
Abstract
The Pacific Islander and Māori (Indigenous peoples of New Zealand) community in Queensland are disproportionately affected by type 2 diabetes mellitus and suboptimal diabetes outcomes have been attributed to medication nonadherence. The study explored how Pacific Islander and Māori peoples with type 2 diabetes mellitus approach medication adherence. Talanoa (Indigenous Pacific form of communicating through storytelling) methods supported discussions that focused on exploration of beliefs about medication management. Discussions were analysed using inductive and deductive thematic analysis. Eighteen participants were involved in discussions. Themes included (1) cultural identity influences how participants approached medication management, (2) emotional response to diabetes: expressing stigma, shame and embarrassment in relation to diabetes, and (3) participant beliefs and perceptions about diabetes and medications that differed with health care professionals. Overall, the research gives insight into the importance of considering cultural identity, beliefs and emotions in Pacific Islander and Māori community members with type 2 diabetes mellitus to better support medication adherence.
Keywords
Introduction
Diabetes is an international health priority and global epidemic affecting 451 million individuals worldwide (Cho et al., 2018). Type 2 diabetes mellitus (T2DM) represents the majority (85%–90%) of all diabetes cases and is a major cause of blindness, end-stage renal disease, coronary heart disease and stroke (Australian Institute of Health and Welfare, 2023; Harding et al., 2019; Zheng et al., 2018). The National Diabetes Strategy has identified T2DM as the sixth leading cause of morbidity in some culturally and linguistically diverse (CALD) communities in Australia (National Diabetes Strategy Advisory Group, 2015). Pacific Islander and Māori (Indigenous peoples of New Zealand) communities have some of the most significant rates of T2DM compared to the rest of the world. In Australia, Pacific Island born men and women were 6.3 and 7.2 times more likely to develop T2DM, compared to the general population (Abouzeid et al., 2013; Colagiuri, 2017). Pacific Islander and Māori communities in Australia were also found to have significantly higher rates of diabetes-related hospital separations, diabetes-related complications and mortality compared to the general Australian population (Australian Institute of Health and Welfare, 2006; Colagiuri et al., 2007; Queensland Health, 2011). Despite these statistics, the prevalence and impact of T2DM within Australia’s Pacific Islander and Māori communities are underreported. Historically, health data for these groups have been inadequately captured because data collection methods focused on country of birth and language spoken at home rather than ethnicity. The 2021 Census has since recorded detailed information on ethnicity and cultural heritage (Australian Bureau of Statistics, 2021). Even with this advancement, diabetes statistics for Pacific Islanders migrating through New Zealand and the Māori population still remains significantly overlooked.
One of the factors identified as a contributor to poor glycaemic control and higher rates of diabetes-related mortality in the Pacific Islander and Māori community in Australia and New Zealand is medication nonadherence (Akbar, 2018; Chepulis et al., 2020; Horsburgh et al., 2019). The World Health Organization defines adherence to long-term therapy as the extent to which a person’s behaviour—taking medication, following a diet, and executing lifestyle changes corresponds with agreed recommendations from a health care provider (Sabaté, 2003). Studies identified that lower levels of medication adherence in Pacific Islander and Māori peoples might be driven by socioeconomic barriers to health care access, however after adjusting for socioeconomic deprivation, difficulties with medication adherence persisted, suggesting other factors may play an important role (Asiri et al., 2023; Horsburgh et al., 2019). Additional challenges the Pacific Islander and Māori community in South-East Queensland have been identified to experience, include navigating language and communication barriers, a new or unfamiliar health care system, lower levels of health literacy, socioeconomic adversity, and different cultural beliefs (Queensland Health, 2011; Sabaté, 2003). Some studies provide evidence to suggest that cultural identity, environmental factors, beliefs and perceptions of the Pacific Islander and Māori community often underpin behaviours around diabetes and chronic disease management including medication adherence (Akbar et al., 2021; Chang Wai et al., 2010).
Pacific peoples or Pasifika (people from the islands of the South Pacific and their descendants) collectively acknowledges the diverse nationalities, ethnic groups, and languages found within the Pacific region. In Queensland, Pacific Islander and Māori communities are often grouped together due to shared cultural traits, geographical proximity to the Pacific, and the relatively small population sizes of some groups in the region (Fa’avale & Fa’avale, 2020). Despite this grouping, it’s important to recognise and respect their distinct traditions and customs. Health and well-being are conceptualised similarly across Pacific Islander and Māori cultural groups, encompassing spiritual, mental, and physical aspects. This holistic view of well-being extends beyond individuals to include communities, the environment, and their interconnected relationships. This perspective is closely tied to cultural identity, which integrates principles of holism, collectivism, and spirituality—found in various Pacific Health Models (Agnew et al., 2004; Healthify, 2021; Ministry of Health, 2014; Tiatia, 2008). Cultural identity among Pacific Islander and Māori communities is integral to their sense of self, shaped by shared characteristics such as ethnic origins, language, religion, and social behaviours (Fu, 2024). These shared beliefs and norms influence health-related decision-making within families, villages, communities, and religious contexts. Understanding these cultural dimensions is crucial in exploring how Pacific Islander and Māori perspectives influence their experiences, beliefs, and behaviours related to T2DM and medication adherence. This research seeks to work with the community to better understand how culture influences experiences, beliefs and behaviours of Pacific Islander and Māori people with T2DM in relation to their medication.
Study objective
To explore how the Pacific Islander and Māori people in Queensland approach medication management.
Methods
Study design
This study used a qualitative descriptive approach informed by narrative inquiry, suited to exploring participants’ lived experiences with T2DM. Discussions were conducted using Pacific storytelling methods, talanoa (Indigenous Pacific form of communicating through storytelling) to engage participants in discussion about diabetes and medications, as well as influences on medication adherence and support for diabetes management (Suaalii-Sauni & Fulu-Aiolupotea, 2014; Vaioleti, 2013). In a research context, it involves sharing stories, co-developing knowledge and building mutual trust and cultural respect between the researcher and participants (Vaioleti, 2013). This culturally appropriate approach supported open, participant-led conversations and provided meaningful insights into medication adherence. The principal investigator (NT) received support from an experienced Pacific Islander researcher who guided NT in conducting talanoa effectively, drawing upon her expertise in diabetes self-management to navigate cultural nuances and engage the community (Akbar et al., 2021).
Ethical considerations and community involvement
The study was developed in consultation with a steering committee comprising elders and members of the Pacific Islander and Māori communities in Queensland. The committee also provided input throughout the project. Ethics approval was obtained from The University of Queensland Health and Behavioural Sciences, Low & Negligible Risk Ethics Sub-Committee (Approval Number: 2020001218).
Participant eligibility
Inclusion criteria were adults of Māori or Pacific Islander descent, diagnosed with T2DM, prescribed at least one diabetes-related medication and residing in Queensland.
Exclusion criteria included individuals with diet-controlled T2DM, type 1 diabetes or gestational diabetes.
Recruitment
Participants were recruited from the community using strategies including advertisements, Pacific Islander and Māori Facebook groups and ethnic radio broadcasting over a 6-month period. The steering committee network was used to circulate participant information flyers to Pacific Islander and Māori community members and organisations. These community facilitators helped build trust and encouraged participation among eligible individuals. Interested individuals contacted NT directly for further information. Snowball sampling was then employed, with participants referring other participants within their networks. All individuals who expressed interest and met the criteria were invited to take part. Each participant provided written or verbal consent. Participants were required to have a basic level of English or a family member or support person available to interpret.
Approach, tools and data collection
Discussions were conducted by NT using Zoom video-conferencing software or by phone call, depending on participant preference and COVID-19 restrictions at the time. All discussions were audio-recorded and transcribed verbatim for thematic analysis. NT was a member of the Pacific Islander community by marriage and has experience in qualitative research. NT led all discussions using the talanoa method and was guided by the overall objectives of the research to shape discussion. A demographic questionnaire was administered to gather basic background information, including participants’ age, gender, cultural background, length of time living in Australia or New Zealand, and their diabetes history. This helped contextualise their experiences during the discussions.
In addition, the validated Medicine Adherence Questionnaire (MAQ)—Morisky Green and Levine version (MAQ-MGL) in its original English-language form was completed, as all participants had a basic understanding of English or were supported by a family member or interpreter (Morisky et al., 1986). The MAQ-MGL adherence questionnaire is a yes or no questionnaire, with a 4-point scale indicating adherence (0 points) or nonadherence (⩾1 point). This version of the MAQ-MGL was chosen for its simplicity and reliability in assessing adherence to diabetes medications. The yes/no format offers a clear and standardised measure of adherence, which was further contextualised through the talanoa discussions, where participants elaborated on their medication-taking behaviours and the factors influencing their adherence. The combination of quantitative MAQ-MGL and qualitative talanoa data provided a comprehensive view of medication adherence. The medication adherence questionnaire was used to assess adherence to diabetes medications and medicines for complications of diabetes. The MAQ-MGL adherence questionnaire was selected as it has been validated against objective measures of adherence and provides a means of both measuring and understanding medication adherence (Morisky et al., 1986). It has been utilised in a randomised controlled trial to measure and understand adherence and tailor interventions accordingly—successfully improving medication adherence (Nguyen et al., 2016).
Reflexivity and validation
A reflective journal was used by NT throughout the study to record thoughts, themes and codes. Reflexivity allowed the primary research to reflect upon their own inherent biases, experiences and knowledge and how this might have impacted communication, interpretation of results and analysis of data, supporting the study’s confirmability. To enhance credibility, a summary of the discussion was emailed to participants after the talanoa to allow them an opportunity to comment on or clarify any aspect of the summary. Dependability was enhanced through documentation of the research process, coding decisions, and theme development, along with ongoing consultation with the research team during analysis. Transferability was not the primary aim of this study, but detailed demographic and contextual information is provided to assist readers in determining the relevance of the findings to other settings.
Data analysis
Demographic information was descriptively analysed and tabulated. Discussions were recorded and transcribed verbatim by the principal researcher and using a certified transcription service. Transcribed notes were imported into NVivo 12Plus software for data management. Inductive and deductive thematic analysis described by Braun and Clarke (2013) was used to identify influences on diabetes management, including medication adherence. The Social Cognitive Theory was applied as the framework for deductive analysis, examining how individuals’ cognitive, behavioural, and personal factors influenced medication adherence (Bandura, 2002). The data were manually coded to identify recurring themes and phrases. The coding process involved reading transcripts multiple times to gain depth of understanding. Initial codes and ideas were generated and grouped into key themes and subthemes. These were continually reviewed and discussed within the research team (NC, HA, and AL) to ensure reliability and to achieve consensus and are presented in the results. Recruitment and discussions with participants continued until thematic saturation was achieved (Braun and Clarke, 2013).
Results
Participants
A total of 18 discussions were conducted with Pacific Islander and Māori participants living with T2DM, recruited through snowball sampling and community-based outreach methods. The final number of participants was determined by the point at which no new themes were emerging from the data, consistent with the principle of data saturation in qualitative research. The median duration of discussions was 79 min (minimum = 37 min; maximum = 139 min). There were eight male and 10 female participants with 61 percent identifying as a single ethnicity and 39 percent of participants identifying as mixed ethnicity. Twenty-six different ethnicities were reported between participants. The largest number of participants identified as Fijian (7), followed by Tongan (5), Samoan (4), Cook Islander (2), Māori (1) and Rotuman (1). Participants identified as mixed Pacific Islander heritage (1), mixed Pacific Islander heritage and Non-Pacific Islander heritage (2), or had resided in Australia or New Zealand for over 10 years (13). Forty-four percent of participants had lived with T2DM for 5–10 years and 39 percent of participants were >10 years since diabetes diagnosis. Table 1 provides a summary of demographic data.
Demographic and characteristics of Pacific Islander and Māori participants.
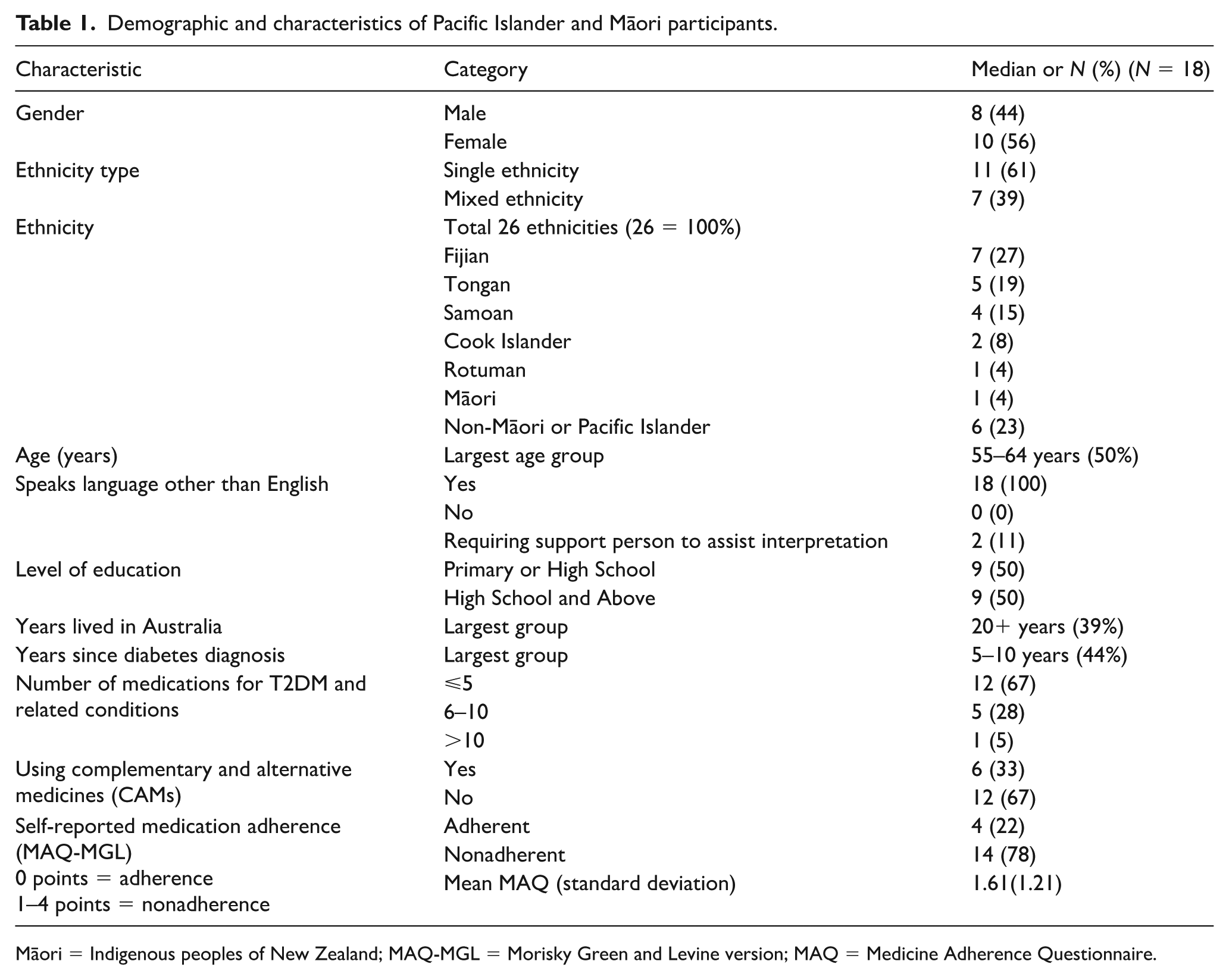
Māori = Indigenous peoples of New Zealand; MAQ-MGL = Morisky Green and Levine version; MAQ = Medicine Adherence Questionnaire.
Seventy-eight percent of patients were nonadherent according to the MAQ-MGL. There were multiple instances where patients answered yes to a question in the MAQ-MGL, however discussion suggested the patient should have answered no. As such, there is less emphasis on the MAQ-MGL questionnaire in this study, and it is suggested that further research might consider more rigorous validation of the MAQ-MGL in the Pacific Islander and Māori community to investigate its appropriateness and cultural acceptability.
Findings
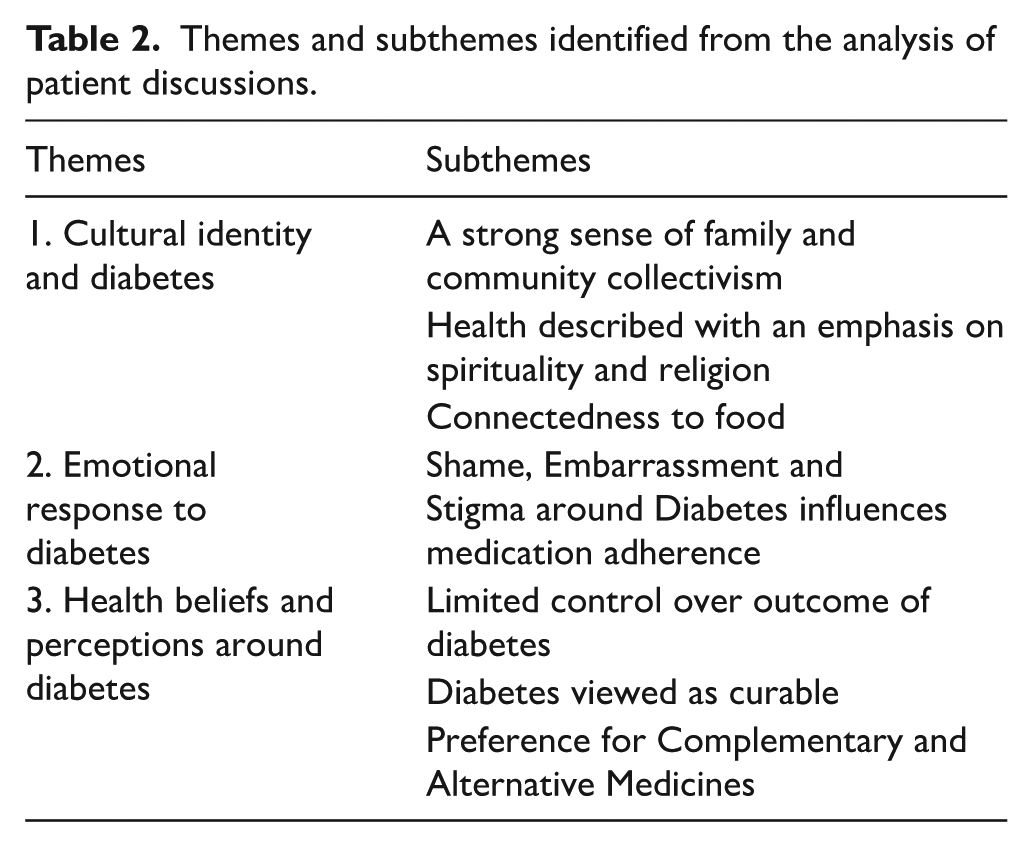
Three main themes and eight subthemes emerged from the analysis (Table 2). The themes and subthemes are interconnected and influenced adherence to medications for T2DM in different ways. All participants identified cultural identity as an important part of their life and the way they managed their medications, influencing health beliefs and perceptions around medications and the patients’ emotional response to T2DM. Despite many participants identifying similar factors influencing medication-taking behaviour, how these factors influenced each individual participant varied.
Themes and subthemes identified from the analysis of patient discussions.
Theme 1: cultural identity and diabetes
Participants identified the importance of cultural identity in the context of medication management, with particular emphasis on family and community collectivism, spirituality and religion, and a connectedness to food.
A strong sense of family and community collectivism
Pacific Islander and Māori participants explained their culture as family and community oriented. Some individuals articulated how family were a fundamental motivator for maintaining their health, underscoring their intrinsic desire to contribute to their family’s well-being through healthy living. Participants highlighted the collective strength of the family unit, describing how family members often reminded them to take their medications and supported them to attend appointments.
Conversely, participants explained how family, nuclear and extended, and community influences presented challenges for managing diabetes. Just as food was often shared between household members, some participants also shared their medications with family in Australia or overseas. Participants’ decisions around medication-taking were prioritised around responsibilities and obligations within their family, community and church and many participants expressed a desire to put their family first and did not want to burden the family with concerns about their health. A Cook Islander participant explained the importance of prioritising family or community needs before buying medication for themselves; “I’d spend $200 on medication. I could be spending that on someone else, helping them . . . . And I think that’s a cultural thing. That’s something that’s a value thing in my family.” (P8, female, 45–54 years)
Respect systems were explained to be of significance within the Pacific culture. These were defined by the way in which younger members of the family or community regarded the feelings and wishes of their elders with great importance. In such instances, younger carers would often adhere to fulfilling the cultural expectations of elders when it came to making decisions about the elder’s health, regardless of the consequences. For example, some family members avoided communicating their concerns to older family members with diabetes, despite acknowledging that their elders were not adherent to dietary requirements or taking medications. A Fijian participant, while recognising the cultural expectation of respecting elders, sought to subvert that expectation:
I’m very well known in our communities for being very outspoken . . . . If I see aunties sitting there feasting . . . I’m in their face, ‘Have you had your meds?’, ‘Why have you not had your meds?’. . . Which is why I’m totally disrespectful. (P5, female, 45–54 years)
Health described with an emphasis on spirituality and religion
The majority of participants described spirituality and their belief in God as an important part of their life and connected to their cultural identity. Spirituality and religion were described as important with respect to overall well-being. Some participants appealed to religious beliefs as a reason to take their medicines and look after their health, while others referred to their religious beliefs as a reason not to take medicines.
Spiritual health and living life to get to heaven, sometimes conflicted with attending to physical health. A Fijian participant described how her religious beliefs had competed with taking medication in the past and believed that God would heal her diabetes; “I used to be hit and miss. There was a battle going on . . . in the word of God. It says, ‘by faith you’ll be healed.’ I quoted all those scriptures and everything, I knew I needed help” (P1, female, 55–64 years).
For other participants, religion reinforced adherence to medications. They expressed that religion and spirituality existed alongside taking medications and influenced how decisions were made about their diabetes management; “He says our body is the temple of the Holy Spirit. And so, if we take care, because our body is just not our body. It’s actually you know, our spirit that being, that comes from him” (P1, female, 55–64 years).
One Fijian participant described a positive interaction with a health care professional who had the same religious faith and would integrate this into consultations with the patient; “So after all this medication and everything, and he give you a little prayer and just one two lines of it. He said, you know, ‘The Lord will help you too’” (P10, female, >65 years).
Connectedness to food
Participants discussed the importance of food in relation to medication management. They explained how difficulty adhering to food recommendations often led to poor glycaemic control and this resulted in medication nonadherence or beliefs that medications were ineffective. One Tongan participant described giving up on his diabetes management altogether and had stopped taking his medications completely.
However, participants spoke about taking medications, so they could eat large portions of high carbohydrate foods, with the view that their medications would counteract any poor dietary choices:
That’s right you got to participate in the celebrations . . . I think part of the problem is we think that we can eat as much as we like, because there’s a tablet available. Thinking that the tablet will make up for the loads of sugar you just piled on in the feast. (P12, male, 45–54 years)
Theme 2: emotional response to diabetes
Some participants expressed a strong emotional response to diabetes and medication-taking. They expressed shame and embarrassment and a feeling of stigma around diabetes and medications. This response was described in relation to the challenges around diabetes management—particularly in the context of cultural identity and beliefs and perceptions around diabetes and medication management in the community.
Shame, embarrassment and stigma around diabetes influences medication adherence
Participants described the stigma attached to diabetes and taking medications and felt that they were often judged or blamed for their condition. Multiple participants referred to their desire not to have diabetes and to reduce or stop taking their medications altogether. Participants explained a sense of shame and embarrassment around diabetes and spoke about how it was uncommon for Pacific Islanders to discuss health matters with others. As a result, participants were reluctant to discuss diabetes or medications with friends and family, or seek help from health care professionals:
They feel like it’s such an embarrassment that they don’t tell people, so they don’t get the support . . . and people might judge you . . . ‘oh it’s because you eat too much’ . . . you know like there’s a bit of a stigma to it. (P4, female, 35–44 years)
One Tongan participant described the reluctance to discuss her health with family members because they would worry:
For me I think with our culture, it’s maybe an embarrassment to go to the doctor . . . . I found that when I moved here that everybody . . . I know they freely talk about their health problem . . . whereas in Tonga you know, you hardly share your health problem unless it’s something very serious and I think that’s part of the reason why we don’t really yeah often visit the doctor . . . . and we don’t want to worry your family when you have a health problem. (P11, female, 45–54 years)
Participants further expressed how feelings of shame and embarrassment led to denial. Some participants described how they initially ignored advice given to them by health care professionals to take their medications as they did not want to acknowledge that they had diabetes. A Tongan participant stated,
But sometimes it’s just hard cause I’m not thinking that it would happen to me . . . I think that’s denial . . . denial as well in medicine and stuff, but I do believe that it helps it works, but I was just sort of in that denial for a long time. (P6, male, 45–54 years)
Participants described how they became more serious about their diabetes management and adhered to their medications only after developing complications of diabetes or being admitted to hospital; “Wait until you got all the complications . . . diabetes is such a silent killer . . . I’m paying the consequences of that every day” (P1, female, 55–64 years).
Theme 3: health beliefs and perceptions around diabetes
Participants had beliefs and perceptions around medications that were often interlinked and influenced how they made decisions around medication-taking and sought out medical treatment. Some participants had perceptions that differed with health care professionals. This was sometimes as a result of cultural beliefs or due to incorrect interpretation or application of information to their circumstances.
Limited control over outcome of diabetes
Multiple participants expressed that they felt a lack of control around diabetes. One Samoan participant explained that despite her efforts to take her medications, that her treatment was unable to control her blood sugars, which almost led to medication nonadherence; “I was going to give up on my medication because I was like—what’s the point in doing medication and injecting myself when my readings are the same” (P4, female, 35–44 years).
Participants often described how taking medication and lifestyle management were not the only factors controlling their diabetes and that the condition was governed by forces beyond their control. While some described diabetes to be a result of fate or God’s will, others attributed diabetes to genetics. Regardless of the perceived cause, many participants described the outcomes of diabetes to be predetermined and inevitable. Although many participants were aware that their lifestyle and medication adherence had a significant role in management of their diabetes, they felt that regardless of their efforts, diabetes was unavoidable and often accepted outcomes of the condition.
Diabetes viewed as curable
Several Pacific Islander and Māori participants described a cluster of beliefs around diabetes that depicted T2DM as curable or short-term. Participants frequently discussed how community members sought guidance from respected elders or pastors, who advised that their diabetes could be entirely resolved through spiritual healing, dietary adjustments, or Complementary and Alternative Medicines (CAMs). Consequently, many participants aimed to discontinue their medications or were optimistic about the possibility of eventually ceasing their use. For most patients in this study, this information was inappropriately applied to their circumstances, where they aimed to stop their medications even though this conflicted with their doctor’s advice or they had late-stage diabetes and complications of diabetes.
One participant explained how she discontinued her medications when her blood sugars were in range as she thought that her diabetes was cured. Another participant used medications intermittently—only when their blood sugars were high. A Fijian participant who had been hospitalised due to diabetes complications, described how his diabetes was temporary and that he had been completely cured by changing his diet. He ceased his prescription medications, that he deemed ineffective for managing diabetes; “But if you eat right, you can reverse it . . . . It’s just my understanding of modern medicine, it’s a quick fix, it doesn’t cure the problem” (P2, male, 55–64 years).
Preference for complementary and alternative medicines
Some participants described a preference for CAMs that were often highly regarded and shared among members of the community. Participants described using noni juice, massage, multivitamins, Chinese traditional medicines, herbal teas such as turmeric, and rongoā (traditional Māori healing systems including native plant-based remedies, massage and spiritual healing). CAMs were described as safer alternatives compared to western treatments on the islands, where medications were often expired, costly or difficult to access. One Fijian participant described how using natural medicines was common on the islands; “Back home my sister’s got diabetes and she’s taking noni juice . . . more natural things because the metformin is just too expensive” (P1, female, 55–64 years).
In contrast to CAMs, patients considered prescription medications to be ineffective, unsafe or unnecessary in comparison. Diabetes medications were described as damaging chemicals by a Samoan couple:
People that we know, that are currently on dialysis. They said that their family members have been taking medication for diabetes . . . for the long run, they end up with dialysis, because their kidneys failed due to the long term of taking the medication for diabetes. (Wife of P7— male, 55–64 years) And that’s why I throw to the rubbish cause I can feel I know this is not working . . . when I drink that [take medication], I can feel the pain in my kidneys. (P7, male, 55–64 years)
Participants recounted how natural treatments were able to cure diabetes and compared this to prescription medications which were described as a temporary solution to controlling diabetes. Some participants chose to only use CAMs, to control their blood sugars—despite the doctor’s recommendations, while others utilised CAMs in addition to, or prior to commencing their prescription medications. A Fijian participant described a lack of trust in prescription medicines and therefore preferred natural treatments. He had ceased taking all his prescribed medications including insulin after a limb amputation, stating that he had reversed his diabetes completely with taking natural remedies:
I am not taking any medication, for almost 6 months now . . . I did a lot of research about Type 2 Diabetes and I looked at what the root cause is . . . I looked at the main organs that produce insulin, and if they’re not producing insulin they are not functioning . . . . I thought I would try a natural way [CAMs] to re-boost it and I’m really happy with it. (P2, male, 55–64 years)
Discussion
The study highlights how cultural identity, emotional responses, and health beliefs significantly impact diabetes management among Māori and Pacific Islanders. While family and community support both motivate and challenge adherence, stigma and shame hinder open communication and medication adherence. Many participants viewed diabetes as curable through spiritual or alternative methods, leading to the discontinuation of conventional treatments. These findings emphasise the need for culturally sensitive interventions to improve adherence, consistent with evidence on the role of cultural and emotional factors in chronic disease management.
Diabetes management challenges cultural identity
Maintaining a strong sense of cultural identity promotes resilience, self-esteem and security and can have a positive impact on the overall health and well-being of Pacific Islander and Māori peoples (Hokowhitu et al., 2020; Manuela & Sibley, 2013). Cultural identity can be defined as an essential part of an individual’s sense of self, defined by shared characteristics of a group of people, encompassing ethnic origins, language, religion and social behaviours (Fu, 2024). Participants in this study described cultural identity in terms of collectivism, spirituality and food. Collectivistic ideals were explained to include; responsibility and contribution to families and communities, respect systems and communal decision-making, spirituality or religion; including beliefs around healing and contribution of tithes for the church, and the centrality of food; including traditional foods and involvement in ceremonial and religious feasts. Such cultural characteristics have been described as important aspects of Pacific Islander and Māori cultural identity in the literature (Akbar et al., 2021; McElfish et al., 2018; McLaughlin & Braun, 1998; Ministry of Health, 2014; Stewart et al., 2012).
Cultural identity was described to be important by the participants in this study, regardless of age, whether participants identified as mixed-heritage or how long they had been living in Australia. It was unsurprising that cultural identity influenced the patient’s emotions, understanding and perceptions around taking prescription medications for T2DM. Akbar and colleagues (2021) describe how T2DM management prevented some Pacific Islander patients from being fully immersed in their culture. Pacific Islander communities have expressed how T2DM self-management precludes participation in important cultural events and impedes them from upholding religious ideologies or maintaining relational bonds to family and community (Akbar et al., 2021). For participants in this study who expressed these desires, they often decided to forgo medication-taking to retain their cultural identity.
It was evident from this study, that a large aspect of Pacific Islander and Māori cultural identity was collectivism, however this often conflicted with the ideals of diabetes management, including medication adherence. Collectivism has been described in the literature as reciprocal systems, where the people within them place higher value on the affiliation and interconnectedness with their extended family or community and put an emphasis on maintaining the well-being of the community as a whole (Manuela & Sibley, 2013). In this study, collectivism influenced medication adherence, as participants often had difficulty prioritising the cost of medications over the responsibilities and obligations of the family and greater community. Therefore, patients often struggled with the thought of buying their own medications before providing for the family. Collectivistic obligations and expectations were also described by a significant proportion (75.4%) of participants, in another study in relation to T2DM self-management activities in a cohort of 148 Pacific Islander women (Akbar, 2018; Akbar et al., 2021). For Pacific Islander patients, research reports T2DM self-management to sit uncomfortably with this community due to its individualistic approach, that focuses solely on the patient and their condition, overlooking the importance of the patient’s culture and collective circle of influence (Akbar et al., 2021). While this might be true, it appears that difficulties with T2DM medication management in this community, could be a combination of self-management being too individualistic and collectivistic cultural values making it challenging for patients to engage. It would be reasonable to suggest that reconciliation between individualised self-management goals and collectivistic patient values would be needed to accomplish patient–practitioner alignment for T2DM medication management.
Participants who experienced a misalignment between Pacific Islander and Māori cultural values and diabetes management, described emotions of shame and embarrassment. Participants described a reluctancy to tell others about their condition, to avoid being a burden on the family and privacy around health issues was often described as social norm among the community. For some participants this often led to denial of T2DM or a refusal to take medications, while other participants managed their diabetes alone, evading social support, disengaging with T2DM or delaying seeking treatment, compromising optimal medication management. Participants in other research also describe negative stereotyping and discrimination around diabetes, as reasons for keeping their condition and medications private (Akbar et al., 2022; Browne et al., 2013; McElfish et al., 2018). Similar to findings from other research, this study also suggests that a combination of emotional reactions, negative associations around diabetes, and previous experiences might extend the time patients take to acknowledge T2DM, seek health care and persist with mediation adherence long-term (Asiri et al., 2023; Horsburgh et al., 2019). The study highlights opportunities to more effectively align diabetes management strategies with cultural needs.
Cultural identity positively reinforces diabetes management
There is growing evidence for recognition and connection to culture, to enhance patient engagement and health outcomes in CALD populations (Verbunt et al., 2021). Studies highlight the importance of recognising cultural determinants of health and acknowledging Country, family and community and cultural identity in Indigenous communities in Australia to work towards cultural safety (Australian Institute of Health and Welfare, 2022; Child Safe Organisations National Principles, 2018; Verbunt et al., 2021). Research by Stewart et al., in an American Samoan community identified how participants indicated that motivators to good medication management included; the doctor’s respect for God and family and encouragement to proactively engage with diabetes self-care to honour their body and live longer for their family (Stewart et al., 2012). Similarly, Pacific Islander and Māori participants in this study emphasised the importance of health care professionals positively engaging with their culture. Integration of cultural ideals, such as the importance of family and religion or spirituality, not only motivated patients manage their diabetes and medications well but also deepened the relationship that they had with their health provider. Furthermore, for participants where practitioners integrated family support for taking medications, they described how it was easier to persist with medication-taking. The literature also suggests that patients who feel they are understood and respected by health care professionals are more likely to accept recommendations from health care professionals (King-Shier et al., 2017; Paez et al., 2009). Similarly, this study describes how increasing cultural bonds and developing trusting relationships with Pacific Islander and Māori patients, positively influences patients to be more amenable to the advice from health care professionals around the management of medications.
Beliefs that differed with health care professionals
People from culturally diverse groups often operate under different disease frameworks shaped by spiritual, religious, or traditional beliefs, which can lead them to dismiss conventional western health care in favour of spiritual practices and CAMs (Gurung, 2010). In this study, Pacific Islander and Māori participants exhibited beliefs and perceptions about medication management that frequently diverged from those of health care professionals, resulting in suboptimal management of T2DM. These differing beliefs sometimes caused participants to misinterpret or inaccurately apply medical information, undermining the effectiveness of their treatment.
Spiritual faith and healing as well as beliefs around traditional medicine frames Pacific Islander and Māori patient’s perceptions around diabetes and prescription medications (Bassett-Clarke et al., 2011; Bean et al., 2007; Stewart et al., 2012). As also stated in other studies, this study demonstrates that spiritual forces controlling health and spiritual healing as a coping mechanism or treatment for diabetes management are predominant views in Pacific Islander peoples (Bassett-Clarke et al., 2011; Capstick et al., 2009; Fabrega, 1972; Ihara & Vakalahi, 2011; Ministry of Health, 2008b). Spiritual healing and safer CAMs were also regarded as more effective cures for diabetes compared to prescription medications and this influenced medication adherence in some instances. A study by Bassett-Clarke et al. (2011) also explains how Pacific Islander and Māori peoples conceptualised prescription medication—describing how it only suppressed rather than cured their condition. Bean et al. (2007) and Barnes et al. (2004) confirm lower treatment control beliefs and perceptions around the acute nature of diabetes in Pacific Islander cohorts with T2DM, which were associated with lower levels of medication adherence. Barnes et al. (2004) further describe how spiritual beliefs might be the reason for such beliefs.
This study also proposes that beliefs around CAMs, may also have a role in influencing medication adherence in Pacific Islander communities. While CAMs were only noted by some patients to directly influence medication adherence in the current study, evidence from Barnes et al. (2004), Bean et al. (2007) and Bassett-Clarke et al. (2011), demonstrates how alternative therapies might have a greater magnitude of effect than what was described in the present study. For example, Bassett-Clarke et al. (2011) describe how use of rongoā in Māori patients often led to dual use of these therapies alongside prescription medication, despite limited evidence around interactions. Nonetheless, it is clear that differing perceptions between Pacific Islander and Māori participants and health care professionals around how T2DM is best managed, might preclude patients from being transparent about their alternative beliefs, interfering with multiple phases of medication adherence including; initiation, implementation and persistence. To address these challenges, health care professionals could look to more effectively engage with and respect patients’ knowledge systems by integrating cultural and traditional practices into care plans, thereby acknowledging diverse perspectives and fostering more effective and culturally sensitive health interventions.
Limitations
NT, a pharmacist and family member of the Pacific community, had an insider-outsider relationship with participants. This relationship facilitated trust-building but also created limitations, as some participants may have been reluctant to discuss sensitive issues, despite reassurances of confidentiality. The researcher reflected on this closeness to ensure biases did not influence data collection and analysis, maintaining a reflective journal throughout the study. The pharmacist role may have led some participants to withhold information about medication nonadherence due to perceived judgement or discomfort, which was considered. Additional attention was given to data from participants who involved a partner or nurse navigator for interpretation. Pacific Islander and Māori peoples come from a number of similar but distinct ethnic groups; however, the methods of this study did not allow for exploration of the differences between these groups. The small number of participants from some of these groups needs to be recognised in addition to the groups not represented in this sample.
Conclusion
The importance of respecting, encouraging and supporting Pacific Islander and Māori culture and understanding customs and traditions, is imperative when supporting diabetes management activities, including medication-taking. Health care professionals should be encouraged to gain an understanding of the culture, in order to develop positive relationships with people in a community where patient–practitioner trust is particularly important and may influence medication adherence (Ministry of Health, 2008a). This study supports the notion to integrate the patient’s cultural context and tailor support towards the patient, to more meaningfully engage Pacific Islander and Māori patients and improve T2DM management—specifically medication adherence (Akbar et al., 2021; McQuaid & Landier, 2018; Ministry of Health, 2014; Nguyen et al., 2016). Establishing the significance of traditional foods, spiritual practices, and CAMs for individual patients in the context of their community and jointly developing a management plan with the patient, can assist patients to achieve optimal management of diabetes and their medications. Development of resources and providing education that accounts for the different ways that this community views diabetes, is likely to improve understanding around diabetes and medication management, decrease communication barriers and increase access to appropriate resources and support. Healthcare professionals are encouraged to positively reinforce Pacific Islander and Māori culture through empowerment, utilising the collective nature of the community to drive positive health behaviours (Fogarty et al., 2018). Acknowledgement that distinct efforts are required to understand, respect and account for the deeply rooted aspects of cultural identity in Pacific Islander and Māori peoples is essential for supporting medication adherence and T2DM management in this community.
Footnotes
Acknowledgements
The authors thank all Māori and Pacific Islander patients who participated in the study and the leaders and community delegates for facilitating participation. The authors also congratulate Dr Neil Cottrell on his retirement and thank him for his involvement as an associate supervisor.
Authors’ Note
Funding
The authors received no financial support for the research, authorship, and publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Glossary
Māori the Indigenous peoples of New Zealand
Pasifika People from the islands of the South Pacific and their descendants
rongoā traditional Māori healing systems including native plant-based remedies, massage and spiritual healing
talanoa Indigenous Pacific form of communicating through storytelling