
Abstract
There is very little research about dementia in Aotearoa (New Zealand) New Zealand (NZ) Pacific communities, but information available suggests that Pacific people are presenting with dementia at a younger age and with more severe cognitive symptoms than do non-Pacific. The Samoan ethnic group is NZ’s largest Pacific population. This study explores experiences and understanding of dementia from family sessions with 25 people from 10 Samoan families living with dementia. Thematic analysis of the interviews showed there was no Samoan concept for dementia as a disease of the brain that required special medical attention; instead, Samoan elders spoke of memory loss as part of ageing, signifying the end to one’s purpose in life. A formal medical diagnosis saw family members honouring their obligations to care for their loved one at home, often at great cost. Culturally appropriate services, incorporating Samoan concepts of care and ageing, were rarely available.
Keywords
Introduction
Aotearoa (New Zealand) New Zealand (NZ) has an ageing population and rates of people with dementia are expected to rise (Ma’u et al., 2021), primarily due to the rapid increase in Māori (the Indigenous peoples of NZ), Pacific, and Asian NZers over 65 years old (Alzheimers New Zealand, 2017). For example, while it is predicted that, by 2038, the number of European NZers with dementia will drop, the number of Pacific people with dementia is expected to increase (Cullum et al., 2018), due to increasing Pacific population growth (Ma’u et al., 2021).
Pacific people are over-represented in social deprivation statistics, including negative health outcomes, lack of resource ownership and control, and environmental risk, and are more likely to be affected by intergenerational effects of racism and disadvantage (Salmond et al., 2006). Life expectancy for Pacific elders (75.4 years for males; 79 for females) is significantly lower than for the dominant NZ European group (81 years for males; 84.5 for females) (Ministry of Health, 2021). Age-related diseases such as Parkinson’s disease and dementia will affect some of these older people, so it is important to understand how services and communities need to respond to provide effective support (Ministry of Health, 2013).
Research literature on Pacific older people and dementia is sparse. What is generally known is that when a family elder is affected by any health issues, the whole family and community are affected (Tamasese et al., 2014). The terms for elder across Pacific groups hold deep cultural meanings, signifying cultural status and spiritual roles as knowledge-holders, leaders, and protectors of families and kin groups, placing them in prestige positions within the community (Tamasese et al., 2014). It has been documented that most Pacific families prefer to take care of elders in their homes (Ihara & Ofahengaue Vakalahi, 2011; Tautolo et al., 2017). As a result, Pacific understanding and experiences of dementia in NZ are not typically seen in public care facilities that operate from Western paradigms of mental health.
The Living with Dementia in Aotearoa (LiDiA) is a research project aimed at better understanding dementia in NZ (Martinez-Ruiz et al., 2021). The study explored local memory service data that suggested that Pacific people present with dementia at a younger age and with more severe cognitive symptoms than their non-Pacific counterparts. LiDiA also aimed to better understand the experiences of living with dementia in Samoan and Tongan communities. This article presents the Samoan qualitative data. Samoans are the largest group of the Pacific NZ population, comprising 49% of those of Pacific descent (Statistics New Zealand, 2013).
Methods
The qualitative component of the LiDiA project was used to explore the experiences of Samoan families living with dementia, recruited through memory clinics, Pacific health services, and the wider Samoan community. The talanoa (interviews using Samoan cultural protocols) method (Vaioleti, 2006) is an established Pacific research method using talanoa to provide authentic research data (Tunufai, 2016). After building relationships with service providers and community groups, the LiDiA project researchers invited participation in the qualitative aspects of the study, primarily to build relationships that may then flow into the full quantitative, population-based study of dementia in NZ (Martinez-Ruiz et al., 2021). Ethics approval was granted by the Auckland Health Research Ethics Committee.
Samoan people diagnosed with dementia and their families living in the community were recruited through memory clinics, following a confirmed diagnosis of dementia (Martinez-Ruiz et al., 2021). The study was outlined and informed consent completed for 10 people with dementia and their main caregivers. The talanoa session with each Samoan family occurred at home or in a community church hall, and used both Samoan and English languages in ways chosen by participants. All talanoa were facilitated by the first and second authors, recorded and transcribed. To maintain the integrity of the narratives such as nuances in the use of words and sentence formation, non-verbal gestures, verbal sounds and tone, the transcripts were analysed in the language used for the talanoa.
Multiple readings of transcripts by the first author, in consultation with the research team, allowed us to familiarise ourselves with the data and identify key themes, using a thematic analysis approach to explore the similarities and patterns of meanings across the talanoa (Braun & Clarke, 2021). Once the coding framework had been agreed, NVivo software was used as the administrative tool to confidentially store the data for sorting, coding, and organising the themes and data online.
Results
Details of the participants are shown in Table 1. There were 25 participants from 10 families. In the first five families (P1–P5), the participant with mild dementia, plus listed caregivers, participated in the talanoa (13 people). For the remaining five families (P6-P10), the person’s dementia was severe, they were present at the talanoa but mostly did not speak; it was their caregivers who shared their experiences (12 people).
Participant demographics.
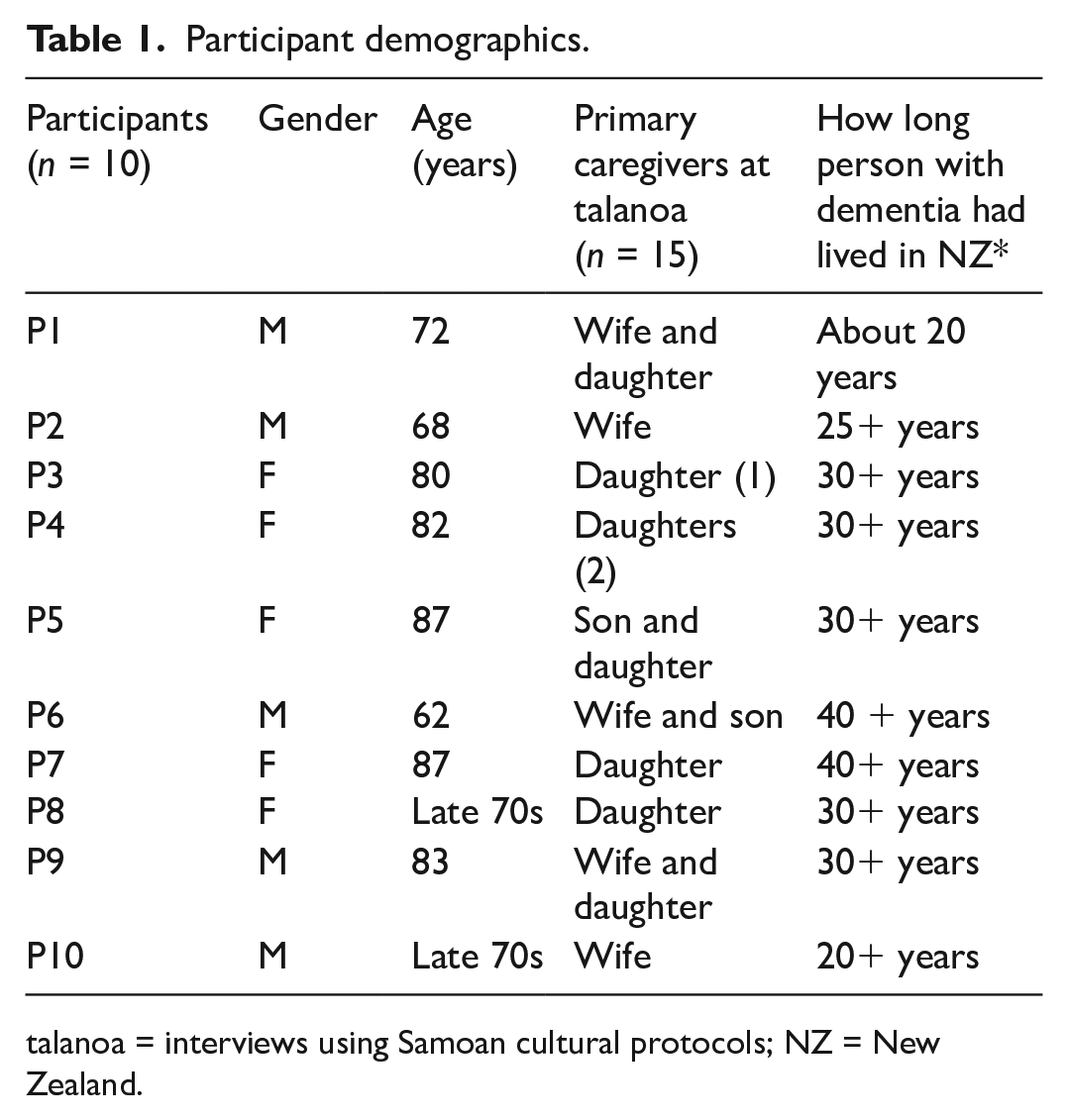
talanoa = interviews using Samoan cultural protocols; NZ = New Zealand.
All participants with dementia were born in Samoa. Caregivers were either Samoan-born or NZ-born. P1–P5 are people with mild dementia and each was interviewed with their caregivers, as listed (5 + 8 = 13 people). P6–P10 experience severe dementia, and their seven caregivers were interviewed, in the presence of the person with dementia (5 + 7 = 12 people).
The 10 participants diagnosed with dementia were born in Samoa, migrating to NZ between the 1950s and 1980s to work. They were great-grandparents, grandparents, and parents, retired from work, and being looked after by spouses, children, and grandchildren in their homes.
The key themes (Table 2) capture how participants understood dementia from Samoan perspectives, issues around diagnosis, the impact of tensions between obligations and care, and the utilisation of dementia support services.
Overview of themes and related subthemes.
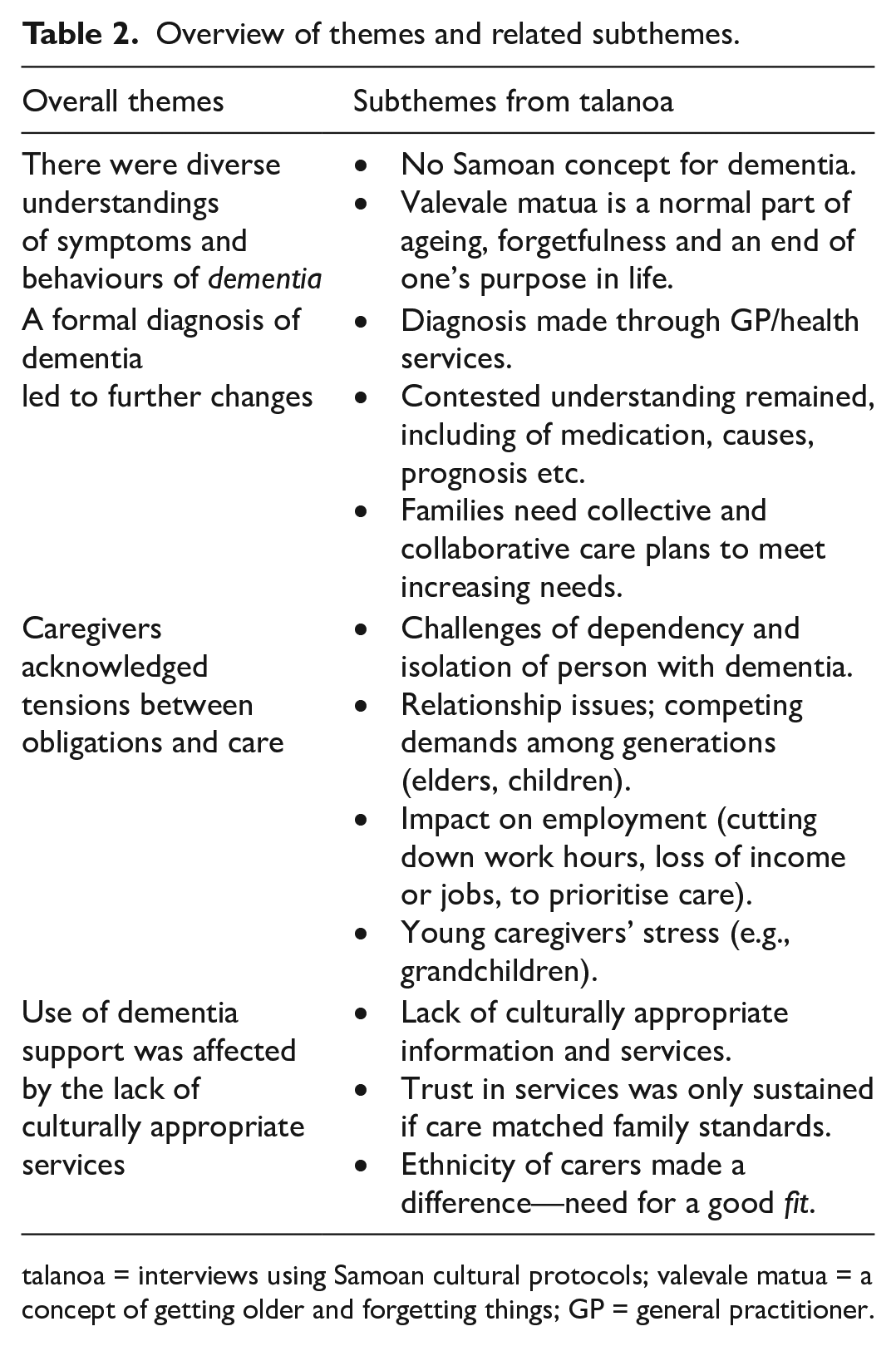
talanoa = interviews using Samoan cultural protocols; valevale matua = a concept of getting older and forgetting things; GP = general practitioner.
There were diverse understandings of symptoms and behaviours of dementia
The definitions and understanding of dementia for Samoan participants varied. The older people (island-born) had a different understanding from the younger caregivers, especially when the latter were NZ-born and highly educated. The Samoan older people normalised memory loss as part of ageing. There was no Samoan term for dementia; older participants described the symptoms of forgetting as a normal part of ageing, using terms like galogalo (forgetfulness). They considered dementia as a palagi (a concept for a Western person) illness. The wife caregiver of her 83-year-old husband (diagnosed with mild dementia) argued that there was no Samoan word for this palagi illness and that forgetting was part of old age: E leai se upu fa’a Samoa o le mea na, le ma’i palagi le na, O le galo o mea o le fa’ailoga le na ua matua le soifua. (Spousal caregiver for P9) There is no Samoan word for this palagi illness, forgetfulness is a sign of old age.
Most older participants spoke of valevale matua. They also spoke of different stages of life where one’s purpose, such as family and church responsibilities, would come to an end when they were older. Valevale matua occurred because one’s life was old, and forgetting things occurred alongside declining physical and mental strength. It was considered by some as the last part of their life journey when there was nothing more left for them to do.
O le valevale matua e mafua ona ua matua le soifua, ua loto galo, ua le manatua mea sa masani ai le olaga, ua matua le soifuaga ma e le toe foi i se lelei. (P3) Becoming forgetful is part of old age and from living a long life, forgetting everyday things in life, are signs of old age, and it is not going back to how it was. Ua matua le soifua ma ua o’o i le faaiuga o le olaga o le tagata, ua uma galuega ma mea e fai, ua o’o ina fa’ai’u’iu le soifuaga o le tagata ola, ua le toe i ai se isi mea o totoe e fai, o le mea lena ua amata ai ona suia le malosi o le tagata ola. (P1) Getting old is the end of one’s life journey, we complete our duties and what we needed to do, there is nothing else left for us; hence, the changes in our strength and life as human beings.
Some participants with mild dementia spoke of different episodes in their lives, confirming the changes they experienced every day as they got older, such as 82-year-old P4 misplacing her jewellery and finding it later in another bag: Ia e galo mea e kuu ai mea i isi kaimi, ia a o isi kaimi, ou ke alu aku o la ga ou kago kuu i le isi ako, (P4) Forgetting where personal belongings are placed sometimes, and other times, she found them in another bag
In contrast, caregivers who were born and educated in NZ tended to have a more explicitly biomedical understanding of dementia, defining it as caused by physiological deterioration of the brain that resulted in memory loss. Others understood their family doctor’s explanation of dementia as a progressive disease of the brain, such as P9’s daughter: The doctor’s diagnosis was mild dementia, and I had no idea what that is, and the doctor said it is a brain disease. I had to go and Google so I can get more information and understanding of what dementia is and what causes it. Now I know it is a brain disease and it can deteriorate over time. (Daughter caregiver for P9)
Other caregivers believed that dementia was due to multiple factors in a person’s life, such as trauma and stressful situations, for example, the sudden or accidental loss of a loved one. Such incidences could affect normal behaviour, so people disconnected and withdrew from everyday routines in life: I think this thing [dementia] a ea, e mafua ona ua ke’i le mafaufau, isn’t it, like a shock to the brain when someone you love suddenly[is] gone without a warning. I do think when someone you love died suddenly, then your whole being is gone too, you let go, a ea, isn’t it, and some people did not want to recover from that shock. (Daughter caregiver for P8)
The spousal caregiver of 62-year-old P6, with severe dementia, shared that her husband’s behaviour changed after the sudden loss of his two siblings some years ago. The husband was the primary breadwinner for their young family until the day he returned from his siblings’ funerals held in Australia. His behaviour changed; he was distant and seemed to be in a different world; his son also noted that his father did not interact with them or respond to any questions, which was very unusual. The most obvious symptom was his sudden inability to remember his regular routines within their home. The participant was taken to their family doctor; after referral on and further assessment, he was diagnosed with severe dementia, but none understood what dementia was and why he was suddenly affected by this illness. The family connected the changes to the loss of two siblings in such a short timeframe: O le fo’i mai ga le maliu o lona sibling, na amata ai o ga faapea, ua ese a le lalolagi la e i ai, ma o loa le makou family doctor fa’amatala i ai le mea ua o’o i ai, refer loa maua i le specialist o le mental health in Greenlane. O le teine foma’i sa sau le fale fai ia test o aka ga kusi, ia fesili aku i ai, ua makua leai a se kali, fai mai la o le galo o mea, ua lost lo ga memory, ia ga fai mai la o le mea ga ole dementia, that’s all they said, ua maua i le mea ga e ka’u o le dementia. (Spousal caregiver for P6) Upon the patient’s return from his siblings’ funerals, he starts to behave differently; he seems to be in a different world. The caregiver took him to the family doctor, and he was referred to a specialist at the local mental health unit. A nurse from the clinic visited the patient’s home and did an assessment, asking him to draw pictures and answer some questions. He did not respond to any questions. The family was told that he had lost his memory and was diagnosed with dementia.
A formal diagnosis of dementia led to further changes
Most caregivers noticed changes in their family member’s behaviour, such as the lack of participation in conversations and their mood shifts. These symptoms caused concern for caregivers and led them to seek advice from their general practitioners; some were prescribed medications, some were referred on to mental health services, or some received both of these options due to the symptom severity. Cognitive assessments resulted in diagnoses ranging from mild cognitive impairment to severe dementia. Most participants and families struggled to understand the diagnosis given and likely prognosis.
Whatever sense made of the diagnosis, participants reported that they tried to follow the instructions from the doctors, like monitoring medications and keeping appointments. They also sought alternatives such as Samoan healing practices and Chinese herbal medicines. Some caregivers learned from doctors that there was no cure for dementia, so they decided to do anything that could help their family members live a good life: We still take our dad to see other doctors such as the Samoan cultural spiritual healers, Māori tohunga, [Maori healer] and we even tried the Chinese herbal drinks. For us, we will do anything that will help dad live and enjoy us. We take him to places and we also try and keep his routines with his church and all that. (Daughter caregiver for P9)
One caregiver explained that when their family member was diagnosed with dementia, they were also told that he was not going to recover: Sa ave i le foma’i ae fai mai ua maua i le ma’i lega o le dementia, e makua ou leiloa a po o le a lea ma’i. Ae fai mai e le koe lelei. (Spousal caregiver for P6) The caregiver took him to the family doctor and he was diagnosed with dementia. The caregiver had no understanding of dementia. The doctor informed the caregiver that he would not be the same again.
Caregivers followed the instructions for prescriptions, but some admitted they altered the medication doses without medical advice when suspecting side-effects and did not go back to the doctor for advice or changes to medications. For example, this caregiver shared that the doctor prescribed pills that were supposed to calm her husband down but did not: E i ai le fualaau ga aumai e calm down ae e fiu e kaofiofi pe a ika, ua fiu e igu le fualaau ga aumai muamua. (Spousal caregiver for P6) There was a medication to help calm him down, but it was hard to calm him down when he was angry, he took the first lot of tablets, but it did not work.
A dementia diagnosis brought many challenges to families. Tautua (to serve, service), is a central value of the Samoan culture (Fa’aea & Enari, 2021). Service includes the obligations of children to look after parents when they can no longer take care of themselves; hence, these study participants were looked after by spouses, children, and or grandchildren.
Caregivers spoke of their fear once their loved ones were diagnosed with this illness; the challenges raised included the parent’s dependency issues and inability to care for themselves, the wider community stigma towards someone with dementia, and the lack of availability of support services. One caregiver reflected on the issues that others also shared: We worry about many things once dad was diagnosed with dementia and the first one was his independence to do things. He resigned from his job of 40 years once he was diagnosed, and that is when things started to change for him and mum. He was very restless because he used to work hard for the family and then suddenly it changed. (Daughter caregiver to P9)
Although there were challenges, caregivers argued that it was the responsibility of the children to have a care plan, and it was their duty, even though they also had to continue providing for their own children: E faigaka lava le mea lea ua oo i ai, but e kakau lava i a makou kids o ga fai makou fuafuaga aua le kausiga o makou makua aemaise ai lava mum. O le galuega lea a makou, but it is also hard o ga we need to work to provide for our families. (Daughter caregiver to P7) It is very hard now, but as kids, we must put a plan in place to take care of our parents, especially mum. It is our duty, but it is also challenging because we need to work and provide for our families.
Caregivers acknowledged tensions between obligations and care
The impacts of caring for family members diagnosed with dementia were reported as unrelenting for these Samoan families. The participants with mild dementia spoke about their vulnerabilities, dependence and the burden on their families. Caregivers acknowledged that dependency, although not intentional, placed a burden on them, but such burdens were considered obligations and commitments as family members, and especially as children. Collectively, it was adult children’s responsibility to ensure their ageing parents were looked after, despite the challenges. The acceptance of collective responsibility may also result in sharing and spreading the load over a larger group of family members: O le matafaioi lea a makou le fagau, [This is the responsibility of us children] we have to look after mum because it is our responsibility as the kids to make sure that she is well looked after. It is quite overwhelming but between us we can make it work. (Daughter as caregiver to P7)
Although the caregivers, especially younger spouses and children, felt indebted to their loved ones, they were faced with multiple challenges and experienced exhaustion. The spouses with limited support from extended families were more likely to experience a breakdown physically and mentally from juggling responsibilities. The children who supported their parents in caring spoke about the restrictions on their freedom to socialise with friends as they prioritised helping out with the grandparent or parent, as this young son who participated in the family talanoa shared: Sa masani na ou alu e tafao i la’u friend, a o le kaimi gei ua maua ai ia le ma’i lea, ua le mafai ona ou alu e kafao pe ou ke alu i ni mea ou te fia tafao ai, because ia ke au, e faigata tele mo si ou tina. I feel sorry for my mum i le va’aiga o ia lea. I worry in case something happens to mum. (Young son as caregiver to P6) He [the son] used to go and spend time with his friends, but because of dad’s illness, he could not go out anymore, to him, it’s hard for mum. He felt sorry for mum, who is the primary caregiver. He worries in case something happens to mum.
The impacts of caring for a loved one with dementia were described as enormous, especially for caregivers with young children. Caregivers and family members who had coordinated a more collaborative care plan had resorted to altering their employment contracts to care for their family member. However, this possibility was not available to all. Overall, such sacrifices created more issues for those with young families, given the rising costs of living and expenses.
Some caregivers indicated that they went through marital problems due to being a principal caregiver to a parent with dementia, where their responsibilities became full-time jobs and left them little time for their partners and children. Such demands were often unanticipated, increasing stress on family relationships. Despite these challenges, all caregivers considered caregiving as their familial duty. As one young caregiver explained, it is the duty of the children, and no matter what the difficulties are, they will find a way to look after their loved ones: No matter what, e fai lava le matafaioi a le fanau [the duties and obligation of the children], we have to find ways to make sure that they are well-looked after. (Daughter caregiver to P3)
Some of the conflicts in fulfilling these duties arose from fear—whether from the medical diagnosis or the person’s unexpected behaviour, which could lead to overprotective and strict supervision of the person with dementia. That, in turn, could produce emotional challenges and conflict with their loved ones, including that the parent with dementia felt infantilised, objecting to being treated like a child instead of as a valued elder.
Use of dementia support was affected by the lack of culturally appropriate services
With the information from their doctors, families knew that their loved ones could not be left alone, and they were encouraged and motivated to do things that would make the person with dementia comfortable and safe. The caregivers all spoke about seeking support and services. NZ has a mix of limited government-funded services such as in-home care, respite, or community activity programmes (Ministry of Health, 2017) and higher needs residential dementia care. Private and community non-governmental organisations (NGO) services include non-residential activity programmes and day care; memory clinics; home help and home nursing which have limited availability; some NGO provision of information and education—whether targeted at dementia or ageing in general, including a few carer support groups; and residential—rest home—activities. Some sought opportunities to learn more about dementia; for example, P8’s granddaughter attended an education workshop at a dementia support NGO. She found the content and language inappropriate for Samoan patients and families: I did not get a lot out of it, they were all palagi, and the way it started, there was not even an introduction or anything at the beginning . . . it was such a weird way of conducting it. The information was good about the brain and the different compartments of the brain, but I wanted to hear and share real experiences, I did not go back to other sessions. (Granddaughter caregiver to P8)
This caregiver also noticed that her grandmother did not show signs of dementia when she was among Samoan people and engaged in Samoan activities, such as singing Samoan songs: You know, the whole cultural thing—that’s what is missing when she goes to the programme . . . she is the only Samoan woman there, there is a Cook Island and a Tokelauan but they are far gone, and nana is very sociable. When she is in her cultural context, she knows what is right and wrong. (Granddaughter caregiver to P8)
Some caregivers shared that their vital support came from talking with friends and families who had also cared for a loved one with dementia: What I found really helpful was just talking to my colleagues who also had parents that they’d looked after who also had dementia and they were Samoan and Māori. (Daughter caregiver to P5)
Participants reported mixed experiences with government-funded or community services. One caregiver’s mother with dementia could spend weekdays at a community programme, while her children were at school and she worked full-time. Others highlighted the cultural and language barriers to engaging with such services. Having a care assistant with the same cultural and ethnic background as the elder was considered very helpful but was inconsistently available: We have had this one carer, Samoan-speaking, and she came in 3 times a day every day and she was amazing, she would keep mum company, they would play cards, you know, and they would sit outside and listen to Samoan radio, they became a companion for mum, but then we moved out here and we had to change providers. The [new service] has a very different way of carers. They don’t have one person coming in and they do not have a Samoan person. They have 3 different people coming in, it was extremely disjointed, and it was just not working for us and her. (Daughter caregiver to P7)
Being able to trust others to care for their loved one was vital to making use of services. For example, a participant with severe dementia had spent 1 day a week at a trusted respite service, which meant his family could take a break. But after he left the service’s premises one time, without supervision, his wife felt she could no longer trust the staff to keep him safe from wandering off, and she stopped using it: Sa ou faatuatuaina outou e vaaia lo’u aiga, ae fai mai e short staff, ae ou fai atu i ai, that is not an excuse, o le mea lena ou te le o toe ave ina i ai lou toalua. (Spouse caregiver to P9) The caregiver trusted the service to look after her husband, but they said they were short-staffed [at the time he left without supervision], and she told them that was not an excuse and the caregiver ceased using this service.
Discussion
Participants in this research showed that there was no single Samoan concept of dementia and its origins. The term dementia does not mean anything in the Samoan language and there is no diagnosis from a Samoan perspective. Older Samoan people interviewed believed that this was not a disease but rather a sign marking the end of one’s purpose in life. Some older Samoans with mild dementia spoke of galogalo, while others used valevale matua. Samoan family members who participated in the research had knowledge and experiences of dementia that were both culturally and socially determined, ranging from Samoan worldviews to mainstream medical diagnoses.
The usual terminology used in NZ is that dementia is an umbrella term for a group of symptoms that are produced by changes in one’s brain (Alzheimers New Zealand, 2017), a definition from within a Western medical paradigm. A mental health practitioner completes standardised cognitive tests and clinical assessments, using Western-validated cognition assessment tools, to diagnose (Ogden et al., 2003). A NZ dementia study with Māori argued that such protocols and tools lack Māori perspectives and are therefore culturally biased and inappropriate (Dudley et al., 2019). The same could be said of using these diagnostic tools with Samoan people. There has been work in the LiDiA project to validate the 10/66 diagnostic dementia tool (Martinez-Ruiz et al., 2022), translated into Samoan and Tongan languages, but the work is incomplete and the validity for assessing Pacific elders unclear (Martinez-Ruiz et al., 2021). Given the increasing number of Pacific elders diagnosed with dementia, there is a need for a Pacific theory of dementia and an appropriate care pathway informed by Pacific worldviews and understanding of mental health (Hughes, 2009).
Where younger Samoan people were diagnosed with dementia, it was more likely to be attributed to psychological trauma, such as the sudden loss of family members, disconnection from familial responsibilities and ongoing stress situations, than to physiological brain changes, in line with Samoan concepts of tausi o aiga (serving or taking care of families) and motusia o mafutaga (breakdown of relationships) (Seiuli, 2013).
Despite the different understandings of dementia within Samoan families, it was evident that once a diagnosis was made, caregivers faced many social and cultural challenges to coping. Most young caregivers spoke of the responsibilities and obligations as their duty of care towards their parents and or grandparents. To fulfil these obligations, some sacrifices were needed around living arrangements and caregiving duties. Similar to a qualitative study on the experience of UK Latin Americans caring for a relative living with dementia, our participants emphasised the importance of fulfilling their familial obligations by providing care (Guerra et al., 2022). A systematic review of published empirical literature by Racine and team (2022) a study by Jacklin et al. (2015) on informed dementia caregiving among Indigenous communities in Ontario, Canada, and results from Williams et al. (2021) on the impact of dementia among American Samoan elders, strongly supported the findings from this study.
Families’ responses to the challenges of caregiving varied. Some reported that they managed to successfully live with the changes in the person with dementia through a coordinated and collaborative care plan. Others struggled with a lack of family support and were more likely to report social, mental, and physical health issues. There were concerns about marriage and relationship breakdowns and depression in the caregivers. Similar to a study of challenges faced by family caregivers in the USA (Strommen et al., 2021), our participants emphasised the financial sacrifices they needed to make and the lack of culturally appropriate services available. The young children and grandchildren assisting caregiving also made tremendous sacrifices, opting to choose between their social life as young people and staying home to help out. Although this duty was considered an important, culturally based obligation to support the main caregiver, there is a possibility of long-term psychological and social impacts on these young people. For example, there can be conflict with the dominant non-Samoan values (that focus on individual rights and freedoms, especially for young people) that need to be well-managed, as research on being caught between cultures (Tiatia & Deverell, 1998, p. 10) has shown.
Dementia support services were under-utilised by the Samoan families we interviewed. Information programmes and respite services did not meet their cultural needs, nor engender trust that these external providers could guarantee to meet the best standards of family-provided care. Similar to a study of home-care provision in the USA (Shaw et al., 2021), our participants emphasised that home-care workers needed to be a fit, providing quality support and meeting their cultural, social, and economic needs. When confronted with services that did not meet these holistic needs, families would disengage and make more sacrifices to accommodate the level of care required.
Implications
This study has important implications for Samoan and other Pacific and minority ethnic groups. Extending this Samoan knowledge base to improve service provision for dementia is essential, as is developing a Samoan theory of dementia, using concepts relevant to Samoan understanding. A more holistic approach to developing assessment tools and protocols for diagnosing dementia, as the LiDiA study is attempting, is clearly needed. Researchers worldwide are emphasising the need for culturally and linguistically appropriate screening tools (Lim et al., 2021), plus dementia information (Huggins et al., 2022) and services for minority ethnic groups (Guerra et al., 2022). For example, findings from a Māori dementia study (Menzies et al., 2021) showed that work embedded in cultural values improved the knowledge and understanding of dementia, known as mate wareware in Māori language, and could usefully inform the assessment of older Māori with cognitive impairment.
Limitations and further research
Having talanoa with Samoan people with dementia and their families, recruited through trusted services and facilitated by a fluent speaker of Samoan and English, has provided a vital glimpse into experiences rarely explored. The limitations of the research are primarily of scale—this was work that was made possible under the umbrella of a larger funded study but limited to its parameters and timeframes. The work was located in a NZ city with many Samoans, but we need to explore if smaller communities have more culturally responsive services. Also, our findings could provide a template for assessing whether other Pacific and minority ethnic populations have similar experiences and needs beyond mainstream services. For example, how is dementia traditionally understood in their languages and cultures? How are medical diagnoses and prognoses understood? How are information and care services engaging with diverse cultures and caregivers of all ages?
Conclusion
Samoans’ worldviews of health, illness, and wellbeing, and their lived experiences of dementia, provide a critical knowledge base that is needed to improve understanding, education, support from services, and management of dementia for Samoans living in NZ. This study of Samoan people with dementia and their caregivers presents experiences and worldviews that have been rarely considered. Pacific people comprise an increasing proportion of NZ’s ageing population, which is increasingly diverse. Dementia assessments and services should incorporate diverse sources of knowledge and experience to better serve Samoan and other Pacific ethnic minority groups.
Footnotes
Acknowledgements
The authors acknowledge all those Samoan families who participated in the talanoa and shared their journey and experiences. They also acknowledge the support from the Pacific community providers for this project.
Authors’ note
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This work was supported by funding from the University of Auckland and the Counties Manukau District Health Board, Auckland New Zealand.
Glossary
galogalo forgetfulness
motusia o mafutaga breakdown of relationships
palagi a concept for a Western person
talanoa interviews using Samoan cultural protocols
tausiga o aiga serving or taking care of families
tautua to serve, service
valevale matua a normal part of ageing, forgetfulness and an end of one’s purpose in life; a concept of getting older and forgetting things
Aotearoa New Zealand
Māori the Indigenous peoples of New Zealand
mate wareware dementia
tohunga healer