
Abstract
This article describes a peer-led intervention called the Sexy Health Carnival (SHC) that takes a strengths-based approach to promoting Indigenous youth sexual health in a culturally safe context. Expanding on an Ontario pilot study, a group of Indigenous youth leaders went to 11 Indigenous gatherings across Turtle Island, also known as North America, from 2017 to 2020 where they administered an offline iPad survey to 150 Indigenous youth (aged 16–25 years) who engaged with the SHC. The survey gathered descriptive data on HIV prevention behaviors and intentions, and the acceptability of the SHC approach within Indigenous community gatherings. Results demonstrate that doing Indigenous peer-led sexual health and HIV outreach through the SHC is well received among Indigenous youth. Indigenous youth are capable of reaching their peers and developing successful sexual health outreach and HIV prevention resources for each other.
Gatherings within and among Indigenous communities are important sites for cultural retention and intergenerational knowledge transfer (Kaplan-Myrth & Smylie, 2006). While local customs and protocols for gathering vary, they are widely understood as a time to celebrate, reclaim, and maintain local traditions and ceremonies (Monchalin et al., 2016). Often, gatherings are opportunities to be with family and friends across multiple generations and to connect with a diversity of Nations. This collective experience can promote health and healing by reinforcing kinship roles within Indigenous communities (Beaufils, 2022; Sylliboy et al., 2021). There is a wide diversity of both size and purpose of gatherings within First Nation, Inuit (Indigenous Peoples of the Arctic region in Canada), and Métis (descendants of early-17th-century fur trade relationships between First Nations communities and European fur traders in Canada) communities, examples of this include the social and cultural celebration of a powwow, Inuit games, and Métis festivals (DesJarlait, 1997; Giroux, 2016; Hoefnagels, 2007; Puvirnituq Snow Festival, n.d.). At larger gatherings, people from all over Turtle Island, also known as North America, participate and this presents unique opportunities for knowledge transfer, celebration, and nation building (Jones et al., 2020).
Recognizing the important role that congregating plays in cultural continuity, the Potlatch Law 1885 was implemented by the Canadian settler government from 1885 to 1951 which outlawed Indigenous community gatherings (Cole & Chaikin, 1992; U’mista Cultural Society, 2023). According to Wilson and Nelson-Moody (2019), the Potlach can be considered a forum, bringing together Indigenous Peoples for economic, social, educational, or political reasons, to bear witness to the business taking place during these events. While the Potlach is unique to Indigenous Peoples of the Northwest Coast and parts of the interior western subarctic (Gadacz, 2019), the Potlatch Law 1885 was also applied to limit other gatherings and ceremonies such as Sun Dance, a common gathering among Indigenous communities of the Plains (Gadacz, 2022; Monchalin, 2016). This law, coupled with a myriad of settler colonial policies that implemented Indian hospitals, residential schools, and the ongoing overrepresentation of Indigenous children in the Canadian child welfare system (Allan & Smylie, 2015; Boyer, 2019; Monchalin, 2016), fractured the intergenerational transfer of cultural, ceremonial, and traditional knowledge. This cleft has had lasting detrimental impacts on cultural understandings of sexual health and well-being within Indigenous communities, including respect for sexual and gender diversity (Hackett et al., 2021). Coupled with inequitable access to the social and structural determinants of health (Reading, 2018; Smylie & Firestone, 2015), Indigenous young people in Canada are particularly vulnerable to the HIV, AIDS, sexually transmitted and blood-borne infections (STBBIs), and other poor sexual health outcomes (Public Health Agency of Canada, 2018).
In an effort to reclaim teachings around our bodies, while recognizing the overrepresentation of sexually transmitted infections (STIs) among Indigenous youth, this article describes a peer-led intervention called the Sexy Health Carnival (SHC).
Background
The SHC was created by Native Youth Sexual Health Network (NYSHN) youth facilitator Alexa Lesperance, with the help of her community, Naotkamegwanning First Nation, and support from the NYSHN team. It was developed to break down barriers of fear, stigma, and shame related to topics around sexual health. The SHC takes a strengths-based approach to promoting Indigenous youth sexual health in a culturally safe context. It offers accessible materials to make learning health information more fun. The approach has proven successful at engaging youth, community members, parents, grandparents, and Elders at dozens of community gatherings (Lesperance, 2016; Monchalin et al., 2016; Native Youth Sexual Health Network, et al., 2023).
The SHC consists of a collection of informative and well-designed booths and interactive games. The booths include topics such as (a) harm reduction; (b) relationships, bodies, and consent; (c) HIV and AIDS; (d) self-pleasure; (e) moon time and menstruation; (f) choice, justice, and birth control; (g) family planning; and (h) Two-Spirit and lesbian, gay, bisexual, transgender, queer, questioning, intersex, and asexual. The interactive SHC games include dart balloons, a bean bag toss, wheel of sex trivia, sex-positive button making, an HIV prevention guessing game, photo booth, steps to putting on a condom, and many more. The SHC is also packed with prizes, culturally safe information, and safer sex supplies, as well as age-appropriate activities (Native Youth Sexual Health Network, 2014). The term carnival was chosen intentionally: by playfully conjuring up images of a traveling circus, it reminds us that learning about our bodies can be entertaining and the teachings can be taken on the road. While Indigenous people have historically been made part of cruel and exploitative circus sideshows, this version allows us to be in control of our own stories, bodies, and narratives.
Recognizing that large gatherings create opportunities for youth to meet, mingle, and celebrate while simultaneously creating a potential atmosphere for STI transmission, the SHC was first piloted at four pow wows in Ontario in 2014. One hundred fifty-four Indigenous youth between the ages of 16 and 25 engaged in the SHC evaluation pilot survey. Survey results from the SHC pilot project highlighted how the carnival was welcomed by Indigenous youth in powwow settings and that culture is fundamental to sexual health education. Youth respondents indicated that a lot of sex and drug use was taking place at the powwows, and that these cultural gatherings are an important place to discuss sexual health and HIV. Furthermore, youth reported the intention of using condoms acquired at the SHC, suggesting that the SHC holds promise in increasing access to safer sex resources.
Based on the successful uptake of the SHC pilot project in Ontario, NYSHN and a research team at York University applied for and received a grant from the Canadian Institutes of Health Research to take the SHC to other Indigenous gatherings across Turtle Island. The goal of bringing the SHC across the country was to understand the landscape, feasibility, and readiness of Indigenous communities to incorporate HIV prevention content into cultural spaces. This article reports on the survey results from the 11 communities, including presenting data from youth’s HIV prevention behaviors and intentions, and their perspectives on the acceptability of the SHC within diverse Indigenous gathering spaces.
Methods
The SHC applied a decolonizing methodological praxis to both explore and promote Indigenous youth sexual health in a culturally safe context. Linda Tuhiwai Smith (1999) shares that decolonizing approaches are about “centering our concerns and worldviews and coming to know and understand theory and research from our own perspectives and for our own purposes” (p. 39). Leanne Simpson (2011) writes about the concept: Biiskaabiyaang, which translates as the need to look back and to carry forward knowledge. Biiskaabiyaang is defined as “returning to ourselves” (Simpson, 2011, p. 49) and returning to our own knowledge systems. Simpson (2011) indicates that Indigenous researchers are using the term biiskaabiyaang in the same way as the term “decolonizing – [meaning] to pick up the things we were forced to leave behind . . . and bring them into existence in the future” (pp. 49–50). In an effort to reclaim intergenerational knowledges surrounding sexual health and well-being that became fractured through colonial law and policy, a group of Indigenous youth leaders brought the SHC to 11 diverse Indigenous gatherings in Ontario, Manitoba, Alberta, British Columbia, Saskatchewan, and Nunavut from 2017 to 2020. Six gatherings were First Nations-specific, three were Métis-specific, and two were Inuit-specific. The events were an average of 2 to 3 days each and the interactive games were modified to be culturally relevant for the local context. Approximately four to eight Indigenous youth leaders attended each gathering to facilitate the SHC. SHC facilitators included core NYSHN staff and trained Indigenous youth from the surrounding areas.
Data collection was conducted by youth facilitators administering offline iPad surveys during the SHC using QuickTap Survey software. The survey was developed by Indigenous youth leaders, with support from NYSHN staff, academic researchers, and the National Indigenous Youth Council on HIV/AIDS (NIYCHA). Surveys included the original 18 questions that were used in the Ontario pilot study (Monchalin et al., 2016), with an added 36 questions that went into greater detail to better understand HIV prevention behaviors and intentions and sexual health among Indigenous youth. The survey took youth participants an average of 12 to 15 min to complete and queried within six major areas of interest: (a) experience of satisfaction and comfort with the SHC and willingness to return; (b) perceived suitability of doing HIV prevention outreach with youth at cultural gatherings; (c) intention to engage in any sexual practices and or drug use at the powwow; (d) intention to use harm reduction supplies, such as condoms; (e) history of sexual practices and drug use; and (f) sociodemographic information.
Recruitment was done through facilitators asking youth who approached the SHC if they fit inclusion criteria. Inclusion criteria included youth being 16 to 25 years old, able to speak and understand English, self-identified as Indigenous, and engaged with the SHC games and booths for a minimum of 5 min. Where literacy or comprehension assistance was needed, one of the youth leaders would provide support. Informed consent was obtained before youth started the survey. Facilitators provided each participant with detailed project information, including a 1-page contact information of the project leaders and York University ethics board. Youth facilitators went through each detail with participants and answered any questions they had before giving them the iPad survey. Participants received a $10.00 gift card as an honorarium for completing the survey.
Ethics approval was received from York University and NIYCHA advised on all project aspects. In addition, NYSHN and the research team consulted with relevant leadership in each community prior to initiating data collection. Survey responses were exported to R version 4.0.3. Frequencies and proportions for the following variables were examined: sociodemographic characteristics, including gender, age, geography, sexual orientation, and Nation; experiences of participants based on gender and sexuality; satisfaction with the SHC; HIV prevention behaviors and intentions; and community perceptions of the SHC.
Results
More than 1,000 youth engaged in the SHC activities, and 150 eligible youth filled out the survey (Table 1). Many of the youth who engaged with the SHC did not complete the survey because (a) they were not eligible as they were below 16 years of age, above 25 years of age, or did not self-identify as Indigenous, or (b) they did not want to fill out the survey—a minority. Others did not get an opportunity to fill out the survey because iPads or facilitators were unavailable when they interacted with the carnival. Some data were lost when a subset of password-protected iPads went missing before responses could be uploaded.
Demographics for survey participants, N = 150 (ages = 16–25, M = 18.7 years old, SD = 2.8 years).
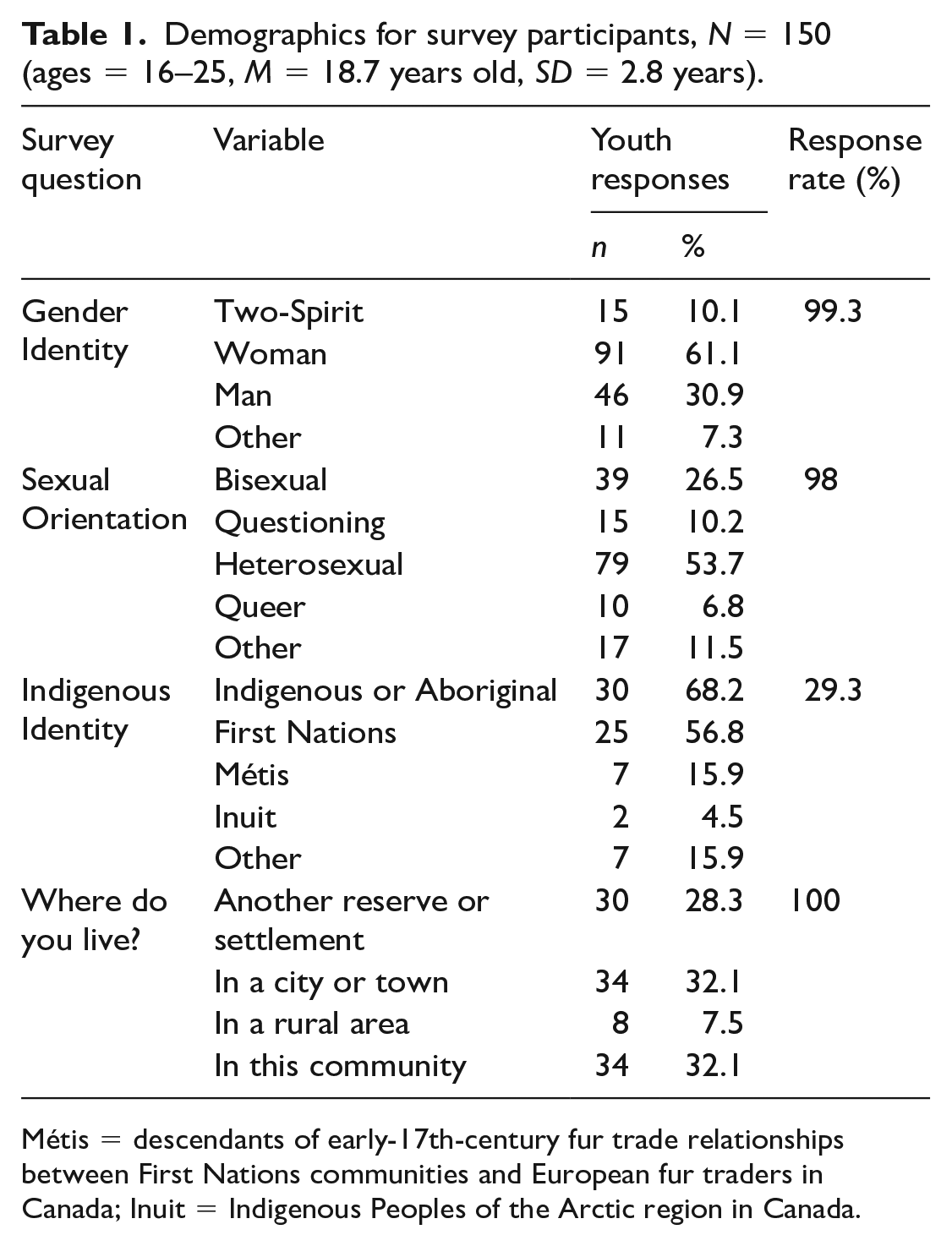
Métis = descendants of early-17th-century fur trade relationships between First Nations communities and European fur traders in Canada; Inuit = Indigenous Peoples of the Arctic region in Canada.
Table 1 summarizes the demographics of survey participants; Nearly all the questions allowed participants to select all that apply. A majority of respondents identified as Indigenous or Aboriginal (68%), followed by over half identifying as First Nations (56.8%). A total of seven participants identified as Métis, two participants identified as Inuit, and 16% participants identified as Other or European descent. Thirty-two percent shared that they live in the community where the event was being held, and another 32% shared that they live in a city or town. Twenty-eight percent of participants shared that they live on another reserve or settlement, followed by eight participants living in a rural area.
For gender identity, 60% of participants identified as women, followed by 31% identifying as men and 10% identifying as Two-Spirit. Seven percent of participants identified as Other, which also included gender non-conforming and trans. For sexual orientation, over half (54%) of participants identified as being heterosexual, over a quarter (27%) identified as being bisexual, 10% identified as questioning their sexual orientation, 7% identified as queer, and 12% identified as other which included lesbian, gay, pansexual, and asexual.
Table 2 presents experiences of participants based on safety at home and food security. Eighty-three percent of participants said that they “always” or “usually” feel safe and secure at home. When broken down by gender identity, of those who identify as Two-Spirit, 50% said they “never” or “sometimes” feel safe at home. Of those who identify as a man, 14% said they “never” or “sometimes” feel safe at home, whereas of those who identify as a woman, less than 1% (0.09%) said they “never” or “sometimes” feel safe at home.
Experiences of participants based on gender and sexuality (N = 150).
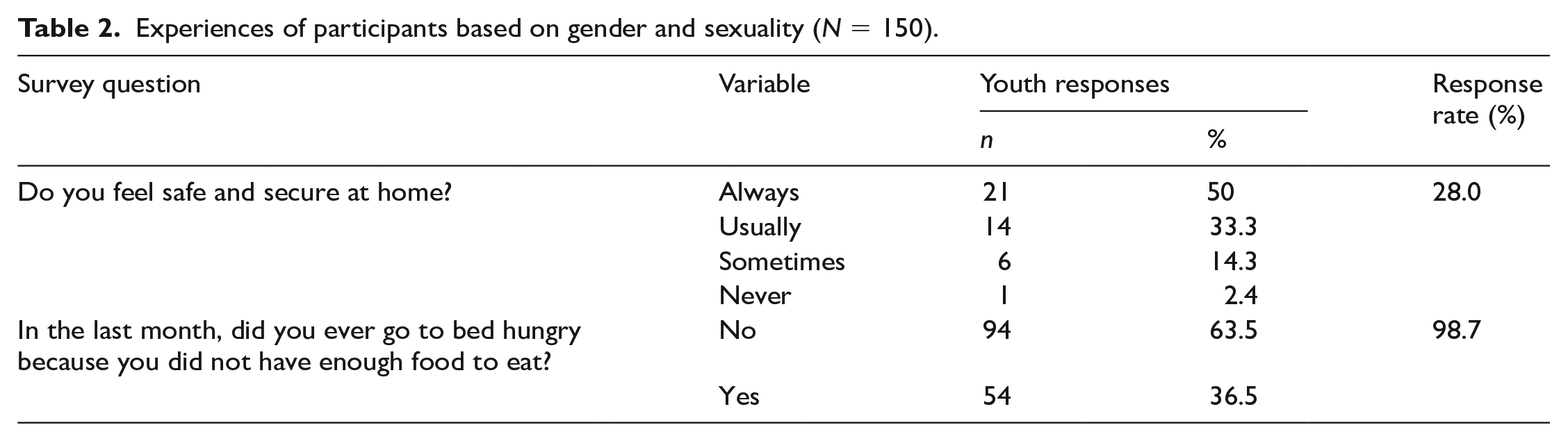
When asked whether they ever go to bed hungry because they did not have enough food to eat, over half (54%) of youth participants said “yes.” When broken down by sexuality, 40% of those who identify as Asexual, Bisexual, Two-Spirit, Lesbian, Pansexual, Queer, Gay, or Questioning, and 33% of those who identify as Heterosexual or Straight, said “yes” to going to bed hungry because they did not have enough food to eat. When broken down by gender identity, of those who identify as Two-Spirit, 21% said “yes” to going to bed hungry because they did not have enough food to eat. For those who identify as woman, 37% said “yes,” and for those who identify as man, 37% also said “yes” to going to bed hungry because they did not have enough food to eat.
Table 3 presents the behaviors and intentions of participants relevant to HIV prevention. Eighty percent of participants reported having had sexual intercourse. Of those who have had sex, 45% had two or more partners in the last 12 months. Thirty-five percent had not used a condom the last time they had sex. When broken down by gender identity, 50% of those who identify as Two-Spirit said “no” to using a condom the last time they had sex, whereas 37% of those who identify as a woman and 21% of those who identify as a man said “no” to using a condom the last time they had sex.
HIV prevention behaviors and intentions of survey participants (N = 150).
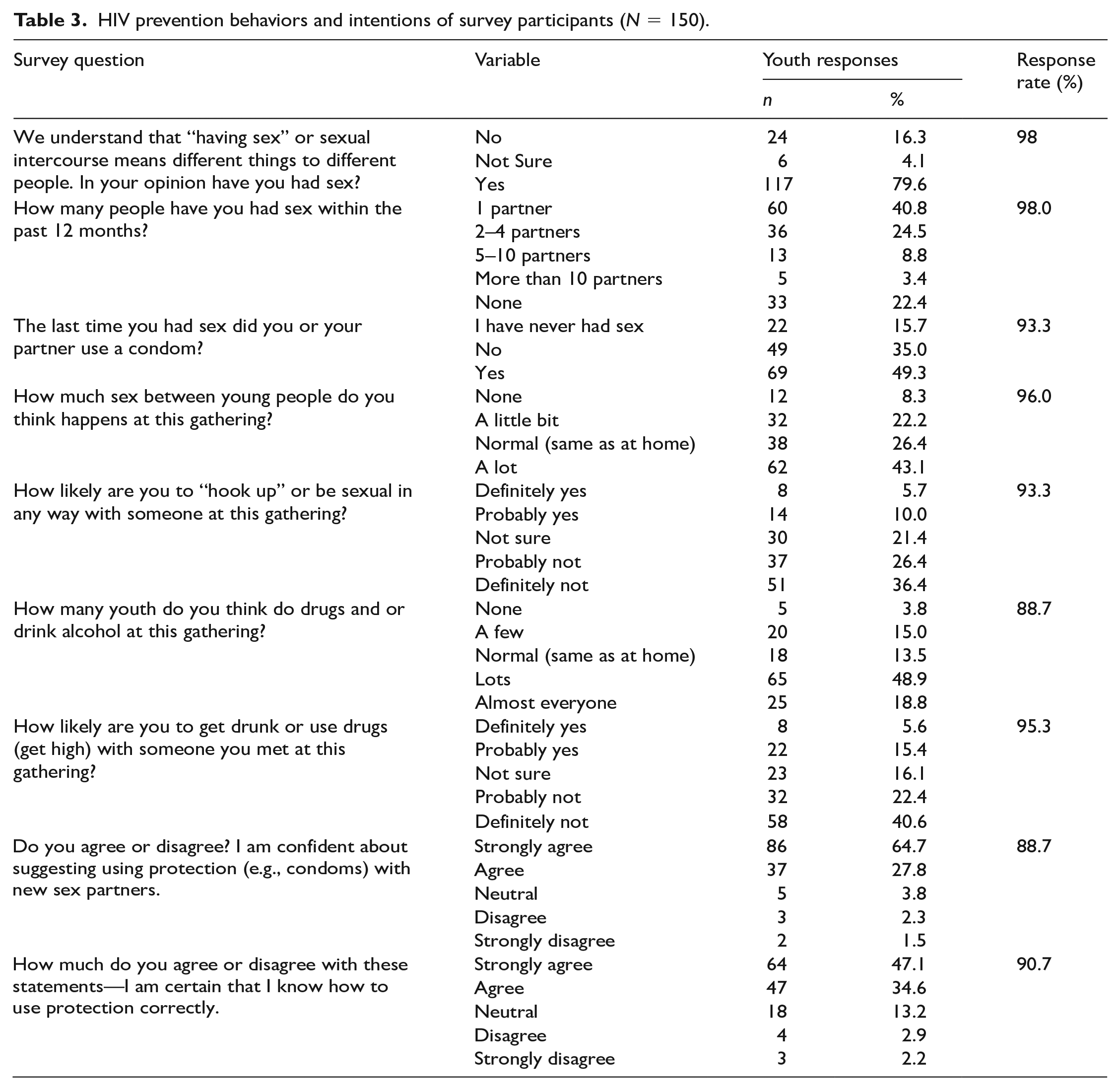
In terms of their perceptions of the event context, 43% of youth thought that “a lot” of sex happens at the gathering they were attending, 26% said “normal—same as at home,” 22% said that only “a little bit”, and 8% said no sex happens at the gathering. Sixteen percent said they were either “definitely” or “probably” going to “hook up” or be sexual with someone at the gathering, and 21% were not sure. Almost all (92.5%) participants said that they were confident about suggesting using protection with new sex partners, and 82% said that they are certain that they know how to use protection correctly.
Nearly 70% of youth felt that “lots” or “almost everyone” does drugs and or drinks alcohol at the gathering, while 14% believed it happened at “a normal amount.” Twenty-one percent thought that they would either “probably” or “definitely” get drunk or high with someone they met at the gathering; 16% were undecided.
Table 4 shows youth reactions to the SHC. Overall, youth rated the SHC positively (85% rated it as “awesome”; another 10% thought it was “okay”). When asked whether the gatherings were a good place to talk about sexual health and HIV, 89% agreed. Almost 90% felt that incorporating culture was either “important” or “very important” for sexual health education with Indigenous youth. When asked whether they have access to traditional knowledge, teachings, and ceremonies about their body, coming of age, sexual health, and reproduction, over a third (76%) “agree” or “strongly agree.”
Responses to the Sexy Health Carnival from survey participants (N = 150).
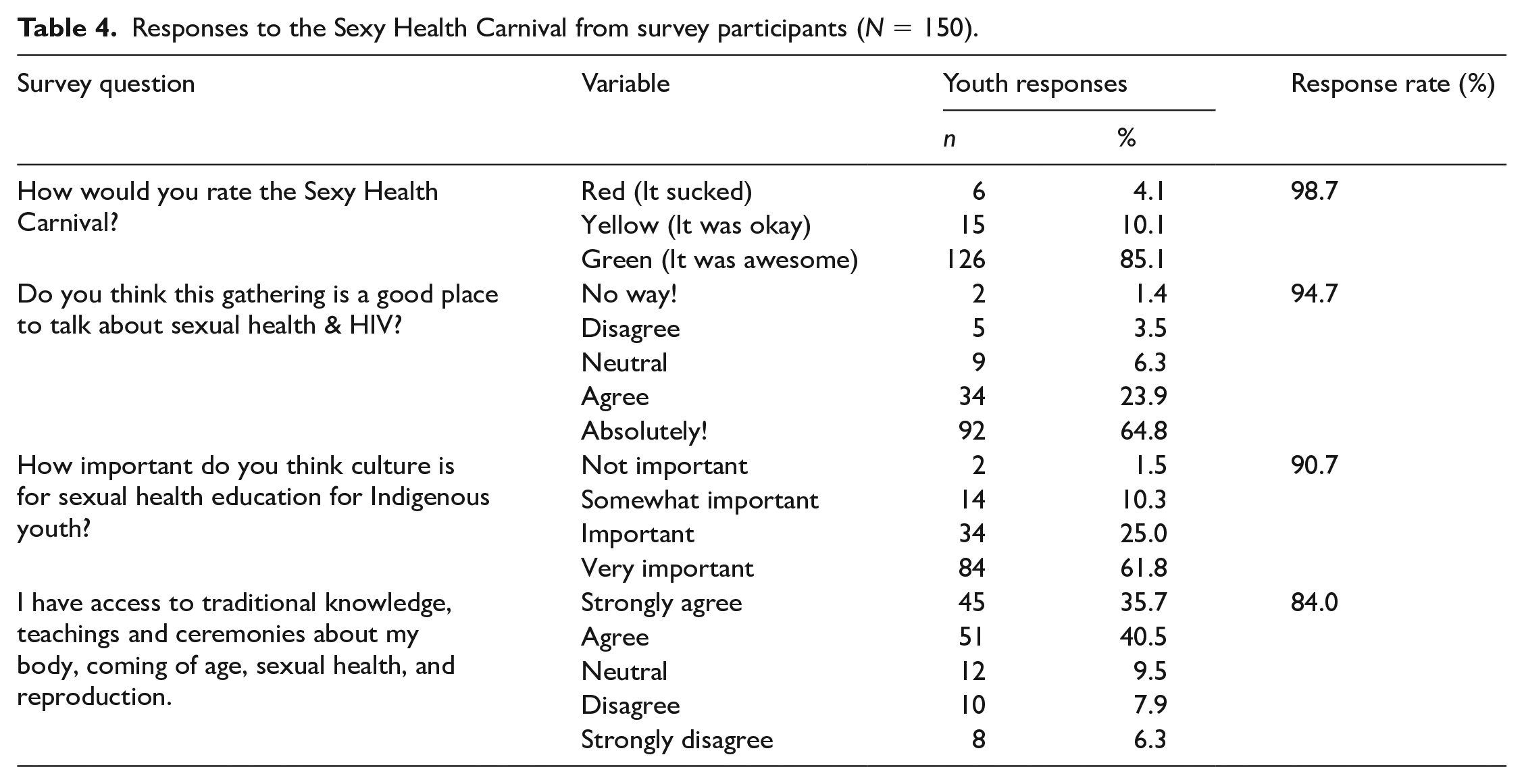
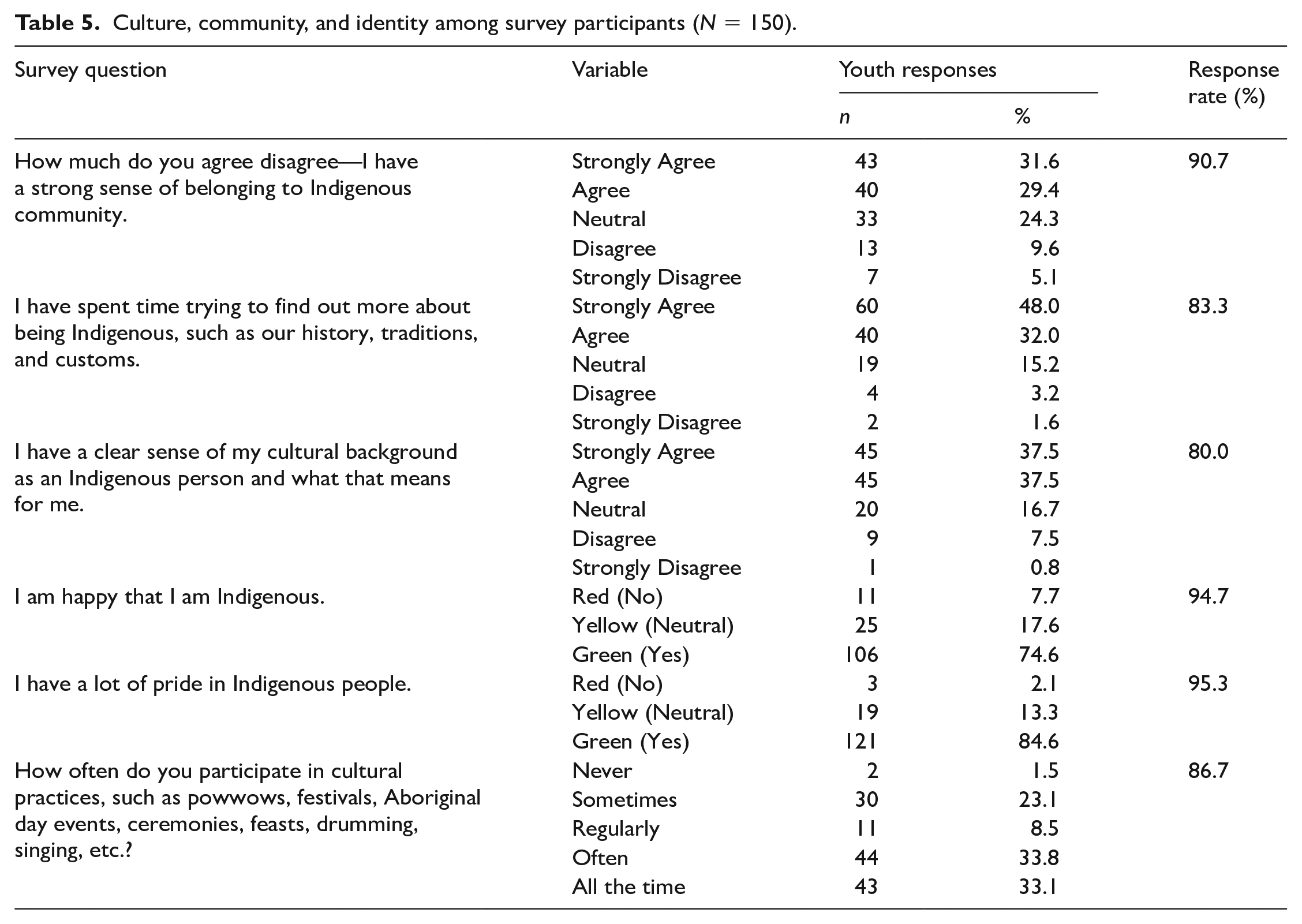
Table 5 presents youth’s responses around culture, community, and Indigenous identity. Sixty-one percent of participants said that they have a strong sense of belonging to an Indigenous community, 80% said they have spent time trying to find out more about being Indigenous, and 75% said that they have a clear sense of their cultural background as an Indigenous person. Seventy-five percent of participants shared that they are happy that they are Indigenous, whereas 17.6% said that they were neutral and 7.7% said they were not happy to be Indigenous. When asked whether they have pride in Indigenous people, the majority of participants (84.6%) responded yes. Seventy-five percent of participants said that they participate all the time, regularly, or often in cultural practices, such as powwows, festivals, Aboriginal day events, ceremonies, and or feasts.
Culture, community, and identity among survey participants (N = 150).
Discussion
The SHC takes a decolonizing approach to Indigenous peer-led sexual health and HIV outreach that centers the concerns and worldviews of Indigenous young people. Through the reclamation of intergenerational knowledges surrounding sexual health that were fractured through colonial law and policy, the SHC illustrates that Indigenous youth are capable of reaching their peers and developing successful sexual health outreach and HIV prevention resources for each other. As a result, our study revealed unique insights into topics such as acceptability of talking about sexual health in a cultural setting and HIV prevention behaviors and intentions.
While the survey revealed low condom use among those who are sexually active, youth respondents said that they are confident about suggesting using protection with new sex partners and that they know how to use protection correctly. It is important to note, however, that we did not have specific parameters for what “having sex” included and also did not collect information about condom use for specific types of intercourse, such as oral, anal. or toy-related sex. This may have created an over-inflated estimate of low condom use depending on the type of sex participants were primarily practicing. Given that youth were required to engage with the SHC prior to participating in the survey, confidence about suggesting using protections holds promise that the SHC may have a positive effect on HIV prevention behaviors and intentions among Indigenous young people. This aligns with evidence surrounding the importance of youth-led and locally tailored sexual health interventions by and for Indigenous youth (Lys et al., 2023). For example, a program called the Healthy & Empowered Youth Project in the United States delivered an Indigenous-specific student-led curriculum with hands-on learning activities to engage students in sexual and reproductive health topics that resulted in increases in condom use (Rushing et al., 2017).
Results highlighted that youth respondents said that they have access to traditional knowledge, teachings, and ceremonies about their body, coming of age, sexual health, and reproduction. This suggests that youth may be receiving education around sexual health and HIV prevention behaviors within their communities. This is significant as it signals that communities may be overcoming stigma and shame that surrounds sexuality caused by ongoing colonial legacies (Flicker et al., 2008; Negin et al., 2015; Restoule et al., 2010; Worthington et al., 2010). It is also likely that youth attending cultural gatherings may be more likely to have access to traditional teachings than youth not present.
Youth respondents also indicated that they have pride in Indigenous people and have spent time trying to find out more about being Indigenous. This may demonstrate that young people are actively seeking out and reclaiming traditional knowledge around their bodies and their sexual health. As Hackett and colleagues (2021) point out, sexuality was not considered shameful prior to colonization. Less than four generations ago, knowledge around sexual health and our bodies was transferred through the generations, and young people were taught to honor sexuality as a gift (Aboriginal Nurses of Canada & Planned Parent Federation of Canada, 2002; Hackett et al., 2021). These findings point to the ways that cultural resurgence efforts are working to help with the return of these traditions.
In regard to gender identity, a similarity to the Ontario pilot is that self-identified women predominantly participated in the SHC survey. This was then followed by men and then Two-Spirit young people. Lower rates of participation among young men in sexual health promotion activities are not uncommon and may be due to dominant constructions of gender that position sexual and reproductive health as women’s issues (Flicker et al., 2009), or an act of weakness (Devries & Free, 2010; Hackett et al., 2021). For Two-Spirit young people, low participation may be due to the lack of privacy in small communities, exacerbating stigma, discrimination, and isolation among those who do not conform to the colonial gender binary. This has been found to result in Two-Spirit and gender-diverse young people leaving their communities for safety and to receive acceptance (Brotman et al., 2002; Corosky & Blystad, 2016; Wilson et al., 2016). The risk of leaving one’s home community might further be exacerbated by Two-Spirit young people in our survey reporting that they do not feel safe at home and were most likely to go to bed hungry. So, while communities may be making some progress overcoming stigma and shame around sexuality as noted above, more effort must be made to ensure Two-Spirit and gender-diverse young people are safe and accepted.
Similar to the pilot project in Ontario, youth respondents indicated that a lot of sex and drug use takes place at cultural gatherings. While many youth respondents said that they do not personally engage in these behaviors at the gatherings, they do believe that others are sexually active and using drugs in these spaces “often” or “all the time.” Youth may have been reluctant to admit that they participate in these behaviors. Nevertheless, the SHC may be reaching youth who are vulnerable to HIV with an intervention and resources about which they are enthusiastic. Furthermore, respondents spoke of how the Indigenous gatherings were a good place to talk about sexual health and HIV, and that incorporating culture was important for sexual health education with Indigenous youth. This aligns with the literature, as Wilson et al. (2016) argue that the incorporation of culture, community, history, and tradition in sexual health education is essential for effective HIV prevention and health promotion initiatives for Indigenous youth. In speaking to the roles that Indigenous Elders can play in HIV community-based research, Flicker and colleagues (2015) echo the importance of including culture into HIV prevention programming.
Limitations
Although more than 1,000 youth engaged in SHC activities, a number of iPads containing encrypted data from hundreds of participants were unintentionally diverted due to an untimely car break-in half way through data collection. Given that the iPad surveys were offline, data were only uploaded when SHC facilitators had access to Wi-Fi. This was not always possible—particularly at rural and remote gatherings. As a result, a significant amount of data were ultimately lost. While this was an important learning for facilitators to upload results more often, it speaks to technology access disparities and also signals the need for more funding to support Indigenous peer-led sexual health outreach initiatives. Youth facilitators were often stretched thin as they tried to both facilitate carnival activities and administer surveys.
While the SHC attended 11 different communities across the country which were inclusive of First Nations, Métis, and Inuit-specific contexts, our results have no representation from the East Coast (New Brunswick, Newfoundland, and Prince Edward Island). Furthermore, while the SHC content was adapted to be locally relevant to the unique geographical context, some northern youth shared with facilitators that there was confusion with one of the games. This demonstrates the importance of peer-led sexual health outreach initiatives being developed and delivered by local Indigenous youth themselves, as they are the experts. In a study exploring STI knowledge and safer sex efficacy among adolescents aged 13 to 17 years in the Northwest Territories, Lys and colleagues (2023) underscore the importance of contextually tailored sexual health interventions with Indigenous youth. Moreover, due to small numbers of eligible youth responses, the survey respondents’ answers were grouped together, resulting in a pan-Indigenous summary of the results. Nevertheless, this project contributes to the limited literature unpacking how to promote sexual health by and for Indigenous youth across Turtle Island.
Another challenge was the diversity in gathering space and weather conditions among the 11 community gatherings. The SHC facilitators had to adapt to gatherings that would range from being indoors, outdoors, windy, rainy, sunny, hot, or cold, causing some gathering attendees to not want to engage with SHC materials. This also resulted in youth facilitators having to deal with information boards or pamphlets being blown around, or facilitators helping people to stay hydrated and fed. Some gatherings had a small space and or limited tables allocated for the SHC, which did not always allow for the full carnival set up. During one gathering that the SHC was brought to, local youth were filling up condoms provided by the SHC to use as water balloons to cope with the heat, stay cool, and have fun. The SHC facilitators supported this as young people became comfortable with handling condoms while decreasing stigma and shame around condom use. Despite this, some adult event staff were offended, tried to shame local youth, and advised SHC facilitators to pick up the discarded latex or they would be asked to leave. The SHC facilitators stepped in to support youth, and cleaned up the latex from the water balloons, despite a significant amount of litter from other event attendees. Reactions from adult staff highlight how further work needs to be done to reduce stigma around sexual health. Stigma and shame are real risks for individuals and communities impacted by HIV, and reducing these exacerbating factors must be prioritized (Lesperance et al., 2015; National Indigenous Youth Council on HIV/AIDS [NIYCHA], 2015). This project is a step forward in reducing stigma in a community setting and is a prime example of how future sexual health outreach needs to shift attention away from shaming and focus on strengths and empowering Indigenous youth (NIYCHA, 2015).
Finally, survey results demonstrate a lack of responses from Métis and Inuit identifying young people. While the SHC attended both Métis and Inuit-specific gatherings, more effort must be made to understand Inuit and Métis youth sexual health and peer-led sexual health outreach initiatives. Available literature demonstrates that Inuit youth experience considerably worse sexual health outcomes than other Canadian youth. For example, transmission rates have been reported to be over 10 times the national average for chlamydia, gonorrhea, and syphilis among Inuit youth and teenage pregnancy is over 5 times the national average (Corosky & Blystad, 2016; Mikhail et al., 2021). For Métis youth, there is a significant gap in the literature surrounding sexual health. This is worrisome as Métis experience cross-cutting health disparities and outcomes compared with First Nations communities (Allan & Smylie, 2015). A 2020 report highlights how Métis youth in British Columbia (BC) are 10 times more likely than non-Indigenous youth to live in foster care, and experience high rates of sexual violence (Representative for Children and Youth, 2020). Data from the 2018 BC Adolescent Health Survey found that only 55% of Métis youth said that they use condoms. When asked about sexual health education, a Grade 11 Métis student shared, “Our sex-ed has to be better. Nobody knows what they’re doing” (McCreary Society Centre, 2019, p. 35). While literature is limited, available information signals the critical need to prioritize Inuit and Métis youth sexual health. We also acknowledge that data from the Métis- and Inuit-specific events may have been taken when the iPads that were stolen.
Conclusion
The SHC is an Indigenous youth-led project that creates a fun and interactive opportunity for other Indigenous youth to become educated about HIV prevention and sexual health. This project illustrates that Indigenous youth are capable of reaching their peers and developing successful sexual health outreach and HIV prevention resources for each other. Furthermore, Indigenous youth think gatherings are a good place to talk about HIV, and that incorporating culture in sexual health education is important. Youth respondents reported that while they have some access to traditional knowledge, teachings, and ceremonies about their body, stigma persists. While several organizations across Turtle Island are doing HIV prevention and sexual health outreach work at Indigenous gatherings, there is little published (or even gray) literature available on the topic—suggesting that communities are focused on doing the work. Indigenous peer-led sexual health outreach and HIV prevention initiatives are effective and must be supported to reduce stigma.
In the time of COVID-19, where pandemic public health protocols, such as physical distancing and stay-at-home measures, stand in sharp contrast to gathering, kinship systems, and intergenerational knowledge exchange systems (Jones et al., 2020), we are once again thinking about how to be innovative with our outreach efforts. While moving elements of the carnival online may be one approach, it is clear that we will continue to pursue strength-based, culturally safe, peer-led models of health promotion that can be integrated into communal festivals and gatherings.
Footnotes
Acknowledgements
We acknowledge the Indigenous communities who participated in the SHC and welcomed NYSHN into their communities.
Authors’ note
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This work was supported by the Canadian Institutes for Health Research (Grant # RN251445-338103).
Glossary
biiskaabiyaang the need to look back and to carry forward knowledge
Inuit Indigenous Peoples of the Arctic region in Canada
Métis descendants of early-17th-century fur trade relationships between First Nations communities and European fur traders in Canada
potlach a ceremony integral to the governing structure and culture of various First Nations living on the Northwest Coast and in parts of the interior western subarctic in Canada