
Abstract
Anas Wayuu is an Indigenous-led non-profit health insurance organization in Colombia. It provides health care coverage to approximately 220,000 people, mostly Indigenous Wayuu, the largest Indigenous population in Columbia, living in La Guajira, the northeast region of the country, and in neighboring Venezuela. Anas Wayuu offers several intercultural health initiatives, among them the inclusion of bilingual guides for Wayuu families. The objective of the study was to describe the use of Anas Wayuu’s bilingual guides and determine whether use was associated with access and quality of care. A 34-item survey was conducted in 2020 to 2021 with a final sample of 2,113 Anas Wayuu enrollees and non-enrollees. Study findings demonstrated the relevance of bilingual guides programming. They suggested that bilingual guides improved individual’s capabilities to navigate the health care system, increased access to care, and increased their experience of quality of care. The findings strengthen the case for Indigenous self-governance over health care.
Keywords
Introduction
Intercultural health care takes place formally and informally in different instances of intervention, for instance, in health promotion, disease prevention, primary care, and secondary care. Also in relation to different health areas such as maternal and child health, mental health, and at different levels of care such as family, community, clinical, institutional—health center and hospital, and health system (Mignone et al., 2007). Intercultural health care can be understood in the following two broad and commonly intersecting approaches: two health care modalities that are articulated and complement each other, for instance, allopathic health care and traditional Indigenous health care, or cultural adaptations within one health care system, for example, within the allopathic health system. The former can be understood as intercultural complementarities in health care, and the latter as intercultural adaptations in health care. Regarding Indigenous peoples, intercultural complementarity in health implies practices in health care that articulate traditional Indigenous medicine and biomedical or Western medicine, where both are complementary. The basic premises of this complementarity are those of mutual respect, mutual recognition of knowledge, the will to interact, and the flexibility to change as a result of these interactions (Mignone et al., 2007). Intercultural adaptations in health care are implemented to compensate for a lack of cultural competence in healthcare providers [which] may cause [unstable] trust and distrust in the patient-healthcare relationship ... [which] may be caused by differences in belief systems, values, perceptions, expectations and style of expression and behaviour. (Alpers, 2018, p. 313-314)
Our study focuses on an intercultural health initiative that fits within the cultural adaptations model—bilingual guides in a Colombian Indigenous health organization, Anas Wayuu (AW, 2018), an Indigenous-led non-profit health insurance organization in Colombia.
In the Americas, the health status of Indigenous Peoples is comparatively lower than that of the general population, according to different indicators such as maternal and infant mortality (Montenegro & Stephens, 2006). The Pan American Health Organization identifies among the most common causes of death of Indigenous Peoples are as follows: malaria, tuberculosis, malnutrition, alcoholism, drug addiction, HIV, AIDS, and suicide (Organización Panamericana de la Salud, 2008). These poor health conditions are associated with poverty and social inequities, as well as limitations in access to health care. Intercultural health initiatives have the potential to decrease barriers in access to health services among Indigenous peoples (Mignone & Gómez Vargas, 2015). There are studies of intercultural health initiatives in Latin America (Fernández Juárez, 2010), but few address empirical outcome questions, largely due to the lack of data available for these types of studies.
There is a broad, varied, and rapidly increasing development of intercultural health practices, programs, and policies in Latin American. A strong basis for their development is the recognition of Indigenous peoples’ individual and collective rights. In fact, 15 countries in the Americas have ratified the International Labour Organization’s Convention on Indigenous and Tribal Peoples 169 of 1989. The Convention states in Section V, Social Security and Health, “that social security regimes should be progressively extended to the peoples concerned and applied to them without any discrimination” (International Labour Organization, 1989, p. 5). As well, it states that “governments must ensure that adequate health services are made available to the peoples concerned or provide those peoples with the means that allow them to organize and provide such services under their own responsibility and control” (International Labour Organization, 1989, p. 5). The Convention also states that “these services should be planned and administered in cooperation with the peoples concerned and should take in to account their economic, geographical, social and cultural conditions, as well as their prevention methods, curative practices and traditional medicines” (International Labour Organization, 1989, p. 5).
In Latin America, most intercultural health initiatives are initiated at the local level, promoted by Indigenous organizations, communities, or governments. One model of intercultural health is where Indigenous organizations have governance over both biomedical and traditional Indigenous health care, and/or over intercultural adaptations of the systems and practices. Health care organizations run by Indigenous authorities arguably are inherently intercultural.
In Colombia, there are approximately 115 Indigenous ethnic groups (Departamento Administrativo Nacional de Estadística, 2018). Among the largest are the Wayuu people, living in the northeast of region of the country, La Guajira. There is also a sizable Wayuu population in neighboring Venezuela. The Colombian Wayuu population in 2018 was 380,460 (Departamento Administrativo Nacional de Estadística, 2018) being 24% of the entire Indigenous population of Colombia. In terms of livelihood, the Wayuu raise livestock, mostly goats, produce and sell hand-woven items such as handbags and hammocks, and rely on multiple other informal income sources. A large proportion of Wayuu live in small rural villages and hamlets, some closer to urban centers and some in remote areas. Access to clean water is severely limited in many Wayuu communities (AW, 2015). In terms of the health situation, frequent pathologies include malnutrition, respiratory, and gastrointestinal infections among children below 5 years of age (Hernández Bello et al., 2017), sexually transmitted infections, uterine or cervical cancer, hypertension, injuries due to violence, and caries and other dental problems among all ages (Boily-Larouche et al., 2013).
Anas Wayuu is an Indigenous led non-profit health insurance organization created in early 2000 by two Indigenous associations representing 120 Wayuu authorities, chiefs of communities. At the time of the study, it was providing health care coverage to 220,000 people, 71% Indigenous Wayuu. A large majority of its management and staff are Wayuu. To provide coverage, AW contracts with a health care network of 27 Indigenous Health Service Provider Institutions and 65 non-Indigenous Health Service Provider Institutions privately owned (IPS) or from the public sector such as State Social Enterprises. The coverage includes health promotion and disease prevention services, and primary, secondary, and tertiary health care. AW offers several intercultural health initiatives, among them the inclusion of bilingual guides for Wayuu families that do not speak, or that have limited fluency, in Spanish (Mignone & Gómez Vargas, 2015).
Bilingual guides have been utilized for many years in numerous countries and in a variety of fields, such as education (Cooper et al., 1999), mental health (Musser-Granski & Carrillo, 1997; Singh et al., 1999), immigrant health care (Gregg & Saha, 2007), and health services of Indigenous peoples (Kaufert & Koolage, 1984). Studies on bilingual guides in health care have shown a positive impact when the guides are well trained (Flores, 2005). Previous studies identified that bilingual guides are more than mere translators. They are interpreters of culture (Gregg & Saha, 2007) because they have the capacity to observe what is unobservable by those who are from another culture (Mignone, 2002). Their task is to communicate subtle and/or implicit meanings, idiomatic expressions, tones of voice, facial expressions, in addition to verbal expressions (Egli, 1991). Furthermore, they interpret potentially discordant knowledge and belief systems (Kaufert & Koolage, 1984) due to their ability to bridge two worlds.
Bilingual guides that work with AW are required to have a clear knowledge related to the uses, customs, and legal system of the Wayuu people; mastery of Wayuunaiki, the language of the Wayuu, although not necessarily reading and writing in Wayuunaiki; communication skills in listening, speaking, reading, and writing in Spanish; and clear knowledge of how the general social security or health system operates. Usually, they have a Western education and a profession. Others, due to frequent contact with non-Indigenous people or due to their role within the communities—for example, traditional authorities—have acquired good bilingual communication skills. All share a fundamental characteristic, that is, the ability to communicate with administrative and health personnel because their Spanish is more specialized. This makes them key actors inside and outside health care centers.
At the time of the study, AW worked with 44 administrative bilingual guides and 26 clinical bilingual guides. Some guides employed directly by AW and some by Indigenous services providers paid through the insurance, such as AW. Of the 70 guides, the majority are based in La Guajira, while some work in Bogota, the capital city of Colombia, 2 hr by plane or 18 hr drive by car from headquarters of AW, and Barranquilla, a 5 hr drive from headquarters of AW. The bilingual guides working with AW provide services in both urban and rural areas and their functions are related to working with and raising awareness among traditional authorities, leaders and the community in general about rights and responsibilities in health; supporting health personnel in promotion and prevention talks in the communities; accompanying patients who are staying temporarily in the hostels and providing intercultural assistance; attending clinical consultations when necessary to facilitate interactions with the health care staff; providing guidance to the patient and providing support with administrative procedures; assisting with the identification of the population potentially benefiting from the health system; accompanying Wayuu patients who require specialized care outside of La Guajira to overcome language and cultural barriers.
Administrative bilingual guides provide support on issues such as enrollment in the system, customer service, procedures related to complaints and claims, scheduling appointments, mobility, portability, disability payments, access to transportation and/or hostels, among others. Their presence facilitates communication between the Wayuu enrollee and the staff at the health institutions.
Clinical bilingual guides work as interpreters in clinical encounters voicing the health concerns of the patient to the health professional and explaining to the patient, and their companion, what the health professional asks and states. Furthermore, they explain about medications prescribed, schedules, and forms of use. The clinical bilingual guides are also involved in health promotion and disease prevention initiatives, laboratory testing, emergency care, and so on.
The expectation is that using of bilingual guides will lead to more efficient navigation of the health care system and, therefore, more timely access to care, more appropriate health care, and better adherence to treatment. In addition, bilingual guides facilitate conversations between the patient and the clinician. Thus, it is expected that patients will receive better quality of care.
The study reported here is part of a larger project examining AW’s intercultural health initiatives. The objective of the study was to describe the use of AW’s bilingual guides and determine whether their use was associated with access and quality of care. We hypothesized that use of bilingual guides would improve Wayuu people’s interactions with the health care system by improving communication and contributing to enhanced understanding. Measurably, we would expect that use of bilingual guides be associated with increased access to health care and improved quality of care. To test this hypothesis, we examined the use of bilingual guides, and tested for associations between bilingual guide use and quality of care per positive experiences with administrative processes, medical consultations, and access to care.
Methods
Survey development and administration
A 34-item survey was developed collaboratively between the researchers and AW staff, including their cultural expert, a Wayuu Knowledge Keeper. The survey included questions about demographic characteristics such as gender, age, region of residence, languages spoken—Spanish, Wayuunaiki, self-rated health—poor to excellent, diagnosed physical health conditions, and receipt of health care in the past 3 years—yes or no. If respondents had used health care, they were asked about the quality of their health care experiences—positive, neutral, negative, use of bilingual guides—yes or no, and experiences with bilingual guides. Quality of care was defined as easiness in navigating the health care system and satisfaction. Quality of care was examined with respect to the following three aspects: administrative processes, medical consultations, and access to health services.
The survey was translated from Spanish to Wayuunaiki so it could be administered in participants’ preferred language. Four surveyors, bilingual in Wayuunaiki and Spanish, contacted prospective participants by cell phone. We had originally planned to administer the survey in-person but were unable to due to the COVID-19 pandemic. Participants’ responses were entered directly into an app designed for the study on the surveyors’ cell phone and uploaded to a central server. The data were regularly assessed for quality, such as duplicates, incomplete surveys, and surveyor patterns.
Sample
A random process was used to generate the sampling frame which consisted of 34,961 Wayuu individuals between 18 and 80 years old who were current or past enrollees of AW, that is, individuals not currently enrolled, although enrolled in a different health insurance organization. For each month of data collection, a random sample, without replacement, was created from the sampling frame. The surveyors attempted to contact each person in the sample. Over the 6 months of data collection, September 2020 to February 2021, the surveyors attempted to contact 25,249 individuals. However, they were only able to reach 2,530 people and of those, 83% agreed to participate, resulting in a dataset of 2,159 records. Duplicates and surveys that were not completed well were removed, resulting in a final sample of 2,113 participants. Current and past enrollees comprised 86.1% and 13.9% of the sample, respectively. This enabled analytical comparisons across three groups of individuals: AW enrollees who did not use bilingual guides, AW enrollees who used bilingual guides, and individuals who were not enrolled with AW and thus would not have access to bilingual guides.
Data analyses
For enrollees who used health care in the past 3 years, we described the characteristics of individuals, for instance, demographic characteristics and health status, who used and did not use bilingual guides, with frequencies and/or percentages, means, and standard deviations.
We performed a logistic regression analysis to determine the factors predictive of using bilingual guides. Next, to address the question of whether bilingual guides improve access and quality of encounters over and above the benefit of being enrolled with AW, we performed logistic regressions. The regression models controlled for potentially confounding variables, those that were significantly associated with the outcome variables in the bivariate analyses (p < .05). Analyses were performed with SPSS v. 25.0.
Ethics
The study topic was chosen by AW. The research questions and methodology were jointly developed by AW staff and university-based researchers. Furthermore, a Wayuu Knowledge Keeper provided advice during all stages of the study. The research team consisted of three AW-based members, two of whom were Wayuu, and three university-based members. Members of the research team that were not from AW signed an agreement with AW committing to follow an adapted version to the Wayuu context of the principles of Ownership, Control, Access, and Possession (OCAP) of information developed by Canadian First Nations organizations. In essence, these principles stipulate that AW owns, controls, safeguards access, and is possessor of all data utilized for the study. Furthermore, the study received approval by the Health Research Ethics Board at the University of Manitoba.
Results
Characterization of bilingual guides utilization
Most survey respondents (84.3%) reported using health care in the 3 years prior to the survey. Of the AW enrollees who accessed health care, 189 (12.1%) reported using a bilingual guide, while 1,369 individuals (87.9%) did not report using a bilingual guide. On average, individuals used bilingual guides 3.8 times (SD = 3.35) during the study period. Bilingual guides were used for administrative procedures (98.3%), accessing health care (94.4%), and medical consultations (94.7%; Table 1).
Reasons for using bilingual guides in the last 3 years for Anas Wayuu enrollees only.
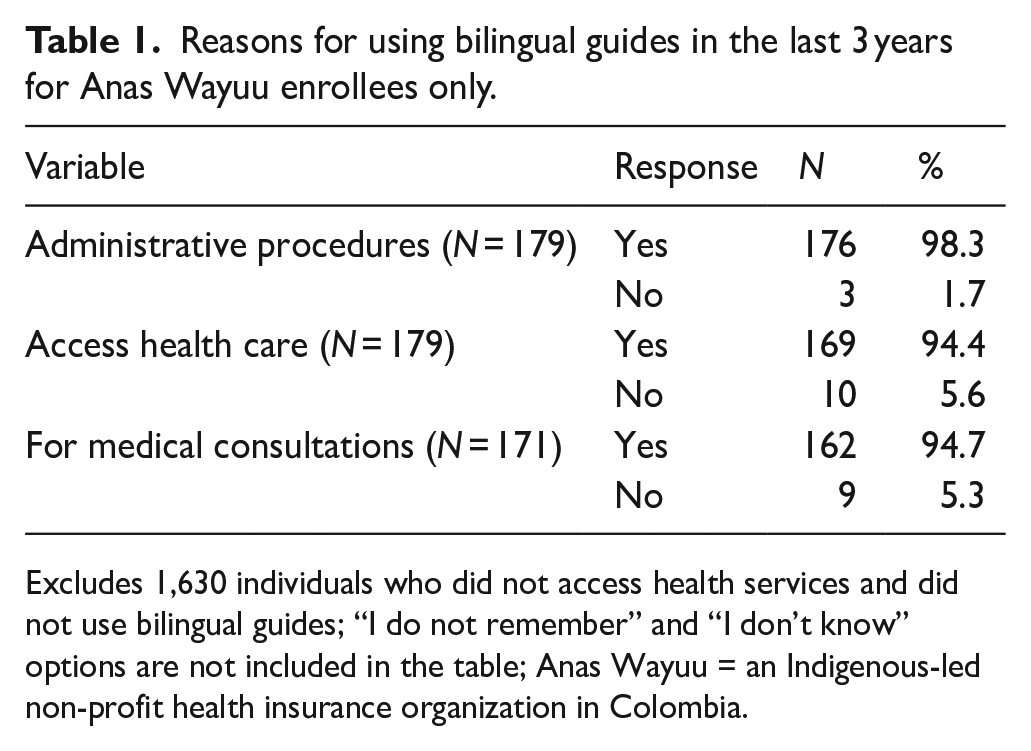
Excludes 1,630 individuals who did not access health services and did not use bilingual guides; “I do not remember” and “I don’t know” options are not included in the table; Anas Wayuu = an Indigenous-led non-profit health insurance organization in Colombia.
When asked about the quality of their experience using bilingual guides, almost everyone reported being better served, understanding the doctor better, finding it easier to access health services, and better understanding and following their treatment plan (Table 2).
Quality of health service experience associated with using bilingual guides for Anas Waayu enrollees only.
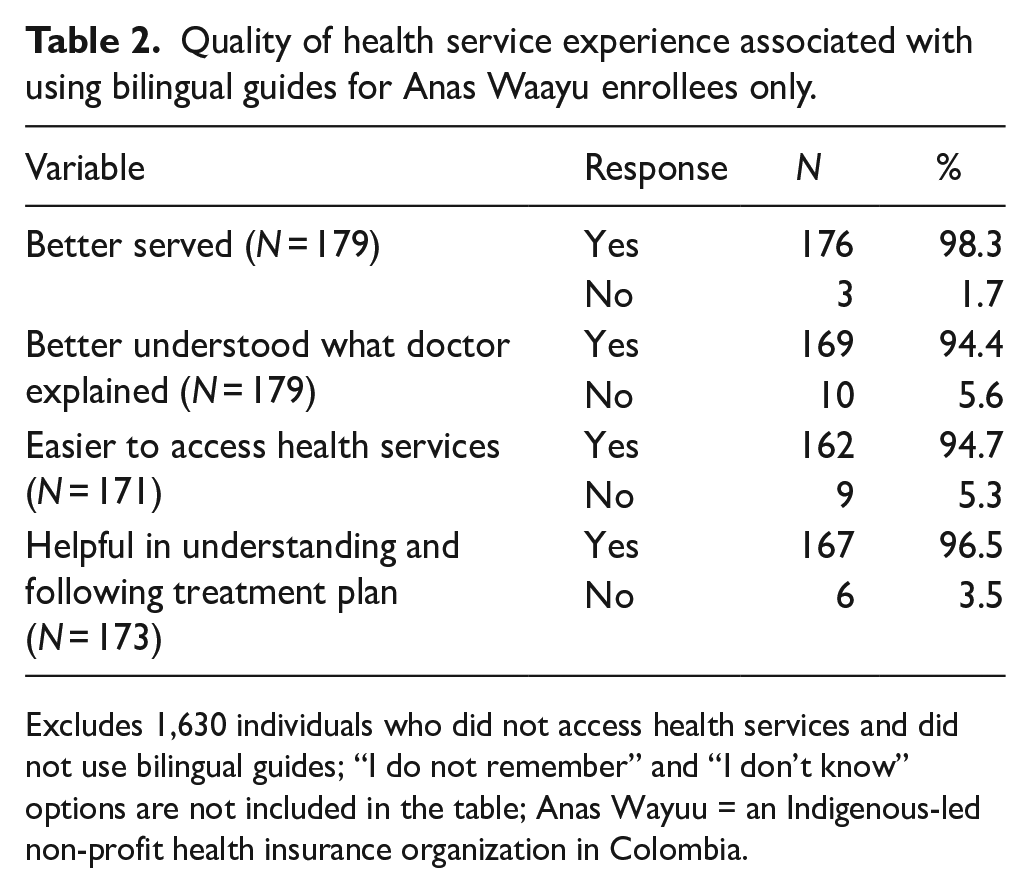
Excludes 1,630 individuals who did not access health services and did not use bilingual guides; “I do not remember” and “I don’t know” options are not included in the table; Anas Wayuu = an Indigenous-led non-profit health insurance organization in Colombia.
As shown in Table 3, use of bilingual guides was significantly associated with gender, type of insurance, languages spoken, self-rated health, and having an infectious disease. Specifically, a higher percentage of women (13.4%) reported using guides compared to men (9.4%). Of the respondents who spoke Spanish, 9.5% used bilingual guides compared to 22.0% of those who did not speak Spanish, and 17.3% of Wayuunaiki speakers used bilingual guides compared to 4.1% of non-Wayuunaiki speakers. Respondents with poor to satisfactory self-rated health (15.1%) were more likely to use bilingual guides than those with good to excellent health (11.1%).
Characteristics of Anas Wayuu enrollees who did and did not use bilingual guides (N = 1,558).
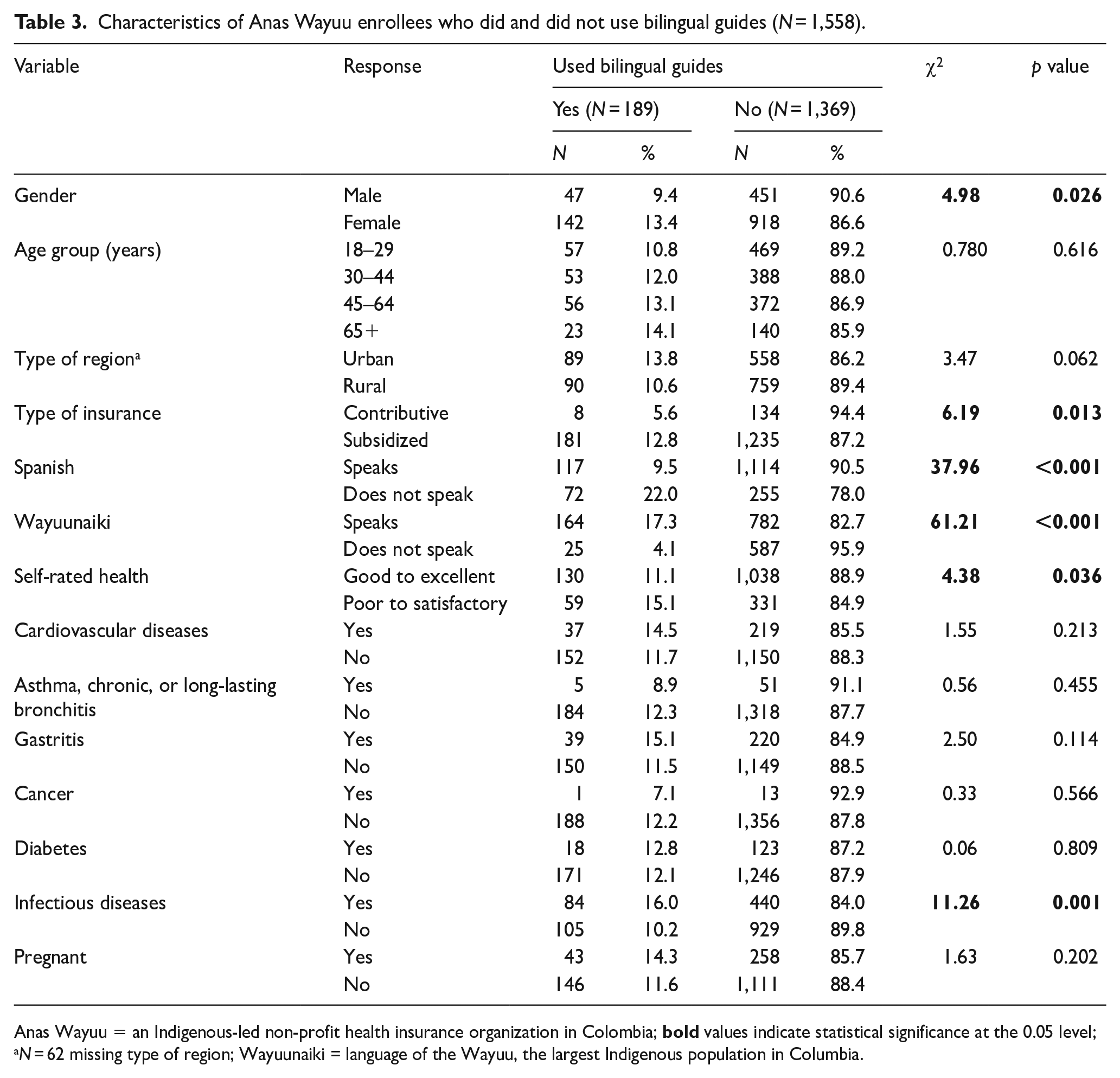
Anas Wayuu = an Indigenous-led non-profit health insurance organization in Colombia;
A follow-up logistic regression was performed to examine which variables were significantly associated with using bilingual guides when controlling for the other variables. The Nagelkerke R2 (pseudo-R2) for the full model was 0.125, suggesting that the model explains 12.5% of the variation in the outcome (using bilingual guides). The Hosmer and Lemeshow test of goodness of fit suggests that the full model was a good fit to the data,
ORs and 95% CIs for using bilingual guides among Anas Wayuu enrollees (N = 1,588).
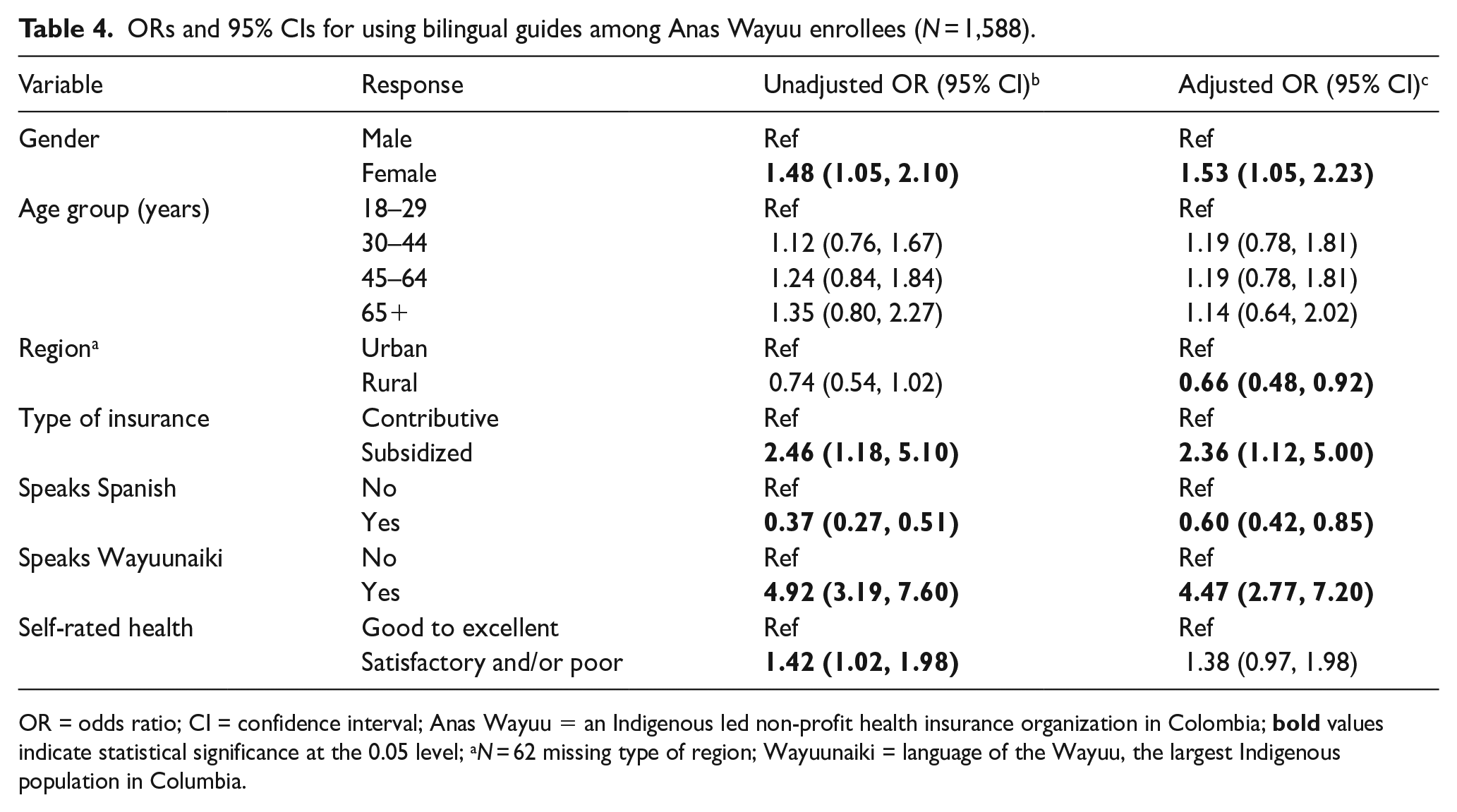
OR = odds ratio; CI = confidence interval; Anas Wayuu = an Indigenous led non-profit health insurance organization in Colombia;
More than half of the individuals (54.7%) who used health care in the past 3 years and who had access to bilingual guides, that is, AW enrollees, reported that they did not need bilingual guides. A logistic regression was performed to determine which factors are associated with not needing bilingual guides. The Nagelkerke R2 for the full model was 0.205, suggesting that the model explained 20.5% of the variation in the outcome, not needing bilingual guides. The Hosmer and Lemeshow test of goodness of fit indicated the full model was a good fit to the data,
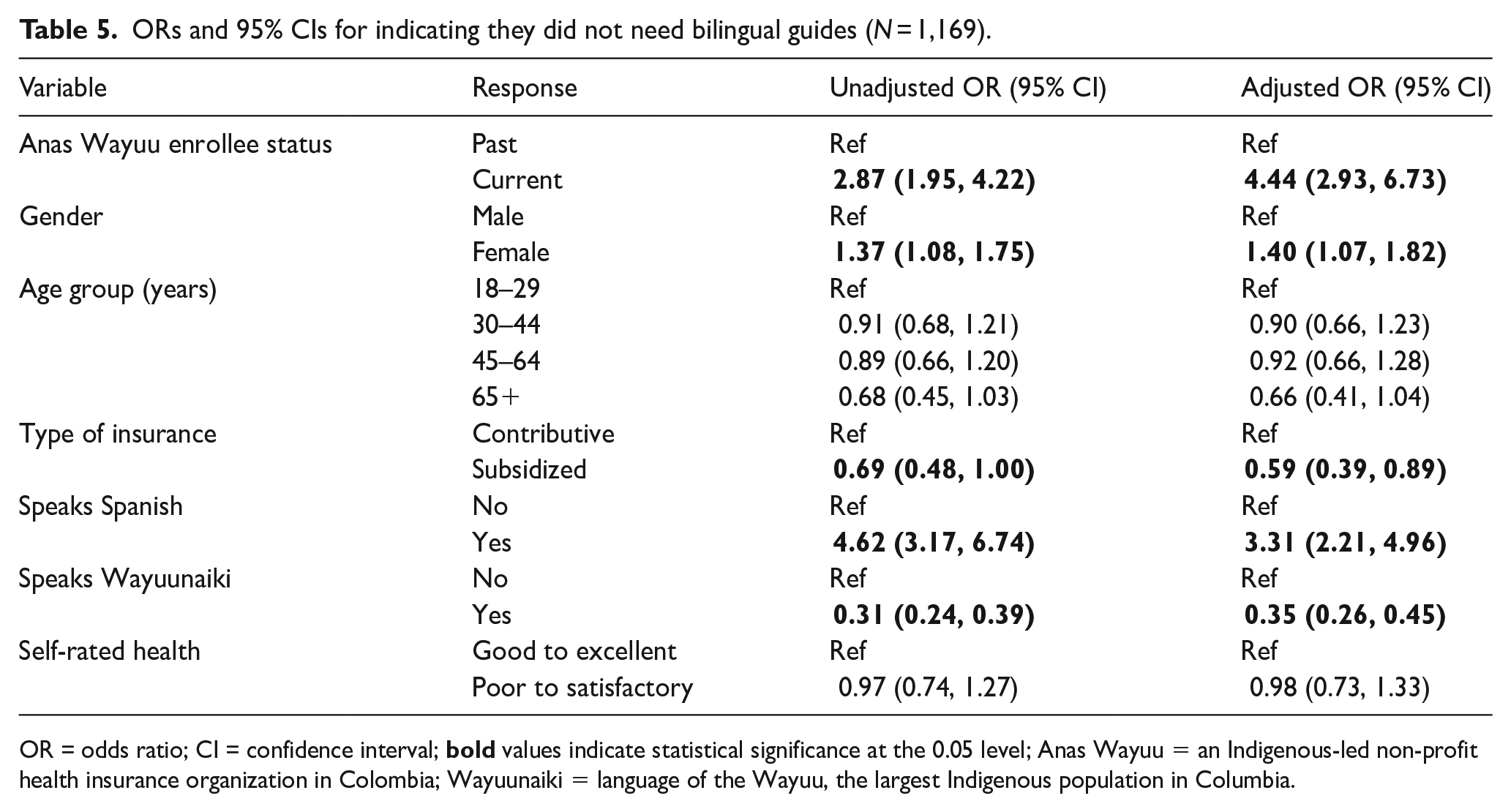
AW enrollment status, gender, insurance type, and languages spoken were significantly associated with need status (Table 5). Current AW enrollees were four times more likely to indicate they did not need bilingual guides than non-AW enrollees. Individuals that spoke Spanish were three times more likely (aOR = 3.31) to not need guides than non-Spanish speakers. Respondents that spoke Wayuunaiki were less likely to not need guides (aOR = 0.35); that is, were more likely to need guides than non-Wayuunaiki speakers. Those from the subsidized regimen were less likely (aOR = 0.59) to not need guides, meaning they were more likely to need guides.
ORs and 95% CIs for indicating they did not need bilingual guides (N = 1,169).
OR = odds ratio; CI = confidence interval;
Utilization of bilingual guides and quality of experience with health services
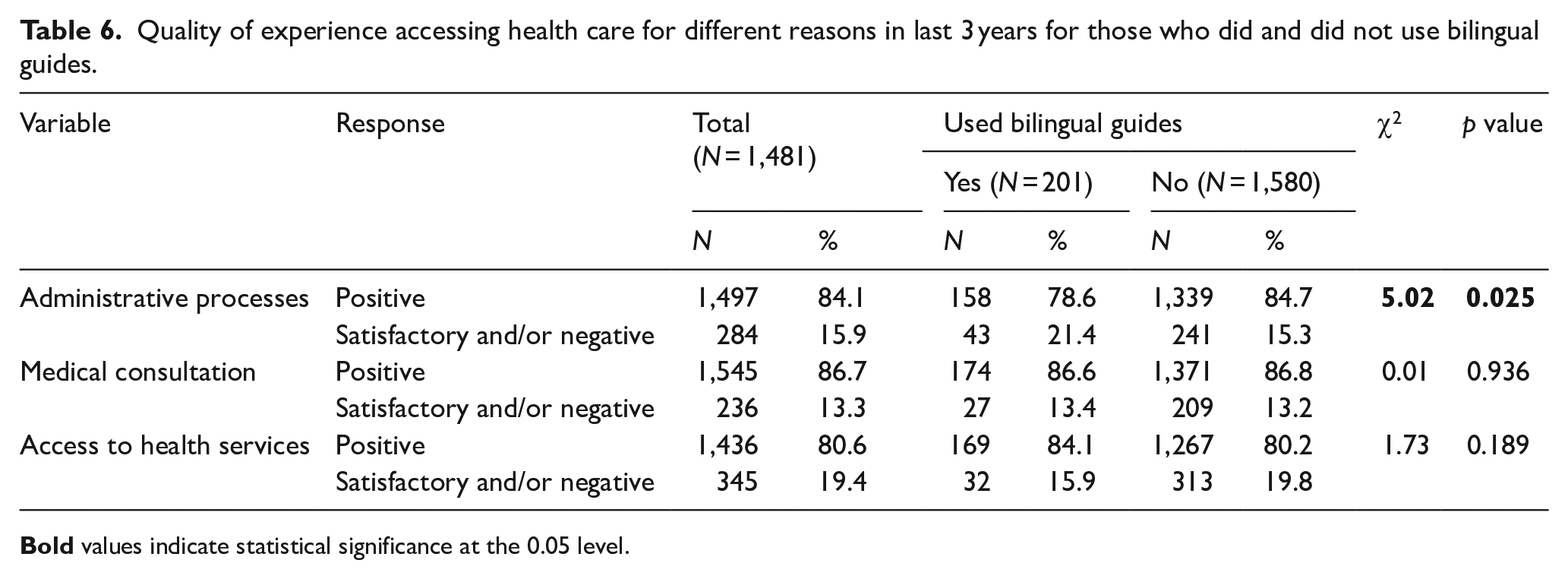
Table 6 shows the reported quality of experiences with the three aspects of health care by use of bilingual guides. A higher percentage of individuals who did not use bilingual guides rated their experiences with administrative processes and medical consultations as positive than those who used bilingual guides, while a higher percentage of individuals who used bilingual guides rated accessing health services positive compared to those who did not use bilingual guides. However, only the association between use of guides and rating of administrative process was statistically significant.
Quality of experience accessing health care for different reasons in last 3 years for those who did and did not use bilingual guides.
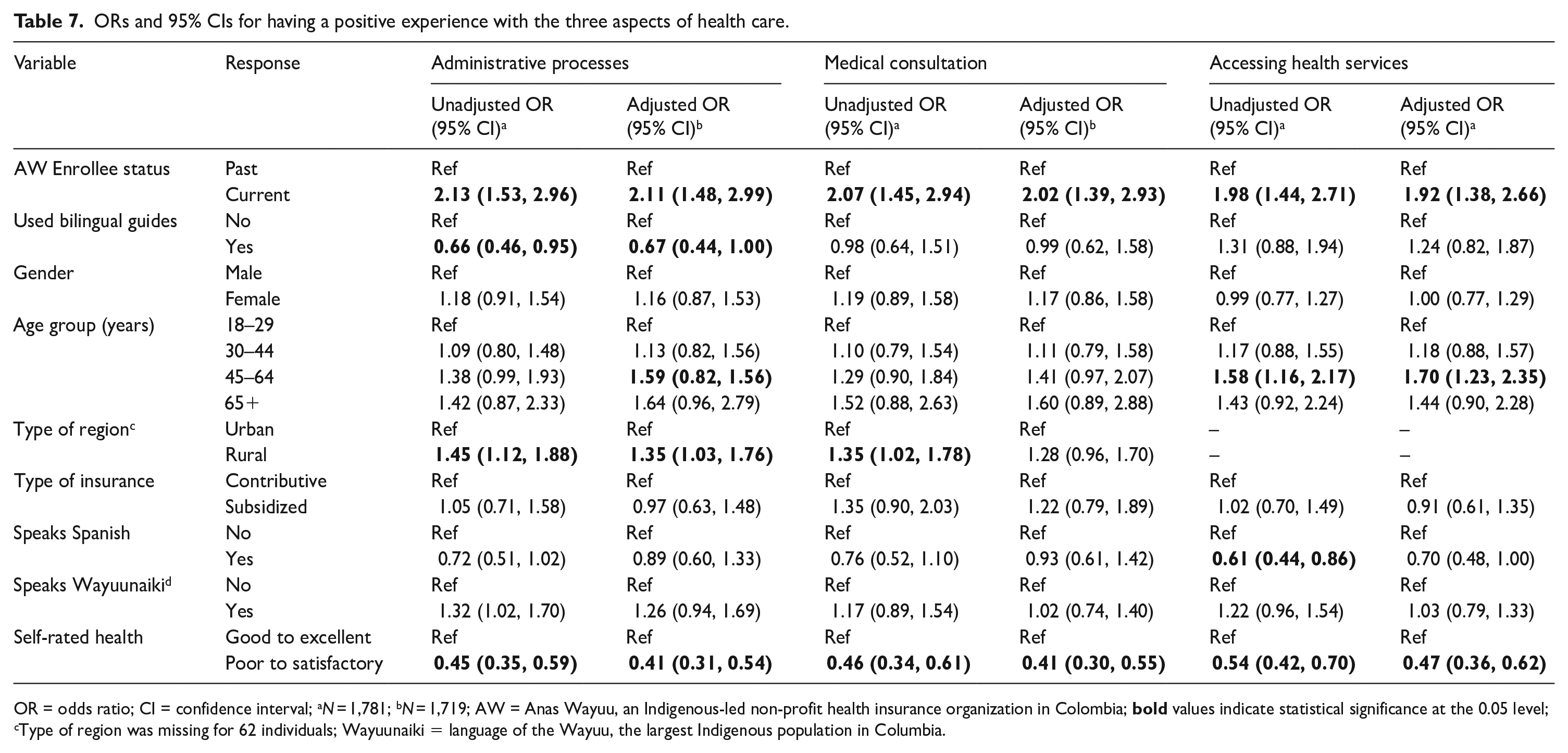
Logistic regressions were performed to determine if use of bilingual guides was significantly associated with quality of experiences with administrative processes, medical consultations, and accessing health services (Table 7).
ORs and 95% CIs for having a positive experience with the three aspects of health care.
OR = odds ratio; CI = confidence interval; a
N = 1,781; b
N = 1,719; AW = Anas Wayuu, an Indigenous-led non-profit health insurance organization in Colombia;
The Nagelkerke R2 for the full model for the three outcomes, administrative processes, medical consultation, and accessing health care, were 0.071, 0.056, and 0.053. The Hosmer and Lemeshow test of goodness of fit indicated the models were a good fit: administrative processes:
AW enrollment status was significantly associated with the three measures of quality of care. Specifically, current AW enrollees were more likely to report positive health care experiences than non-AW enrollees. Self-rated health was the only other variable statistically significant across the three models. Specifically, individuals with poor to satisfactory self-rated health were less likely to have a positive than those with good to excellent health.
Use of bilingual guides was significantly associated with quality of experiences with administrative processes; however, it was in the direction opposite to what was hypothesized. That is, individuals who used bilingual guides were less likely to report a positive experience with administrative processes than those that did not use bilingual guides. Use of bilingual guides was not significantly associated with quality of medical consultations or accessing health services.
Discussion
A recent article states that “emerging evidence suggests that Indigenous-led health service partnerships improve holistic health outcomes for Indigenous Peoples, as well as access to care, prevention uptake and adherence to care plans” (Allen et al., 2020, p. 208). However, as the authors of a report of the Economic Commission for Latin America and the Caribbean argue that “the assessment of the impact of these actions is limited due to the lack of systematic and timely information” (Comisión Económica para América Latina, 2014, p. 217). Our study is one of several that are seeking to address this gap. One central aspect of AW’s intercultural health initiatives is the potential for improved access to health services, and more timely and appropriate health interventions by reducing cultural and language barriers. AW has implemented numerous approaches. Using survey data, we empirically characterized bilingual guides utilization, assessed the association between bilingual guide use, quality of care, access to care, and factors associated with the use of bilingual guides. As well, we assessed the availability of bilingual guides as predictive of increased quality of care as per positive experiences with administrative processes, medical consultations, and access to care.
Of those who accessed health care in the last 3 years, almost 14% had used a bilingual guide, and on average, individuals had used bilingual guides almost four times in the last 3 years. Respondents used bilingual guides in very similar proportion for administrative procedures, access to health care, and medical consultations. Not surprisingly, the region with highest percentage of respondents utilizing guides was Alta Guajira, followed by Media Guajira, and the lowest in Baja Guajira. This corresponds well with what would be expected because the Alta Guajira has more remote populations and has a higher proportion of non-Spanish speakers, followed by Media Guajira. Consequently, the findings for the most part correspond with what would be expected; regions and people with higher fluency in Spanish tend to utilize bilingual guides less, and those with poorer health tend to utilize them more.
A summary of results shows that individuals not enrolled in AW were four times more likely to indicate that they needed bilingual guides than those enrolled. A possible reason for this is that among AW employees and its network of IPSs, there is an important number of staff members who are fully or partially fluent in Wayuunaiki, which is an intercultural factor in itself. Furthermore, approximately 70% of AW staff are Wayuu themselves, which facilitates cultural understanding, added to the fact that AW includes other Wayuu-appropriate features in its settings and operations.
In relation to the quality of enrollee’s experience with using bilingual guides, the great majority reported being better served, being able to understand better the treatment plan, and having easier access to health services. These are strong findings supporting the relevance of bilingual guides. AW enrollees were twice as likely to have a positive experience with administrative processes, with medical consultations, and having a positive experience accessing health care services than non-AW enrollees.
Our findings seem to corroborate what two other published studies suggest. A study by Dodgson and Struthers (2005) found that improving the communication skills of biomedical health providers in the Quechua language helps build a relationship of trust. As well, a 2016 qualitative study by Patiño and colleagues (2016) examined the use of bilingual guides to decrease cultural barriers to health care access among Wayuu Indigenous communities and noted that bilingual guides were key agents in reducing these barriers.
Among limitations of the study is the fact that the use of cell phones for the survey may have been introduced a bias of overrepresentation of urban dwellers due to less reliable connectivity in rural areas. Furthermore, that the survey was sometimes conducted in Spanish and sometimes in Wayuunaiki, which could have introduced differential understanding of the questions. Finally, as can be expected with surveys that ask about events in the recent past, it is likely that there were recall errors in the information provided by respondents.
Conclusion
To our knowledge, this is the first study that has empirically assessed intercultural health initiatives in Latin America. Our study empirically characterized an intercultural health initiative of AW, bilingual guides, and assessed it in terms of access to health care. Intercultural health care can be understood as including the following two broad, and often intersecting, approaches: (1) cultural adaptations within a health care system, such as biomedical health care system and (2) as two systems that are articulated and complement each other. AW’s initiatives studied here fall, for the most part, within the former approach, albeit with a highly significant and positive caveat. That the biomedical health care system of AW is under the governance of Indigenous authorities and that AW is composed of a majority of Indigenous staff and management.
The study findings have demonstrated the relevance of bilingual guides programming. The findings suggested that having bilingual guides improved the capabilities to navigate the health care system and increased access to care. While it is not possible to disentangle bilingual guides as unique factor in increasing access to care and the experience of quality care, the value of having bilingual guides was made evident by the findings. The study showed that bilingual guides are an important complement to the array of elements within AW that facilitate access to care and increase enrollee’s experience of quality of care. More so, these findings strengthen the case for Indigenous self-governance over health care.
Footnotes
Acknowledgements
The authors acknowledge the invaluable support of Reynaldo Ipuana, Knowledge Keeper and cultural advisor to Anas Wayuu in the development and translation of the survey, and of Crister Cotes for his superb coordination of the implementation of the survey.
Authors’ note
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: Inter-American Development Bank.
Glossary
Anas Wayuu an Indigenous-led non-profit health insurance organization in Colombia
Wayuu the largest Indigenous population in Columbia, living La Guajira, the northeast region of the country, and in neighboring Venezuela
Wayuunaiki the language of the Wayuu