
Abstract
This article presents a study on the experiences of Indigenous Australians living in the Greater Darwin Region in the Northern Territory during the COVID-19 pandemic. The main aim is to understand the impacts of the pandemic on various aspects of the lives of Indigenous Australians. A survey with open-ended questions was distributed during the period of May to December 2021 to potential participants and responses were collected either face-to-face or online. The responses were analysed using descriptive statistics and inductive thematic analysis. Results of the analysis showed that the pandemic experiences can be grouped in to five key themes: restricted travel, mental health issues, vaccination contention, work and employment changes and fifthly, for some participants, the pandemic caused only minimal impact which can be interpreted as the positive impact of the border closure policy measures.
Introduction
This study delves into and analyses the firsthand experiences of Indigenous Australians who were at risk disproportionally during the COVID-19 pandemic because of their aggravated social vulnerability in comparison to the rest of the society. Although community transmissions and cases of COVID-19 infections have remained low in Australia compared to other countries, proportionally more COVID-19-related deaths were recorded for people with low socio-economic status (Australian Institute of Health and Welfare [AIHW], 2021). The Australian Government considers Indigenous Australians, remote communities, elderly people, people in aged care facilities, people with chronic conditions, people with disability and travellers were most at risk during the COVID-19 pandemic (Department of Health, 2021). Many of the Indigenous people in the Northern Territory (NT) were therefore in combined risk groups causing an increased chance of experiencing severe impact when exposed to COVID-19. Despite that, there is only a limited literature recording or reporting the actual experiences of Indigenous people during the COVID-19 pandemic beyond their high vulnerability as predictive factor for severe impact from the pandemic.
This research is aimed at analysing the firsthand experiences of Indigenous Australians living or staying in the Greater Darwin Region (GDR), NT, during the COVID-19 pandemic. Data on livelihood changes were collected during the period of May to December 2021 through direct face-to-face and, for computer literate participants, online survey. The main research question was, how has COVID-19 impacted the lives of Indigenous Australians in the GDR? The direct answers from individual participants served as the primary data for the analysis to provide a more generalised picture of Indigenous experiences. The target participants were Indigenous Australians aged 18 years and older. The research was conducted by Indigenous and non-Indigenous researchers, and together with Indigenous Australian cultural consultants. The non-Indigenous researchers have had extensive experience working closely with Indigenous people and Indigenous communities, and they have been working and practicing in the NT for more than 5 years.
This article covers, first, a brief overview of the literature on how Indigenous Australians were more at risk during the pandemic through their exacerbated social vulnerability in comparison to the rest of the society. This provided vital information for the authors to identify emerging themes on the impacts of COVID-19 on Indigenous Australians. Second, we highlight the specificity of the NT and the GDR, as a distinct remote area within Australia geographically isolated from the urban-metropolitan core of the continent with its specific socio-demographic configuration and the related risks during the COVID-19 pandemic. This allowed us to posit the survey and to discuss its results by identifying the potential impacts from the socio-demographic specificity of the geographic location. This was necessary to provide a more generalised outcome in a broader, Australia-wide context. Third, we presented the key findings based on a systematic analysis of the responses and discussed these findings. Finally, we highlighted the generalisable knowledge gained by this research and addressed ethical issues and limitations, followed by our recommendations.
The disproportionate vulnerability of Indigenous Australians
The COVID-19 pandemic which started in early 2020, can be interpreted as a worldwide disaster event (World Health Organization [WHO], 2020). Disasters can put people at risk disproportionately based on their social vulnerability (Karácsonyi et al., 2021). Social vulnerability of the populations or individuals can be characterised by their demographic composition such as age, gender and marital status, as well as racial, cultural, housing, and socio-economic situation such as income level and employment (Donner & Rodríguez, 2008; Robinson, 2003). Furthermore, their vulnerability also depends on where they are, if they are on the move such as temporary visitors, tourists, and refugees (Naik et al., 2007). The variation in the levels of social vulnerability of different populations emphasises the scale and timing of the impacts from COVID-19, are inherently a function of social circumstances, which in turn determine who is at risk and who is impacted (Blaikie et al., 1994; Wisner et al., 2004). Thus, the hazard event, the spread of the virus is a trigger which exposes pre-existing vulnerabilities generated by power–law relationships as well as underlying social and economic inequalities (The Lancet, 2020; Wisner et al., 2004).
Based on the social vulnerability approach, homelessness, low socio-economic status, namely poor living conditions, having low or inadequate income, insufficient education and unemployment has been the most prevalent cause of increase in the vulnerability of certain groups of people around the world during the COVID-19 pandemic (AIHW & National Indigenous Australians Agency, 2021; Dut, 2021; Karácsonyi et al., 2021; United Nations, n.d.). Minority and Indigenous peoples are particularly hard hit by the COVID-19 pandemic (Bertocchi & Dimico, 2020; Gaynor & Wilson, 2020; Kim & Bostwick, 2020; Poteat et al., 2020). Consequently, epistemological and ontological debates concerning high variations in COVID-19 mortality rates across countries, regions and populations cannot be resolved without understanding social vulnerability (Brown, 2020) since mortality rates are primarily determined by the social status of the population (The Lancet, 2020).
Aboriginal and Torres Strait Islander people, also referred to as Indigenous Australians were also disproportionately impacted during the COVID-19 pandemic. Most Indigenous Australians are within the low socio-economic category due to factors such as historical marginalisation, colonisation, and living in rural and remote areas geographically (Jardim et al., 2020; Karácsonyi et al., 2021; Yashadhana et al., 2020). The Australian Government’s Closing the gap report 2020 indicates that although there are improvements from previous years, the employment rates and educational attainment for Indigenous Australians are still below the rest of the society (Department of the Prime Minister and Cabinet, 2020). Indigenous people in Australia are suffering from the highest unemployment rates particularly in remote communities located in the sparsely populated inland and northern areas of the continent.
For Indigenous people, their vulnerability is also elevated due to pre-existing poor health and living condition (United Nations, n.d.) and for many Indigenous Australians, complex health, social and economic issues have been prevalent in their lives even before COVID-19 crisis began (Follent et al., 2021). As socio-economic status is one of the determinants of health (AIHW, 2020), it therefore places the Indigenous people in an increased susceptibility to experiencing adverse impacts during COVID-19 pandemic, especially in an event of severe outbreak. For instance, considerable proportion of Indigenous population suffer from chronic diseases such as heart diseases, diabetes, kidney disease, alcoholic liver diseases, respiratory and cerebrovascular diseases, and cancer (AIHW, 2014). The 2018–2019 National Aboriginal and Torres Strait Islander Health Survey revealed that almost half (46%) of Indigenous people had one or more chronic health condition (Australian Bureau of Statistics [ABS], 2019). These chronic diseases are likely to worsen the impact of the COVID-19 pandemic (Power et al., 2020; Treskova-Schwarzbach et al., 2021). Indigenous people living in the remote and regional areas are more susceptible to the swift transmission of communicable or infectious diseases, hence in higher level of vulnerability in case of the spread of COVID-19 (Crooks et al., 2020; Eades et al., 2020; Yashadhana et al., 2020).
One of the most effective ways to minimise transmission of infectious diseases is by vaccination (Antia & Halloran, 2021). Vaccination against COVID-19 is important to keep people safe and reduce the burden of disease especially among vulnerable population. Indigenous people have been one of the priority groups since the first vaccine roll-out (National Aboriginal Community Controlled Health Organisation [NACCHO], 2021). Nevertheless, in media articles, there were news of vaccine hesitancy among Indigenous people which was due to factors such as misinformation, conspiracy theories, fears, concerns and distrust (Brennan, 2021; Jash, 2021; Richards et al., 2021; Tsirtsakis, 2021). While there were news articles and many studies on COVID-19 vaccine hesitancy, a limited number was found specifically for Indigenous Australians. One such study was by Graham et al. (2022), who reported that vaccine hesitancy among Aboriginal people in Western Sydney was due to concerns of vaccine safety, misinformation and a lack of confidence in governments and health institutions.
Beside the direct health impact, there were socio-economic consequences of the pandemic as well. For example, Follent et al. (2021) reported that during lockdown, there was limited supply of food and essential services to Indigenous communities, often with staggering increased prices. Remote communities experienced disruptions in supply of essential services and goods and the price for essential grocery items had risen by 400% compared with buying them in Darwin. This has impacted the Indigenous people financially and families found themselves going without food daily. They experienced significant financial and emotional strain due to inability to meet essential needs, concerns about food insecurity and limited access to financial services and support (Central Land Council, 2020). On the contrary, there were reports of positive impacts of COVID-19 restrictions such as some people were able to spend more time on country, feeling safe in the community and the ability to learn more about culture and traditions (Smith et al., 2020).
In summary, there are many studies and reports since 2019 that have been dedicated to evaluating the impact of COVID-19 including in Australia. Many of the publications we listed so far supplied valuable contributions on understanding the underlying and ongoing issues. Most literature agree that Indigenous people are more at risk to be impacted by infectious diseases due to existing social and economic disadvantages. However, limited literature has been found that are recording the actual experiences of Indigenous people during the pandemic. Therefore, the authors considered it important for this study to include face-to-face and online surveys of the relevant population.
Methods
Study area
This article put Indigenous Australians and their firsthand experiences during the COVID-19 pandemic in the middle of its investigation. Indigenous Australians are demographically, socially and geographically very diverse population. In this section, we discuss first the specificity of the case study area, the NT and its Indigenous population. This is necessary to identify the impacts from the localised socio-demographic and geographic contexts and by that to deliver a more generalised knowledge on Indigenous experiences. The description of the study area is supplemented by thematic maps designed by the authors where public census 2016 statistics by ABS (2017) were managed and visualised in ArcGIS software.
NT is a specific place both in terms of its remoteness, sparseness, and its specific demographic and economic environment (Carson et al., 2011) where highly productive raw material extraction and tourist industries are co-existing with socially and economically marginalised remote Indigenous communities (Carson & Koster, 2012; Taylor, Johns, et al., 2011). Outside the capital city area, the entire territory is considered as either remote or very remote area (ABS, 2018). Remote and very remote areas have a significant Indigenous population in Australia in general: 18.6% of the Indigenous population (148.5 thousand people) lives in these areas contrasted to the only 1.5% of the non-Indigenous population (350.1 thousand people) (ABS, 2017). Within the NT itself, this ratio is even higher: 79% of Indigenous Territorians live in remote and very remote areas, while 21% live in the GDR. In this study, GDR refers to the area covering the cities of Darwin and Palmerston, and their surrounding rural areas called the Litchfield local government area. As shown on Figure 1, Indigenous Australians form an absolute majority population, typically over 80%, outside GDR and except mining and tourist towns.
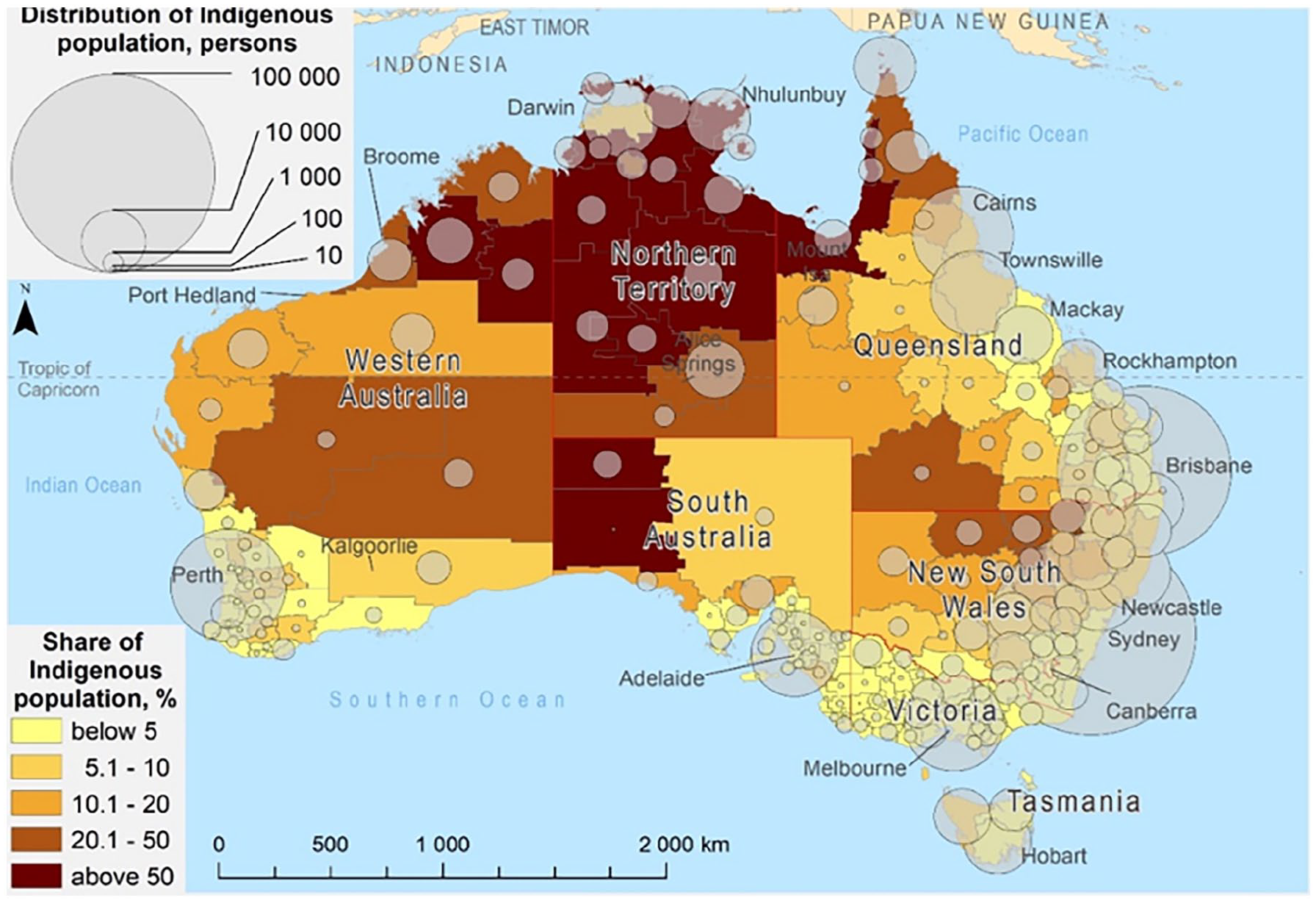
Share and distribution of Indigenous population in Australia.
At the census night of 2016 (ABS, 2017), 74,546 Indigenous Australians lived in the NT which is 30.3% of the total population of the territory, the highest share across states and territories of Australia.
In the NT, 59.6% of Indigenous population has spoken one of the Indigenous Australian languages at home in contrast to only 9.8% of the total Indigenous population of Australia. This strong socio-demographic and cultural differentiation within the Indigenous population is also highlighted on Figure 2, which further stresses the specific situation of the NT and its Indigenous populations. For example, during the onset of the pandemic, it was essential that relevant information was provided in Indigenous Australian languages as well to the population of the NT (Northern Territory Government, 2020).
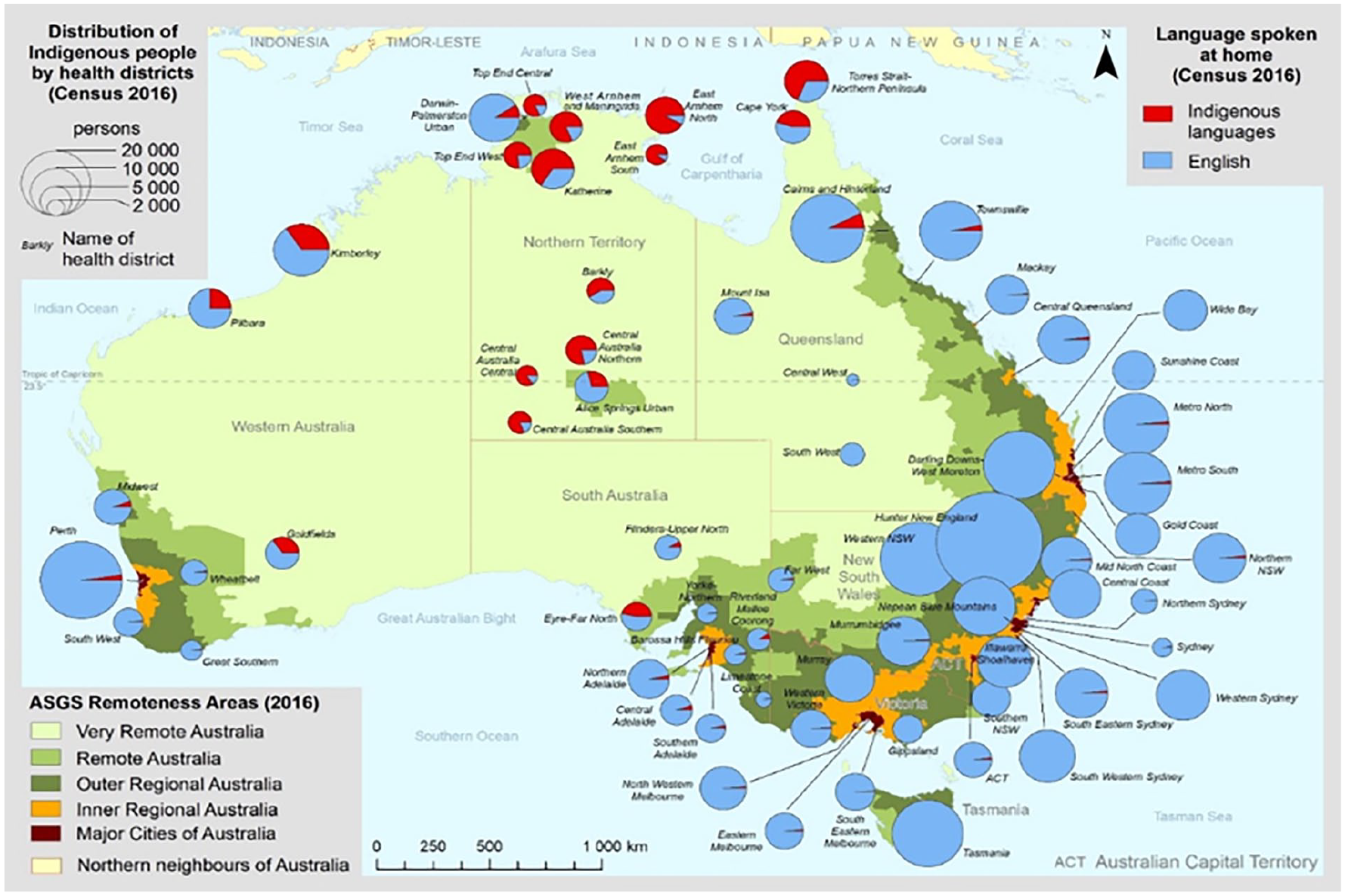
Remote and very remote areas and the language spoken at home by Indigenous Australians.
Data by ABS also shows many Indigenous people fall in the category of low socio-economic status due to high unemployment rate, low income and lower education. As shown on Figure 3, unemployment within the Indigenous population is not only much higher than within the non-Indigenous population, but it is the highest in remote and very remote areas. In contrast, the unemployment rate within the non-Indigenous population is lower in remote areas than in non-remote areas and main urban centres. This means that remote locations have a larger socio-economic gap between Indigenous and non-Indigenous populations which also underlines the specific situation of Indigenous Australians in the NT (Taylor, Larson, et al., 2011).
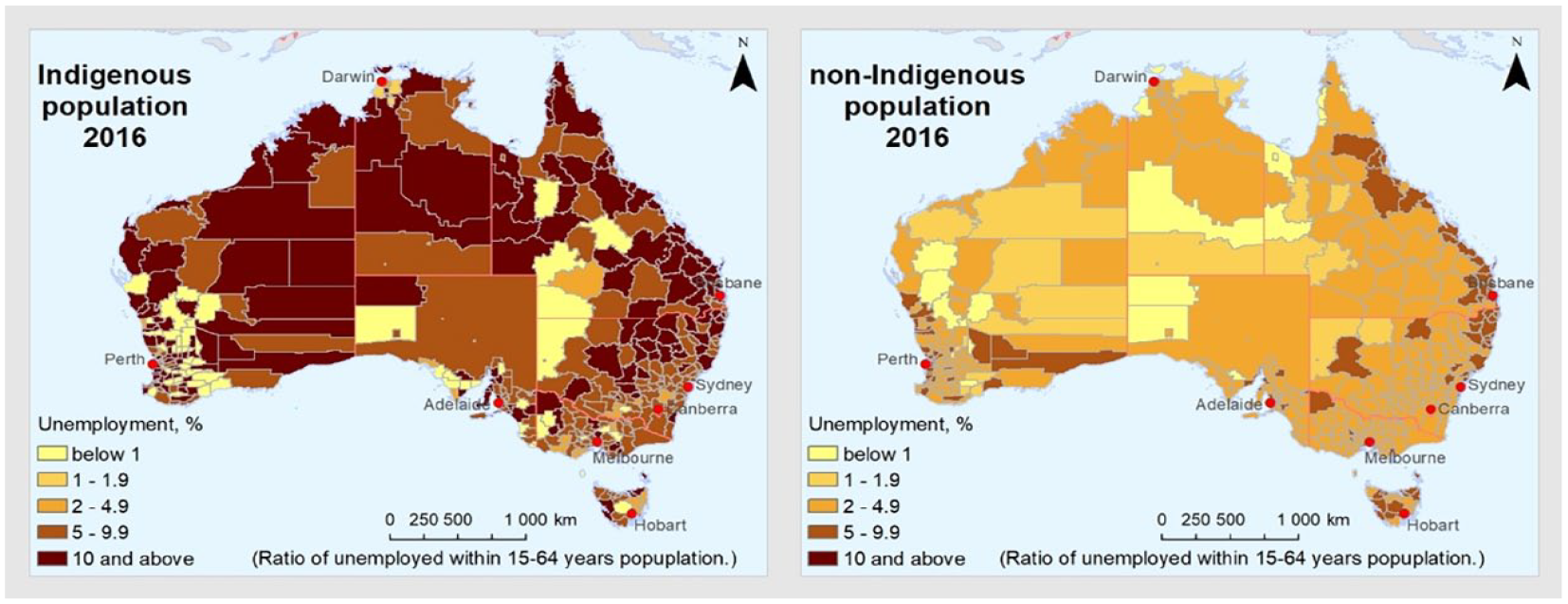
Indigenous and non-Indigenous unemployment in Australia.
While old age was a significant vulnerability factor during the COVID-19 pandemic, as shown on Figure 4, ratio of people aged 60 and above is lower than among the non-Indigenous population particularly in remote areas. Despite that, the shortages of hospital beds, limited health services, and shortages of medical practitioners and health workforce (Higgins, 2020) means a significant risk in remote areas of the NT. The NT has only one major hospital, the Royal Darwin Hospital and six smaller hospitals spread across the NT.
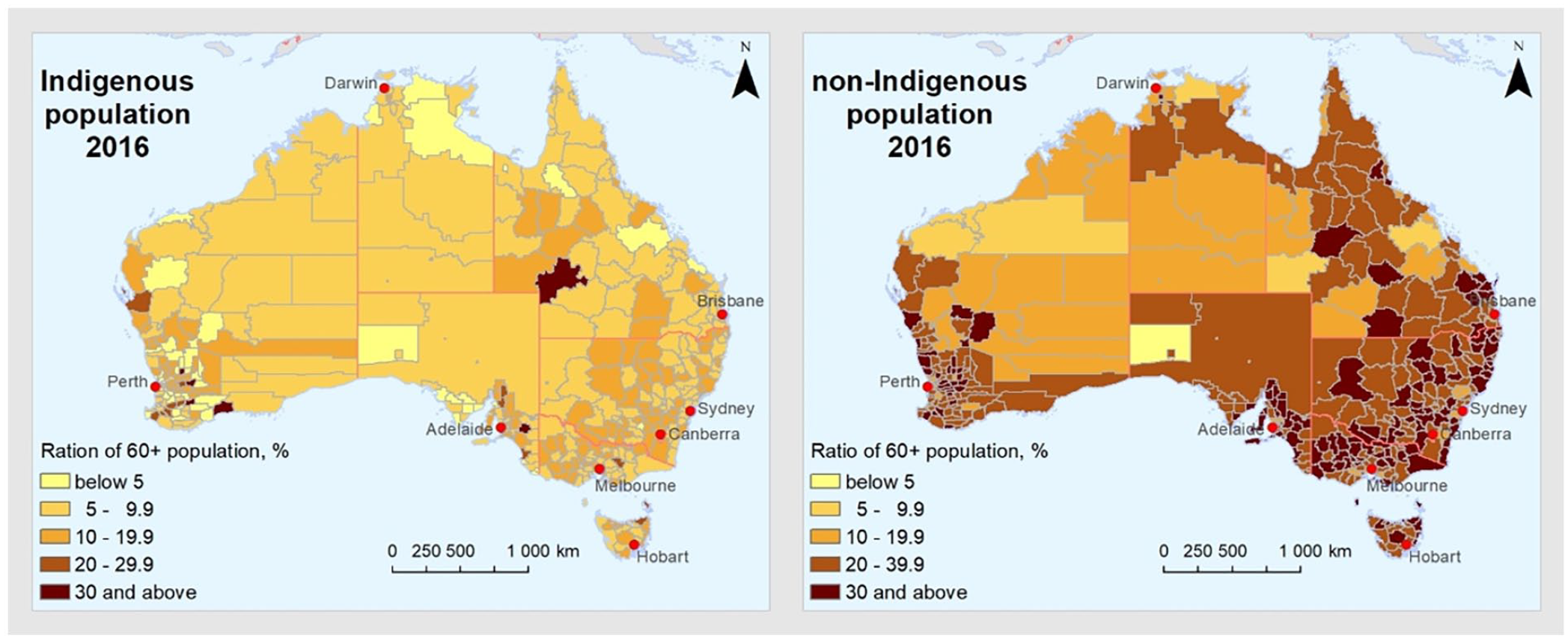
Aging of Indigenous and non-Indigenous populations in Australia.
Furthermore, GDR is strongly connected to the rest of the Territory as a significant service hub for Indigenous Australians living in remote communities (Taylor, Johns, et al., 2011; Taylor, Larson, et al., 2011). Indigenous people from remote communities often travel to Darwin for health care services, visiting relatives, accessing governmental and other essential services or attending court. Their mobility in terms of their residential address, as shown in Figure 5, is however lower than the non-Indigenous population. The latter one is mostly working in remote mining communities temporarily, but not living permanently in the Territory which means a high residential turnover in remote areas. During the pandemic, the access to remote Indigenous communities was restricted to protect their residents (Eades et al., 2020) such as the instigation of biosecurity zones (Northern Land Council, 2022). This, however, has caused further difficulties for local remote residents under COVID-19 movement restrictions.
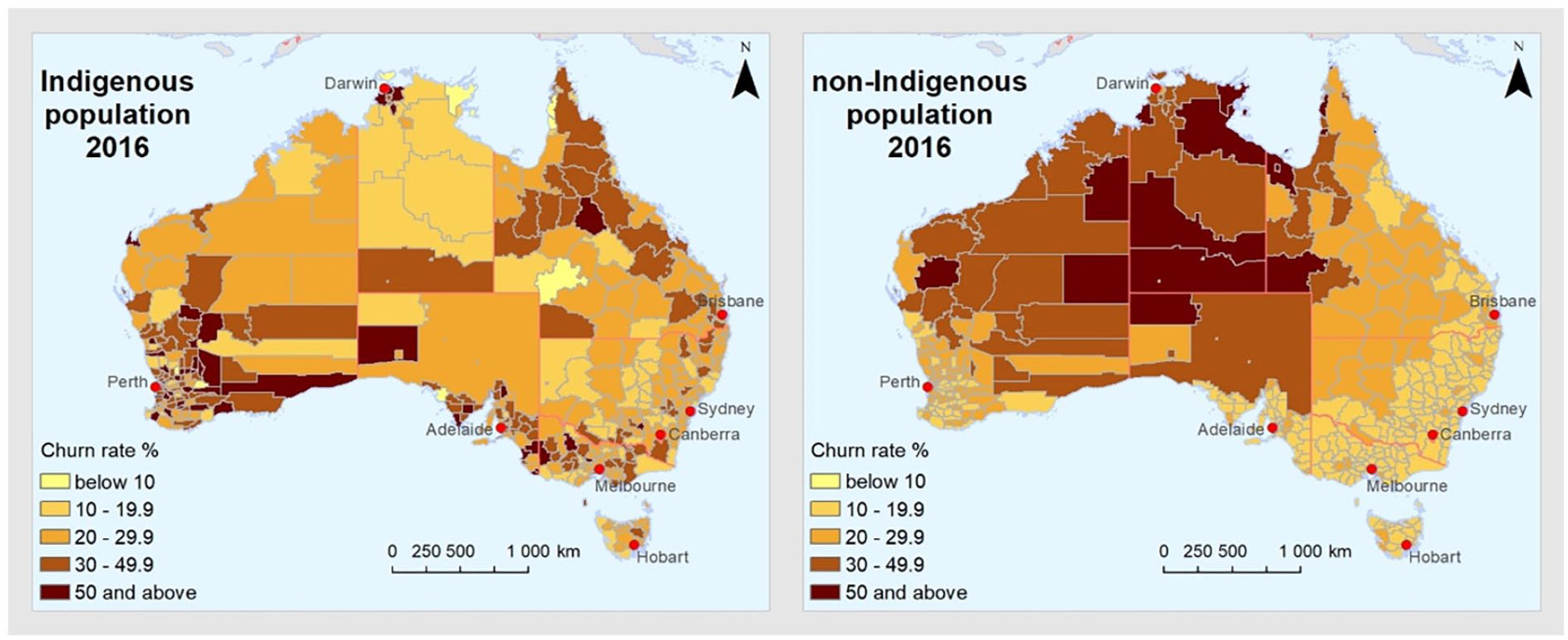
Churn rate or migration turnover in percentage of the resident population of Indigenous and non-Indigenous population.
Based on these socio-economic, demographic, cultural and mobility characteristics, the Indigenous population in the NT was in a vulnerable situation during the COVID-19 pandemic. In frame of this research, we aimed to do the face-to-face and online survey to better understand their experiences during the pandemic beyond quantifying only their vulnerabilities. The methodological detail of our survey is described below.
Survey
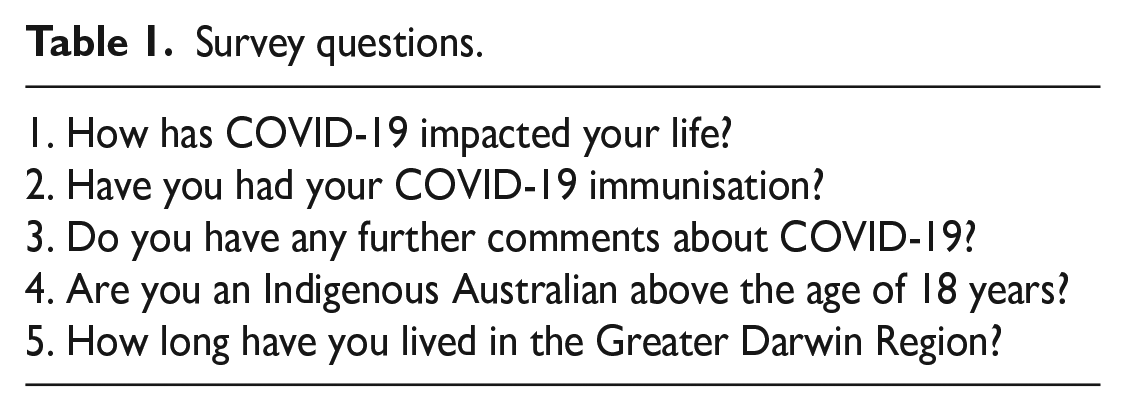
Anonymous survey with open-ended questions as shown in Table 1 was distributed by the research team members and the local Indigenous research consultants to residents in GDR between May to December 2021. Questions 1, 2, and 3 were designed to collect qualitative information from participants. Questions 4 and 5 screened for the targeted participants, which were Australian Indigenous people aged 18+ who live or visit the region during the study period. This research has obtained clearance from Charles Darwin University’s Human Research Ethics Committee, ID: H20070.
Survey questions.
Non-probability convenience sampling, as by Neuman (2014), was the most culturally suitable strategy to collect data. Many of the participants agreed to do the survey as they were approached in a culturally proper way by Indigenous researchers. Members of the local Indigenous community played a crucial role in the research as cultural research consultants by engaging with local people to be surveyed either in their community, at home, in public spaces or online. It was a significantly important task to gain the trust and respect of those who agreed to participate. Responses from the participants were collected either face-to-face or by using SurveyMonkey, an online survey platform.
Responses from the participants were analysed using inductive thematic analysis (Braun & Clarke, 2006; Creswell & Creswell, 2018; Neuman, 2014). Survey responses were coded based on the recurring main ideas. Codes were initially identified separately by one Indigenous author and one non-Indigenous author with the aid of Microsoft Excel for manual coding and NVIVO survey auto-code. The coding process included multiple rounds of coding, team discussions and refining. The initial codes were then used to generate final themes relating to the experiences of Indigenous Australians living in the GDR during COVID-19 pandemic.
Results
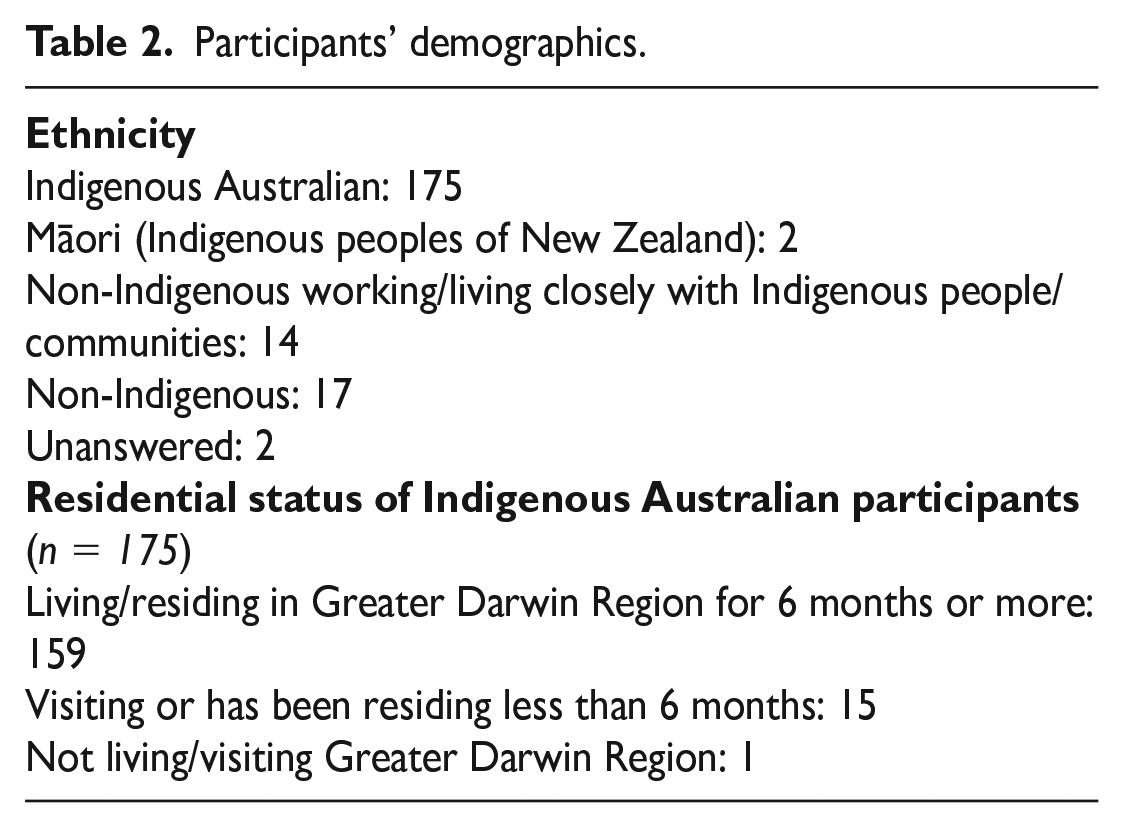
There were 170 face-to-face and 40 online participants, a total of 210. From this total, 83 responses were recorded from May 2021 until before the first official lockdown in Darwin on 27 June 2021. Meanwhile, 127 responses were recorded afterwards until just before NT borders were fully open on 20 December 2021. Results reported in this article are from the responses of 175 Indigenous Australian participants. Responses from 35 participants were excluded as their demographic data are not within the scope of this study. Table 2 outlines the participants’ demographics. Since the data collection was conducted before significant local transmission happened in Darwin and in many of NT remote communities, none of the participants commented on any direct impact of getting infected by COVID-19. This puts the results in a specific context where the fear from infection, the vaccine hesitancy and the indirect economic and social impacts of the lockdown and border closure is more significant than the direct health impacts from COVID-19 infections.
Participants’ demographics.
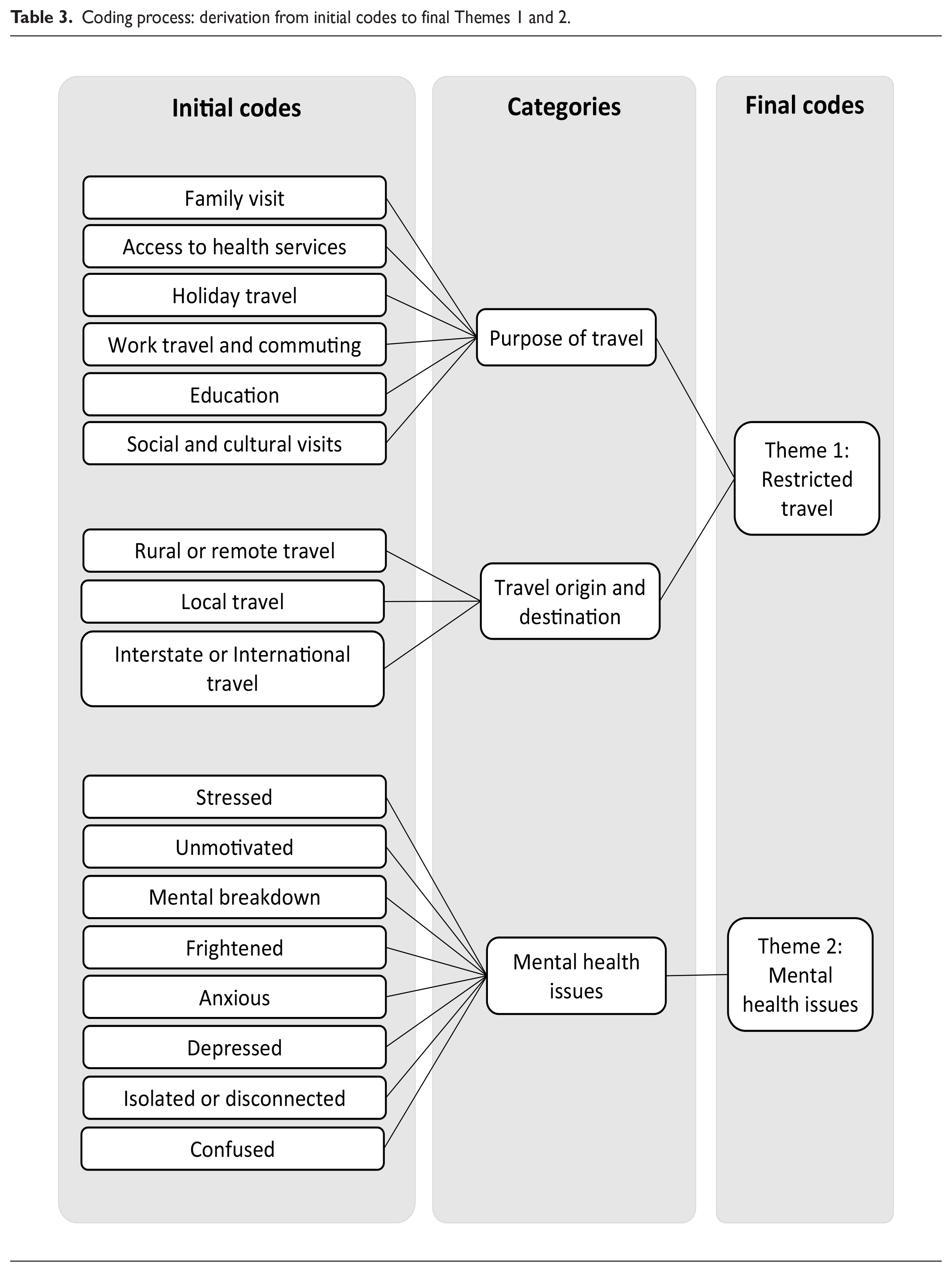
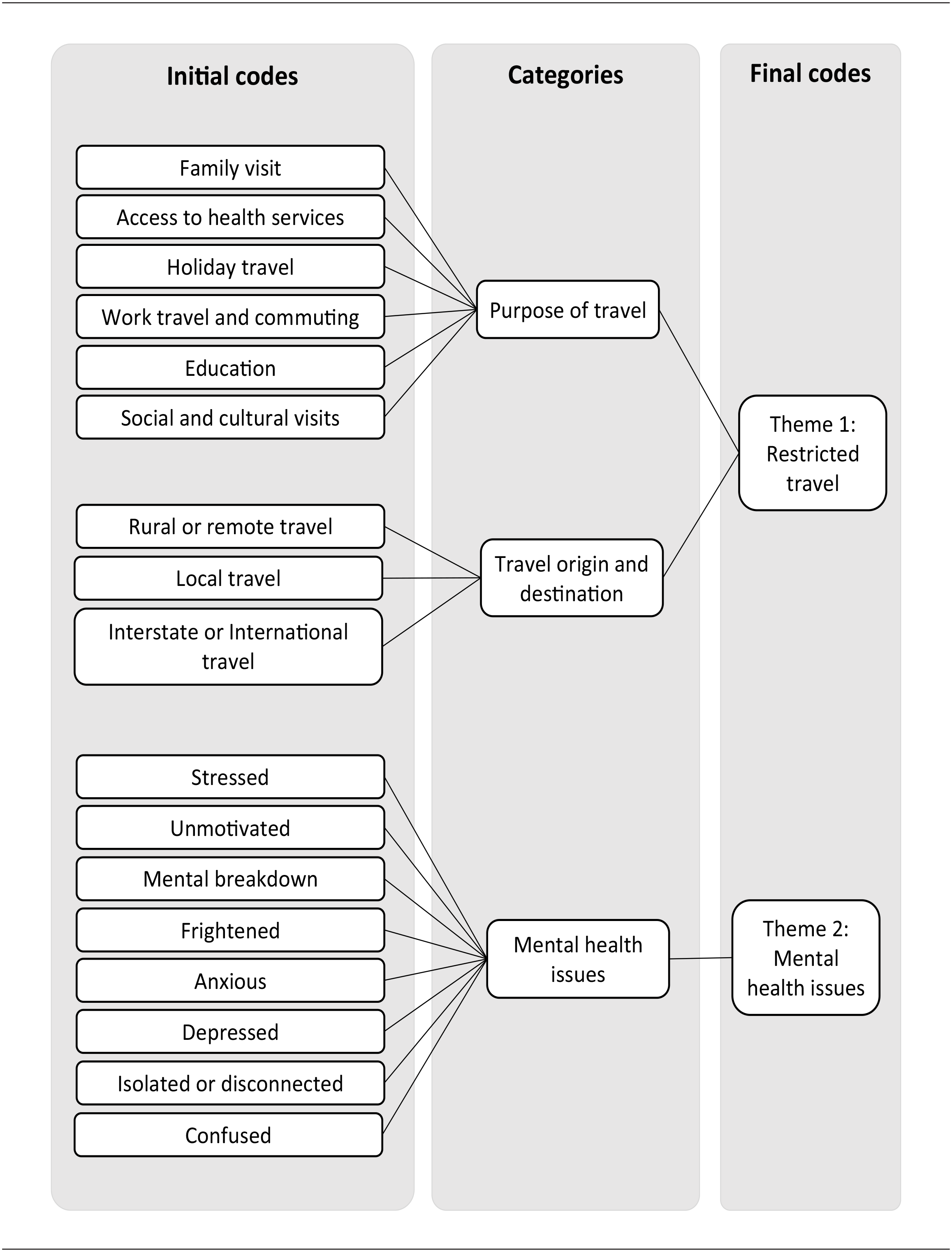
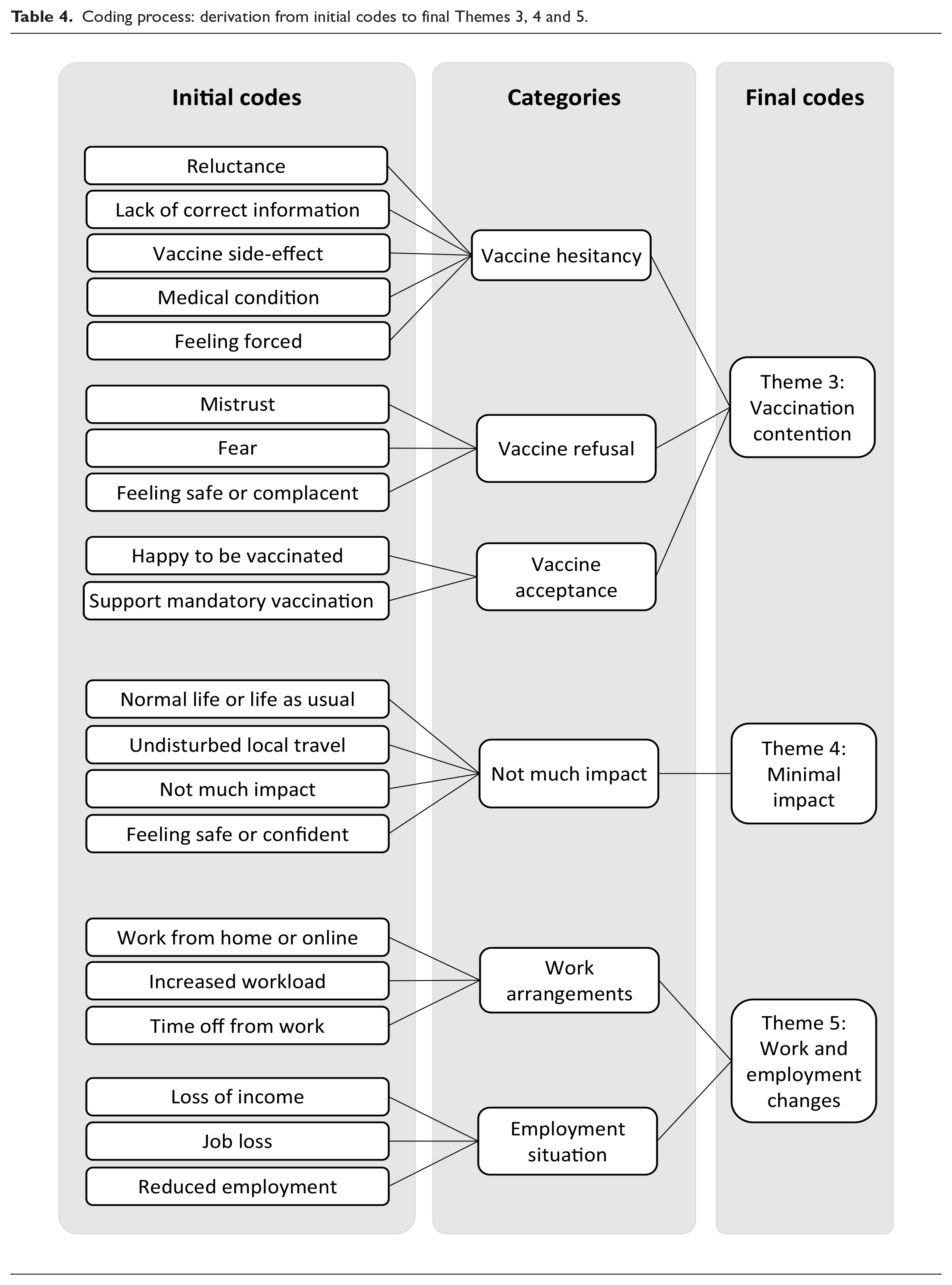
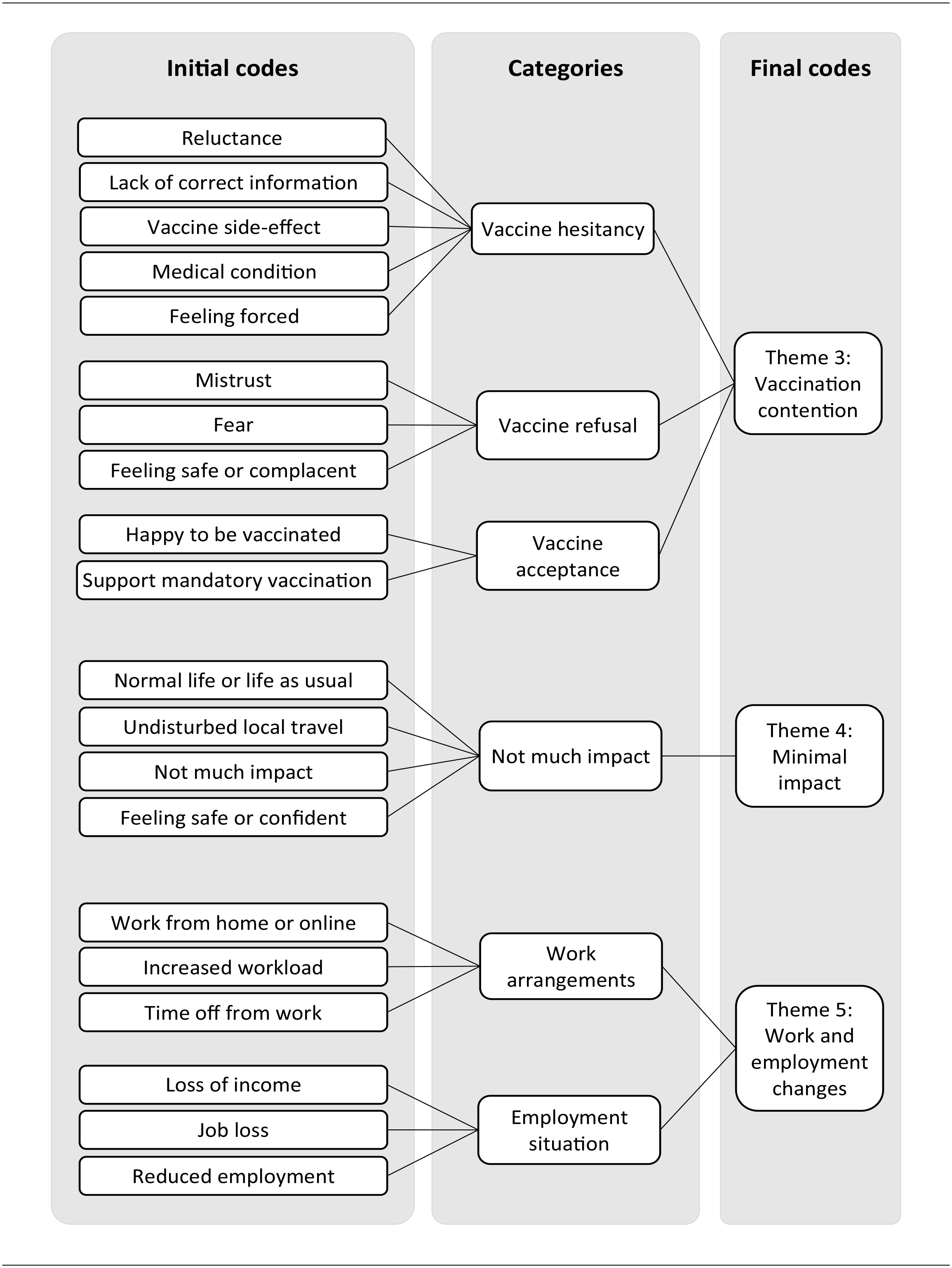
Based on an inductive thematic analysis on participants’ responses, the authors identified several initial codes as outlined in the first column in Tables 3 and 4. From the initial codes, five key themes emerged which revealed the experiences of the participants. These themes are Restricted travel, Mental health issues, Vaccination contention, Minimal impact, and Work and employment changes. The coding process and the themes as derived from the initial codes are outlined in Table 3 for Themes 1 and 2 and in Table 4 for Themes 3, 4 and 5.
Coding process: derivation from initial codes to final Themes 1 and 2.
Coding process: derivation from initial codes to final Themes 3, 4 and 5.
Restricted travel
This theme includes the responses related to visiting or be visited by families interstate or in remote communities, travels for social and cultural obligations, travels for education or work purposes, holiday travels and travels to access health services.
Around 34% (60 of 175) participants said that COVID-19 had changed their regular travel pattern. For some, it has restricted them to visit families living interstate and in NT remote communities. The inability to visit their families due to travel restrictions, lockdowns, and border closures has been difficult: Not being able to travel interstate to see my children and family. (P198) Isolation, not being able to visit/travel family interstate was hard. (P007) Made it difficult to maintain family connections and almost impossible to visit country and family in remote parts of the NT. (P211)
According to some participants, there were difficulties to access health services due travel restrictions and social distancing measures. This has caused “delayed check-up” (P173) and restricted travel for people from remote communities for medical reasons (P014). Meanwhile, other participants reported that travel restrictions have hindered their work travels, holiday plans, travel for educational purposes and have limited their social and cultural obligation activities such as attending sorry businesses or funerals: Stopped work FIFO in mining site. (P012) I . . . have not attended funerals. (P075) Restricted further tertiary education interstate + travel. (P192) Restricted holidays + possible career paths + opportunity interstate. (P194)
These were substantial changes for many of the participants.
Furthermore, travel restrictions have brought disruptions and increased anxiety for some, while others acknowledged the necessity of the restrictions and were appreciative: Restricted travel to my extended family interstate. NT has been in a bubble and am thankful to be safe. (P118) Our people need to be protected, close borders maintained and monitored. (P030)
Mental health issues
Restrictions on movement and travel, fears of getting infected and of its possible fatal consequences, worries of the uncertainties and unknowns, abrupt changes and concerns about vaccination have generated a hard, difficult, and stressful time for many participants. This theme of mental health issues covered the category ranged from fear of catching the virus and the uncertainties of the future to concerns of disruptions to daily lives. It also covers responses such as feeling of having a hard time, worries, anxiety about isolation and lockdowns, and having to make decision about vaccination. At least 89 participants (51%) reported that they experienced challenging times related to COVID-19. Some had felt isolated, disconnected, anxious or worried, fearful and depressed: Disconnection from family who live interstate. Concern/anxiety about travelling with our little ones. (P087) Stressed about getting sick. (P076) worried about my underlying health issues, and for my son. (P210)
The amount of people that have died is very upsetting, and there does not seem to be an end to COVID yet. (P076)
Impacts on mental health have been reported in relation to the inability to connect with families as normal, to perform work as usual and to vaccination.
Vaccination contention
Vaccine hesitancy, refusal and acceptance have been reported among the participants. Some were delaying the opportunity to get vaccinated because they were unsure about getting vaccinated while some have chosen to refuse vaccination. As shown in Figure 6, more than half of the participants (61%; 106 of 175) had been vaccinated with either one, two or three doses of COVID-19 vaccine, while 39% have not had their COVID-19 vaccination.
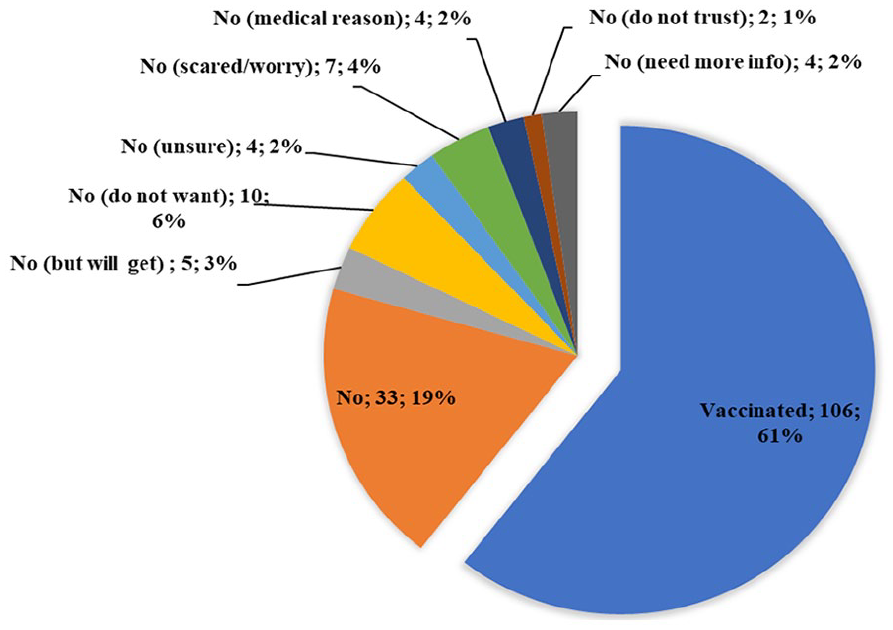
Participants’ responses about their COVID-19 vaccination status.
The reasons for not getting vaccinated including fear of vaccine side effects, medical condition and feeling safe with traditional resources: No [I have not had], probably later, a bit scared of dying from blood clot. (P002) a little cautious about the short trial times of the vaccines. (P085) I got bush medicine to look after [or protect] my body. (P004)
One participant reported of losing their employment due to refusing vaccination:
[I] lost my job because I’m not getting immunised. (P158)
Of the 61% participants who had received their COVID-19 vaccination, some felt forced or pressured due to mandatory vaccination: felt like I have been forced into having the COVID-19 vaccination. (P212) I get pressure for immunisation. (P064)
Meanwhile, some participants accepted that COVID-19 vaccination is essential that they “wish the vaccines were compulsory to all” (P090), and commented that there is a need to “Push to get all peoples immunised to save culture” (P190).
Minimal impact
Based on the analysis, minimal impact is also emerged as a separate theme. Around 29% (50 of 175) participants responded that life was just as normal, they experienced not much impact and some even reported of feeling safe and confident. There has been little to no significant impact of COVID-19 in their lives during the study period. They mentioned that: [COVID-19] has not really impacted anything. (P093) [Life was] no different. Everything still normal. (P004)
Some participants expressed their contentment that life in Darwin is still going on normally and COVID-19 did not affect them in any way: Not much [impacted]. Happy living in Darwin. (P019) Living in Darwin it hasn’t really impacted my life that much. (P080) Those who do not do much travel or do not have the necessity to travel reported that their lives were still as usual.
Work and employment changes
Work and employment have been affected by COVID-related restrictions for some participants. This theme covers responses around working from home, working online, increased workload, losing job and income and reduced employment. One participant reported that he had to voluntarily opted to work from home during lockdown because he: Had kidney transplant for 6 years, immunocompromised. (P171)
Meanwhile, other participants have had to change their mode of work: Having to work from home for almost 4 months in 2020 and feeling isolated and unmotivated. (P087)
Despite many negative experiences recorded due to the restricted life, a few participants acknowledged positive changes in their lives: It was difficult [with] lockdown and isolation, but also good [because] no gambling, save money. (P036) Enjoyed working at home during lockdowns. Learnt to use Zoom and Teams. (P121)
Discussion
This research was aimed at providing firsthand experiences of Indigenous Australians living in the GDR of the NT during COVID-19 pandemic. It used online and face-to-face survey to collect individual experiences from participants which served as the database to provide some generalised outcomes which will be discussed in this section. For the participants in this study, the significant experiences that have impacted their lives include restricted travels, mental health issues, vaccination issues, minimal impact and changes to work and employment situation.
For many Indigenous Australians, visiting and maintaining connections with families, relatives and Country are culturally and socially important in term of health and wellbeing (Butler et al., 2019). These include travelling interstate and to remote communities. Therefore, travel restriction had been one of the significant factors that have directly impacted the lives of Indigenous Australians particularly in the NT. NT is a specific environment characterised by long distances and geographic isolation even without travel restrictions. As travel restrictions to remote communities and border restrictions were announced in March 2020 (Storen & Corrigan, 2020), many people started to experience the disruptions to travel plans which had been echoed by many of the participants in our research as well. Border closures and closing down the communities impacted cross-border and cross-community movement patterns along with the movement between the communities and service centres such as the GDR. Apart from family visits, other impacted travels include access to health services, work, education or study-related trips, holiday, and cultural visits. Although telecommunication and internet technologies have been helpful in keeping people connected, there were times when those could not replace in-person connections.
While travel restrictions and lockdowns, in contrast to large cities in other parts of Australia, had been beneficial in preventing severe COVID-19 outbreak in communities (Smith et al., 2020), these have contributed to increased mental health issues for many participants due to socio-cultural disconnection. Furthermore, in term of work and employment, COVID-19 had caused unprecedented changes in people’s lives. For example, some participants reported of losing their job hence losing source of income, reduced employment, and some had to work from home or switched mode to working online. These had caused some degree of anxiety and elevated stress level.
Meanwhile, other participants have also reported a range of experience related to mental health issues such as being frightened of catching the virus, worried of the uncertainties, stressed about the changes and disruptions to daily lives, and anxious about vaccination. In summary, COVID-19 pandemic has caused more significant secondary impacts in the lives of Indigenous people in the NT than immediate health impacts. These secondary impacts have also highlighted the ongoing challenges and disparity issues in the lives Indigenous Australians in terms of housing, living costs, socio-economic, health and education.
Indigenous people were among the prioritised groups to receive COVID-19 vaccination due to the identified vulnerability and higher health risk (NACCHO, 2021). Vaccination, especially vaccine mandate, however, had become a real issue. The mandatory approach to immunisation may have caused more resistance since there had been a lack of understanding among some people of what the COVID-19 vaccination would do to keep them and their community safe. A targeted socio-cultural approach for vaccination with effective communication on the importance of getting the vaccine may have produce greater acceptance and less mental health issues. This sub-topic will need further investigation.
Our finding showed that there were vaccine hesitancy and refusal among the participants. The major reasons for the participants to delay or refuse vaccination including feeling scared of vaccine side effects, feeling pressured or forced, wanting more information, mistrust, as well as feeling safe. This has several similarities with the study by Graham et al. (2022, p.1) where they reported “fear of vaccine side effects; negative stories on social media; and distrust in Australian governments and medical institutions” were the reasons of vaccine hesitancy among the participants who were Aboriginal people living in Western Sydney.
The experience of having minimal impact, such as little to not much impacted, can be associated with the positive impact of the border closures which kept the virus outside of the NT and allowed a more-less normal life within a COVID-free bubble. For example, no or little impact was predominantly experienced by those respondents who do not usually travel long distances such as to remote communities, interstate or international. In the early 2020, there were a few restrictions in place such as work from home advice (Storen & Corrigan, 2020). However, disruptions experienced by participants were minimal as access to shops, government services, schools and workplaces in GDR was not significantly disrupted during the survey period. Since the start of the pandemic until before the first lockdown, life in GDR was pretty much like normal for many of its residents including the Indigenous people. Living in the GDR at the time when other areas across Australia had been COVID-19 hotspots had created some sense of normality and feeling content and secure. People were free to move around in the NT, and there was no need to wear masks.
As result of the COVID-free situation, none of the participants commented on any direct health impact such as getting infected by COVID-19 virus or were sick due to COVID-19. This sense of being secure is attributable to prompt initiatives from the Australian authorities and Indigenous elders, leaders and organisations to close interstate borders and introduce Biosecurity Zone measures to the NT remote communities. As reported by Crooks et al. (2020), engaging First Nations people to be in leading roles in COVID-19 planning, response and management is proven to be both crucial and beneficial for Australian Government and the wider public. Hence, government initiatives should strongly consider inputs from Indigenous elders in the respective communities.
Conclusion
This study found that during the COVID-19 pandemic in 2021, the major impacts experienced by participants in the GDR were related to restricted travel, mental health issues, vaccination contention, and work and employment changes. Furthermore, several participants reported that they have experienced minimal impacts which can be interpreted as the positive impact of border closures. These findings are important to inform decision-makers in dealing with any pandemic events. An even greater task for the government is to find better solutions to address disparities in access to health care services, facilities and recruitment of workforce, and food security services. This is especially significant for regional areas such as GDR and remote areas in the NT such as those outside GDR, to reduce the level of vulnerability of people at risk during pandemics.
The results of this study have proven the importance of supplying support and ways to communicate to the Indigenous communities, not only when there is urgent situation such as pandemics, but also post-pandemic strategies to support the most vulnerable populations. There is, therefore, a need for the dissemination of correct, simple but focused information to communities during a pandemic and post-pandemic. Furthermore, there is an urgency for continuous attention and practical actions to address existing health and socio-economic gaps for Indigenous people to reduce vulnerability and increase resilience. Since the impacts and experiences related to COVID-19 are ongoing, longitudinal studies or applied social research covering multiple urban and remote communities in the NT would be necessary.
While this study has covered the most populated parts of the NT, it can be extended to exploring the experiences of people in remote Indigenous communities to get better perspectives of their experiences.
Footnotes
Acknowledgements
The authors acknowledge and thank the Indigenous research consultants and all the participants in this study.
Authors’ note
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This study was funded through ARC Special Initiative grant NIRAKN 2012–2022 (grant no. SR120100005).
Glossary
Māori Indigenous peoples of New Zealand