
Abstract
This study aims to explore the impacts of COVID-19 on birthing for wāhine (women) and whānau (immediate and extended family) in Aotearoa (New Zealand) during the lockdowns of 2020 and 2021. This rangahau (research) provided whānau with an opportunity to share their whakawhānau (birthing process) experiences via interviews. The data were analysed through interpretative phenomenological analysis. Themes identified in the results included the importance of whānau tautoko (family support), the experiences of isolation and trauma, and the effect of birthing under COVID-19 restrictions. Indigeneity was a core identity that was crucial to maintain, during these sacred times. Whakawhānau is a pivotal transition with the potential to engage with medical services. The findings of this study contribute to the knowledge of whānau Māori (Māori [Indigenous peoples of New Zealand] families) experiences to enhance service provision.
Introduction
Aotearoa (New Zealand) was impacted by COVID-19, and experienced changes in health care delivery, significantly affecting whānau (immediate and extended family) and wāhine (women), who gave birth during this time (Bloomfield, 2021). Nationwide level 4 lockdowns in March to April 2020 and August 2021 resulted in significant reprioritization of health care services (Bloomfield, 2021). Wāhine giving birth had to adapt to changing regulations and guidelines affecting maternity care clinicians, pregnant people, whānau, and their pēpi (infants) (Pavlidis et al., 2021). Lockdown measures were successful in keeping the burden of COVID-19 on health services contained. Those at the highest risk of morbidity and mortality related to COVID-19 include whānau Māori, due to the compounded effects of underlying health conditions, social determinants of health and wellbeing, colonisation, and structural racism (Steyn et al., 2020).
Understanding the impact of colonisation, which has resulted in historically unmet health need, is fundamental. Aotearoa has a long history of health outcomes for Māori (Indigenous peoples of New Zealand) that are not the same as those of Pākehā (New Zealanders of primarily European ancestry) (Durie, 2012). The differential effects on health outcomes seen in pandemics are an example of unmet health need. An example of colonisation and the systemic inequities that have persisted across time were seen in the 1918 influenza and the 2009 influenza pandemic death rates, rates of infection and severity being higher for Māori (Steyn et al., 2020). Furthermore, the effects of unmet health need, the impact of colonisation, and systemic inequity can be seen clearly in the realm of wāhine and pēpi health. For example, pēpi Māori are twice as likely to have a potentially preventable death and have higher neonatal intensive care unit admissions (Stevenson et al., 2016). All these areas are vulnerable to the impacts of COVID-19, especially during the level 4 nationwide lockdowns and the reprioritisation of health services which has the potential to amplify systemic inequity. Solutions to these systemic challenges in the wider context of health highlight the need for Kaupapa Māori (Māori-centric) rangahau (research) to meet the challenges faced by whānau Māori (Māori families) (Graham & Masters-Awatere, 2020). Other rangahau in the field of Māori maternal health indicates the importance of including tikanga (cultural protocols, customs, and practices) and mātauranga (knowledge), whānau systemic issues, and adaptation to parenthood for wāhine and their whānau in their journey through whakawhānau (birthing process) (Stevenson, 2018).
To achieve positive health outcomes, services, systems, and rangahau in relation to health, it is necessary to apply a broad perspective to the investigation of potential explanations. Focusing primarily on patient and Māori cultural explanations risks victim blaming and fails to acknowledge dominant cultural explanations, the role of providers, and structural influences (Harris et al., 2007). Previous rangahau indicated that health outcomes could be improved by focusing on what is vital to whānau Māori (Durie, 2012). The incorporation of mātauranga Māori (Māori knowledge) around birthing is essential for the protection and preservation of identity for wāhine Māori (Māori women) and vital for whānau wellbeing and empowerment. Creating space for Māori to share their own stories, experiences, and histories creates a pathway that has the power to facilitate healing in regard to validating the experiences of diverse whānau Māori (August, 2005).
This rangahau provides an opportunity to explore the impact of COVID-19 on whānau Māori and their birth experiences, by providing an opportunity to share their stories of birthing during the COVID-19 lockdown. The aim of sharing lived experiences and narratives allows for increased knowledge, understanding, and opportunities to enhance support service accessibility for whānau Māori in our changing world.
Methods
Study design
In areas of rangahau where ethnic inequities exist, priority needs to be given to the group with the inequity—their voice should be heard, and their reality understood. We undertook a qualitative study to provide insight into and understanding of participants’ lived experience as explored by other rangahau (Denny & Weckesser, 2019; Pope & Mays, 1995; Reid et al., 2017). Kaupapa Māori principals guided the study design and provided a structure in which the rangahau values and privileges Māori experiences leading to the challenging of current systems to enable system transformation and a pathway towards equity (Cram, 2019; Smith, 2019).
Study setting
Participants were whānau Māori recruited by invitation or self-recruitment through personal connections, who gave birth during COVID-19 national lockdowns between 2020 and 2021. Semi-structured interviews took place in two small rural localities in Te-Ika-a-Māui (North Island of New Zealand) and an urban city in Te Waipounamu (South Island of New Zealand). Participants chose to be interviewed either on their own or with whānau as a collective.
Data collection and analysis
Data collection occurred in participants’ homes or via Zoom. Interviews took approximately 1 hr and involved a range of open-ended and closed questions. Interviews were undertaken, recorded on an audio recording device, and transcribed into narratives for analysis. Interpretive phenomenology analysis was used alongside a grounded kaupapa Māori approach to analyse the experiences of the whānau participants and develop the experiences into key themes (Jones et al., 2010; Larkin et al., 2021; Struthers & Peden-McAlpine, 2005). The key themes identified in this article are grounded in the many ways the whānau participants made sense of their hapūtanga (pregnancy) experiences during the pandemic.
Approvals
Ethical approval by the Health and Disability Ethics Committee (HDEC), Aotearoa was obtained (21/057). Verbal and written consent was obtained from each participant.
Results–whānau voices
Participants (n = 5) included four whānau collectives. The participants interviewed ranged in age from 22 to 42 years old and included both wāhine and tāne (male). Three whānau experienced whakawhānau and hapūtanga in the first nationwide level 4 lockdown in 2020 and one in the subsequent nationwide lockdown in 2021. Two of the whānau lived in a rural area, and two lived in urban locations. The majority of whānau birthed in a hospital setting in contrast to the majority desired birthing location being either within a home birth setting or a primary birthing setting.
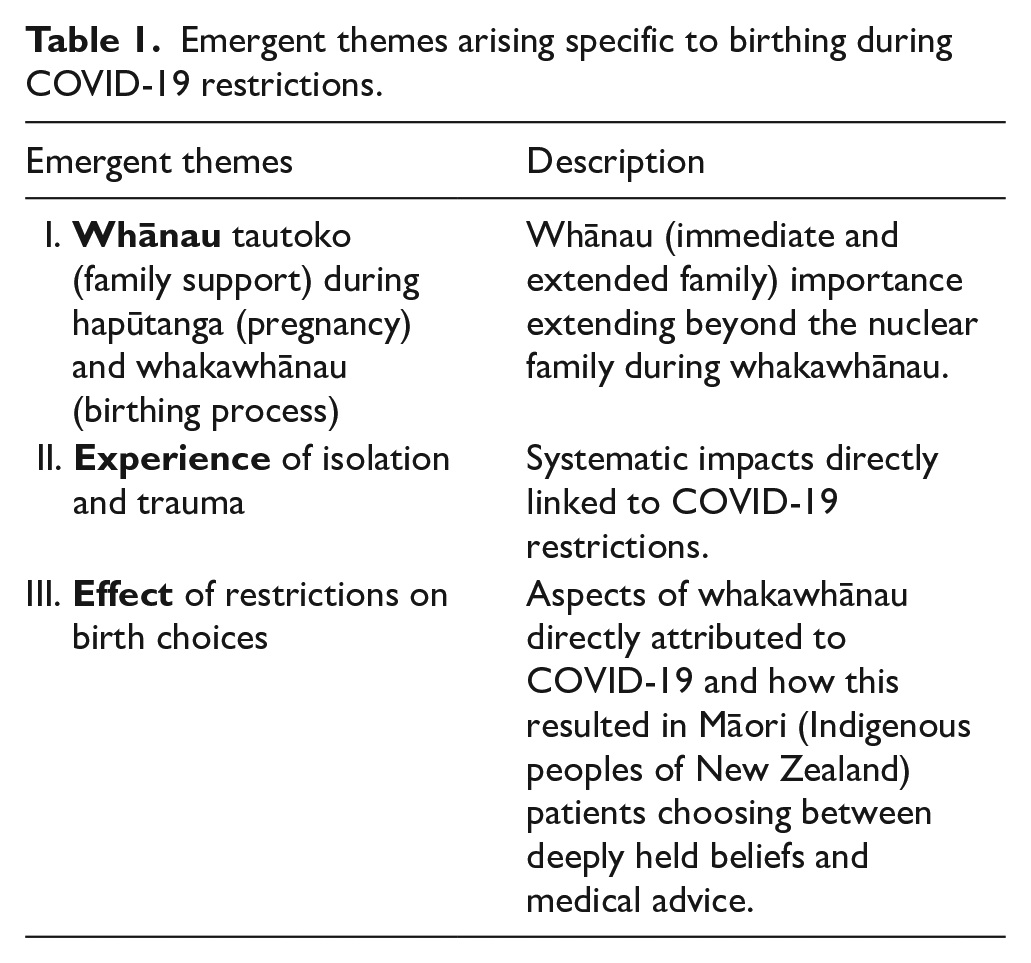
Three emergent themes were identified as part of the analysis of whānau voice. Each theme is discussed in the following sections leading with whānau quotes first and expansion of the theme following. Table 1 is provided at the end of this section to summarise the emergent themes.
Emergent themes arising specific to birthing during COVID-19 restrictions.
Context of whānau individuals interviewed
All the individuals interviewed shared views and experiences connected to the complexities of birthing, being a partner as part of a whānau context, and parenting during a time of global crisis. The themes pull together the difficulty of birthing in an environment of isolation and uncertainty. The participants have self-identified their relational ties to their whānau whether they are a māmā (mother) or pāpā (father). These identity roles within the context of the rangahau are important and serve to place their perspectives in the time period they have generously shared about.
Emergent theme 1—whānau tautoko (family support) for hapūtanga and whakawhānau process: We were raised by a whole village, and you usually feel the sense of that village more intensely once a baby is born into the world, but it couldn’t happen because of lockdown. I felt the weight of that, and the depression I went through afterwards got me real good. (Whānau Tahi, māmā, 30 years old)
The backbone of support during hapūtanga and whakawhānau was provided by whānau and was consistently reflected throughout the interviews. This theme showed the connection to a collective way of living as vital to the whakawhānau journey, and the absence of such led to apprehension about giving birth in the COVID-19 environment: I had to leave my partner on her own in the hospital with our new baby, it felt unnatural and wrong leaving the hospital when my partner only just had the baby that day on her own in a room full of strangers and their own babies. (Whānau Rua, pāpā, 34 years old)
The pāpā interviewed as part of Whānau Rua described being pushed into the corner which diminished his ability to be involved, or to advocate for their pēpi or partner. This impacted their sense of being able to be of support before and after the pēpi was born due to visitation restrictions: [my husband] come through this whole journey of hapūtanga, and whakawhānau. [When] the midwives arrived, he was kind of ushered into the corner, caught on the periphery of what was happening. (Whānau Tahi, māmā, 30 years old)
Emergent theme 2—experience of isolation and trauma: We don’t have anyone else around or other whānau down here at the hospital. I was out of the room when our baby was born. I was away dropping our son off because we were not able to have another child in the room with us; in that 20mins away from the hospital, that’s when our baby was born. (Whānau Rua, pāpā, 34 years old)
Childbirth, in normal times, often involves a sense of celebration which is interwoven with pain and sometimes injury. Birthing under COVID-19 restrictions without key support raised a sense of isolation and vulnerability that was mentioned by all whānau interviewed. This lack of support was felt to be a traumatic entry point into parenthood: In te ao Māori [the Māori world], we’re not anything without our whānau, and our whānau are our support system, they hold us up, they are our pink batts against the world, our insulation. (Whānau Tahi, māmā, 30 years old)
The COVID-19 lockdown levels involved restrictions that prevented some practices from being carried out as they normally would. The biggest change for all the whānau was the limited capacity for whānau involvement in pregnancy care and birth, as well as the restructuring of prenatal and postnatal care: We didn’t get any support from Plunket or have any visits at home after our baby’s birth, we just had video calls, which is different from actually looking at and checking the baby. Because I was worried that we hadn’t had much support around our baby’s development. (Whānau Rua, māmā, 41 years old) I thought I’d be [birthing] by myself, which was hard because I wanted my mum and my baby’s father there with me . . . I locked down at Mum and Dad’s place. My baby’s father lives just around the corner, but he couldn’t attend appointments or anything which was really difficult for him to not be there. (Whānau Toru, māmā, 22 years old)
Health is fundamental to enjoying life; any health complications during pregnancy were linked to a lot of self-blame and anxiety. Whānau at this time also had to contend with going to appointments alone without significant support people, as well as a lack of kanohi-ki-te-kanohi (face-to-face) interactions: When I was diagnosed with gestational diabetes, I felt like I had failed in my duty to have a healthy pregnancy. I didn’t know anything about gestational diabetes and had never met with anyone face-to-face about the condition. I went through the third trimester being fearful that I was making a baby that wouldn’t be able to fit through the birth canal. Every time I would eat, my blood glucose levels would spike. I was stressed about eating and what I could eat or what I couldn’t eat and thought if I didn’t manage my GD (gestational diabetes) I was being neglectful of my baby’s health. (Whānau Tahi, māmā, 30 years old) Our baby had hip dysplasia when she was born, and because we were in full lockdown, I had to go to her appointments by myself. I was still breastfeeding, so I had to be the one to take her and couldn’t digest all of the information. (Whānau Rua, māmā, 41 years old) During my [baby’s] gender scan, it showed that [my baby] had something wrong with one of her lungs. So during the lockdowns, I was referred to get ultrasounds to check her growth but being able to do that in lockdown was very hard. [We] weren’t allowing any support people to go with you to get the scans. On top of that, you’ve got in the back of your head what’s going on with my baby and then you can’t get an appointment. So it was very hard with everything going on. (Whānau Toru, māmā, 22 years old)
In contrast to the connection described under normal times, the whānau enjoyed with their communities and extended whānau, this time was one of isolation in both rural and urban settings: During lockdown, you could only get into the hospital when you are in active labour, and the ambulance trip from the hospital is about an hour and half. It was very scary being so far away from a hospital if something was to go wrong. We’ve got a lack of all resources around here, and that got worse over lockdown. We don’t have mental health services, counsellors, anything like this normally but I know that lots of people went through domestic violence and stuff during the lockdown, and not having access to help would have been hard. (Whānau Toru, māmā, 22 years old)
Emergent theme 3—effect of restrictions on birth choices: When we got to the hospital, the front doors weren’t open, and you had to go through A&E. We got to the reception, and I said, I need to go to the maternity unit, I’m having a baby. The receptionist said you need to fill out these forms first for COVID. I lost it. . .having driven 2 hours to the hospital and being fully dilated, they could have bought them in after I had the baby. From the time we got to the hospital, and the time I birthed, it was 10 minutes. (Whānau Toru, māmā, 22 years old)
The rangahau uncovered that small acts can have big impacts. A lack of manaakitanga (kindness, support, care for others) was seen in each birth story. With COVID-19, there was a scaling back of systems and a tightening of rules. This at times led to experiences that were felt to be lacking in care for what the whānau were going through at one of the most significant moments of their lives.
I had enrolled in a breastfeeding course, but it got cancelled so I didn’t get any education about breastfeeding. In hindsight, if I had received the resources and the education that I needed, I probably would have avoided a lot of the postnatal depression that I experienced. (Whānau Tahi, māmā, 30 years old)
The individualised care model can often be at odds with te ao Māori. In usual times, this lack of cultural awareness or cultural safety can be deeply painful, but when lockdown and birth collided, there was a feeling of trauma that came through in the interviewee’s accounts: If we want to be Māori, we have to lead the process by talking through the “why” behind everything. It’s not actually me that they’re dealing with in isolation, it is my tipuna [ancestors], my whakapapa [genealogy or lineage], my whānau, my community but they only saw me. The individualised care model complicated my pregnancy because none of my whānau were able to come to any appointments. That might be a symptom of COVID-19 and lockdown, but I would also argue that Māori worldviews have never been given much attention in the broader healthcare system. (Whānau Tahi, māmā, 30 years old)
Most of the whānau had birth preferences that were altered due to the pandemic. The whānau who were interviewed as part of the study found themselves choosing between deeply held beliefs and medical advice. For many of the whānau, it was a highly unfair situation to make decisions while striving to achieve optimal health outcomes: I was home birthing out of necessity because if I didn’t home birth, my whānau weren’t able to be there, and that was not something that I was keen to entertain at all. It meant more to me than having any type of pain relief, being Māori was way more important to me than anything. (Whānau Tahi, māmā, 30 years old)
Discussion
This rangahau is the first to explore whānau lived experience of birthing and parenting during a crisis within the context of Aotearoa. Our rangahau provides an exploratory narrative analysis of whānau Māori lived experience during these challenging times. From a Māori perspective, maternity is inseparable from the broader politics of whānau, equity, identity, tikanga, and spirituality. Hapūtanga and whakawhānau connect past, present, and future generations and is a time of paramount importance (Mikaere, 2017; Simmonds, 2016). Transitioning through this sacred time during a global pandemic is uncharted territory; we need to explore the impact of COVID-19 restrictions on Māori maternal and whānau mental and physical health, and health outcomes. The whanau Māori who participated highlighted this in their lived experiences of health care during these restrictions.
It is essential to acknowledge the historical and contemporary experiences of health care for Māori in Aotearoa. Rangahau has indicated that wāhine Māori already often feel excluded and marginalised from Western spaces during pregnancy (August, 2005). The impact of COVID-19 lockdowns on maternal mental health is a side effect of preventing infectious disease transmission. Among other detrimental outcomes, increased maternal stress and anxiety are associated with an increased risk of preterm delivery, reduced mother–infant bonding, and decreased odds of breastfeeding (Davenport et al., 2020; Dib et al., 2020). During the pandemic, the increase in distress experienced by pregnant and postpartum wāhine included experiencing feelings of being robbed of the joys of motherhood and this was seen with the rangahau participants in keeping with our findings (Dib et al., 2020). The actual impact of increased isolation and stress will take years to assess. When perinatal stresses intersect with the wounds of ongoing colonisation, an intensification of negative outcomes for Māori and other colonised peoples is likely.
To coherently support a change in health outcomes, an understanding of Māori culture needs to include meaningful investigation into how Māori view the world and conceptualise their place within it (Mikaere, 2017). Humanity is believed to share whakapapa connections to the natural environment but as the junior sibling. Whānau-centred tikanga-informed practice lessened the trauma that whānau have often encountered in the hospital or clinical environment, promoting a relationship of trust. Having whānau support during birth was crucial, to the extent that whānau described weighing up medical advice against the ability to birth with whānau support—sometimes ignoring best practice in favour of birthing with whānau present. Tāne and birth partners provide an essential part of the process of whakawhānau. This is not often considered when we are thinking about whakawhānau and hapūtanga; however, it does remind us of the positive impact of bonding and support for the birthing person and whānau if the vital role of the tāne or birthing partner is recognised. This is identified in our rangahau findings.
The qualitative nature of the narratives within this rangahau provides a depth to the kōrero (discussion) which explored the narratives of those who took part. Consistent themes were heard across all whānau coming from different localities giving a broad range of experiences across geographically diverse populations. Participants were self-selected and potential selection bias may limit the generalisability of the rangahau. However, the whānau who agreed to participate in the rangahau were well engaged despite the experiences they described during COVID-19 restrictions. Recruiting during a pandemic brought its own challenges and convenient sampling enabled recruitment. While the sample size may be thought to restrict the generalisability of the findings, the depth of the kōrero and consistency of the emergent themes is a strength of the rangahau.
Given health resources in many areas are already stretched, COVID-19 regulations risk the hard-fought gains that have been made towards supporting indigeneity, especially in the birthing space, being seen as a luxury. After generations of a paternalistic medical system resulting in significant harm to the Indigenous peoples of Aotearoa, there is legitimate concern that the power shift during COVID-19 with forced regulations and regulatory approaches may have compounding impacts on maternal health care for Māori. Breakdowns in understanding and communication can be catastrophic for feeling safe and heard, and engendering trust in a therapeutic relationship. When a clinician approaches whakawhānau without acknowledging or understanding what is essential to the patient, communication suffers. Clinically essential details may not be heard, or hold the significance intended by the clinician. This breakdown of understanding and feeling unseen can lead to decisions taken against clinical advice, as trust and understanding have been broken. Several of the whānau in this rangahau reflected that being Māori meant more than medical advice.
Being Māori is a constant, a source of immense pride and an identity to be protected at all costs. During the process of whakawhānau, maintaining a Māori identity is of utmost importance. Empowering their pēpī and providing the best start to life by bringing them into the world connected them to their tipuna and tikanga. Being Māori is not an identity that goes up and down like alert levels. It does not change, as medical advice sometimes can. It is a journey of rediscovery to be maintained and protected, especially during whakawhānau, a time where identity is imperative. During the pandemic, the whānau interviewed wanted to birth and act in a way that prioritised their Māoritanga (Māori culture, practices, and beliefs; Māori way of life) alongside their pregnancy and birth process.
Conclusion
Whānau Māori health outcomes in many areas, including maternity, are unequal, complex, and multifactorial. Inequities occur across the continuum of care and are associated with wider determinants of health, and health disparities are a manifestation of how the current maternal-infant health care system is failing whānau Māori. Our rangahau findings are in keeping with existing findings about whānau experiences of the public health system. Our study has a focus on whakawhānau contributing to the evidence in perinatal health. We hope that the findings from this rangahau can be used to help address some of the shameful health inequities and lead to broader discussions to transform maternity health care. In the words of one whānau, The process of whakawhānau and hapūtanga was fraught with so many challenges during this time of separation or isolation. This could be the new normal, but we have a choice about how we will respond to these challenges, to re-imagine what it would be like to birth with empowerment with the people at the centre of this movement being wāhine and their whānau. (Whānau Tahi, māmā, 30 years old).
Footnotes
Acknowledgements
The authors acknowledge the wāhine and whānau who generously shared their birthing stories with them. Their stories have woven a tapestry of knowledge that will ignite hopeful change in the world of the authors’ tamariki mokopuna.
Authors’ note
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors received no financial support for the research, authorship, and publication of this article.
Glossary
Aotearoa New Zealand
hapūtanga pregnancy
kanohi-ki-te-kanohi face-to-face
kaupapa Māori Māori centric
kōrero discussion
manaakitanga kindness, support, care for others
Māori Indigenous peoples of New Zealand
Māoritanga Māori culture, practices, and beliefs; Māori way of life
māmā other
mātauranga knowledge
mātauranga Māori Māori knowledge
Pākehā New Zealanders of primarily European ancestry
pāpā father
pēpī infants
rangahau research
tāne male
te ao Māori the Māori world
Te-Ika-a-Māui North Island of New Zealand
Te Waipounamu South Island of New Zealand
tikanga cultural protocols, customs, and practices
tipuna ancestors
wāhine women
wāhine Māori Māori women
whānau immediate and extended family
whānau tautoko family support
whakapapa genealogy or lineage
whakawhānau birthing process