
Abstract
This study implemented Indigenous research methods, including yarning, to understand First Nations youth’s perspectives of social and emotional well-being and how e-health can support their well-being. Six First Nations youth (aged 18–25 years, M = 21.33) based in Victoria, Australia, yarned with the First Nations researcher between April and July 2022. Yarns emphasised the importance of connection to family, Community, Mob, Country, and Spirit in maintaining and strengthening well-being. These findings were extended to yarns about e-health, where it was recommended that trust and cultural safety be considered in their design and implementation. These considerations should be explored in light of the ongoing impacts of colonisation, which contribute to fear and mistrust of governments experienced by First Nations youth. The findings provide meaningful contributions to the growing field of e-health and amplify First Nations voices to guide the development of culturally safe and effective e-health.
Keywords
Introduction
Over the past decade, there has been a burgeoning body of literature examining the use of e-mental health tools, broadly referred to as e-health among youth, commonly including digital mobile applications and online websites (Doraiswamy et al., 2019). Defined as “digital resources and interventions to support and improve mental health” (Jones et al., 2020, p. 928), e-health is gaining traction particularly within the field of youth mental health. Growing evidence supports the use of e-health for a myriad of benefits for users seeking digital and virtual mental health care worldwide (Sharma et al., 2020; Wies et al., 2021). Representing the largest potential for benefit, youth are a group most at risk of mental illness while being the primary-end users of e-health (Lattie et al., 2019). Studies have highlighted the potential for youth targeted e-health to enhance accessibility (Grant et al., 2020), autonomy, and empowerment of users (Ignatowicz et al., 2018).
To achieve this potential, it is essential that young people have input into the development and evaluation of these tools, including populations such as Aboriginal and Torres Strait Islander youth, hereafter referred to as First Nations. Technology usage among First Nations youth is estimated to be 60% of the population—20% higher than their non-Indigenous counterparts, revealing a significant opportunity for the benefits of e-health (Rice et al., 2016). Hence, this study aimed to amplify the voices of First Nations youth, placing value on their unique insights and perspectives.
In seeking First Nations youth’s perspectives of e-health, it is essential to first consider how mental health is uniquely viewed and conceptualised within First Nations communities. Contrary to western models which confine views of health to the absence of illness (Coe, 2021), First Nations communities typically view well-being holistically. For example, the social and emotional well-being (SEWB) model (Gee et al., 2014) highlights the importance of intertwining relationships between family, culture, spirit, Community, and connection to Country as a framework for health. Consequently, western models of mental health within mainstream Australian health services often fail to meet the SEWB needs of First Nations Australians (Gee et al., 2014).
Furthermore, First Nations Australians often have significant distrust towards the Australian health system which comprises their sense of cultural safety (Korff, 2019). Culturally unsafe environments can be characterised by normalised racism, perpetuated both interpersonally and institutionally, impacting health policy and the health system environments in which staff practice (Laccos-Barrett et al., 2022). In contrast, cultural safety identifies a space of shared meaning, knowledge, and respect, whereby First Nations Australians feel comfortable to express themselves openly (Taylor & Guerin, 2019). Despite the growing number of studies related to First Nations Australians (Bennett & Gillieatt, 2022), few acknowledge or appropriately integrate cultural safety, nor implement culturally appropriate methods of data collection (Fitzpatrick et al., 2017). This problem extends to e-health, a field inherently built on data collection and storage.
Few studies have considered the perspectives of First Nations youth and the role of cultural safety in the design and use of e-health (Hensel et al., 2019). Although limited, current research surrounding the efficacy of e-health for First Nations users indicates positive outcomes (Brusse et al., 2014). Strong engagement and favourable use was reported by First Nations users aged 15–25 of iBobbly, one such mental health app which integrates cultural knowledge and expertise (Tighe et al., 2017). Furthermore, apps which incorporate traditional localised language and a culturally appropriate worldview were also preferred by First Nations adults (Davies et al., 2015). Hobson and colleagues (2019) emphasise that more research exploring First Nations youth perspectives is needed to increase understanding of mental health apps efficacy for this population. In particular, co-design of health interventions and trusted Community partnerships are important considerations for culturally safe and effective e-health design and usage for First Nations users (Gilbert et al., 2021; Han & Lee, 2018).
Despite co-design with First Nations youth being imperative to the development of e-health for First Nations youth (Schueller et al., 2019), research has primarily been conducted on rather than with First Nations populations (Uink et al., 2022). Only in recent decades have decolonised research methods grounded in First Nations ways of knowing, being and doing commenced being recognised within academia (Battiste, 2013; Smith, 2012). Driven by Indigenous values, decolonised research methodologies reflect First Nations cultures and disrupt the colonial imbalance of power in researcher–participant relationships (Wilson, 2008). In aiming to decolonise knowledge and shift our position from being observed, to being collaborated with, it is imperative that Indigenist research methodologies, which have a history pre-dating colonisation (Adams & Faulkhead, 2012; Murrup-Stewart et al., 2021), be implemented in research related to First Nations communities (Martin & Mirraboopa, 2003).
Current study
This study aimed to understand First Nations youth aged 18–25 years perspectives on (a) SEWB and (b) e-health in supporting their well-being. In line with Indigenist research methodologies (Bessarab & Ng’andu, 2010), yarning was used for data collection and analysis. Yarning, understood as a technique aiming to form trusting, reciprocal relationships, allows the researcher and participant to share knowledge through storytelling of memories, experiences, and perspectives (Shay et al., 2021). With over 150 First Nations language groups still spoken today (Australian Bureau of Statistics, 2021), it is important to acknowledge Australia’s First Nations communities are vastly diverse and each comprise their own languages, cultural structures, and belief systems (Leong et al., 2019; Mawson, 2021). The current study was undertaken by a Warumungu (a First Nations people, Northern Territory, Australia) woman with participants, herein referred to as knowledge-holders (Murrup-Stewart et al., 2021), from a range of First Nations communities.
Method
Research paradigm
This study was guided by Indigenous Standpoint Theory, which emphasises the positionality of the researcher within their research paradigm (Foley, 2003). The first author’s own cultural values and beliefs shaped the research purpose to align with ethical responsibilities and First Nations epistemologies (Murrup-Stewart et al., 2021). Taking this approach involves negotiating the “cultural interface” (Nakata, 2007, p. 195). As a First Nations woman, I, the first author, am situated in the contested domain of western methodologies, in which the field of psychology is built, versus my cultural knowledges (Harvey & Russell-Mundine, 2018). Although I recognise my privileged position of education, to the knowledge-holders I may be deemed an insider as a First Nations woman and an outsider located within a university which prioritises western ways (Ansloos et al., 2019). Here arises the ongoing discourse whereby the researcher must negotiate two worlds, which is not at all Black and White. Accordingly, I carry relational accountability to First Nations communities, specifically young people, for the data gathered, analysis conducted, and words written (Barlo et al., 2021).
To negotiate these two worlds, this research was guided by Kirkness and Barnhardt’s (1991) four Rs—Respect, Relevance, Responsibility, Reciprocity, and involved seeking guidance, collaboration, and co-authorship from First Nations academics in utilising Indigenist methods for both data collection—Research Yarning—and analysis, Collaborative Yarning (Bessarab & Ng’andu, 2010). These practices ensured the ethical and cultural integrity of this research project (Australian Institute of Aboriginal and Torres Strait Islander Studies, 2020; Caverley et al., 2020). Study protocols were approved by the Monash Human Research Ethics Committee (32203).
The authorship team consisted of First Nations researchers M.N.W., J.R., and C.M.-S. with experience exploring First Nations SEWB and youth, First Nations academic K.A. with extensive experience in utilising Indigenous research methodologies, and supervisor L.J. with extensive research experience in cultural psychology.
Knowledge-holders
Stories were shared through Yarning (Bessarab & Ng’andu, 2010) with six First Nations young people aged 18–25 years (M = 21.33 years). Four knowledge-holders identified as women and two identified as men. Like other Indigenous Standpoint research, knowledge-holders and the researcher had existing relationships (Pidgeon & Riley, 2021).
Knowledge-holders were recruited via email, with information about the study provided over time to build familiarity with the research and carefully consider their involvement. Yarns were held in mutually agreed-upon locations or via Zoom. Pseudonyms were used as nominated by each knowledge-holder.
Data collection
Three types of Yarning were used: Social Yarning, Research Topic Yarning, and Collaborative Yarning. Social Yarning commenced the Yarns, whereby freedom, openness, and trust were emphasised to lay the foundations of a reciprocal relationship between knowledge-holders and the researcher (Atkinson et al., 2021). Research Topic Yarning, which is described as a “yarn with a purpose” then followed (Bessarab & Ng’andu, 2010, p. 40). This explored the research aims within a defined beginning and end (Bessarab & Ng’andu, 2010). Social Yarns comprised up to 60 min, while Research Topic Yarns were on average 42 min, reflecting the importance of relationality and cultural communication protocols.
A Yarning Guide was developed by the researcher in collaboration with a First Nations academic, ensuring the guiding questions were culturally safe and framed to promote open yarns.
Written informed consent was obtained from all knowledge-holders and verbally confirmed prior to commencing the yarns. Audio recordings of each yarn were transcribed. Knowledge-holders were provided food and drink and received an AUD$50 voucher as compensation for their time.
Knowledge analysis
Collaborative Yarning is an Indigenist method of data and knowledge analysis which aims to gain a deeper understanding of First Nations stories (Shay et al., 2021). Murrup-Stewart et al. (2022) outline how Collaborative Yarning, as a tool of reflection, is a valid and culturally appropriate approach to data analysis. As shown in Figure 1, Collaborative Yarning first involved two researchers independently reflecting on each transcript. Guided by the research aims, researchers sought to draw meaning from the knowledge shared in the yarns before meeting for Collaborative Yarns to identify common reflections related to the aims. This method was then replicated between two researchers who reviewed one third of the transcripts to further strengthen the validity of findings before sharing and seeking feedback from the knowledge-holders. Collaborative Yarning took place over an 8-week period, creating opportunity for ongoing reflection. Complemented by a layered approach to sharing and understanding, these reflections helped to uphold the quality, credibility, and validity of the final findings (Murrup-Stewart et al., 2021).
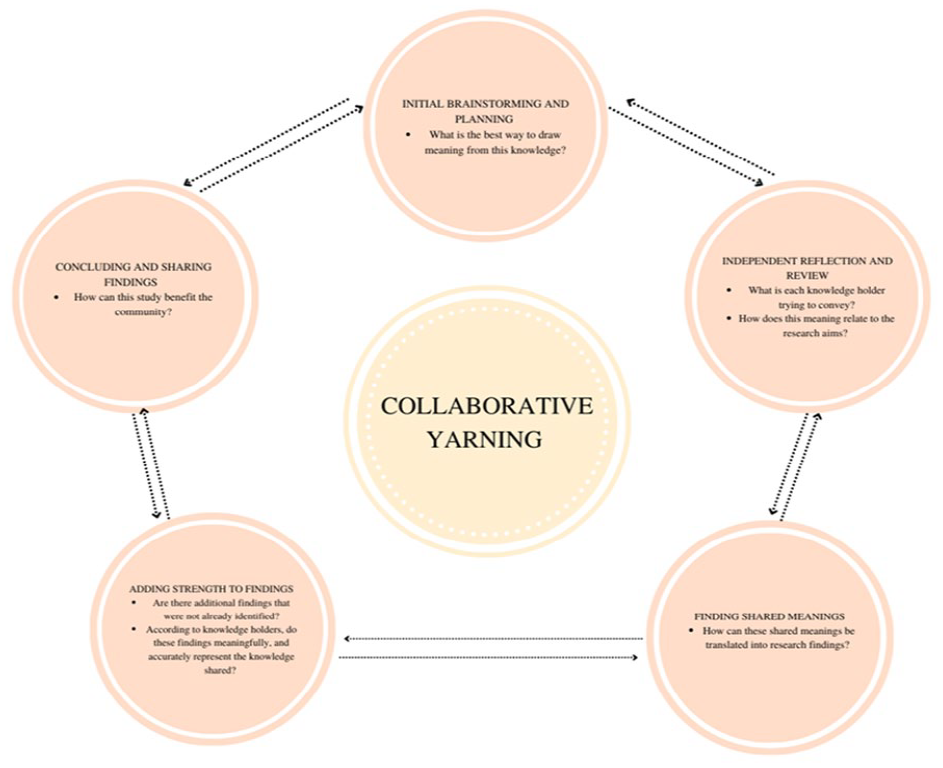
Visual representation of how Collaborative Yarning was undertaken.
Results
SEWB: connection
The theme of connection underpinned all knowledge-holder’s perspectives of SEWB, with connection to family, Community, Mob, Country, and Spirit and friends serving to strengthen and maintain First Nations youth well-being: Unless we have our connection to Mob, Country, our totems, and our forms of spirit we are not at our peak of social-emotional wellbeing. (Audrey, female, 24 years old)
When prompted about what strengthens one’s SEWB, knowledge-holders highlighted the importance of family, Community, and friends. As Audrey (female, 24 years old) noted, “I always have to be connected in with family of some sort, whether it be friends, whether it be Mob.” For some knowledge-holders, there was overlap between the three. When describing what strengthens SEWB, Pete (male, 19 years old) defined his family and Community as one: “having Community there around you—your family.”
Importance was placed on connection to Country and Spirit in strengthening SEWB. For some, being connected to Country comprised being physically on their Traditional Country, or on land described by knowledge-holders as “away from colonisation”. Audrey (female, 24 years old) drew parallels between uncolonised land and sacred places, describing forming a connection to places untouched by colonisation as a compromise for not being on her Traditional Land.
E-health: trust and cultural safety
Knowledge-holders extended the theme of connection when providing their perspectives of e-health for supporting well-being. Specifically, they noted that where familiarity and connection is established, trust and cultural safety may be supported. Furthermore, yarns generated wider themes including the ongoing impacts of colonisation, what happens with First Nations data collected on e-health, and e-health Aesthetics. The following sections explore each theme.
Familiarity and connection
Given knowledge-holders’ emphasis on connection underpinning strong SEWB, it is unsurprising that knowledge-holders identified feeling more likely to trust e-health when they experienced a sense of connection and familiarity. This familiarity was facilitated through seeing photographs of First Nations communities or knowing someone who has used and recommended the tool. Building on this, knowledge-holders’ distrust and scepticism of using e-health and willingness to share data seemed to be a direct consequence of a lack of representation and familiarity.
When it was identified e-health was mob-led, trust and cultural safety was almost automatically established. Most knowledge-holders expressed a clear preference for mob-led e-health; “If it’s for Mob it should be by Mob” (Gwendaline, female, 23 years old), and “If it’s meant to be supporting Indigenous people, then I believe an Indigenous org[anistaion] should head it” (Tammy, female, 22 years old).
Reflecting the diversity of perspectives, some knowledge-holders expressed the view that government developed e-health had potential for trust to be established. Montgomery (male, 19 years old) noted his acceptance of e-health which involves government, “it wouldn’t change how I use it”, but reflected he would take “more cautionary” steps.
The yarns highlighted the importance of familiarity in fostering trust, as without familiarity, some knowledge-holders may be reluctant to share identifiable data regardless of the tool’s origins.
Ongoing impacts of colonisation
Black fellas don’t trust the government for reasons going back hundreds of years. (Gwendaline, female, 23 years old)
The ongoing trauma and impacts of colonisation were identified barriers to establishing trust and cultural safety on e-health, for example, through a fear and mistrust of the government. Referencing the Stolen Generations, one knowledge-holder described their hesitancy to share personal data with e-health led by government organisations as they felt this could lead to “being reported and having children taken away” (Audrey, female, 24 years old). Through these discussions, safety and trust were considered essential, but for some, deemed almost unattainable when involving government. “I don’t think you can have a culturally safe place with a government organisation to begin with” (Audrey, female, 24 years old).
Although knowledge-holders acknowledged the efforts made to address the negative impacts of colonisation, some were deemed tokenistic or ingenuine. For example, Acknowledgements of Country were described in some cases as “tick a box” (Tammy, female, 22 years old) features of e-health. While seeing an acknowledgement was appreciated, knowledge-holders emphasised the importance of genuineness, which many perceived to be lacking in e-health. Tammy (female, 22 years old) described her experience viewing two websites: One had this massive acknowledgment, and it was surrounded by all this beautiful Aboriginal art .. . . Then the other just had such a generic one. It was like maybe blue and white—and I was like [obsenity] that . . . the other just felt more . . . safer. It just looks very generic and slapped together—like this is a government website.
What happens with First Nations data
It’s not the fact that they want the information . . . what are they actually going to use that for? (Montgomery, male, 19 years old)
Knowledge-holders reported concerns with what happens to their data once it is collected. Gwendaline (female, 23 years old) and Pete (male, 19 years old) described issues of data being used against them rather than for them, as common occurrences in government data collection. It was also noted that often First Nations data collected by governments is represented as numbers and figures. Knowledge-holders felt this disregarded their culture and identity and failed to represent them. They wanted to be represented in terms of their identity and have their data used to advocate for them and their Communities. As described by Pete, “it doesn’t look like it [government e-health] would advocate towards me . . . I would look like a number . . . rather than an Aboriginal man.”
This also ties into the lack of transparency about data usage in government institutions. In addition, knowledge-holders described wanting clarity around exactly what data would be used, and for what purpose. As identified by Gwendaline (female, 23 years old), a lack of transparency related directly to trust; “Black fellas don’t trust people with their data, and they don’t want to talk about it. They don’t know where it’s going.”
Where e-health was transparent around data collection and usage, allowing knowledge-holders to “know what I was getting myself into” (Montgomery, male, 19 years old), a greater sense of trust was established, making knowledge-holders more likely to share their data. Knowledge-holders described their preference for seeing an explicit statement explaining why their data would be collected, how it would be used, as well as “an option to pull away” (Montgomery, male, 19 years old).
What does it look like? How does it make me feel?
I want to see the words [cultural safety] and I want to see the actions. I want both. (Audrey, female, 24 years old)
Knowledge-holders described how e-health aesthetics impacted their perspectives on e-health, particularly on establishing a sense of cultural safety and trust.
“Clinical” and “governmenty” (Tammy, female, 22 years old) aesthetics, including bland colours—blue, yellow, white, long paragraphs of information and limited visual components, led to a lack of cultural safety. Parallels were drawn between a lack of cultural safety felt on e-health to other generic environments not designed for them or their families; “To me it feels very clinical like it doesn’t feel like a safe [e-health tool] because it just . . . it feels like I am in a hospital” (Audrey, female, 24 years old).
Knowledge-holders also identified a link between cultural safety and First Nations artwork or design. Knowledge-holders often quickly pointed out a lack of First Nations artwork on some tools and the negative effect this had on their perspectives of e-health. For instance, Pete (male, 19 years old) noted, “Just the plain text and no pictures or anything, it doesn’t look as inviting,” and Tammy (female, 22 years old) stated, “It seems really governmenty . . . that’s definitely a negative.”
In contrast, where First Nations artwork was included on mob-led e-health, Gwendaline (female, 23 years old) noted “it’s obviously for Black fellas so immediately I know that I’ll be culturally safe.” Audrey (female, 24 years old) reinforced this impression, “it’s got warm colours, it’s got that connection, it’s got the feet which represent the journey, like it’s got all these things that point to it being culturally safe.” However, it is important to note that while these cultural elements may infer trust and cultural safety, this alone was not enough for knowledge-holders to deem a tool culturally safe. “I would be a bit more trusting but I’m still overall not trusting enough to give my information away” (Tammy, female, 22 years old).
The importance of familiarity was further emphasised through photographs showing First Nations Communities using e-health, or groups of Community members smiling together, being positively regarded by knowledge-holders. In addition, seeing photographs of well-known and respected First Nations Community members inferred trust for knowledge-holders towards e-health through association.
Discussion
This study explored First Nations youth perspectives on SEWB and the potential role of e-health on supporting their well-being. Collaborative Yarning found that knowledge-holders characterised their well-being as connection to the SEWB domains of family, Community, mob, friends, Country, and Spirit. Knowledge-holders offered recommendations for how this well-being could be supported via e-health, noting the importance of connection, trust, and cultural safety, and recognising the impacts of colonisation. Echoing the perspectives of other First Nations youth (Murrup-Stewart et al., 2021), knowledge-holders placed importance on connection to family, Community, Mob, friends, Country, and Spirit in strengthening and maintaining SEWB (Gee et al., 2014), thereby reinforcing the need to reflect these understandings when designing and implementing health services for First Nations youth (Farah Nasir et al., 2021). Understanding and valuing these perspectives of SEWB are key to dismantling western colonial models of health, which often preclude First Nations youth from accessing culturally safe care (Gee et al., 2014). Such paradigm-shifts are essential for strengthening First Nations youth well-being (Tighe et al., 2017) and bridging the gap between health and well-being disparities of First Nations and non-First Nations Australians (Ketheesan et al., 2020).
The yarns highlighted that connection to SEWB extends to the use of e-health. Where connection or familiarity is felt, trust and cultural safety may be established when using e-health. Consistent with current research (Hobson et al., 2019; Tighe et al., 2017), there was a clear preference among knowledge-holders for e-health that included First Nations artwork, photographs, and other visual elements that represent First Nations communities. While knowledge-holders emphasised that these elements contributed to a sense of cultural safety and trust, the mere presence of these aesthetic features was not enough to guarantee a genuine culturally safe engagement with e-health. Knowledge-holders identified feelings of fear and mistrust of e-health, drawing links to the impacts of colonisation and highlighting a need to consider and address wider systemic barriers. These systemic barriers relate to how the Australian health system is embedded within a settler colonial structure, which fails to address SEWB, perhaps preventing First Nations youth from experiencing the potential benefits of e-health.
Although research covers impacts of colonisation in a variety of settings, such as primary education, healthcare, and research (Aguilar et al., 2021; Gatwiri et al., 2021; Snow, 2018), little attention is paid to the perspectives of First Nations youth and the ongoing role that colonisation plays in their lives (Murrup-Stewart et al., 2021). This study provides new insights into how colonisation affects First Nations youth’s SEWB and considerations for e-health tools targeting SEWB. The findings reveal how even in online formats, the presence of colonisation is felt by First Nations youth. There is an ever-present reminder of the trauma experienced by them, their families, and their communities. This study suggests e-health must go beyond aesthetics to consider systemic barriers which prevent the attainment of cultural safety and trust. Service providers designing and implementing e-health tools must work to understand the impacts of colonisation and the experiences of First Nations youth, to build genuine cultural safety for users.
Where First Nations’ conceptualisations of SEWB are included, e-health may offer potential solutions to further reducing the gap between health outcomes of First Nations and non-First Nations Australians (Melia et al., 2020). By amplifying the voices of First Nations youth, health and well-being services in Australia can be realigned to strengthen and maintain First Nations SEWB through supporting and valuing connection to family, Community, Mob, friends, Country, and Spirit. The study highlighted how this can be achieved through tools designed by, and for, First Nations people. In addition, it was important to consider transparency around any data usage, suggesting e-health tools must clearly inform users about how and why their data will be used. This connects to the idea of autonomy and sovereignty, that First Nations users should have choice over their data usage and that data should be used to further benefit the individual and their Community.
This study offers the following recommendations for how e-health can strengthen and maintain First Nations youth’s SEWB. First, it is recommended that e-health seeks to facilitate a connection with First Nations users by (a) understanding and prioritising their conceptualisations of SEWB and (b) incorporating culturally safe aesthetic features. Second, e-health developers should address the ongoing impacts of colonisation that can effect First Nations youth’s establishment of trust and cultural safety. Figure 2 visually represents key recommendations and quotes from knowledge-holders which may help facilitate connections between users and e-health in a culturally safe way. It is important to note that these insights are unique to the six knowledge-holders included in this study, who each carry with them individual connections to family, Community, Mob, friends, Country, and Spirit. Therefore, recommendations should be interpreted as such, serving as valuable insights to direct further research in this field.
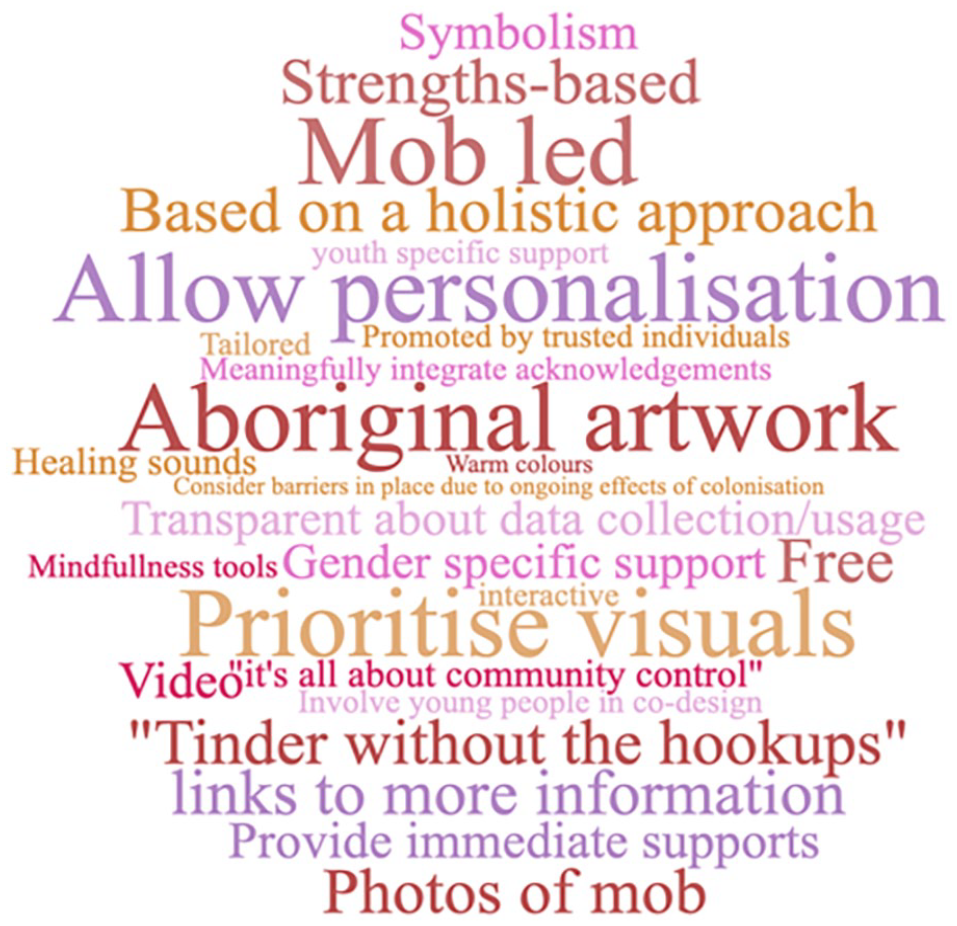
Word cloud showing a visual representation of knowledge-holder recommendations for e-health.
A potential limitation of this study is a lack of gender diversity. The relationship between researchers and knowledge-holders can determine how First Nations people, particularly youth, communicate and hold trust throughout the Yarn (Davidson, 1988; Kearins, 1981; Westerman, 2010). The limitation of gender difference between the researcher and knowledge-holders may be demonstrated as the two shortest research topic yarns were held with male knowledge-holders. Therefore, future research should seek to incorporate more diversity in the research team and knowledge-holders to allow the voices of gender diverse, and others with unique needs, such as LGBTIQ+ and young people with disabilities to be heard. By decolonising research, to value First Nations epistemologies and incorporate cultural safety into the research process, First Nations youth may feel safe to share their much-needed insights to contribute to a growing body of research around how their SEWB can be strengthened and maintained via e-health.
In sum, this study reinforces the value of privileging First Nations youth perspectives on their own well-being needs. By utilising Indigenist research methodologies, First Nations epistemologies allowed the researchers to gain insightful knowledge which can contribute to emerging field of e-health and its cultural adaptability. Specifically, e-health targeting First Nations youth should be built on a holistic conceptualisation of SEWB; e-health must go beyond aesthetics to establish genuine trust and cultural safety. These are vital steps for e-health to strengthen the SEWB of First Nations and help bridge the gap between well-being outcomes of First Nations and non-First Nations youth. However, this potential must contend with the ongoing effects of colonisation. Crucially, it was identified that even where e-health makes efforts to consider cultural safety by facilitating a sense of connection, without recognising the inherent mistrust of governments that First Nations communities experience, SEWB may not be effectively supported via e-health tools. Future efforts must aim to address these gaps by decolonising the western deficit-based notions of health that dominate the existing Australian mental health landscape.
Footnotes
Acknowledgements
We acknowledge the lands of the Kulin Nations on which this article was written, and those of the generous Knowledge Holders and authors. We also acknowledge Elders past and present for their ongoing care and connection with the lands and waterways, and thank them for protecting this Country since time immemorial. We acknowledge the contributions of Community members, Murrup bung-Allambee and the Action Lab team.
Authors’ note
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors received no financial support for the research, authorship, and publication of this article.