
Abstract
Jordan’s Principle is a legal requirement for the Canadian government to address gaps in services for First Nations children and ensure timely services that meet their needs and best interests. This article synthesizes and discusses some of the key research findings described in a report on the implementation of Jordan’s Principle in Manitoba, produced by a team of academic researchers in partnership with the Assembly of Manitoba Chiefs. Findings provide insights into a relational approach to the implementation of Jordan’s Principle and inter-related structural factors that constrain the efficacy of this approach. Findings reinforce the need for First Nations–led processes and Jordan’s Principle policies that fully fund and support First Nations in addressing high caseloads and growing waiting lists, complex responsibilities, stress and staff turnover, administrative burden, and inadequate physical and digital infrastructure. Sufficient resources for First Nations capacity enhancement initiatives and regional coordination and support are also identified priorities.
In Canada, a central strategy of colonialism was to break the bond between First Nations children and their parents (St. Denis, 2022). This strategic form of colonial violence was rationalized and presented by the federal government as benevolent action that was in the best interest of First Nations children. Starting with the residential school system in the 1800s, this colonial violence continues today within child welfare systems that continue to be largely bound by provincial or territorial laws and policies (Truth and Reconciliation Commission of Canada, 2015). The heightened risk and increased service needs created by governmental policies have been compounded by persistent failures to reform federal and provincial policies to eliminate discrimination and provide adequate funding for health, education, and social services for First Nations children living on reserve (Gaspard, 2022).
Given the impacts of colonial violence on First Nations families’ lives, many First Nations parents or caregivers are understandably vigilant about who they trust and what information they share when it comes to their children. The level of mistrust and caution that many First Nations parents experience in deciding whether to use and engage with seemingly beneficial services may be viewed as a prudent and warranted means of exerting their agency over what is best for their families. Providing child-related services in a context of mistrust and potential risk with First Nations families requires that service providers rethink and transform practice as usual (Gerlach et al., 2017, 2020).
In this article, we examine how structural factors are constraining the potential of Jordan’s Principle to transform practices with First Nations children and families in Manitoba. In the introduction, we provide overviews of Jordan’s Principle, First Nations children and families in the Manitoba region, and relational approaches to care. This is followed by a description of the research methods and findings. The findings provide important insights into how a relational approach to the implementation of Jordan’s Principle in the Manitoba region is severely constrained by inter-related structural factors. In the discussion section, we explore how these structural factors are pressuring relational worldviews on family-child well-being and tacitly recentering dominant colonial narratives and practices. While focused on the Manitoba region, this article provides policy insights and recommendations that are relevant to other jurisdictions in Canada and similar settler-colonial nation states.
The context of Jordan’s Principle in Canada
Jordan’s Principle is a legal requirement for the government of Canada to address gaps in services for First Nations children and ensure timely services that meet the best interests and needs of First Nations children in keeping with the principle of substantive equality (First Nations Child & Family Caring Society of Canada, 2023). Jordan’s Principle was initially conceived as a child-first principle designed to ensure that First Nations children did not experience denials, delays, or disruptions because of the complicated framework for services with First Nations (First Nations Child & Family Caring Society of Canada, 2005). It is named in honor of Jordan River Anderson, from Norway House Cree Nation in Manitoba. Jordan was born with a rare genetic disorder requiring specialized care from birth. He was denied the services and supports he required to live at home due to federal and provincial governments and departments fighting over who would bear the cost. Jordan never made it home and passed away in hospital in 2005, at the age of 5 (First Nations Child & Family Caring Society of Canada, 2005). The disputes that occurred with Jordan resulted from unclear delineation of federal and provincial government responsibilities to First Nations peoples.
Despite advocacy from First Nations and First Nations organizations, strong support from allied organizations, a unanimous House of Commons resolution supporting Jordan’s Principle, and federal claims to have implemented Jordan’s Principle, Jordan’s Principle was not meaningfully implemented. Between 2010 and 2015, as a result of the federal government significantly narrowing Jordan’s Principle eligibility and mandating complicated case conferencing and approval processes, the federal government indicated that it knew of no Jordan’s Principle cases in Canada (Sinha et al., 2021). The scope and implementation of Jordan’s Principle started to change in 2016, when a series of Canadian Human Rights Tribunal (CHRT) rulings in First Nations Child and Family Caring Society & Assembly of First Nations v. Canada mandated the full implementation of Jordan’s Principle and interpreted Jordan’s Principle broadly. Today, Jordan’s Principle applies to a wide range of health, education, and social needs for all First Nations children below 19 years of age, living on- or off-reserve, including children engaged with, or in the care of provincial or territorial or First Nations child welfare systems (Indigenous Services Canada (ISC), 2023).
Under the CHRT’s interpretation of Jordan’s Principle, the federal government must fund services and supports in keeping with the principle of substantive equality. Linking Jordan’s Principle to substantive equality requires that services extend beyond provincial standards if required to meet First Nations children’s needs and that “both the concrete conditions of inequality be remedied and the structural sources that reproduce it be transformed” (Sinha et al., 2021, p. 25). In response to CHRT rulings, the federal government radically expanded the funding available for services for First Nations children. However, in its current form, Jordan’s Principle has simply been layered on top of the pre-existing system of funding and services. Accordingly, there continue to be well-documented, unmet gaps in funding across a range of services for First Nations children which must be addressed alongside the provision of Jordan’s Principle funding to meet the needs of First Nations children (Gaspard, 2022).
First nations children and families in the Manitoba region
In the Manitoba region, First Nations people account for 15% of the provincial population (Government of Canada, 2021). There are 63 First Nations, representing five different language groups and signatories to seven Treaty territories, across 650,000 square kilometers. First Nations children living in this region may have rights under, and be served by, the provincial government, the federal government, and First Nations.
First Nations have always had their own laws around, and systems of caring for children and supporting families, and these have persisted despite assimilationist and genocidal policies, including the residential school system and the ongoing, mass separation of families and children by child welfare systems in Canada (Truth and Reconciliation Commission of Canada, 2015). Across Canada, the intergenerational impacts of First Nations, Métis (an Indigenous people of mixed Indigenous and European ancestry, particularly those with historic connections to the Red River area of what is now Manitoba, Canada), and Inuit (an Indigenous People of northern Canada, Greenland, and Alaska, USA) peoples’ experiences of mass family separation include increased risk of suicidal ideation and suicide attempts, heightened mental health distress, greater child and family services (CFS) involvement, and higher chances of growing up with food insecurity in crowded, low-income households (Gone et al., 2019; McQuaid et al., 2022; Moon-Riley et al., 2019). As a result, First Nations children consistently experience higher levels of risk and poorer outcomes across a broad range of health and well-being measures compared to other children in Canada (Beedie et al., 2019; Chartier et al., 2020).
Relational approaches with First Nations children
Prevailing biomedical and developmental worldviews and approaches tend to view children against White, Euro-Western ideals of normal development that are incompatible with First Nations’ worldviews (Ineese-Nash et al., 2018). Moreover, this viewpoint overlooks how First Nations families and children’s lives are profoundly influenced by colonial violence and systemic racism within benevolent systems, including early child development, health care, and child welfare (Allan & Smylie, 2015; Gerlach et al., 2017; Loppie & Wien, 2022).
Transformative approaches to addressing First Nations children’s health highlight the centrality of relational and collectivist approaches to care (First Nations Health Authority, 2019). Relational worldviews are central to many Indigenous knowledge systems (Battiste, 2000; Little Bear, 2000). As described by Greenwood (2005), The foundations of Indigeneity, then, are comprised, in part, of values that privilege interrelationships among the spiritual, the natural, and the self; reflect a sacred orientation to place and space; encompass a fluidity of knowledge exchanged between past, present, and future, thereby allowing for constant and dynamic knowledge growth and change; and honour language and orality as an important means of knowledge transmission. (p. 554)
Wellness, from an Indigenous perspective, is often understood as a holistic balance and interdependency between physical, emotional, mental, and spiritual dimensions that are deeply connected to and supported by kinship relationships linking “family, community, and all extended human and more -than-human relations” (Campbell et al., 2020, p. 9). Relationships to family, community, Nation, the spirit world, and the land are vital sources of health and wellness (First Nations Health Authority, 2019), as is the intergenerational transmission of ways of life that are embodied in languages, songs, ceremonies, and protocols (Tsuji et al., 2023). Thus, relationality provides a critical shift away from pathologizing narratives and deficit-focused care, to holistic, strengths-based, context-specific, and relationship-focused care (Gerlach et al., 2018), that are critical for engaging First Nations, families, and children in Jordan’s Principle funded services (Gerlach et al., 2020; Sangster et al., 2019).
Methods
The findings discussed in this article are based on a large, mixed-methods study that has previously been summarized in an extensive report (Sinha et al., 2022). This larger study examined the impact of Jordan’s Principle on the structure of services for First Nation children in Manitoba. This research was commissioned by the Public Interest Law Centre (https://www.legalaid.mb.ca/pilc/public-interest-law-centre/) and was guided by an Advisory Committee with broad representation from First Nations across Manitoba. Research activities were co-designed and implemented by policy experts from the Jordan’s Principle Implementation Team at the Assembly of Manitoba Chiefs (AMC), and a team of researchers in the fields of social policy, social work, child and youth care, and community health who have built relationships and trust over years of collaborative work on Jordan’s Principle and health-related services with First Nations families and children (Gerlach et al., 2017; Jordan’s Principle Working Group, 2015; Sangster et al., 2019; Vives et al., 2017).
Relationship building with all stakeholders was a primary focus throughout the research process to codesign research methods and respond to the shifting contexts of Jordan’s Principle and the ongoing COVID pandemic. In 2020, research ethics was approved by the researchers’ university ethics boards. The research team, including members of the AMC, co-developed a Research Collaboration Agreement outlining responsibilities of the research team to uphold the principles of ownership, control, access, and possession which included AMC’s right to data sovereignty.
Data collection
The data informing the findings discussed in this article were generated by mixed methods, as summarized in Table 1, and collected from the summer of 2020 to the summer of 2022. Research proceeded during the COVID-19 pandemic with all interviews, focus groups, and meetings taking place virtually.
Summary of data collection methods.
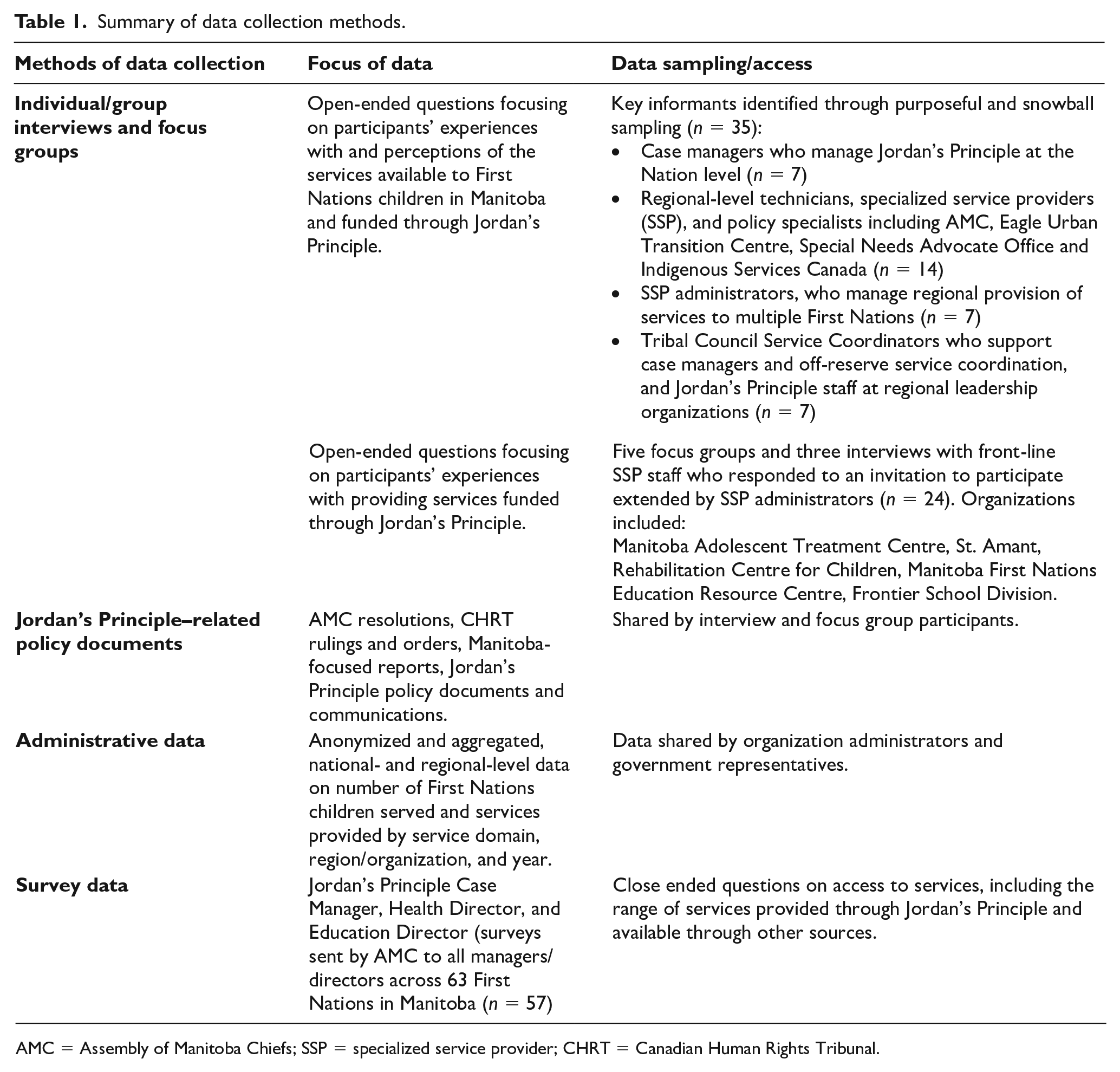
AMC = Assembly of Manitoba Chiefs; SSP = specialized service provider; CHRT = Canadian Human Rights Tribunal.
Due to concerns about identifying participants within the relatively small Jordan’s Principle sector in Manitoba, and no intention of doing a gender-based analysis, sociodemographic information about participants was not collected beyond their role.
Data analysis
All interviews and focus groups were recorded, transcribed, and anonymized. All participants received their own transcripts and were consulted prior to any direct quotes being used. Interpretation of transcripts and meeting notes was guided by a reflexive thematic analysis approach (Braun & Clarke, 2023). The research team read the transcripts and notes to identify recurring themes, compiled the segments of each transcript and set of meeting notes that related to each theme, and created memos summarizing key patterns in the data for each theme. Data from other sources were then integrated to add further detail to the memos. These memos formed the core of the analysis. Collaboration with research participants, Jordan’s Principle service coordinators, and organizations providing Jordan’s Principle funded services generated insights to further inform the findings and ensure that they were located within appropriate historical and policy contexts.
Knowledge mobilization
A final research report (Sinha et al., 2022) was submitted to the CHRT as independent expert evidence and supported determination of a settlement in a Jordan’s Principle–related case. The report and infographics (https://csprg.research.mcgill.ca/jpmanitoba) were co-developed with the Advisory Committee and disseminated to every First Nation in Manitoba. Also, an online symposium was hosted by the AMC to discuss the findings with First Nations in the Manitoba region.
Findings
Relational approaches in implementing Jordan’s Principle in Manitoba
The data suggest that fulfilling the potential of Jordan’s Principle funded services to improve the health and life opportunities of First Nations children requires a de-centering of dominant biomedical worldviews and approaches and a recentering of relational approaches to care. Fostering and regaining trust was described by one participant as “deep healing work” that was foundational to increasing: First Nation communities, families, and children’s access to and engagement in health, education and social services and supports, especially with families that have experienced trauma associated with histories of difficulty accessing services, inappropriate or damaging services, and inter-generational policies of cultural genocide such as residential schools and contemporary CFS. (Case Manager)
In a context of mistrust and fears of engagement with provincial CFS, the data illuminated how Jordan’s Principle funded service providers prioritized time being present in community. This facilitated building relationships within Nations, including with families, Elders and Knowledge Keepers and other service providers, and leaders across health, education, and social service sectors. Working across these sectors provided new opportunities for breaking down silos and fostering greater collaboration. Time invested in rebuilding trusting relationships also facilitated greater intersectoral collaboration, information sharing, and understanding of the often socially complex circumstances of families’ lives and priorities: If you are spending many hours a day figuring out how to get water to your house, if there’s big holes in your floor and in your walls. . .. and there are the social determinants of health and very basic housing problems in the communities that I go to are a massive, massive problem. (SSP)
To respond to social determinants, service providers frequently expanded their scope of practice and took on complex responsibilities as they sought out additional supports and services that extended beyond traditional disciplinary boundaries. Shifting and tailoring practices in response to the self-identified priorities and contexts of individual families and children and their respective Nations were treated as a necessary foundation for improving the accessibility and uptake of Jordan’s Principle services. However, there were also strong findings on how this relational, socially responsive, and intersectoral approach to implementing Jordan’s Principle was being eroded by multifaceted structural factors, which are summarized in Figure 1 and represent the primary focus of the findings in this article.
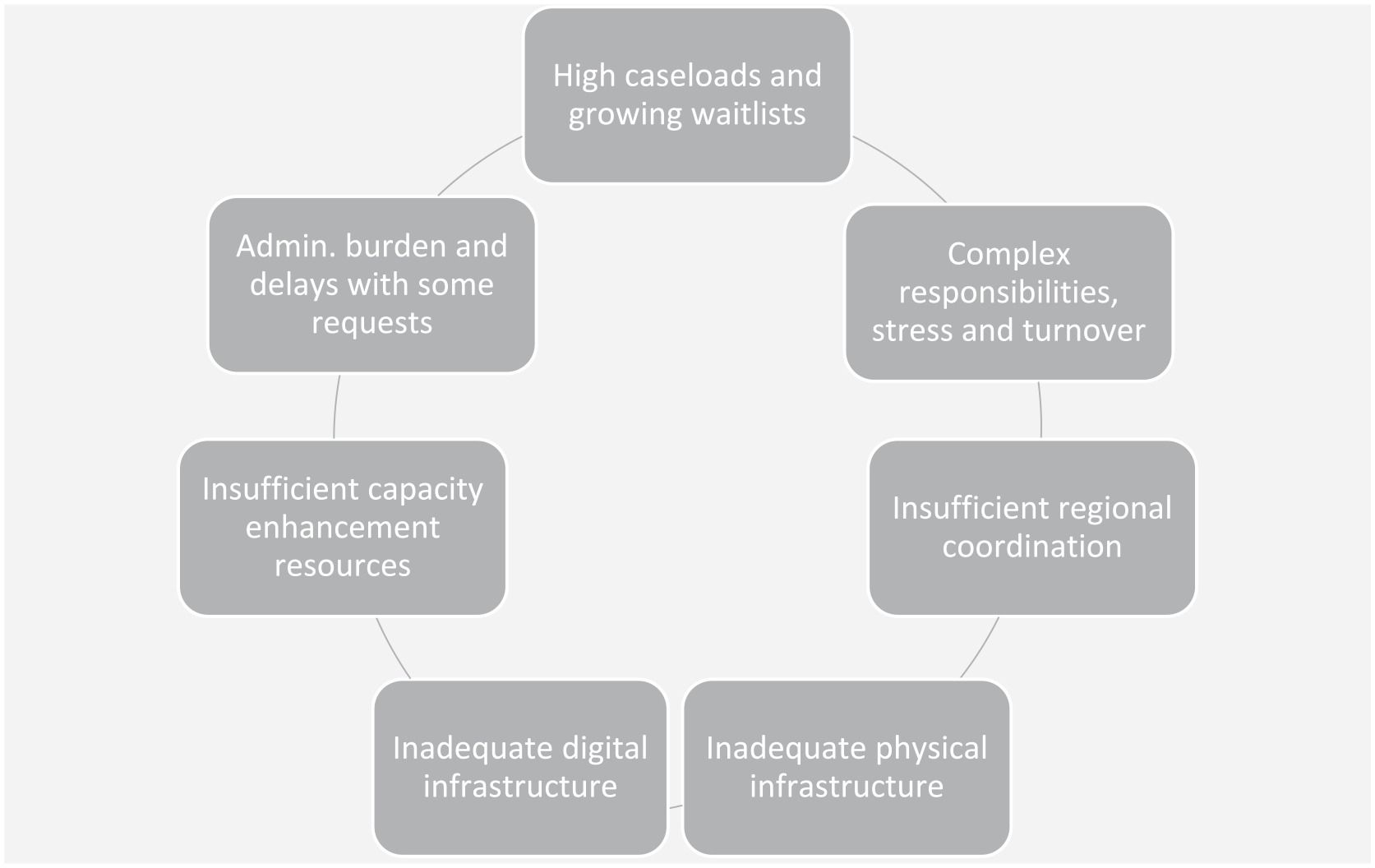
Inter-related structural factors that constrain the implementation of Jordan’s Principle in the Manitoba region.
High caseloads and growing waitlists
Growing caseloads and waitlists for Jordan’s Principle services in Manitoba simultaneously reflect and undermine a relational approach to practice. Analysis of case load and waitlist data for four of the specialized service providers (SSPs) that offer services in many First Nations in Manitoba shows that from 2017–2018 to 2019–2020 caseloads grew dramatically, from 150% for one SSP to 425% for another. In 2019–2020, two of these SSPs reported waitlists that were approximately 50% of their total caseload. Other SSPs reported serious concerns about waitlists. The growth in caseloads and waitlists is evidence of the success of relational approaches that enabled Jordan’s Principle service providers to engage and build relationships with families who may have been initially disconnected from and or been wary of services.
However, SSPs described how the pressures of growing caseloads and waiting lists severely compromised their capacity to spend time (re)building and maintaining relationships with local Knowledge Keepers and Elders, thereby ensuring that their services respected local practices and protocols and avoided inadvertently perpetuating harm: There are only two [SSPs] and we currently have 1,000 referrals. So, it’s not enough time. . . because the travel; it’s remote access and the time it takes to get there and establish yourself, and the unpredictability of school might not be open because there’s no teacher, or there’s no water. . . So there does seem to be a big-time crunch when we are there—it’s go, go, go, go . . . I find it high pressure and not enough time to do the things that we want to do. (SSP)
SSPs also reported that time pressures were limiting their ability to collaborate with other service providers and Nation leadership to ensure coordination and continuity of care and “forced them to focus on crisis work.”
The growing pressures on services also made it challenging to meet the CHRT mandated timeline set to respond to families. Jordan’s Principle managers were able to mitigate some service delays by creating locally based services or seeking alternate referrals. However, some children went without services while on waitlists or received watered-down services. In some cases, children waited for over a year before receiving specialized services. Such delays in service compromise the fundamental purpose of Jordan’s Principle—to ensure First Nations children have timely access to needed services.
Complex responsibilities, stress, and staff turnover
The under-resourcing of Jordan’s Principle in the Manitoba region by ISC meant that Jordan’s Principle case managers, service coordinators, and service providers took on broad, wide-ranging responsibilities in addition to managing the pressures of providing relational approaches in Nations with growing caseloads and waitlists. For example, participants suggested the job description of a case manager can include working across disciplinary boundaries and multiple levels of relationships to develop and manage services while also carrying out day-to-day responsibilities of supporting families. Their responsibilities can include developing and administering services across the health, education, and social service domains; building and maintaining relationships with Nation leadership, other service providers, and Jordan’s Principle workers and administrators; and recruiting, hiring, and managing respite workers, child development workers, educational assistants, and other staff working directly with children and families whose needs can require extensive knowledge of highly specialized supports and services. As one participant shared, “I basically just oversee everything and I’m on call all the time. So, I take any client messages and phone calls during the day and after hours” (Case Manager). Participants expressed concerns that the unsustainable stressors placed on Jordan’s Principle-funded case managers and service providers, and subsequent high staff turnover, disrupted established relationships, reduced the ability to address family- and child-specific needs, and restricted or eliminated continuity of care.
Administrative burden for some Jordan’s Principle requests
Participants also described how the administrative burden of making Jordan’s Principle requests took time and energy away from their relational work. The approach to Jordan’s Principle in Manitoba features the transfer of substantial power for decision-making around individual requests for Jordan’s Principle-funded services to First Nation Service Coordinators. Participants did not note concerns about the timeline for decisions made by Service Coordinators. However, requests for higher cost services and supports that cannot be provided within a Nation, as well as a shifting list of other services, must be assessed by the federal government. Over time, the requests that must be reviewed by the federal government have included, but have not been limited to, dental care, medical equipment, educational supports, and housing.
Administrative requirements associated with requests assessed by the federal government were described as time-consuming and burdensome, requiring the submission of substantial supporting documentation. For example, participants indicated, and policy documents confirmed that, a typical request could include an intake form, a service request, an assessment from a health care professional, a letter of recommendation from a different health care professional, a letter justifying the need for the service based on substantive equality, and a detailed quote or cost estimate. Depending on the service being requested, additional requirements can include documentation of denial of services by Non-Insured Health Benefits, a letter from the school, Education Director, and or Chief and Council attesting that they cannot fund the requested service, letters of support from Chief and Council or the Health Director, or additional assessments (ISC, 2023).
Inadequate physical infrastructure in communities
A further recurring theme was that the lack of safe, welcoming, and family-friendly physical spaces that were conducive to nurturing relationships between families accessing Jordan’s Principle services and Jordan’s Principle service providers: One of the things that we’ve been asking for, for a long time, is our own space, our own building . . . having our own place where people can go to and they’re not pushed out of it, they’re not rushed through it. They’re not turned away from it. But they can come there with their kids, they can be there if they need to be . . . There’s a room for kids to play in, there’s a kitchen for us to teach cooking or provide food for families. There’s assessment space . . . Families do not want child development workers and therapists coming to their house. There’s so much shame about it. There’s judgment that they feel. There’s—they just don’t want it. They want to be able to go somewhere and have the appointment, learn what they need to learn, and then take it back to their house. I really think that it could be a community hub for many different places. (Case Manager)
The majority of case managers (83%) who responded to an AMC survey indicated that the space for their Jordan’s Principle programming was “insufficient.”
Shortly after qualitative data collection for this study ceased at the end of 2021, the CHRT ruled that the federal government does have an obligation to cover capital costs associated with Jordan’s Principle. In response, the federal government developed and made public broad guidelines, for federal officials as well as First Nations and service providers, on capital expenditures for health, education, and social services. However, there is no systematic funding for planning or coordination to eliminate, for example, situations in which Nations feel they have to choose between Jordan’s Principle space and a new health facility, or to help Nations address technical considerations around designing multi-service spaces that support maintenance of confidentiality and collaboration between colleagues and group activities (Government of Canada, 2022). Without sufficient, properly designed infrastructure, opportunities to foster coordination and collaboration are lost.
Inadequate digital infrastructure in homes and communities
Another recurring theme was the benefits of connecting with and providing services to families virtually. A participant highlighted the potential for virtual services to allow for more continuity in care and relationships—when there is good internet: If all the communities could have really good Internet, that would be great. Internet access is huge, obviously over the past year, [and] has been a huge challenge in providing better virtual services. That being said, the one thing that we’ve learned is that for the few kids that we have been able to connect with virtually, is that this is an option to fill in between visits as well. Being able to provide those virtual kinds of appointments in between our four to six, sometimes eight-week visits. So, communities need and deserve internet access. (SSP)
The findings highlight that many Nations in Manitoba lack cell phone and or affordable, stable, high-speed internet access and the telehealth connectivity necessary to facilitate flexible and ongoing engagement between service providers and families. The lack of digital infrastructure across First Nations in the Manitoba region was emphasized during the COVID-19 pandemic. Nonetheless, participants recognized its long-term potential in addition to in-person services.
One of the things that we have learned or had to learn with COVID, is that there is room for technology in the services that we provide and ways that we can incorporate it that can be helpful. You know, a lot of the families that we provide services to . . . don’t have access to phone or access to internet, or at least reliable versions of that. And so, you know, when it comes to doing in person services again, number one, we’re going to be able to consistently see those families and those clients again. But also understanding that virtual services can sometimes be faster and more efficient . . . .And now hopefully by the end of the pandemic, communities will be a little bit more open to it and receptive to trying to do those things. (SSP)
In 2021, the federal government announced funding for high-speed internet in 11 First Nations in Manitoba (CBC News, 2021). The provincial government also announced plans to extend high-speed internet to 30 First Nations, but First Nations were not consulted or engaged in the process of deciding on a service provider in this project, and the AMC has objected to the lack of transparency and inclusion in the decision-making process.
Insufficient resources for capacity enhancement initiatives
Jordan’s Principle in Manitoba was rolled out rapidly, with little time for planning or preparation. Many First Nations and service organizations found themselves simultaneously recruiting and training staff while implementing services with families and children. An SSP pointed to the need for Jordan’s Principle to resource ongoing educational supports and systems for building and sharing knowledge, and noted that these had been decreasing over time: When Jordan’s Principle was first rolling out, there was a lot of initial training offered for Case Managers and child development workers, and coming together with the SSPs and helping them understand what each of the different programs could offer and how they could work with their community. . . . [Now,] I don’t know that the new Case Managers get that information clearly. (SSP)
Participants also indicated that the uncertainty, complexity, and short-term nature of capacity enhancement funding made it difficult to establish or sustain capacity enhancement initiatives for all First Nations. Some established initiatives were based on funding that was limited to a subset of Nations. Others that did extend across Nations, lapsed because of cuts in funding, staff turnover, and constraints on resources as caseloads and waitlists had increased.
One participant pointed to the Manitoba First Nations Education Resource Centre (MFNERC), which in its fifth year of funding through an ISC training grant, reported cohorts of 12 graduating psychologists, 25 First Nations literacy specialists, six speech therapists, five occupational therapists, one physiotherapist, 110 First Nations resource teachers, and 120 people participating in training to become therapy assistants. This organization has hired over 50 full-time, First Nations staff over 5 years. A participant who was a graduate of one of the MFNERC training initiatives spoke to the long-term outcome of this type of capacity enhancement: “[We have been] moving away from a Western medical model and moving to a First Nation world view of inclusion. So, we’ve undergone a big paradigm shift . . . to a more rights-based approach, reflecting First Nations worldviews” (SSP).
Insufficient regional coordination and support
There was evidence that progress toward a system of Jordan’s Principle services that is grounded in First Nations’ worldviews has been undermined by the federal government’s failure to fund and support a First Nations–led regional coordination structure. Consistent with a relational approach, the sharing of case-level information was highlighted by participants as being key to facilitating effective collaboration between different service providers involved with a family, reducing the burden on families to repeatedly share the same information with multiple providers, and preventing the provision of services based on conflicting or misaligned intervention strategies. Regional infrastructure to support the development of shared policies, standards, promising relational practices, and necessary technical resources was also identified as essential to the ongoing development of Jordan’s Principle in Manitoba. In the absence of a regional structure that facilitates information sharing and capacity development, participants worried that Nations with greater experience in providing and developing services may benefit from a full range of Jordan’s Principle opportunities, while Nations with lesser experience fall behind, compounding inequities between Nations.
To help ensure equitable services for First Nations children throughout the Manitoba region, participants expressed a strong desire for increased data collection and data sharing tools that could support Nations in achieving a common baseline of services, and other supports for enhanced collaboration. Participants also suggested that data sharing protocols and shared databases may help to eliminate delays and disruptions in services that can occur when service providers lack strong, informal systems of collaboration and coordination. At the same time, they also highlighted complex and serious issues that must be addressed to develop data sharing systems and protocols. These include obligations around protecting confidentiality, the need to ensure security of data once in a database, in addition to shared and accepted processes for making decisions around shared or regional resources. Consideration of these issues should be supported by a formal—recognized by First Nations leadership and consistently funded—regional body that has the support of First Nations leadership, consistent funding, and sufficient technical capacity needed to navigate these complexities.
Discussion
The findings of our research in Manitoba add to evidence demonstrating the importance of service providers doing the essential deep healing work of nurturing trusting relationships and, in turn, learning from and about each Nation and each family’s story (Gerlach et al., 2018, 2020). By adopting a relational approach, Jordan’s Principle service providers are challenging normative and prescriptive ways of being, knowing, and doing as they tailor their services for and with each Nation, family, and child. The effectiveness of this approach can be seen in the growing number of First Nations children and families seeking Jordan’s Principle funded services in Manitoba (Sinha et al., 2022).
However, the findings clearly show how inter-related structural factors are undermining the efforts of Jordan’s Principle case managers, service coordinators, and service providers in the Manitoba region to implement responsive and relational approaches and provide continuity in relationships and care. Moreover, the findings on increasing caseloads and waitlists, heavy administrative duties, and multifaceted responsibilities raise concerns that the current structure of Jordan’s Principle is tacitly pushing toward reactive and crisis-oriented work that prioritizes efficiency. This push reinforces colonial practices and narratives that have served to disempower and disadvantage First Nations peoples in the past and in the present day.
Any cost analysis aimed at advancing Jordan’s Principle therefore needs to consider the amount of time required to work in an effective, relational way. This will require both top-down government-driven and bottom-up Nation-driven approaches to co-creating a Jordan’s Principle budget model that includes the experiences of front-line service providers to estimate the true costs of building and sustaining relational approaches to service provision. Moreover, this budgeting process needs to explicitly recognize and consider the differences in regional models of Jordan’s Principle and support a flexible approach to funding centralized services that supports self-determination in service design and delivery. Development of new cost, or budget models for Jordan’s Principle, must be undertaken in parallel with efforts to redress known gaps in other budgetary areas such education, CFS, water, housing, sanitation, and other domains (Gaspard, 2022). Any attempt to redress gaps across such diverse budgetary domains through Jordan’s Principle can only increase the complexity of the job descriptions and administrative requirements.
A new structure for Jordan’s Principle must also include stable funding for long-term capacity enhancement initiatives. By failing to adequately fund capacity enhancement efforts, the current system upholds dependency on largely non-Indigenous SSPs and tacitly (re)centers individualistic, developmental, and biomedical child health approaches. Individualized practice approaches, albeit emanating from seemingly benevolent systems of care, are inherently cultural, political, and potentially harmful, perpetuating the assimilation of First Nations families and children (Ineese-Nash et al., 2018). Funding for Jordan’s Principle in the Manitoba region must support capacity enhancement initiatives to establish a core group of First Nations service specialists equipped with the credentials to lead a First Nations system of specialized services that can center relational worldviews and approaches in Jordan’s Principle services. Such transformation requires long-term, intensive investment in education and mentoring, with diverse training programs across levels of education, staff positions, and service domains. Consistent with First Nations rights to self-determination, the design and development of capacity enhancement initiatives to support the implementation of Jordan’s Principle need to be undertaken by First Nations, with the support, rather the oversight, of ISC (Sangster et al., 2019).
Regional coordination, and sufficient, flexible federal funding is also required to address noted deficits in physical and digital infrastructure. Many Nations lack the physical infrastructure to house Jordan’s Principle services and provide a comprehensive hub of Nation-designed and delivered care for families whose children have dis/abilities, complex and or chronic conditions. There is also a need for digital infrastructure to foster continuity in relationships and coordination and continuity of care, particularly in remote and northern Nations where year-round physical access can be challenging (Hanlon-Dearman et al., 2014). Addressing these infrastructure challenges will require coordinated efforts that allow for the collective creation of knowledge about the needs within Nations and sharing of the technical expertise required to address these needs.
Conclusion
Jordan’s Principle offers an opportunity to re-vision and re-create First Nations controlled services that are locally based, culturally grounded, and focused on wellness and prevention, rather than being dis/ability or problem-focused. Collectively, the multifaceted structural inequities described in this article systematically challenge the potential of Jordan’s Principle service providers to undertake the relational work that is required to effectively engage with and support First Nations children’s optimal health, well-being, and human rights. Accordingly, the current structure of Jordan’s Principle threatens a return to dominant, reactive, and crisis-driven approaches. This research reinforces the need for Jordan’s Principle policies that fully fund and support First Nations in addressing high caseloads and growing waiting lists; complex responsibilities, stress, and staff turnover; administrative burden; inadequate physical and digital infrastructure; insufficient resources for capacity enhancement; and insufficient regional coordination and support.
Footnotes
Authors’ note
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors received no financial support for the research, authorship, and publication of this article.
Glossary
Inuit an Indigenous People of northern Canada, Greenland, and Alaska, USA
Métis an Indigenous people of mixed Indigenous and European ancestry, particularly those with historic connections to the Red River area of what is now Manitoba, Canada