: a service offered out of a mainstream organisation and a kaupapa Māori service. This article focuses on the qualitative data from 11 research participants who were enrolled in the kaupapa Māori service regarding their experience of a group intervention.
Description of kaupapa Māori perinatal mental health service
The perinatal mental health service attended by the 11 participants in this article was offered by a community based kaupapa Māori organisation. The wider organisation provides a range of health and social services for mothers and birthing parents with children under the age of 5 months. To access the perinatal mental health programme, Māori mothers and birthing parents are referred by their well child nurse or midwife. A multi-disciplinary team comprising of two clinical psychologists, a mental health nurse specialist, a midwife, a social worker, and two cultural advisors, provide individual therapy, mental health support, cultural support and social support. In addition to the individual support, three programmes form a group pathway within the service and are described in Table 1.
Kaupapa Māori perinatal group pathway.

* = Tree Tree of Life Narrative therapy tool (Ncube, 2006).
Kaupapa Māori research methodology
Kaupapa Māori research (KMR) methodology guided this qualitative study. KMR is led by Māori researchers with and for Māori participants, and incorporates Māori knowledges, practices, and values. This methodology ensures that Māori worldviews and understandings are privileged and protected within the research (L. Smith, 2012). A systematic review highlighted the lack of Indigenous mothers and birthing parents’ voice in the literature surrounding perinatal mental health (Meredith et al., 2023). This guided the research team to ensure the research approach and methodology centred the voices and perspectives of whānau Māori (Māori families) and highlighted the strengths and aspirations of Māori participants. Mana Wāhine (prestige and dignity of women) theory (Pihama, 2001) informed the research and ensured respectful and responsive research methods. This was a priority, given the sensitive nature of the research topic. The research team comprised of a Māori midwife who has worked alongside Māori mothers experiencing mental distress during the perinatal period, and three Māori co-authors who have extensive KMR, Māori health, and health research expertise. Coding was initially undertaken by the lead researcher (CM) and peer reviewed by the co-authors. This collective Indigenous approach and collaboration guided the coding and analysis throughout the research process.
Ethics
Ethics approval was gained from the Health and Disability Ethics Committee of New Zealand (ID: 13768), and locality authorisations were granted by the two sites where interviews were undertaken. The Consolidated Criteria for Strengthening the Reporting of Health Research Involving Indigenous Peoples (CONSIDER) statement (Huria et al., 2019) guided the planning, design, and reporting of the research and Māori consultation was completed through the University of Otago processes.
Recruitment
Staff from two perinatal services provided study information to all eligible participants. To be included in this study, participants needed to be Māori and have engaged with a perinatal mental health service within the previous 12 months. Interested participants made direct contact with the researcher either via email or phone.
Interview process
Participants provided written informed consent prior to interviews. Interviews were conducted either within the participant’s home or at a venue offered by the Māori organisation, with the majority of participants choosing to be interviewed in their homes. A semi-structured interview schedule was informed by a systematic literature review (Meredith et al., 2023) and designed to provide appropriate space and time for participants to report their experiences in the perinatal service and explore the enablers to engaging with the service. Interviews were recorded, transcribed, and sent to participants for review prior to any analysis. Transcriptions were then anonymised and allocated a number.
Data analysis
NVIVO software was used to display and code the interview transcripts. Two coding cycles were completed incorporating structural, descriptive, and pattern coding (Saldana, 2021). The first cycle comprised two phases. Phase one utilised structural coding to identify data that aligned to the framework adapted from Aotearoa New Zealand’s Maternity frameworks (Te Whatu Ora, 2022a, 2022b). The second phase used pattern coding to further refine and make sense of the data by clustering similar content matter. The second cycle of coding was applied only to the data of participants who were enrolled in the kaupapa Māori perinatal group pathway. Phase one employed descriptive coding to draw out specific categories of information being discussed and described. The second phase then applied pattern coding to cluster categories together where the same phenomena were being described from different perspectives to form themes.
Results
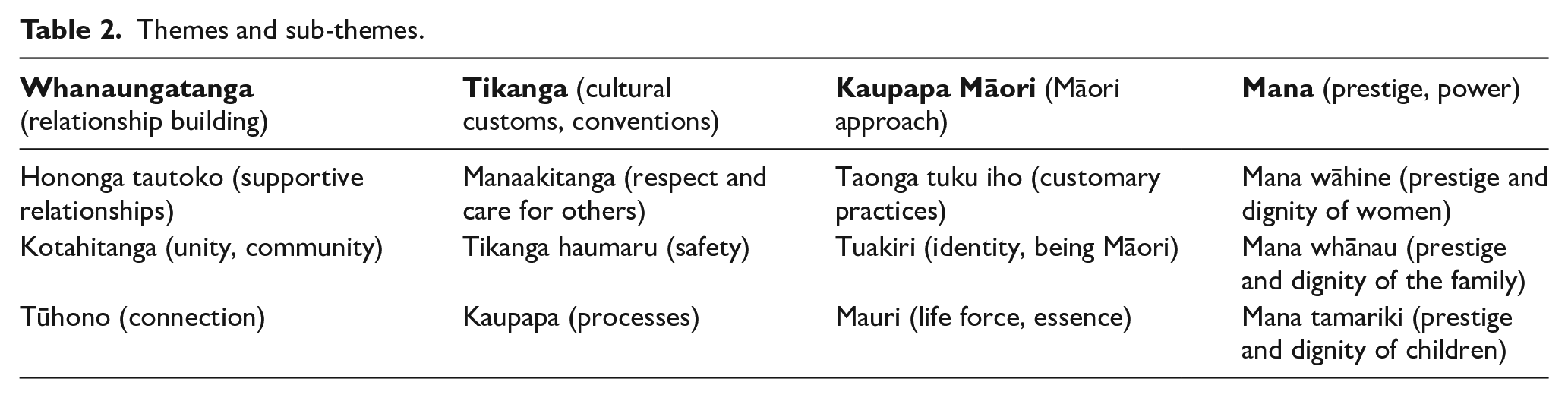
Four themes—whanaungatanga (relationship building), tikanga (cultural customs, conventions), kaupapa Māori, and mana (prestige, power)—were identified through the analysis of participants’ experiences of the kaupapa Māori perinatal mental health service. These themes and their sub-themes are presented in the Table 2.
Themes and sub-themes.
Whanaungatanga (relationship building)
The theme of whanaungatanga captured the importance of relationships within the group context as described by the participants. Strong relationships supported access to, and engagement with the group programme. Relationships were also viewed as being crucial to the success and efficacy of the group programme. Whanaungatanga encompassed three sub-themes: kotahitanga (unity, community), tūhono (connection), and hononga tautoko (supportive relationships). Participants described the groups as providing a space where these three aspects of whanaungatanga were experienced and shared among the mothers and group facilitators.
Hononga tautoko (supportive relationships): participants reported that successful whanaungatanga required the development of relationships that often began long before the participant entered the group setting. Participants discussed the importance of team members working alongside them individually and discussed the benefits of what the group programme could offer to them as Māori parents. Goal setting then provided the opportunity for the group programme to be identified as a process that could support participants’ goals. Sometimes this supportive approach took weeks or months before a participant would agree to attend the group. Accessing the group programme was often dependant on the strength of the relationship participants had with the team member. The closeness, trust, and relationship were reported to be instrumental in the eventual decision to attend: what made me decide to trust [the team member]? I got to know her better. Over the weeks, which turned into months and then you know—I liked her. She tried to show me a different path that I was afraid to take. When I was ready to finally step up, I did it and I met lots of other mums who were going through the same situation that I was going through, and I didn’t feel alone. (Anahera)
These supportive relationships between participants and kaupapa Māori service staff also helped in practical ways. For example, when lack of transport was a barrier to attending group programme, the team member would provide transport for Māori parents and their baby, facilitating access. If the group facilitator was unknown to the participant, meeting them prior was also noted to be helpful which supported participants to attend despite having anxieties.
I went to the group and she [the clinician] was there to welcome me into the group and kind of meet me and that’s when I met [the group facilitators]. (Kahu)
A strong emphasis was placed on the value of relationship building during the initial part of the group programme. Once relationships were established, then deeper aspects of group therapy were introduced. Participants reported that having known faces from the group programme encouraged them to commit and progress along the group pathway. Peer support mentors (parents who had previously completed the group programme and undertaken peer support training) were another important relationship within the kaupapa Māori group setting. Participants appreciated the presence of other parents who had previously completed the group programme and shared how mentors were a motivating and inspiring influence. Despite finding the group programme daunting initially, participants stated that they appreciated feeling comfortable enough to be open and ask questions. Responses from the facilitators and other attendees were reported to be supportive, validating, and non-judgemental. Having these responses reflected to them in the context of the group developed trust and strengthened the relationship building process further. Kaupapa Māori approaches of the group supported relationships to thrive. Approaches included karakia (blessings, prayers) and setting intentions, collective decision-making and shared values, the sharing of kai (food), and aiming to minimise any power imbalances that existed between facilitators and group participants.
Kotahitanga (unity, community): participants highlighted a key outcome of whanaungatanga was the sense of community and unity, or kotahitanga, that being with others brought. Kotahitanga contrasted with the isolation and separation they had been experiencing prior to attending the group. Continuation on the group pathway strengthened community building. Participants related the group experience to a sense of belonging they had previously felt in other spaces such as church. In this way, the group provided a space where they felt valued, where they could prioritise their own wellbeing because they were sharing their experience of Māori parenting within a collective. Kotahitanga was seen as a strong connection between facilitators and group participants with all being part of the same collective and was an essential feature that contributed to the success of the group: and it’s not just about relying on the team. It’s creating a space and a community where you can flourish and be the strong māmā that we’re supposed to be. (Kahu)
Open discussion and hearing the experiences of other Māori parents contributed to this feeling of community, especially when the stories shared were similar to a participant’s own. Again, having their experiences validated within a group setting and knowing that they were not alone in any challenges encouraged participants to look outside of their own situation and offer each other support. Cultural practices specific to the group such as sharing of food, acknowledging the space and each other through karakia, and taking the time to focus on whanaungatanga promoted the creation of kotahitanga.
Tūhono (connection): whakawhanaungatanga (process of establishing relationships) facilitated the development of strong friendships and support networks not dependant on the group, the facilitators, or the organisation. Participants shared how they valued these connections and the feeling they were part of creating community where they could uplift and support each other. Participants reported that this was what they felt was supposed to happen, and how community was meant to be. The sense of community came through shared connection around mental health or social circumstances: The friendship, the community. And having a space where you’re not the only one with problems. You’re not the only one that’s not feeling a hundred percent in their life. (Ana)
Tūhono occurred even when attendees of the group programme were low in number. One participant shared how she was initially disappointed that the group she attended only had two participants, as she had been hoping to make many connections. However, she now reflected positively on the experience as she and the other participant had developed a particularly deep connection. These deeper connections suggest that the group’s kaupapa Māori approach was more responsive. As one participant explained in her experience connections made with parents in other non-kaupapa Māori groups felt superficial in comparison. Within this group, conversations and connections were not superficial but experienced as deeper and more authentic.
You know it’s nice [the group programme] being more based in the Māori culture. With other mum groups it’s like they’re my friends but it’s just a surface level connection. With the kaupapa Māori group we’re a bit more real. (Hana)
Participants reported appreciating how group facilitators and peer support workers in the group also shared their own lives and experiences with them. This created connection, built trust, and was identified as an important aspect of whanaungatanga. Mutual sharing indicated to the participants that the facilitators knew and understood the challenges or circumstances they were going through, and this made deeper connections possible.
Tikanga (cultural customs, conventions)
The theme tikanga described the experiences of being in the group and the specific practices and activities the participants were exposed to. Tikanga also referred to the cultural customs and conventions embedded in the group pathway. Three sub-themes interwove within the theme of tikanga: manaakitanga (respect and care for others) was described by participants as being expressed in both practical and untangible ways. Tikanga haumaru (safety), refers to the sense of safety created in the group through the practice of manaakitanga. Kaupapa (processes) refers to how knowing and understanding the kaupapa of the group supported the participants to engage with and appreciate the tikanga of the group.
Manaakitanga (respect and care for others): participants conveyed a sense of being cared for and a familiarity that made them comfortable within the group space. Familiarity related to the group facilitators acting and behaving in a manner similar to how family would operate. Participants reported that they felt loved, seen, and respected and stated how they appreciated facilitators making efforts to make contact, show interest in their lives, and encourage them to attend the groups.
Honestly, it was amazing. The moment that I walked in, they made it feel comfortable. I felt like I’d just like, found my long-lost Aunties, like they were amazing. All of them just wrapped around us in a really loving way that we needed at the time. (Kahu)
Small gestures or expressions of care during the group sessions were noticed and appreciated. For example, one group facilitator would bring in homemade rēwana (a Māori sourdough bread) and the sharing of this and other food was always appreciated. Having others in the group be there to support by holding baby or providing food for them to eat was articulated as being pivotal in making participants feel welcomed and valued: To actually enjoy myself for me and to have someone else hold my baby and be okay. And to ask me, do you want me to make you some food? And someone to put two buns in front of me that are filled with food and eat it, you know, like those little things. And that was so nice. I’ve eaten today, you know, I’ve had someone hold my baby. (Manaia)
Reciprocity was an important aspect of manaakitanga. Participants expressed the shared responsibility they felt for the group to behave with kindness and respect towards the facilitators and other group participants, reciprocating the respect, warmth, and kindness they themselves had experienced.
Tikanga haumaru (safety): a sense of safety was a key aspect of tikanga. Participants discussed the importance of having a space that was just for them. Safety was described as being created in two ways: the initial group was strictly closed with only attendees and facilitators allowed to enter the group space after the first session. Participants shared how they appreciated the closed group tikanga as this created a space that felt safe for all the group members. The privacy provided a space where participants could focus on and explore their identity and wellbeing outside of sometimes unhealthy relationships. Some participants relayed they did not realise that they needed this space until they experienced it. The closed group sessions also ensured that there was a consistent group of attendees which participants reported offered the predictability of knowing who would be attending each session. This predictability reduced stress and anxiety about who they would share the session with and allowed for the building of trust and connection with each other.
The closed groups definitely help with my anxiety. You know who’s going to be there. You know what’s going to happen. (Hine)
Second, the facilitators set boundaries for the group programme at the very beginning. These boundaries were co-created, with all members of the group contributing to a set of understandings and commitments that they all agreed to—for example maintaining confidentiality. Participants reported that collectively setting the tikanga of the group made the space immediately feel safe. Knowing and understanding these agreements meant that they could share without fear of judgement and the knowledge that everything would be kept confidential. It also meant knowing that they would only need to share what they felt comfortable with, as one group agreement was to ensure no one felt pressured.
Participants articulated how the closed group tikanga and the co-created boundary setting created a space that allowed them to be open and show vulnerability. The expression of emotions was able to occur more freely, and they also felt able to ask questions without fear of judgement. One participant reported that from her perspective this made the group and the content flow more easily and be more effective.
[The facilitators] went through what was expected of them and what was expected of us. It was for the safety of all the mums, which was really nice. They painted the borders of how the group would look and it instantly felt safe. And that was what I think was the beginning, the domino effect that just made everything else easier. (Kahu)
Kaupapa (processes): understanding the kaupapa of the group was instrumental in the success of the group. For instance, formalising the commitment at the beginning of the programme with group attendees and facilitators helped ensure regular attendance. One participant stated that if it was a casual drop-in group there would have been no obligation to go, and she would have been more likely to find excuses not to attend.
Participants appreciated the pathways offered by the group programme and reported that these pathways led to the development of relationships, unity, and support networks. Participants spoke of the relief of knowing that once the initial group programme was completed, they could continue to be part of the programme as much or as little as they wanted, either through the ongoing follow up group or training as peer support mentors. Participants stated that they appreciated the ongoing support that the group pathways offered and the opportunity to give back as peer support mentors.
I’m able to reach out to them, and I feel comfortable to reach out. And I know that after group we can go on to the next group and come back through as [peer support] and help other mums as well. So, I know it’s not just going to be group’s over, and it’s finished. I know, there’s ongoing support, which is really nice. I don’t want it to be over, I really enjoy being with them. (Hana)
Participants appreciated the regularity of the group sessions, discussing how at that time they needed weekly check-ins to focus on their wellbeing. The group was often the only adult social interaction in their week. Participants reported feeling a sense of purpose and stated that attending the regular group sessions gave shape to their week. Generally, participants spoke of not wanting the group programme to end.
It gave me purpose because I didn’t have anything do all day and I didn’t have anywhere to go. So, for that one day a week there was a reason to get up and get dressed, a reason to get out the house to go somewhere. You had a destination to go to, it was a nice little drive. It was a reason to throw on nice clothes and not wear, you know, your soft clothes at home. (Manaia)
Kaupapa included the content of the group such as psychoeducation, emotional regulation skills and traditional knowledge, which were all highly valued. Participants relayed how they were able to draw upon these skills and knowledge within other relationships or situations and felt that they had gained foundational life skills.
Kaupapa Māori (Māori approach)
The theme of kaupapa Māori emerged from discussions related to the inclusion of Māori practices, the Māori language, and Māori ways of knowing or worldviews within the group. The sub-themes relate to specific aspects of these kaupapa Māori: taonga tuku iho (customary practices), tuakiri (cultural identity), and the mauri (life force, essence) of the group.
Taonga tuku iho (customary practices): participants spoke enthusiastically about engaging in customary practices such as karakia, poi (a light ball tied onto a string used for Māori performance art), weaving with harakeke (flax), and waiata (traditional songs). Engaging with these practices during shared activities enhanced connection.
When we did the harakeke weaving here, it was just really nice. We all found it nice just sitting down and doing something with our hands and weaving but then just talking and catching up. (Hana)
One participant identified that reconnecting to Māori ways of being and worldviews during challenging times lifted her depression. Participants appreciated the sharing of information around customary practices and the Māori language, and the opportunity to be creative and have fun. Participants reported enjoying the use of pūrākau (myths, traditional stories) and metaphor. They stated that the content and characters within these pūrākau were relatable and this appeared to be a safe way to explore aspects of mental illness. The inclusion of ceremony such as pure (spiritual cleansing) at the beach was also appreciated as a method of acknowledging challenges and creating intentions with positive future-orientated goals.
I think it is important, because before knowing and finding my iwi [tribe] and before going on that Māori journey, which is recent, I didn’t know anything. So then learning karakia, and singing waiata and learning about the atua (Māori gods), was a huge deal because I knew nothing about it, and I could relate to those stories. (Ana)
Tuakiri (identity, being Māori): a focus on cultural identity was deemed to be fundamental to the group’s success. Participants reported that they connected more to the group programme and its content as it was grounded within a Māori worldview. Culture, language, and identity being acknowledged and celebrated increased a sense of connection. The group community became the platform where participants developed their sense of identity and sense of self, and they felt stronger for it: And it hit my heart really hard and me really hard because part of it was based in Māori ancient things, it connected with me a lot more, so it was a lot easier for me to take in and be like I want to be a strong wahine [woman] like the wāhine (women) back in the day. (Kahu)
A celebration at the end of the 8-week programme included a graduation ceremony wearing traditional attire. One participant shared how wearing moko kauae (a traditional chin tattoo) was a dream of hers, and she enjoyed being able to wear a temporary version for the group graduation photos. Another participant shared that when her whole identity and culture were recognised and understood it felt less likely that she would be labelled with a mental illness but rather be seen and treated as a whole person.
Two participants spoke of how connection to cultural identity had not been important in the past. One shared how she had not previously felt pride in her identity. The knowledge and practices explored within the group had changed her perceptions of identity. Within the group participants had the opportunity to learn some history of Aotearoa New Zealand, colonisation, and the impacts for Māori. Information was enlightening and fostered an appreciation of the Māori language, a pride in the culture, and an understanding of the significance of some practices. Seeing this pride reflected in others, understanding the history, and gaining knowledge of culture, language and identity was seen as important for mitigating ignorance and negative perceptions in the media or in others.
Learning the history of New Zealand was a huge eye opener to me. Before that I had no idea so learning about it was really helpful. Beforehand, I wouldn’t say I was embarrassed but I definitely wasn’t proud to be Māori. But now I am. (Ana)
These aspects were highlighted as being unique to kaupapa Māori services. In contrast, previous experiences with non-Māori services lacked an acknowledgement of culture, language or identity. Participants spoke of actively trying to connect, and where Māori identity was not acknowledged it felt disrespectful and led to disengagement and disconnection.
Mauri (life force, essence): the mauri or essence of the group programme was experienced as an energy that supported participants to feel happy and comfortable in the space, trust in the group process, and connect. The mauri of the group programme was seen as holistic and more conducive to healing and wellness. One participant explained that she did not want to only focus on her mental health, as it was important to her that others understood her context, her family, her spirituality, and all that she brought with her. Without this mauri within the group programme any attempts to support her mental wellbeing would not work: Because who wants to go into a session and all they’ve got to talk about is what’s going on in my head? If you want to get to know who I am and understand me, that’s part of where we need to start. But if you don’t know how to connect with me on a spiritual basis, or basis of where I’m coming from, then it’s not going to work out. (Tui)
Having spaces that reflected the Māori world made group programme feel less clinical. When compared to other groups offered by mainstream organisations, participants preferred the kaupapa Māori group. They reported that it felt that it was more whānau (family) focused and a more comfortable, relaxed space. Previous experiences with other non-kaupapa Māori groups had felt like the agenda took priority whereas this group was described as more flexible and accommodating to their needs on a day-to-day basis.
The other [non-Māori] group was really good, but it felt like a tick box. Like they just had to check everything off and send you on your way sort of thing. It was still good, and they knew what they were doing but coming to [Kaupapa Māori group] was so much better—more family orientated and more homely. (Hine)
Mana (prestige, power)
The theme of mana emerged from discussions around the group programme’s impact on self-esteem, respectful interactions, and feeling valued and honoured by others. Sub-themes identified were mana wāhine, emphasising the participants’ own sense of mana; mana whānau (prestige and dignity of the family), where their whānau was acknowledged and respected, and mana tamariki (prestige and dignity of children), where the mana of their baby or children was upheld and considered. These aspects of mana were all perceived to be prioritised by the group facilitators and appeared to be the ultimate outcome of the group programme.
Mana wāhine (prestige and dignity of women): participants discussed that even though there were differences with unique and diverse experiences between group members, the commonalities of shared experiences of parenthood, mental health distress and as wāhine Māori (Māori women), was unifying and validating. They felt seen and honoured. The lack of judgement within the group was mentioned frequently by participants. One participant spoke of not wanting to be labelled and judged and being more likely to return to a place where she did not experience this. Being respected and responded to in an honouring way enhanced her sense of mana.
I think in all honesty a big reason why it worked so well was because I honoured and valued their input just as much as they valued mine. It was a reciprocated feeling. It felt like my opinion was important. But not just that. I think the respect that I gave them made them feel more comfortable to be better able to support me. (Kahu)
Participants who had completed the peer support training felt confident enough to support a group themselves, organising activities and developing their own resources. The development of leadership skills plus being able to manaaki (show care and respect for) others contributed to participants own sense of mana and wellbeing: My partner and I were talking the other day about me being a support for the group this time. I had not noticed, but he was like you know what’s really cool is that the mums probably look at you the way that you were looking at your support team when you were in there. I said, don’t say that—they were amazing, I looked at them like they all had their stuff sorted, they were incredible women. He was like, yes, that’s probably how they see you right now. And I was like, gosh, really? It was just cool to kind of be like a broken shell to now being like a strong mama. (Kahu)
The experience of participating in the group programme developed a sense of self-respect and positively impacted participants’ mana. Participants reported feeling validated, recognised as a parent, and being of value in the world. Previously, the participants explained that mental distress had inhibited them from recognising their own value or mana. An increased sense of mana was a motivating force. For example, one participant discussed finding the confidence to enrol in university because of the strength and belief in herself she had gained during the programme. Another spoke about the value of having new things to look forward to or to build into their life, of being able to find their voice and gaining clarity of their thoughts. Mana gains supported them to manage challenging days long after the group was completed. Completing the group pathway provided a sense of accomplishment with the graduation ceremony and presentation of certificates reinforcing this achievement.
Participants felt respected and honoured by other group members, with the reciprocity between group members and facilitators meaning everyone’s input and stories had equal value. Mana wāhine was elevated through the group as it provided a community where they had an equal place of standing, a place where they belonged, where they were just as important as other community members.
Mana whānau (prestige and dignity of the family): mana whānau referred to the impact on the group on the wider family. Participants spoke of how the positive changes within themselves had positively impacted their immediate household and wider whānau. Engagement in customary practices benefitted the whole whānau as the participants shared their experiences and practices. One participant spoke about her partner’s strong engagement with the Māori language and culture. Developing her own confidence in these practices had strengthened their relationship.
My partner is led by his culture, you know, he works in a Māori organisation, and he does all the pōwhiri [welcoming ceremonies] and he lives in that world. When I was going through my troubles, and I got really depressed, I found te ao Māori [the Māori world] and that’s what lifted my spirits and connected me. So, I felt it rescued me. And he wants to live his life that way, you know, it resonates with him. (Manaia)
Participants spoke of the burden they felt of being the primary support person for their partners. Being the primary support added further stress, exacerbating any existing mental distress they were experiencing. The skills acquired during group helped them to feel better equipped to support partners or other whānau, and this strengthened their relationships and supported them to navigate challenges together with their whānau.
They didn’t only help me, but helped me with trying to help my partner as well, because he has underlying issues. He was at rock bottom and things were not good for him. At that point in time, it was really bad. We got in touch with the Men’s Centre for counselling and we’re in a good place now where we can talk about stuff. (Kiri)
Mana tamariki (prestige and dignity of children): mana tamariki referred to the babies and children of participants being honoured and cared for. The group programme functioned as a place to go with their children and was seen as a physically, emotionally, and spiritually safe space for their children. Protecting the mana of their children was important. Participants were concerned about their children being labelled if they displayed behavioural issues or if their parenting was judged negatively. They felt that a kaupapa Māori group was less likely to label, whereas the wider mental health system tended to resort to labels and diagnoses. For some, this had been their experience as children, and they did not want that for their own child: I don’t want my kids labelled like I was. I don’t want to make them feel like they’re any less of a person, like I was made to feel. That was the hardest thing for me. The Māori Kaupapa [as stated by the participant] organisations don’t label you. They would never label anybody. And that’s the best thing about it. (Tui)
Aspiring to be the best parent possible for their children was also cited as being a motivating factor for attending group. Participants shared how they felt that their children deserved a parent who was happy and well, and if they were well, their children would be well. Participants felt strongly that more opportunities and options for groups that could be attended with their children were needed in the perinatal space.
But I know there was a huge change in me, and in the household, when I started going to the group. I started feeling so much better, and more confident in going out. (Ana)
Discussion
This study elucidates the important role of relationships, community, and cultural identity within the perinatal period for Māori mothers and birthing parents. Mana of the participants, their whānau, and their children was the ultimate outcome of this group programme, with all aspects of the participants’ mana being elevated and respected throughout. Outcomes that contributed to mana were identified by participants as increased confidence and self-esteem, strengthened identity, deeper connections and community, self-determination and improved mental wellbeing. These were facilitated by whanaungatanga, tikanga, and kaupapa Māori. Participants of this study identified that kaupapa Māori and Māori values were instrumental in providing a culturally responsive and safe environment. This environment supported ongoing engagement with a perinatal mental health intervention that was responsive and effective for Māori mothers and birthing parents within a health system that is often unsafe and discriminatory for whānau Māori (Cormack et al., 2018; Thayer et al., 2019).
Whanaungatanga is key to facilitating and maintaining engagement (Pitama et al., 2017) and arguably increased engagement provides increased opportunities to improve symptoms of mental distress. As described within this study, increased engagement with a group intervention generated kotahitanga, and created strong relationships, which provided a sense of belonging, unity, and connectedness between group participants. The wider literature corroborates the positive impact of supportive relationships on mental wellbeing in the perinatal period (Evans et al., 2020; Meredith et al., 2023; Worrall et al., 2018). The effectiveness of this group intervention aligns with previous research demonstrating the positive impact group interventions have on mental health outcomes (Cruwys et al., 2020; Jones et al., 2014; Rice et al., 2022; Seymour-Smith et al., 2017). In addition, offers of support are more likely to be volunteered and accepted between group members, within the context of a shared identity (Seymour-Smith et al., 2017), explaining the success and positive experiences related to relationships with peer support mentors (PSM) found in this study. This finding adds to the increasing body of evidence demonstrating PSMs can destigmatise and validate the experience of people with perinatal mental illness and provide benefits to both peer mentor and mentee (Faulkner & Kalathil, 2012; Jones et al., 2014; Oetzel et al., 2024; Rice et al., 2022).
The unique qualities of kaupapa Māori approaches to the group delivery were highlighted by this study to be instrumental in the effectiveness of the perinatal mental health intervention. This included devolving the power dynamics traditionally held by health practitioners in western biomedical interventions, allowing for deeper connections to occur between facilitators and group participants (Bennett & Liu, 2018; Rolleston et al., 2020). Findings highlighted the value and effectiveness of utilising customary practices as supported by a vast range of literature demonstrating the inclusion of customary practices being crucial both within the perinatal period and within mental health interventions for Māori and Indigenous populations (Adcock et al., 2021; Ansloos et al., 2019; McLachlan et al., 2021; V. Smith, 2017; Te Huia et al., 2023; Thompson et al., 2017). Adaptation of therapeutic spaces to best serve a community’s unique needs aligns with the literature on culturally responsive care (Quimby & Agonafer, 2022). Kaupapa Māori approaches embed a “whānau principle” (L. Smith, 2012, p. 187) and centre Māori identity, practices, and understanding of the world (Kopua et al., 2020). Utilising toi Māori (traditional Māori creative arts) is known to transmit ancestral knowledge, strengthen cultural identity, and pass down traditional cultural skills such as weaving. These cultural activities provide therapeutic value, contributing to mental wellbeing (McLachlan et al., 2021). Kaupapa Māori interventions are well established in Aotearoa New Zealand despite continued tensions round secured funding availability within the dominant western health system (Crengle, 2000; Rolleston et al., 2020).
The positive mana enhancing outcomes described in this study appeared to mitigate the impact of racism, discrimination, and perceived judgement experienced by Māori mothers and birthing parents and their whānau elsewhere in the health system (Cormack et al., 2018; Reid et al., 2019; Thayer et al., 2019, 2023). For Māori mothers and birthing parents, the fear of judgement is not unwarranted. Māori have for generations faced scrutiny and judgement in the face of western and racist ideals of a good mother (Gabel, 2019; Neely et al., 2023). Consistent with international evidence, the link between the experience of racism and its negative effects on mental wellbeing is well established within Aotearoa New Zealand (Becares & Atatoa-Carr, 2016; Cormack et al., 2018; Talamaivao et al., 2020). Despite this, limited research exists on effective interventions that may mitigate the impact of racism on health (Talamaivao et al., 2020). A strength of this study is the prominence given to Māori mothers and birthing parents’ perspectives, providing rich qualitative data that describe several buffers to the discriminatory interactions experienced elsewhere in the health system. This study also offers key insights from Māori mothers and birthing parents around what constitutes an effective and engaging perinatal mental health intervention. Limitations of this study relate to the size of the sample of participants and the generalisability of this small cohort to other Māori communities and experiences.
Conclusion
There have been several urgent calls for the improvement of perinatal mental health care for Indigenous peoples both in Aotearoa New Zealand and internationally (Hickey et al., 2021; Law et al., 2021; PMMRC, 2022; Walker, 2022). This article provides evidence centred on the perspectives of Māori mothers and birthing parents highlighting key factors that increase and support ongoing engagement with perinatal mental health services. This is an important research outcome, given the inequities experienced by whānau Māori in the perinatal period. It is imperative that perinatal mental health care for Māori considers the context of colonialism, experiences of racism, and the concepts of health, parenting and culture that are important to the community it serves.
The whakataukī at the beginning of this article alludes to the strength found within a collective. This collective strength was clearly identified by the research participants as being a key factor of an effective approach to perinatal mental health care. The results of this study support the design of future programmes in Aotearoa New Zealand, that encompass kaupapa Māori approaches for perinatal mental health that encourage community building through whanaungatanga, the integration of tikanga and customary practices, and supporting Māori mothers and birthing parents to develop skills in peer support.
Footnotes
Acknowledgements
The authors acknowledge the participants of this research study, without whom this mahi would not have been possible. We also acknowledge the Health Research Council of New Zealand for their support of the project in the form of a Māori Clinical Research Training Fellowship.
Authors’ note
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: Cara Meredith is the recipient of the Health Research Council of New Zealand—Māori Clinical Research Training Fellowship (grant no: 22/501).
Glossary
atua Māori gods
harakeke flax
hononga tautoko supportive relationships
iwi tribe
kai food
karakia blessings, prayers
kaupapa processes
kaupapa Māori Māori approach
kotahitanga unity, community
manaaki show care and respect for
manaakitanga respect and care for others
Māori Indigenous peoples of New Zealand
mana prestige, power
mana wāhine prestige and dignity of women
mana whānau prestige and dignity of the family
mana tamariki prestige and dignity of children
mātauranga Māori traditional Māori knowledge
mauri life force, essence
moko kauae a traditional chin tattoo
poi a light ball tied onto a string used for Māori performance art
pōwhiri welcoming ceremonies
pūrākau myths, stories
pure spiritual cleansing
rēwana a Māori sourdough bread
taonga tuku iho customary practices
te ao Māori the Māori world
tikanga cultural customs, conventions
tikanga haumaru safety
toi Māori traditional Māori creative arts
tuakiri identity, being Māori
tūhono connection
wahine woman
wāhine women
wāhine Māori Māori women
waiata traditional songs
whakataukī a Māori proverb
whakawhanaungatanga process of establishing relationships
whānau family
whānau Māori Māori families
whanaungatanga relationship building