
Abstract
First Nations, Inuit, and Métis, Indigenous peoples in Canada, have long experienced racism within health services resulting in a health service system that many Indigenous people in Canada do not want to access. Research informing Indigenous health services must consider how findings and analysis happen within the community, what information is shared, and how it improves access to health services. Information shared in Indigenous research methods was communicated at the end and throughout the project. Indigenous knowledge mobilization in Indigenous research methods requires researchers to receive knowledge from the community and research participants. Also, knowledge sharing and moving into practice happen continuously throughout the research process. These qualities of Indigenous knowledge mobilization facilitate increasing accessibility to health services through Indigenous knowledge identified in research. This article describes an Indigenous knowledge mobilization framework that may be adapted within Indigenous communities looking to make transparent how Indigenous knowledge is incorporated within health services.
Background
Indigenous peoples facing barriers to health services are an example of how a colonial system intersects with Indigenous knowledge and the need to consider Indigenous knowledge mobilization throughout health services. If Indigenous knowledge was present within health services Indigenous people would have ready access to them; recent reports and investigations demonstrate that Indigenous knowledge is not present as systemic racism continues to limit accessibility to health services (Gunn, 2016; Turpel-Lafond & Johnson, 2021). Over the last decade, Indigenous health research practices and the study of knowledge mobilization have grown. Yet there continues to be a lack of information on Indigenous knowledge mobilization and efforts to evaluate them. The purpose of this article is to provide a framework for discussion when considering Indigenous knowledge mobilization and ways to evaluate such efforts. The attention on knowledge mobilization results from needing to make relevant, evidence-based, informed decisions from the ever-expanding bodies of knowledge that are shared. The term knowledge mobilization describes ways of moving knowledge from identification to application. Knowledge mobilization is also known as knowledge exchange or knowledge transfer (Straus et al., 2009). Regardless of terminology, knowledge mobilization seeks to lessen the research-to-practice gap, referring to the failure of research uptake in relevant areas (Bowen & Graham, 2013; Van De Ven & Johnson, 2006). This article demonstrates how knowledge mobilization is realized across Indigenous research methods at an Indigenous community-based health research lab. The article challenges described barriers, identifies new barriers, and shares a framework for adaptation to facilitate effective, culturally safe Indigenous knowledge mobilization in different contexts.
Widely accepted research methods and knowledge mobilization practices have the potential to reproduce colonial ways of knowing and doing (Estey et al., 2010; Smylie et al., 2014). Research methods and knowledge mobilization are intricately connected and applying research paradigms that privilege Eurocentric knowledge reinforces Eurocentric ways, including racialized, gendered, and classist ways (Morrow et al., 2022). That being said, decolonizing research and knowledge mobilization practices are possible when Indigenous people determine how and what research is practiced (Smith, 2012; Tuck, 2013) and how research is mobilized into practice. Indigenous scholars argue that knowledge mobilization strategies with Indigenous peoples must be re-conceptualized and evaluated (Crosschild et al., 2021; Estey et al., 2008, 2009; Hanson & Smylie, 2006; Morton Ninomiya et al., 2022; Ranford & Warry, 2006; Smylie et al., 2014). While the Canadian Institutes of Health Research (CIHR, 2012) distinguishes Indigenous knowledge mobilization from general population integrated and end-of-grant knowledge mobilization approaches, there are no consistent mechanisms or sources for Indigenous communities to hold researchers accountable for adhering to Indigenous knowledge mobilization principles (Morton Ninomiya et al., 2017). This article describes a framework that may be adapted in those spaces looking to inform knowledge mobilization evaluation methods.
Knowledge mobilization and Indigenous research
Knowledge mobilization within Indigenous research contexts requires recognizing the diversity of Indigenous cultures and knowledge systems. Knowledge mobilization must fit within the priorities and ways of knowing identified by Indigenous peoples. Indigenous ways of knowing underpin Indigenous healing practices and must be respected and considered alongside western medicine and research as per the 22nd Truth and Reconciliation Commission of Canada’s (TRC, 2015) Call to Action. Indigenous knowledge mobilization is distinct and needed; however, the question remains of how Indigenous knowledge has been most effectively mobilized in colonized spaces.
There is a long-standing history of deficit-based research being enforced on Indigenous peoples while ignoring Indigenous knowledge (Crosschild et al., 2021; Straus et al., 2011). Using a strengths-based approach, carried out in partnership with community-identified research priorities that seek to benefit the community, is necessary to avoid this deficit-based research and the perpetuation of further colonial harms within research processes (CIHR, 2012; Estey et al., 2009). In an Indigenous Canadian health context, Smylie et al. (2014) reiterate this idea that knowing and doing are intertwined and indistinguishable. Indigenous knowledge mobilization is integrated within these Indigenous systems of knowing and doing. Creating knowledge within these Indigenous practices must be respected and implemented as communities are respectfully engaged within health projects (Estey et al., 2009).
Smylie et al. (2014, p. 17) define Indigenous knowledge mobilization as “Indigenously led sharing of culturally relevant and useful health information and practices to improve Indigenous health status, policy, services, and programs.” However, knowledge mobilization within Indigenous and community-based research is not well documented (Boydell et al., 2012; Estey et al., 2009; Martens et al., 2010; Morton Ninomiya et al., 2020; Ramsden et al., 2017). The documented knowledge mobilization is focused primarily on cultural safety within health services. Cultural safety calls on health care professionals to reflect on personal, institutional, and systemic power imbalances and biases. Reflecting on power imbalances to affect positive change is the ultimate aim of creating a more respectful health care system for all (Ward et al., 2016). Although, reflection on the fact that there are indeed significant power imbalances is only the first step toward creating more respectful systems for change and justice to begin. This need to reflect allows for non-Indigenous people to recognize other worldviews or how others are experiencing the same systems and begin to acknowledge that there is a need for a disruption of systems that benefit them and continue to harm others. Understanding that health care spaces have not incorporated Indigenous knowledge is one example of how power imbalances have privileged other knowledge within spaces that should be informed by Indigenous peoples.
At the Indigenous community-based health research lab, the combined efforts of Indigenous peoples and researchers realize shared goals through Indigenous research methods that blur the lines of traditional knowledge mobilization. In other words, disrupting the largely accepted or westernized ways of knowledge mobilization to recognize that varied worldviews need to be considered in this space. Indigenous research methods and the orientation toward community participatory research frameworks blend knowledge mobilization efforts throughout the research process. Importantly, the uptake of findings beyond those participating in the research introduces questions of ethics and representation across populations. As Indigenous research methods are focused on regional- and people-specific research questions, the following questions arise: (a) How does the application of knowledge from one nation be applied within new spaces elsewhere respectfully? and (b) How are research findings from Indigenous research methods applied in new spaces? These questions are essential considerations for Indigenous knowledge mobilization as they focus on discussion in Indigenous research methods.
The article will describe how Indigenous knowledge mobilization has been conceptualized and operationalized across several different research projects at the Indigenous community-based health research lab. And, it will examine the role of knowledge mobilization efforts during research projects and the outcomes of knowledge mobilization at the end of grants. Throughout this article, Indigenous knowledge mobilization will be demonstrated as distinct from integrated knowledge mobilization. Integrated knowledge mobilization proposes that knowledge mobilization is unidirectional, while the Indigenous community-based health research lab shows that Indigenous knowledge mobilization is multidirectional and upsets the typical hierarchy of knowledge producer and user. The Indigenous community-based health research lab flips western ideas of who is the expert, creating the need for critical reflection on power structures.
Indigenous knowledge mobilization demonstrates the need to reconsider the operationalization of knowledge holder and participant, as Indigenous research methods confront western systems of knowledge mobilization by redefining participants as experts and co-researchers. Indigenizing western systems require changing academic language and policies to respect Indigenous knowledge and those who produce, and share in, the knowledge mobilization efforts. As such, this article challenges the rigidity of westernized knowledge mobilization efforts, offers examples of how Indigenous knowledge mobilization can be realized in a good way, and also offers a flexible framework for others to utilize within Indigenous communities to ensure community-specific reciprocal knowledge mobilization can be realized across disciplines.
Methods
A literature review focused on the most recent research, seeking what is currently known, understood, or agreed upon regarding Indigenous knowledge mobilization while highlighting disagreements within the literature. Other associated terminology was also explored within Indigenous and non-Indigenous service delivery which revealed a significant gap when it comes to how to realize Indigenous knowledge mobilization. To accompany this review, several Indigenous and ally scholars with experience in Indigenous research methodologies and Indigenous knowledge mobilization reviewed knowledge mobilization within Indigenous research at the Indigenous community-based health research lab. To articulate how community partners contribute to Indigenous knowledge mobilization, the authors and Indigenous community-based health research lab staff reviewed five of the lab’s relatively recent and ongoing research projects. Through the review of the literature and knowledge mobilization at the Indigenous community-based health research lab, the authors identified several necessary components to inform the development of an Indigenous knowledge mobilization framework. The researchers and staff described each component thematically to create a framework with shared themes and supportive components.
While many non-Indigenous researchers refer to their collaborators as participants, the Indigenous community-based health research lab terminology co-researcher addresses the inherent power imbalance that generally exists within the roles of researcher and participant. Indigenous community partners, or co-researchers, include various people who play different roles throughout research projects. Generally, Elders and knowledge keepers guide Indigenous community-based health research lab researchers in what is researched and how research is conducted within their communities. Co-researchers who are not Elders or knowledge keepers are often workers in relevant fields, knowledge users, people with lived experience, or community members. Each co-researcher holds expertise and experience that adds significant value to the Indigenous community-based health research lab’s understanding and helps bridge the research-to-practice gap. Co-researchers and community research assistants (RAs) mobilize relevant knowledge to help bridge the research-to-practice gap within their communities and throughout the research process.
Current state of knowledge mobilization
Knowledge mobilization is demonstrably a necessary topic of discussion as Straus et al. (2009) noted that health care services do not respond effectively to new research. The outcomes of poor knowledge mobilization are realized in the well-being of those accessing, or not accessing, health services (LaRocca et al., 2012). Indigenous populations’ health outcomes are partially due to health services discontinuity with Indigenous knowledge and knowledge mobilization.
LaRocca et al. (2012) summarized barriers that disrupt evidence-informed decision-making, including barriers across all levels of health systems, organizations, teams, professions, and clients. Barriers to evidence-informed decision-making across all levels include, but are not limited to: lack of motivation to incorporate new information, lack of evidence, the inability to change standards of practice, lack of personal knowledge, attitude, values, and skill to use evidence, lack of time, and resistance to change impact knowledge mobilization (LaRocca et al., 2012). LaRocca et al. (2012) also note that knowledge mobilization strategies are specific to discipline and sub-disciplines or particular areas of concern and that there is no general knowledge mobilization strategy. Of the knowledge mobilization strategies systematically reviewed by LaRocca et al. (2012), the most effective strategy included organizational change, while the least effective incorporated provider feedback. The reviewed knowledge mobilization strategies spanned various methods, including peer education, workshops, technical assistance, internal and external training opportunities with different levels of interaction, web-based databases, information services, discussion lists, pre-processed knowledge mobilization, and tailored messaging (LaRocca et al., 2012). As a result of the variety of techniques for knowledge mobilization, and the lack of consistency in describing strategies, LaRocca et al. (2012) could not identify a shared method of evaluation across any of the studies reviewed.
The valuable review by LaRocca et al. (2012) identified characteristics of interventions, participants, and organizations that affected knowledge mobilization. Interventions that included tailored messaging and access to online databases of pre-processed knowledge mobilization were more effective than those interventions that just used an online database or paired the databases with a knowledge broker. Participant characteristics also affected knowledge mobilization. Generally, willingness to incorporate research findings did not scale with education level as lower levels of education, 2-year certificate program recipients, had a more willingness than those with higher levels of education (LaRocca et al., 2012). That being said, some professions like nurses with higher levels of education were more likely to include research than doctors with similar levels of education.
The reviewed strategies showed that tailored messaging was the most effective strategy across all education levels. Tailored messaging includes making sure the message is relevant and applicable to the intended audience (Dobbins et al., 2009). The type of change resulting from the research also affected the uptake of knowledge mobilization, with simple behaviors more readily adopted than complex behaviors (Forsetlund et al., 2009). Interventions inclusive of active engagement were more successful, while passive interventions also found an important role in specific contexts (LaRocca et al., 2012).
Organizations that could apply knowledge mobilization had a research-based culture where policymakers were employed (Morton Ninomiya et al., 2020). Meijers et al. (2006) found a relationship between research use and the role of the knowledge user, access to resources, organizational climate, support, time for research activities, and provision of education. Knowledge mobilization must address existing barriers to the uptake of research into practice. One attempt at improving knowledge mobilization is to include those who are using the knowledge in the research. This inclusion is meant to integrate knowledge production with knowledge mobilization.
Integrated knowledge mobilization is an approach to research within western-informed knowledge systems where researchers and research users collaborate throughout research from development to dissemination (CIHR, 2012). Integrated knowledge mobilization aims to engage key stakeholders and target audiences throughout the research life cycle with the motivation of stakeholder investment in research results, inevitably increasing the potential uptake of research findings (Morton Ninomiya et al., 2020). Integrated knowledge mobilization is a fundamental methodological approach within Indigenous health research because of its ability to act as an interface between two distinct ways of knowing that often seem in opposition (Estey et al., 2009; Sherwood & Edwards, 2006; Smylie et al., 2004, 2009). With integrated knowledge mobilization, both the knowledge user and the research partners bring valuable expertise to the research processes. Tobias and Richmond (2016) further explain that integrated knowledge mobilization is a transformative method that nurtures the emergence of research environments wherein all collaborators can benefit from the experience of applying research in ways in which they may have had little experience. In contrast, end-of-grant knowledge mobilization is a process in which research findings are analyzed and disseminated to knowledge users. End-of-grant knowledge mobilization ranges from publications to tailored messages for target audiences and commercialization.
Indigenous knowledge mobilization
Neither integrated knowledge mobilization nor end-of-grant knowledge mobilization completely meets the needs of Indigenous communities when it comes to bridging the knowledge and research-to-practice gap. Integrated knowledge mobilization acknowledges both the user and research partners as having expertise in the research processes; however, it doesn’t acknowledge the multidirectional knowledge mobilization between researcher and knowledge user that is a requisite of appropriate and culturally safe knowledge mobilization. While end-of-grant knowledge mobilization is an effective practice and has become the expected norm, it certainly should not be the only knowledge mobilization in research with Indigenous peoples. Increasing and ensuring continued engagement throughout a multiple-year project make it imperative to have knowledge mobilization throughout.
Indigenous ways of sharing knowledge are deeply embedded within their knowledge systems (Bendall et al., 2016; Smylie et al., 2014; Tobias & Richmond, 2016). Indigenous research methods are simultaneously inclusive of knowledge mobilization via the nature of the research and the construction of the research process. Creating and sharing knowledge are intrinsic to each other in the Indigenous research process, incorporating those that are necessary to formulate the questions, methods, analysis, and discussion (Bourassa et al., 2021).
Estey et al. (2010) suggest four essential activities for researchers in the context of planning knowledge mobilization with Indigenous peoples across Canada: (a) clarify what knowledge mobilization means to both Indigenous communities and researchers; (b) acknowledge past negative research experiences between Indigenous research participants and researchers and discuss how future negative experiences can be mitigated; (c) reach consensus on what doing knowledge mobilization will look like for the project; and (d) discuss and agree on stakeholder roles and responsibilities in knowledge mobilization activities. These are all imperative actions and should be foundational to all efforts toward Indigenous knowledge mobilization.
Cooper and Driedger (2018) propose seven questions to consider when creating valuable and relevant knowledge mobilization products:
Can the community easily make copies of the resource?
Are there aspects of the product which do not require any written literacy skills?
Is there a component of the message which is strengths-based and hopeful?
Is the product interactive?
Has the knowledge from participants and communities been acknowledged?
Is there an active learning component that spans beyond encounters with the research team?
Has the product been returned to the community quickly (preferably under 6 weeks)?
Smylie et al. (2009) explain that seeking understanding and including local processes of knowledge creation, dissemination, and utilization are prerequisites to designing and implementing knowledge mobilization with Indigenous communities. Smylie et al. (2014) expand on this by identifying contextual issues for knowledge mobilization in Indigenous contexts, including cultural safety; health literacy; protection of Indigenous knowledge; underlying unmet material, health, and social needs; publication bias; reciprocity; and location. Scholarship in Indigenous health research suggests that having champions and engaging influential stakeholders make research credible and valuable to communities (Ranford & Warry, 2006; Smith, 2012; Smylie, 2011).
From the literature review, both Cooper and Driedger (2018) and Estey et al. (2010) provide foundational considerations; however, the authors argue that neither are exhaustive and are missing key considerations that are required to ensure Indigenous knowledge mobilization is effective. Estey et al. (2010) list the first of four essential activities for researchers is to clarify what knowledge mobilization means to both the Indigenous communities and researchers; however, the authors would pose that this, as well as privileging the Indigenous communities’ realization of knowledge mobilization, is key to successful Indigenous knowledge mobilization. At the Indigenous community-based health research lab, Indigenous knowledge mobilization occurs within local languages, conceptualizations, ways of knowing and doing, and how these are realized. Researchers’ knowledge mobilization needs to be ethical using a community-driven approach to create and identify knowledge and mobilize it to the community.
Knowledge mobilization at an Indigenous community-based health research lab
Understanding and including local knowledge creation, dissemination, and utilization are prerequisites to designing and implementing knowledge mobilization (Smylie et al., 2009). At the Indigenous community-based health research lab, a mentorship model facilitates capacity building and multidirectional learning by rejecting the hierarchical relationships typical to the research environment (Karnieli-Miller et al., 2009). The Indigenous community-based health research lab privileges the voices of community members by establishing Community Research Advisory Committees (CRACs). The Indigenous communities set the requirements for CRAC membership. Once verified, CRAC members become active directors of research design, implementation, dissemination, and mobilization. Knowledge mobilization differs within each project and community as knowledge mobilization follows community lead and need.
The Indigenous community-based health research lab prides itself in the authentic relationships we engender as our mandate to the foundation for ethical research with our partners. The Indigenous community-based health research lab relies on transparency and opens discussion throughout the research process to build relationships and ensure ethical investigation and knowledge mobilization. The lab also engages in cultural practices and acknowledges many ways of knowing and doing, ensuring that we help create a safe space for working with Indigenous peoples toward their various priorities and visions.
As community members hold invaluable expertise, the hierarchical relationship that is typical to research is entirely inappropriate. Therefore, the Indigenous community-based health research lab employs a mentorship model that resists hierarchies, promotes cultural safety, and creates a space optimized for multidirectional learning. At the very foundation of how the Indigenous community-based health research lab works, the CRAC members and participants are all referred to as co-researchers to challenge the power imbalance that occurs within the researcher, participant, or expert knowledge user language of western research.
The Indigenous community-based health research lab’s significant amount of time learning about community history, protocols, and ceremonies helps improve cultural safety and relationship authenticity. While the individual ultimately determines cultural safety, the lab has considerable experience building safe, reciprocal, and beneficial relationships with a wide range of Indigenous communities, organizations, and peoples. Indigenous community-based health research lab’s mentorship model’s ability to rebalance power relations promotes cultural safety while forcing researchers to reflect on their positionality.
At the Indigenous community-based health research lab, CRACs formulate research priorities and questions. CRAC members are often far more aware than researchers of potential concerns regarding health literacy. As a result, previous CRAC input has addressed health literacy by requesting knowledge be presented orally, visually, in traditional Indigenous languages, through storytelling, and in various other mediums. CRAC members, such as Elders, are skilled communicators, and their guidance and support help research overcome barriers relating to personal knowledge, attitude, values, and skills. By having knowledge production defined and led by Indigenous peoples research is underpinned by local Indigenous worldviews. Research with CRACs adheres to Indigenous ways of knowing, doing, and knowledge mobilization as described by Jull, Giles, and Graham (2017) who asserted that Indigenous knowledge mobilization is an approach to knowledge sharing defined and led by Indigenous peoples involved in research and is, therefore, underpinned by local First Nation, Inuit, or Métis, Indigenous peoples of Canada, worldviews.
Indigenous research methods focus on regional- and people-specific research questions. As a result, applying Indigenous research outcomes in communities where they did not emerge creates an ethical problem. While Indigenous peoples and communities are far from homogeneous, some specific experiences and values are shared by many (Reading & Wien, 2009). Shared experiences like colonialism, racism, and cultural disruption may extend to shared experiences of the relevance of research outcomes. Therefore, research must be adapted, not applied, to new contexts.
Table 1 shows what knowledge mobilization the Indigenous community-based health research lab and the partnering CRACs have produced and how it differs according to community relevance across projects while being a consistent presence throughout the research process as guided by the CRAC members.
Knowledge mobilization in Indigenous research, case examples from the Indigenous community-based health research lab.
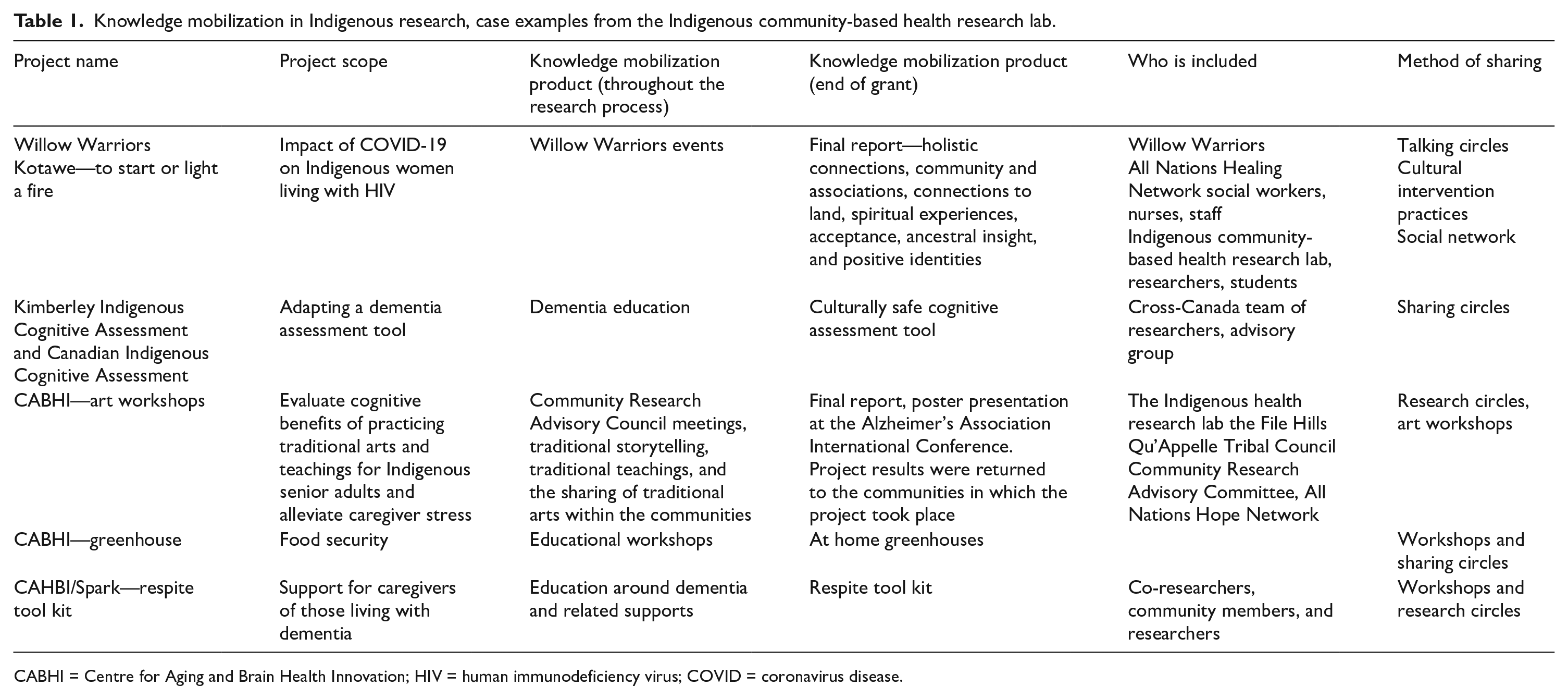
CABHI = Centre for Aging and Brain Health Innovation; HIV = human immunodeficiency virus; COVID = coronavirus disease.
Each of the projects in Table 1 occurred in response to the lab’s community partner concerns and was responsive throughout the projects to the communities’ needs in regard to knowledge mobilization needs and expectations. Kotawe (to start or light a fire) is a project the lab did in support of Indigenous women who were experiencing varied effects of human immunodeficiency virus (HIV). The Kimberley Indigenous Cognitive Assessment (KICA) and Canadian Indigenous Cognitive Assessment (CICA) work began in north western Australia and originally was called KICA looking at culturally appropriate cognitive assessment for Indigenous older adults and was adapted with Indigenous communities in Canada and renamed CICA. The Centre for Aging and Brain Health Innovation (CABHI) Spark art workshops work was developed in response to concerns about increased cognitive delay being experienced by partnering communities’ older adults. The CABHI Spark greenhouse work was developed in response to concerns around food security and food prices in rural and remote partnering communities. The CABHI Spark Toolkit work was developed in response to concerns raised in partnering communities by caregivers of older adults experiencing cognitive delays.
One contextual barrier for knowledge mobilization in Indigenous contexts, identified by Smylie et al. (2014), is the protection of Indigenous knowledge(s). Work at the Indigenous community-based health research lab adheres to the principles of ownership, control, access, and possession (First Nation Information Governance Centre, 2011) and the collective benefit; authority to control; responsibility; ethics; and findable, accessible, interoperable, and reusable principles (Research Data Alliance International Indigenous Data Sovereignty Interest Group, 2019). Unless otherwise requested by communities, this ensures that ownership of data rests with Indigenous communities, who retain control and enforce their own protocols for its access and possession (Schnarch, 2004).
The Indigenous community-based health research lab considers any products derived from research in Indigenous communities as belonging to those communities. Therefore, when presenting research to academia, it is only logical that the research owners are included in whatever capacity they desire, including where and how information is shared. Research owners often prefer working in an advisory role. The team at the Indigenous community-based health research lab will format research in a manner that satisfies the needs of academic journals, while research owners will review article drafts and provide feedback. This process reduces the potentially erroneous influence of researcher bias.
When research is presented at conferences, having research owners present findings has produced overwhelming results. There is already recognition of the need to increase the number of Indigenous peoples in academia (TRC, 2015), indicating the importance of research capacity building. Indigenous research owners are integral to all of the Indigenous community-based health research lab’s knowledge mobilization processes. The following quote from a CRAC member, regarding her experience at an AGE-Well Annual Conference demonstrates just how overwhelming academic interest can be: The conference participants were very receptive, asking many questions . . . . We were the only First Nations group involved in the dementia research. People just flocked around us afterward, asking questions about our current research projects. And just on and on, I couldn’t even get to go to any other people speaking, because we had a lot of comments and they really enjoyed our presentation. It was great. (R. McKay, Personal communication, October 9, 2019)
The work presented in Table 1 is expanded here to further describe the various Indigenous knowledge mobilization processes as led by each of the leading communities.
KICA tool adaptation into Canadian Context: Multi-directional knowledge mobilization—The Australian (KICA) was adapted into the Canadian context and renamed as the CICA tool. Partnering academics and many Indigenous community-based health research lab RAs were part of the transdisciplinary CICA team tasked with developing a culturally appropriate dementia screening tool for Indigenous adults in the Northern Ontario, Canada, Anishinaabe First Nation community (Jacklin et al., 2020). The CICA team began the process in conversation with community advisors. There are many differences between Kimberley Indigenous peoples in Australia and the Anishinaabe people of Northern Ontario, Canada; however, commonalities were leveraged to benefit all parties involved.
Before piloting the adapted tool, there were nearly 2 years of iterative monthly consultation between an expert Anishinaabe language group and researchers, with ad hoc consultations with an Indigenous Elder, community advisory council, and the KICA authors (Jacklin et al., 2020). During this process, every item of the KICA required varying degrees of modification to account for Anishinaabe culture, language, and history (Jacklin et al., 2020). The adaptation process demonstrates that throughout a research process, Indigenous knowledge mobilization is multidirectional.
Research must include local contexts. Within the local contexts of different Indigenous communities, local expertise, shared experiences, and preferences can and do differ. Combining researcher skills with community expertise requires continuous and multidirectional knowledge mobilization throughout the research process. While developed in other contexts, previous research can provide a strong base from which local adaptation can begin.
Kotawe and the Willow Warriors: individual-level knowledge mobilization at an Indigenous community-based health research lab
The Willow Warriors (WWs) are women living with HIV in Regina, Saskatchewan, Canada, who receive support and programming from the All Nations Hope Network (ANHN). An Indigenous community-based health research lab RA works with ANHN and the WWs to support the research and ensure the investigation is led by community needs. A most recent example of this work occurred during COVID-19. The RA and ANHN sought to better understand the impact of COVID-19 on Indigenous women living with HIV in Regina and further support them through this unprecedented time. To do this, researchers and WWs participated in sharing circles. Sharing circles eliminate power imbalances between researchers and participants by making all members joined in the circle as equals (Lavallée, 2009). Sharing circles align well with the Indigenous community-based health research lab’s assertion that community members are experts and co-researchers, and, as a result, a hierarchical researcher–participant relationship is inappropriate and avoided. Furthermore, sharing circles minimize researcher influence over what is shared, resulting in potentially unexpected, and in this case, highly valuable, results. Most important of these results was that the researchers and WWs were effective in mobilizing knowledge that proved beneficial to WW health and well-being. The eagerness to accept culturally based teachings and the positive results that followed suggest that connection to culture is beneficial and desired among WWs. Kotawe provides evidence that successful knowledge mobilization is likely to follow when research is guided by those Indigenous peoples with lived experience that it is intended to benefit.
A surprising finding of the sharing circles was that the teachings are mobilized beyond the group receiving the intervention. Specifically, WWs spoke of bringing teachings back to their home and community fires. Home fires and community fires refer to their loved ones and support networks within these spaces. When culture is incorporated into interventions or research, as is the case with the research approach at the Indigenous community-based health research lab, the end product is eagerly accepted and, potentially, disseminated throughout social networks. Examining and articulating the specific aspects of the work that influenced this external sharing of knowledge would represent a significant academic contribution within the field of Indigenous knowledge mobilization.
CABHI Sparks projects: community motivation and resilience toward prioritized knowledge mobilization
While each CABHI Sparks Project dementia caregivers’ respite tool kit, greenhouse, and art workshops was significantly affected by COVID-19, each continued to varying degrees under the guidance of community. The CRAC members insisted that each of these projects continues due to their importance to community health and well-being, especially during the uncertainty of COVID-19. Together with Indigenous community-based health research lab RAs, the CRAC members thought of innovative ways to continue the work; for instance, CRAC members took on much of the community recruitment as Indigenous community-based health research lab RAs were restricted from entering communities during the pandemic. These creative, resilient, and motivated communities show the level of buy-in by communities when the work is initiated by them and relevant to the communities’ needs, further suggesting the importance of community-led research.
Indigenous knowledge mobilization framework
The literature review and knowledge mobilization teachings produced through various community-led Indigenous community-based health research lab projects allowed for the development of this Indigenous knowledge mobilization framework. Each component of the framework can be described as a pillar or lodgepole. Each pillar holds up, and is foundational to, sacred spaces for Indigenous peoples. The shared themes included context, content, and relationships. Each theme has many components to support the themes. Realizing each component within each theme enhances knowledge mobilization within Indigenous health services.
The framework has qualities shared across each theme; for instance, the framework must be fluid, be relevant, be reciprocal, and focus on required end-of-grant knowledge. The Indigenous knowledge mobilization framework describes the ability to focus and refocus on emerging issues and shifting priorities; it is adaptable and fluid, with the funder-required end-of-grant knowledge always in focus as well.
The Indigenous knowledge mobilization framework also must consider boundaries, capacity, scope, and skill set. As noted by Smylie et al. (2014), content-specific considerations must also be made in Indigenous knowledge mobilization. Content considerations that have been described by Smylie (2011) are apparent in the Indigenous knowledge mobilization framework include:
Boundaries—roles of those included in knowledge mobilization, how do they use information or knowledge,
Capacity—the human and material resources within the community available for appropriate knowledge mobilization to be realized,
Scope—what can be done within the spaces the knowledge mobilization is happening describes what is being acted upon, and
Skill set and training—how is the information used and by whom, knowing each person’s contribution to the project and how they can use the information.
Relationships are the core of the Indigenous knowledge mobilization framework and require specific actions to realize Indigenous knowledge mobilization. These actions include:
Engagement principles—describe what knowledge mobilization is for each stakeholder, what are the terms of reference, how is a safe place created,
Reciprocity—each stakeholder is suitably contributing, investing in the project, and receiving benefits of the project,
Co-creation—each stakeholder is invested in and contributing during the project and is engaged in knowledge mobilization efforts, co-creating from the beginning of identifying the need to the mobilizing of knowledge,
Power relations—acknowledge power relations, history of relations, how knowledge was produced in the past, and
People specific—inclusive and specific to First Nations, Inuit, and Métis.
While building these relationships it is imperative to ensure reciprocity while also ensuring community expertise is prioritized for knowledge mobilization to be effective. Knowledge mobilization also needs to be a space of transparency to acknowledge past negative research experiences and discuss how similar experiences can be mitigated. In addition, an agreement on stakeholder roles and responsibilities in knowledge mobilization activities is imperative for everyone to feel confident in their roles and expectations.
While we offer an Indigenous knowledge mobilization framework, we do not assume that a single model or framework of Indigenous knowledge mobilization is appropriate for every context; therefore, we have also defined criteria for models to realize so that they can be adapted in new spaces:
Robust—the framework does, or intends to, move evidence to practice and can be described in practical ways,
Measurable—has a method of evaluation and can demonstrate evidence to practice, and
Flexible—can adapt to ever-changing situations and circumstances
Discussion
The level of community involvement demonstrated by the Indigenous community-based health research lab guarantees community ownership and, therefore, increases community motivation to incorporate research results (Morton Ninomiya et al., 2017) and be significantly involved in knowledge mobilization. The four knowledge mobilization examples show how effective knowledge mobilization is realized when communities have control and ownership over the research affecting their lives. However, these examples of knowledge mobilization are certainly more generalizable to other fields, other than health that the research lab is based within. The examples shared are indicative of the various ways in which Indigenous knowledge mobilization is realized when community ownership and voices are prioritized. Community ownership lends to greater uptake of research results (Morton Ninomiya et al., 2017), benefiting both communities and researchers. Greater uptake of evidence-based information can support communities to develop more effective services and programming. Also, the reciprocal learning of the researchers to understand a different worldview and how knowledge mobilization can be realized in various communities allows for growth and depth in their professional development.
In reviewing the knowledge mobilization processes and products the Indigenous community-based health research lab and their community partners based in Treaty 4 and 5 territories in Canada have utilized, we have developed a framework and criteria for Indigenous knowledge mobilization in various Indigenous communities globally. The framework itself is flexible and fluid as we propose that it can be helpful in multiple contexts, across many fields of work. Still, we also do not assume to know all Indigenous contexts and so chose to include criteria to be used, with community’s lead, for appropriate and culturally safe Indigenous knowledge mobilization. With individual communities’ leading or co-leading efforts of Indigenous knowledge mobilization, their community needs and priorities can be directly addressed, ensuring an anti-pan-Indigenous approach. This integrated engagement of community leadership within the work also allow for the flexibility of the Indigenous knowledge mobilization framework to be utilized to its fullest potential as they work with the teams to adapt it to these community needs and priorities.
Future research requires a systematic review of knowledge mobilization efforts in cultural safety, asking such questions as: How do they include tailored messaging? What was the most effective strategy across all education levels? Tailored messaging includes making sure the message is relevant and applicable to the intended audience; and How has relevance and applicability been measured or realized? More detailed documentation of knowledge mobilization efforts and measurements is required, similarly to the detailed work of Morton Ninomiya et al. (2022) or Brinckley et al. (2022). To measure the effect of knowledge mobilization or identify measures a more thorough review of programs and publications must be completed looking specifically for measures of knowledge mobilization in Indigenous communities.
Decolonizing knowledge mobilization
Through Indigenous knowledge mobilization, we aim to disrupt the ideas of knowledge mobilization created in colonial research methods and bring forward Indigenous understandings to the concept of knowledge mobilization in health research. Mainly, we center our discussion around the broader context of situating Indigenous knowledge within scientific discourse. Several distinctions exist between Indigenous knowledge mobilization and western knowledge mobilization. Unlike western knowledge mobilization approaches such as integrated knowledge mobilization or end-of-grant knowledge mobilization, Indigenous knowledge mobilization is rooted in the understanding that knowledge gained from Indigenous communities belongs to the community.
Conclusions
Indigenous knowledge mobilization is the acknowledgment that knowledge mobilization must be based on Indigenous knowledge and worldviews. George Dei observed that we could not talk about decolonization without talking about Indigenous knowledge (Tłıchǫ Research and Training Institute, 2015). Therefore, the process of knowledge mobilization must be led by Indigenous peoples and centered on Indigenous knowledge. There also needs to be an appreciation that different pieces of knowledge bring their unique knowledge-sharing systems. Indigenous ways of sharing knowledge are deeply embedded within the systems that create the knowledge (Bendall et al., 2016; Smylie et al., 2014; Tobias & Richmond, 2016). As these systems can vary, respecting them through the process of sharing knowledge resists continuing colonial practices of adopting a pan-Indigenous approach to research and knowledge mobilization. The colonial practice of adopting a pan-Indigenous approach to Indigenous issues ignores the heterogeneity of Indigenous peoples, silencing individual voices and weakening knowledge mobilization efforts. As an example, for communities that value oral communication as a learning method and to avoid pan-Indigenous approaches, providing tools from which people can talk about critical concepts rather than distributing written materials is vital in breaking down barriers to utilizing dissemination products, regardless of literacy.
Therefore, the key to Indigenous knowledge mobilization is the acknowledgment of differences in ways to mobilize knowledge. Knowledge mobilization is an ethical consideration in Indigenous knowledge mobilization—Indigenous ways of knowing and being are honored in Indigenous knowledge mobilization. Particularly, orality and reciprocity are valued, community members, knowledge keepers, and Elders are held as experts, knowledge sharing is fluid, and messaging is strengths-based. In conclusion, we argue that Indigenous knowledge mobilization must be centered in such a way to resist and decolonize the hegemonic practices of knowledge mobilization. We write this article in hope that the framework and examples offered throughout this article allow for others who seek to resist colonized ways of doing and being to consider Indigenous knowledge mobilization in a more practical instead of abstract way.
Footnotes
Acknowledgements
The authors acknowledge the community partners that made the work possible and led and co-developed the various types of Indigenous knowledge mobilization listed in ![]() ; File Hills Qu’Appelle Tribal Council (FHQTC) Communities, Cumberland House Métis Settlement, Regina Urban Indigenous community, All Nations Hope Network, and Anishinaabe communities in Ontario. They also acknowledge the academic partners and research teams from across Canada with whom they have collaborated. Also, sincere, heartfelt acknowledgements to their own research team leads, Miranda Keewatin, Marlin Legare, Mikayla Hagel, and Peyton Juhnke, who work hard every day to prioritize Indigenous voices and priorities in the research space. They also acknowledge the various funders of these projects, Centre for Aging and Brain Health Innovation, Canadian Consortium on Neurodegeneration in Aging, and Canadian Institutes of Health Research.
; File Hills Qu’Appelle Tribal Council (FHQTC) Communities, Cumberland House Métis Settlement, Regina Urban Indigenous community, All Nations Hope Network, and Anishinaabe communities in Ontario. They also acknowledge the academic partners and research teams from across Canada with whom they have collaborated. Also, sincere, heartfelt acknowledgements to their own research team leads, Miranda Keewatin, Marlin Legare, Mikayla Hagel, and Peyton Juhnke, who work hard every day to prioritize Indigenous voices and priorities in the research space. They also acknowledge the various funders of these projects, Centre for Aging and Brain Health Innovation, Canadian Consortium on Neurodegeneration in Aging, and Canadian Institutes of Health Research.
Authors’ note
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors received no financial support for the research, authorship, and publication of this article.
Glossary
Anishinaabe a group of First Nations in Canada
Inuit an Indigenous people in Canada
Kotawe to start or light a fire
Métis an Indigenous people in Canada