
Abstract
Understanding what culturally safe care means to First Nations people is the first step to reimagining how healthcare can be conceived and operationalized. This study explored the meaning of culturally safe cancer care with Algonquins of Pikwakanagan First Nation in Canada, including community members’ perceptions of barriers to receiving it. Two focus groups using journey mapping were held with cancer survivors and family members (n = 16) and healthcare providers (n = 12), followed by individual interviews (n = 13). Discussions were video-recorded, transcribed verbatim, and thematically analysed. Culturally safe cancer care encompassed: (a) family and community, (b) culture as healing, and (c) stories for sharing cultural teachings. Ongoing systemic racism was described as prevalent in cancer care today and a significant barrier to culturally safe care. Further research is needed for health system change to dismantle the systemic and structural factors that continue to make healthcare unsafe and harm Indigenous People.
Introduction
First Nations are the largest group of Indigenous peoples in Canada, accounting for 60%, or nearly one million people (Statistics Canada, 2022). A long history of settler colonialism in Canada has created profound health disparities for First Nations People including higher cancer prevalence and lower 5-year survival rates (Chiefs of Ontario et al., 2017; Mitchell et al., 2019). While the causes of this increased cancer burden are complex and include low rates of screening and late-stage diagnoses (Chiefs of Ontario et al., 2017; Kewayosh et al., 2015; Marrett & Chaudhry, 2003), more pervasive reasons stem from colonial legacies of systemic racism, social exclusion, and structural violence that continue to shape their lives today (Canadian Partnership Against Cancer, 2013; Hammond et al., 2017; Shahid et al., 2011; Treloar et al., 2014). One pervasive and ongoing impact of colonialism is the erasure of Indigenous values, cultural norms, and belief systems. As a result, western healthcare practices do not typically align with Indigenous ways of knowing about health and healing, and Indigenous People continue to be marginalized and disenfranchised from engaging in cancer survivorship supports (Chiefs of Ontario et al., 2017; Gifford et al., 2021).
Culturally safe care is a model of healthcare delivery that aims to transform services and supports to be more equitable and free of racism and discrimination for Indigenous People (Health Council of Canada, 2012). First described by Māori (Indigenous People of New Zealand) nurse Irihapeti Ramsden in the 1980s, culturally safe care grew out of the recognition that the attitudes and approaches of nurses and other health professionals play a significant role in their healthcare experience (2015). Culturally safe care is premised on the understanding that power imbalances are inherent in the healthcare system and requires an awareness and reflection on the biases, prejudices, and assumptions that position contemporary healthcare values and practices as “normal”, while the practices, customs, and traditions of Indigenous People as “different, exotic and other” (Ramsden, 2002, p. 116). Culture in culturally safe care relates to socioeconomic status, gender, age, ethnic origin, sexual orientation, (dis)ability, or religion; it incorporates an awareness of past injustices and discriminations that continue to impact the lives of Indigenous People. What is crucially important is for health providers to recognize that culturally safe care is not about gaining insights into the cultural customs, and traditions of Indigenous People, but rather requires an understanding of the pervasive government policies, racism, and systemic inequalities that continue to harm Indigenous People today (Brascoupé & Waters, 2009; Curtis et al., 2019; Ramsden, 2015). Consciously or not, healthcare providers are complicit in perpetuating the dominant beliefs, values, and assumptions that reinforce structural violence and racist stereotypes, and thus, they must personally examine and reflect on their attitudes, biases, and practices that contribute to the ongoing marginalization, alienation, and trauma of Indigenous Peoples. For care to be culturally safe, a reflexive shifting in power relations is required, from healthcare providers as scientific authorities, to Indigenous patients and families as the experts in their own care and cultural safety (Ramsden, 2002). As emphasized by Papps and Ramsden (1996), cultural safety is relevant to every healthcare interaction and extends beyond the mere knowledge of different customs and traditions.
Indigenous People have demonstrated incredible resilience to colonization and it is imperative to build upon their strengths and visions of cultural safety to support cancer survivorship care (Canadian Partnership Against Cancer, 2011; Chiefs of Ontario et al., 2017). A recent scoping review found that key components of culturally safe healthcare initiatives for Indigenous People include collaboration and partnerships, power sharing, understanding the broader context of patients’ lives, a safe environment, self-reflection, and healthcare provider training (Brooks-Cleator et al., 2018). A central tenet of culturally safe care is that receivers of care define and determine what cultural safety means to them (Ramsden, 2015), making it necessary to understand how Indigenous communities conceptualize culturally safe cancer care.
Study aim
The aim of this study was to understand the meaning of culturally safe cancer care among Algonquins of Pikwakanagan First Nation in Ontario. We also explored barriers that participants encountered to receiving culturally safe care on their cancer journeys.
Setting
Pikwakanagan First Nation is a proud Algonquin community on the shores of Golden Lake in Renfrew County, Ontario, with over 2,000 members and approximately 500 people living in the community. This study was conducted in partnership with Minopimàdiz-i Gamik (Healing House), the Pikwakanagan Health Services and Family Health Team, which provides holistic health programmes to members of the Algonquins of Pikwakanagan First Nation (Algonquins of Pikwàkanagàn First Nation, 2018).
Methods
Our study recognizes that Indigenous People have a long and established history of developing and using their knowledge in practice through engagement, oral traditions, and cross-cultural sharing (Smylie et al., 2004). We used a qualitative participatory research design that emphasizes cultural values, community engagement, and mutually respectful relationships. Early discussions with community partners identified journey mapping as a culturally relevant strategy to elicit the meanings of culturally safe cancer care. Journey mapping is a process where patients, family members, and healthcare providers trace their interactions through the healthcare system to understand problems in service delivery and identify areas for improvement (Koski et al., 2017; McCarthy et al., 2016).
This study was reviewed and approved by the University of Ottawa’s Research Ethics Board (File # H-06-18-787). We took guidance from the Tri-Council Policy Statement: Chapter 9: Research Involving the First Nations, Inuit and Métis Peoples of Canada (Government of Canada, 2018); OCAP® principles of knowledge ownership, control, access, and possession (First Nations Information Governance Centre, 2018), and recommendations from our First Nations partners. With a history of working collaboratively in research, our community partners readily engaged throughout the research process, identifying the research priorities and ensuring the methodology and interpretation of findings reflected their perspectives and ways of knowing.
Data collection
We held two sharing circles with: (a) people who had experienced cancer or family members who had cared for someone along the cancer journey including diagnosis, treatment, survivorship, and palliation (n = 18); and (b) healthcare providers from the Pikwakanagan Health Team (n = 12).
Similar to focus group discussions, sharing circles are used to explore and construct knowledge in small groups. However, procedures and protocols vary. Sharing circles are considered more egalitarian with everyone recognized as an expert contributor to the discussion, and they can also have sacred meanings in Indigenous cultures through growth and transformation for participants (Lavallee, 2009).
Using journey mapping methods, sharing circles were collaboratively conducted by a community member, a university researcher, and a facilitator with prior experience conducting journey mapping in the community. We facilitated a storytelling exchange with questions to elicit participants’ experiences receiving or providing care along the cancer journey, and areas for improving care among healthcare providers (Table 1).
A sample of the questions asked in sharing circles with people who experienced cancer and their family members.
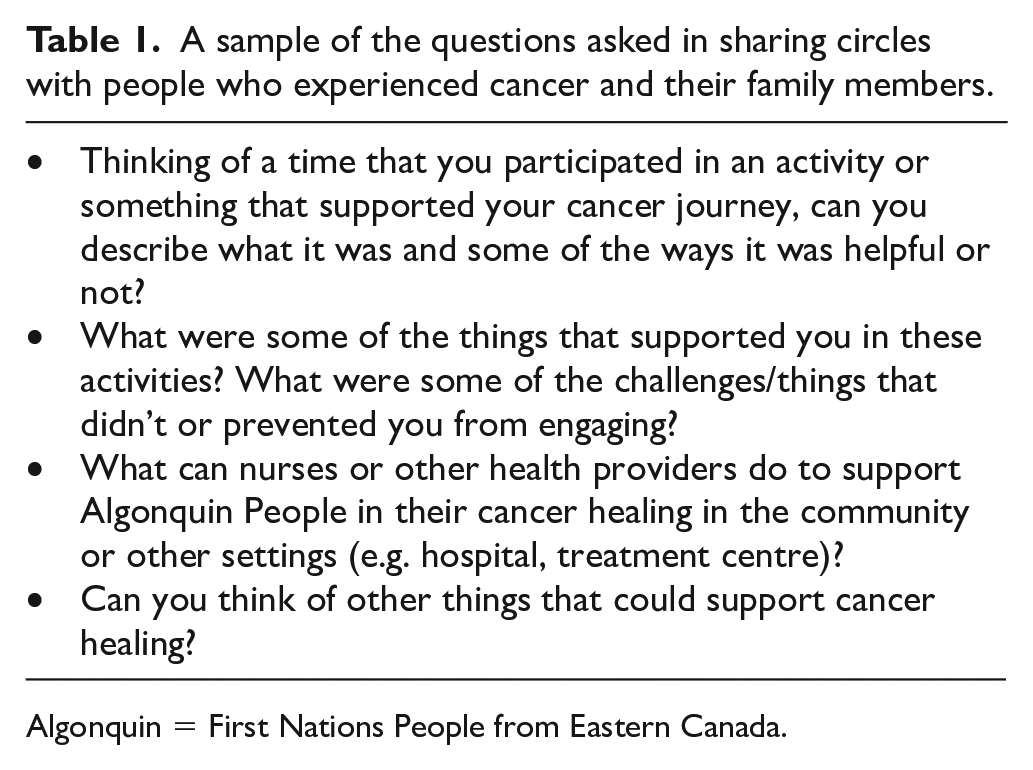
Algonquin = First Nations People from Eastern Canada.
At the end of each sharing circle, participants were invited to discuss their experiences further in an individual interview. Thirteen interviews were conducted with cancer survivors or family members who had cared for someone with cancer (n = 7) and health providers (n = 6), with similar questions to those in the sharing circles, but designed to elicit more in-depth information.
Data analysis
Sharing circles and interviews were video and audio-recorded. The audio recordings were transcribed verbatim and imported into NVivo 12 software to facilitate analysis (Q. S. R. International Pty Ltd., 2020).
Audio transcripts were analysed collaboratively by University of Ottawa settler researchers (WG, DR, ZA) and Pikwakanagan community partners (MB, MS, PD). First, two researchers (DR, ZA) read the transcripts in their entirety to familiarize themselves with the data, before performing line-by-line coding and creating a list of initial codes to capture main ideas. This list and its supporting data were reviewed in face-to-face meetings between university researchers (WG, DR, ZA) and community partners (MB, MS, PD), and codes were synthesized and categorized into preliminary themes. Following that, the lead researchers from the university (WG) and Pikwakanagan First Nation (PD) refined each theme by integrating concepts that tie the data together and generating clear definitions and descriptions.
The final analysis stage involved selecting vivid data extracts that represent the meaning of culturally safe cancer care among Algonquins of Pikwakanagan First Nation. Based on the analysis, video recordings were used to develop a documentary film about the meaning of culturally safe care for Pikwakanagan community members (https://vimeo.com/552368203/fcb1c00d4b).
Results
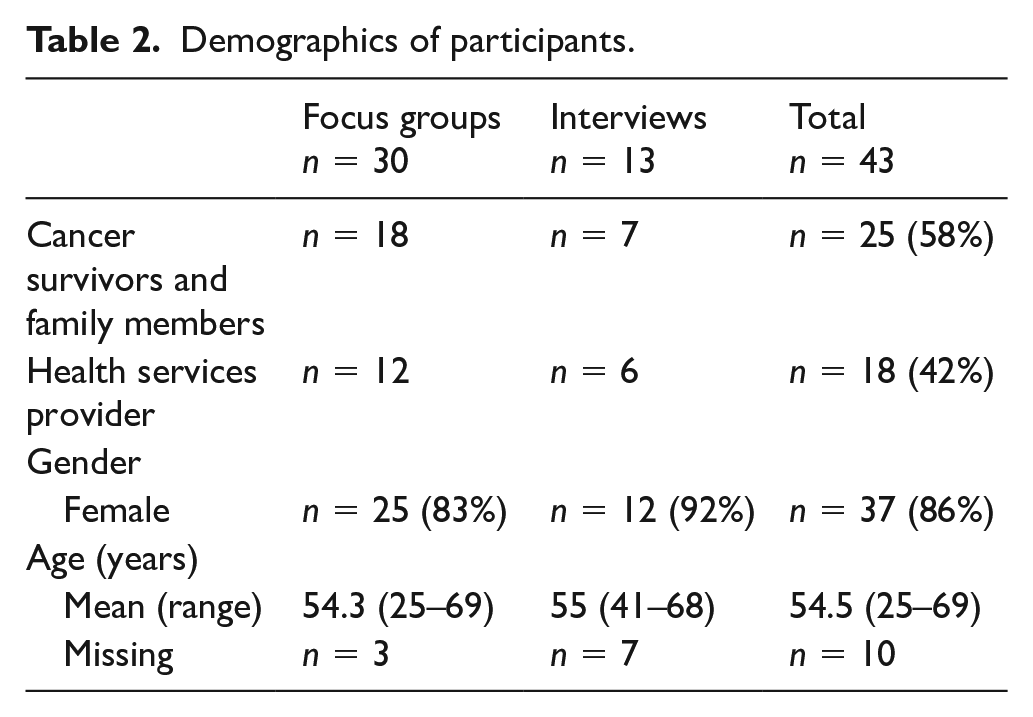
A total of 43 people participated in the study: 25 cancer survivors and family members and 18 healthcare providers. All cancer survivors and family members were First Nations. Healthcare providers included a nurse practitioner, a community health representative, registered nurses, personal support workers, and health services coordinators (see Table 2).
Demographics of participants.
Three overarching themes emerged that encompassed the meaning of culturally safe care for Algonquins of Pikwakanagan First Nation: (a) family and community, (b) culture as healing, and (c) stories for sharing cultural teachings. Each theme had core components considered key to culturally safe care (Figure 1).
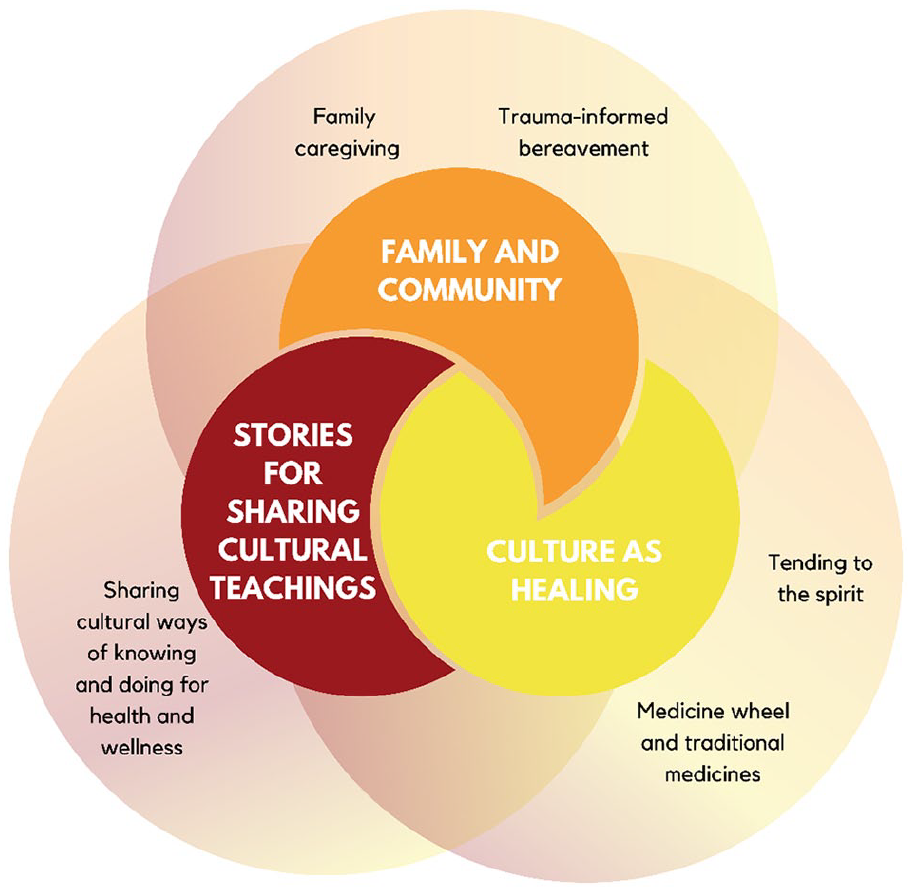
Themes encompassing culturally safe care.
Family and community
For participants, family was described as a complex network of people, relations, and connections that does not correspond to settler conceptualizations of the nuclear family: I don’t think they [settler healthcare providers] understand our family orientation, where we’re just not our immediate family; we have extended families . . . there are people that we treat just like brothers and sisters. . . . So they worry about us like brothers and sisters. (PF1, sharing circle, person with cancer or family member)
They described the community as part of their family, so cancer care became a dynamic and supportive community experience: Everybody comes to the home. Like, the house opens up and it’s like everybody’s bringing food and everybody’s, like, talking. And, you know, they’re offering their condolences but even though they haven’t passed away, they’re like, “You know, like, we’re so happy to see you today.” . . . people are always coming, all the time. And this is very normal, like, from, like say, like, eight o’clock in the morning until, like, eight o’clock at night, you know, people just coming in and saying, “Oh, hey,” whatever. They’re asking, like, talking in the living room, they’re talking outside. So it’s quite normal. So family is very strong here and they all rally together when these things are happening and people end up in palliative care as well as their cancer care too. (HCP1, individual interview, female, healthcare provider)
Participants emphasized that community members were part of their family, and that the provision of culturally safe care involves healthcare providers respecting and accommodating large groups of people: Understanding that when 30 people show up at the hospital wanting to be seen, that they all get a fair chance to see you. I know when I was in ICU, I had 30 people waiting for me . . . people would drop off tobacco ties for me, they dropped off little prayers, those little things for me, and this is what people feel they need to do. (PF2, sharing circle, person with cancer or family member)
Family caregiving: Participants emphasized the integral role family has in caregiving for care to be culturally safe. This was described as both a traditional practice and one that community members were returning to, particularly in the home. Family caregivers were described as assisting people with cancer navigate the healthcare system, communicate with professional healthcare providers, manage appointments and medications, and coordinate transportation. Although it was “emotionally, physically, mentally . . . exhausting”, (PF6, individual interview, female, person with cancer or family member) it was considered a prominent aspect of traditional community caretaking: My dad spoke of that in the old days. He referred to “the old days” when in the old days, they looked after their family member, whether they were trained or not, they just looked after them. And that’s really evolved over the past century, I find, even more so now, . . . So, traditionally, on the traditional side, it’s almost like history repeating itself . . . and when we had the health team come in, that’s where the connection was made . . . they broke bread with us, they had coffee with us, they went and held my father’s hand and held theirs. And it was the same with my mother. So I think, on the Algonquin side of it, for the traditional ways, I think it’s much more comfortable and easier for the person to transition from this plane to the next when they’re in their own comfort zone with family. (PF3, individual interview, female, person with cancer or family member)
Caregiver participants emphasized their desire to be involved in all aspects of care, but often felt too proud or unsure how to ask for help, despite being pushed beyond their limits: We took it upon ourselves, as family, to take him to all his . . . appointments, not using the medical transportation or so forth. And it was, it was, I guess, challenging . . . he was a bigger man, to get him out of, like, his wheelchair and back into the car and, I think that maybe we should have asked for supports, or maybe those supports could have been, like, pushed on us a little more, to be like, like, “Is it safe?” Like, “Are you guys able to do this?” (PF4, individual interview, female, person with cancer or family member) Healthcare providers also described their relationships with community members and the close connections that reinforced their unique aspects of care: I had to go out to community events and be part of the community and seeing everything. That’s something I would never do in mainstream. (HCP1, individual interview, female, healthcare provider)
Trauma-informed bereavement: Participants emphasized that bereavement around a cancer diagnosis or death can trigger past trauma from the legacy of abuses, violence, and harms of colonization. As part of culturally safe care, participants described the need for healthcare providers to understand the compounding effects that cancer has on First Nations community members because of past and ongoing traumatic experiences: And then when things became a challenge, he would draw on those experiences because he was a Native person and he was discriminated quite a bit . . . on this reserve and how they were treated and how he had to go to school here, ‘cause there used to be a school . . . he’d be in trouble all the time . . . ‘cause he hated it . . . but he also knew that he wasn’t going to tell that teacher, but he couldn’t stand the nuns, right. ‘cause the nuns ran it—nuns were mean. (HCP1, individual interview, female, healthcare provider)
The extent of loss that many family caregivers and healthcare providers had experienced in the community was discussed as a trigger for vicarious trauma: We need to start looking at the vicarious trauma. We’re picking up a lot of these feelings because we’ve had so many deaths in the community over a short period of time. We had 17 deaths since February in the community, out of those, four were sudden deaths, 13 were palliative care and then 11 had end of life care. So that’s a lot of deaths to handle. (HCP2, sharing circle, healthcare provider)
Participants described the permanent presence of intergenerational trauma in the community and the challenges of supporting family members through their cancer journeys while experiencing the accumulative effects of ongoing traumatic events including cancer diagnosis: Vicarious trauma is something that we have to be a little bit more realistic with. We always said it was there, it’s just a matter of how much are we experiencing now. (HCP2, sharing circle, healthcare provider)
Culture as healing
While participants described the negative impact of colonization on the lives of First Nations People, many discussed how their traditional cultural values, beliefs, and practices had strong, affirming, and healing effects on cancer survivors. As discussed, broad definitions of family are an essential aspect of First Nations culture. Thus, community and family are key components of traditions that support healing: We have a loss of culture due to . . . residential school and . . . sixties scoop . . . one thing that we held onto when my uncle was dying was that family togetherness, that family support . . . it was loud and the kids were running around, and they were going up and asking him questions, and that’s what it was like every single day. It was just the family togetherness . . . it was so important for him. (PF4, individual interview, female, person with cancer or family member)
Medicine wheel and traditional medicines: Participants reported that culturally safe care for their community incorporated caring for the spiritual, emotional, mental, and physical aspects of health found within the medicine wheel: If you believe in the medicine wheel, everything is in balance. And if you don’t deal with all parts of it, the physical, the emotional, the spiritual, the mental . . . if you don’t deal with all of that, then you’re not dealing with the whole illness. (PF2, sharing circle, person with cancer or family member)
Many participants described the importance of understanding and accommodating First Nations people’s use of traditional medicines to holistically heal in their cancer journey: I think there’s a misunderstanding of what Aboriginal medicines are . . . people will drink Chaga tea and that’s off the Birch bark tree. It’s the moss that grows on the Birch bark tree and they make tea out of it . . . and I think we share stories about our medicines and all that. And I think that was misconstrued with regards to prescribing medicines. We’ve got to take that into consideration, it’s the client’s choice and what they want to do. (HCP, Sharing Circle)
Tending to the spirit: Ceremonies and cultural practices like smudging; laying down tobacco, cedar, sage, or sweet grass; lighting a sacred fire; or drumming were considered “treatments” in the cancer journey. Many of these practices were described as important for people to tend to the spirit and connect with their creator, purify and cleanse their soul, and prepare themselves to transition into another life: There’s a fire that’s made, immediately, and that fire burns for so many days, until the person makes their final journey. So that fire never goes out . . . like, when [redacted name] passed . . . we had rain, we had hail, we had everything, but the boys, like, each person that tended the fire made sure that it never went out, and that’s a very strong traditional thing . . . So that’s what that’s for. It’s . . . an Algonquin thing. It’s a Native thing. (PF3, individual interview, female, person with cancer or family member) She was satisfied that she received the prayers. It gave her peace. And her son was doing the smudging, which helped her, she said, kind of helped her get her soul ready. (PF5, individual interview, female, person with cancer or family member)
Participants reported that cultural practices gave them “peace of mind and a sense of empowerment to continue the journey” (PF6, individual interview, female, person with cancer or family member). These practices were described as distinct and unique to their First Nation: That’s the kind of things that they wouldn’t get from a mental health counsellor. They wouldn’t understand that because our way of doing things is totally different. The way our ancestor did everything it was, it’s totally different. . . . I do the spiritual part. And sometimes that’s the biggest part, getting that positive energy to stay positive. (PF2, sharing circle, person with cancer or family member)
Although cultural practices within hospitals are beginning to be incorporated at a systems level, healthcare providers must still be knowledgeable about First Nations cultural beliefs and practices.
We had some resistance when it comes to ceremonies, but we actually worked through that because I think that they just need to be reminded that they, under the Hospital Act, that they have to provide space for ceremony. So we had worked with the [redacted name] hospital, to create a smudge policy that’s going to be rolled out across the [redacted name] region to involve the hospitals so that those ceremonies could occur. (Person with cancer/Family, Sharing Circle) But I also think that maybe even just education on Aboriginal beliefs and culture would be great if they had that part of the programming . . . ’cause we’re dynamic and different. (PF1, sharing circle, person with cancer or family member)
Stories for sharing cultural teachings
Stories were described as a valued form of communication for sharing cultural teachings about health and healing.
Sharing cultural ways of knowing-and-doing for health and wellness: Participants explained the importance of stories for sharing cultural ways of knowing-and-doing about health and wellness with healthcare providers and community members so they can understand cancer care priorities and healing practices: “Sharing the story is probably what’s most important. And so that’s what we can learn from each other and communicate” (PF1, sharing circle, person with cancer or family member). Stories were described as foundational to upholding individual and community-based values and knowledge in healing that were integral to culturally safe care: He [my dad] had lots of things to offer people and he had all kinds of stories. But now the stories are gone, . . . people who are passing away . . . have so much to share . . . and that could be something that we could be asking them, like, “Do you remember what it was like a long time ago when they had the train coming through here?” . . . and then you’re also helping them out through their journey and then . . . their family’s journey and the community’s journey. (HCP1, individual interview, female, healthcare provider)
Barriers to experiencing culturally safe care
Our participants identified salient barriers to experiencing culturally safe care: (a) hospital visiting policies; (b) lack of well-connected services between and within hospital and home; and (c) systemic racism.
Hospital visiting policies: Hospital policies typically limit the number and relations of people who can visit patients while hospitalized. Our participants identified that this practice does not reflect First Nations people’s concept of family and is therefore a barrier to culturally safe cancer care: The staff, like, they didn’t want everybody in, just two visitors, but we said, no, that’s not how we work. We’re First Nations and everybody wants to be there supporting each other. (HCP3, individual interview, female, healthcare provider)
Lack of well-connected services within and between hospital and community: Participants reported that community members were typically unaware of resources and services linking healthcare services within the community and the hospital, and vice-versa. Adding to the already existing burden was the arduous process of accessing the federal government’s non-insured health benefits that cover the financial costs of services not covered by provincial health insurance such as medical transportation, prescriptions, medical supplies, and equipment (Government of Canada, 2022). Limited resources and support to understand and apply for the services, and at times misinformation, created frustration and significant barriers for community members to have culturally safe transitions in care throughout their cancer journey: When [redacted name] had called for medical transportation for her papa, she was told that he had to utilize First Nation transportation. So, there was misinformation . . . I had to be a little bit cross with non-insured and be like, “No, this person has the right to take her papa down.” And if she didn’t know that and if it wasn’t questioned or rebutted then she would have just drove him down and not got that financial support. It was misinformation from the non-insured health benefits. Because it wasn’t true. And I actually said, like how many people have you told this to? (PF7, sharing circle, person with cancer or family member)
Participants described how western healthcare providers did not seem to understand First Nations Peoples’ capacity or desire to provide care in their communities. One family caregiver in the sharing circles reported a family member who “want[ed] to come home and die at home and the doctors are telling ‘no,’ trying to advise against it when they just want to be in their comfortable space and good environment” (PF2, sharing circle, person with cancer or family member). Participants perceived that prolonged hospitalizations were due to a lack of trust between themselves and western healthcare providers as well as a lack of awareness on the part of healthcare providers regarding services and resources in the community. Participants explained they continually had to advocate or fight to bring community members back home for care once they were hospitalized: The doctor at that time was really trying to say well, you know, if he’s going to go home, he’s only going to last a few days and he’s not going to have the care with the IV and the medication . . . we would tell the doctor and the palliative care team that we could offer [this care] where the client would come home—we’d have the hospital bed set up, we’d have the personal support workers . . . and then us as nurses or registered nurses, we would be on call for the PSW [Personal Support Worker]s. And then we had to tell them about for transportation, because he had to come home by ambulance. (HCP3, individual interview, female, healthcare provider)
Most participants described the processes for services between hospital and home—from diagnosis to treatment to survivorship—as slow and disconnected, jeopardizing patients’ and families’ physical and mental well-being. Most participants believed that hospitals in the city do not trust the care that is done outside the city hospital: We do find people experience their primary care differently when it comes to cancer treatments, or cancer care initially, or in their first diagnosis and that. So some people are going through a full gamut of testing, only to have to repeat it when they get down to [redacted city]. So it kind of stalls the referral processes. (HCP2, sharing circle, healthcare provider)
Racism: Participants expressed the presence of harmful stereotypes and lack of sensitivity and respect by healthcare providers as contributing to systemic racism towards First Nations People which was an ongoing barrier to culturally safe care. Healthcare providers in the community revealed many First Nations People had experienced people negatively judging them because they were Indigenous and thus were reticent to go to hospitals or see western healthcare providers because of the way they were treated: I’ve heard negative comments as well from some clientele that have had to stay in hospital, and then not only that, the judgement against First Nations People for drug-seeking or you know they felt almost neglected because of their culture. . . . So that’s why patients want to come home so that they get better care and they’re in their own home and they have their family taking care of them. (HCP4, sharing circle, healthcare provider) They’re scared and some people just don’t go to doctors. They could be in their 60’s and 70’s right now and they just don’t go to doctors unless they’re really, really, really, sick. (HCP3, individual interview, female, healthcare provider)
Cancer survivors similarly felt that there was prejudice against them because they were Indigenous: “I found that there was, I guess you could say, prejudice-prejudism there. And they’d leave you alone, like that’s what my experiences have been” (PF8, individual interview, female, person with cancer or family member).
Discussion
This study explored the meaning of culturally safe cancer care for Algonquins of Pikwakanagan First Nation and revealed obstacles to receiving culturally safe cancer care in western healthcare systems. Our findings reveal that the meaning of culturally safe cancer care for our participants was complex and nuanced but centred around culture and family. Our findings also showed that cancer care for First Nations People can be fraught with racism, and with the compounding legacy of colonization, often triggers trauma responses. While racism typically manifests interpersonally between patients and providers, it reflects larger systems issues such as the disconnect between community and hospital services described by our participants. Nurses, healthcare providers, administrators, and staff have an integral role to play in deconstructing these interpersonal and systems-level issues to effect meaningful change in the lives of Indigenous cancer patients.
Culture as healing
Many participants reported they used cultural knowledge and practices during their cancer journey to create a social context and relationality which supported their cancer healing. In this study, cultural knowledge and practices included a broad conceptualization of family and caretaking of caregivers; both these aspects were central to community wellness and individual healing. As described by Horn-Miller (2016), Indigenous histories and practices have been distorted, obscured, and corrupted to the point that many people don’t remember their significance, meanings, and teachings. In addition, the violent practices at residential schools taught Indigenous children to “see themselves through the eyes of white disapproval . . . disconnecting . . . from their language, culture, and their communities and also, but most painfully, from their own sense of identity as being Indian” (Horn-Miller, 2016, pp. 49–50). Indigenous scholars emphasize that reclaiming cultural practices is not about returning to a nostalgic Indigenous past. Rather, it involves reclaiming Indigenous knowledge and practices to make sense of the present, provide affirmation, pride, and dignity, and heal the body, mind, and spirit (Altamirano-Jiménez & Kermoal, 2016; Battiste, 2000; Jobin, 2016). Even if distorted and reconfigured to a contemporary context, cultural traditions, and practices can be important elements of culturally safe care in the cancer healing process for First Nations People.
Stories for sharing cultural teachings
An essential aspect of culturally safe care is stories for sharing cultural ways of knowing-and-doing among First Nations people in healing and wellness. Stories were central for participants to understand their cancer journey and identity as First Nations People. When unwell or displaced from their homes with cancer, stories can serve to remind cancer survivors and family members where they belong, offering a sense of identity for healing the body, mind, and spirit (Horn-Miller, 2016). Storytelling is also a powerful way for healthcare providers to understand First Nations Peoples’ history, cultural, and spiritual beliefs, and can strengthen relationships in the provision of care (Chan, 2021). Stories are a way of privileging Indigenous knowledge about health and healing, reinforcing the interconnections among the social, political, spiritual, and natural aspects of life (Altamirano-Jiménez & Kermoal, 2016; Jobin, 2016). Despite the awareness that healthcare must be culturally safe, little attention has been given to how Indigenous knowledge and stories can contribute to the processes of cancer care.
The colonial project concertedly sought to erase Indigenous knowledge, culture, and practices by disqualifying them as illegitimate and dangerous. In a letter in 1921 by Duncan Campbell Scott, the Minister of Indian Affairs in Canada between 1913 and 1932 who oversaw amendments to the Indian Act that mandated residential school attendance for all Indigenous children, he decries how “dances by Indians on their reserves is increasing” (para. 1), declaring “Indian dances” as “demoralizing amusements” (para. 2) and directing the Government’s representatives on First Nations reserves, known as Indian Agents, to end them “By the use of tact and firmness, you can obtain control and keep it, and this obstacle to continued progress will then disappear” (para. 3) (Martell, 2017; C. Smith, 2017). It is important to note how Duncan refers to Indigenous practices as obstacles to progress. Progress in this context refers to the enlightenment ideal of reason and a capitalist economy, which materializes in, for example, the scientific method and classical liberalism. The settler state justified the suppression of Indigenous knowledge by deeming it irrational, thus anti-scientific, and justified the extraction of land which is central to Indigenous life, under the imperative of a capitalist economy; this conceptualization of progress overtly disqualifies any Indigenous knowledge. Contemporarily, Indigenous knowledge is often considered at the bottom of the scientific hierarchy of evidence, exemplifying how these beliefs about Indigenous knowledge persist (Kincheloe & Steinberg, 2014; Moreton-Robinson, 2013). In our study, participants revealed how stories are an essential means of re-establishing subjugated and disqualified knowledge about cancer healing and survivorship. These historical knowledge of struggles can support cancer healing and underscore the importance of stories and other forms of Indigenous knowledge as legitimate forms of evidence.
Racism
Participants in this study experienced racism through stereotyping, lack of trust, and lack of services and supports that value First Nations People with cancer. Based on their race and affiliation(s) leads to stereotyping and perpetuating marginalization (Burns & Shor, 2021), participants discussed how many of the stereotyping perceptions that western healthcare professionals have about First Nations People, such as seeking drugs under the guise of illness, prevent them from interacting with the health system. As mentioned, although this form of racism is experienced at an interpersonal level, it is directly linked to the social, political, and economic arrangements instilled through colonialism. These arrangements create and perpetuate structural violence and inequalities, many of which are invisible, resulting in unsafe healthcare practices that jeopardize Indigenous People’s health (Farmer et al., 2006).
Our participants perceived prolonged hospitalizations as an obstacle to culturally safe care, which they attributed to western healthcare providers’ lack of awareness and understanding of services and resources within the First Nations community. Participants explained they continually had to fight to bring their family members home to their communities following a hospital admission. In and of itself, this can trigger trauma both for patients and family caregivers, given its similarity to the forcible removal of Indigenous People—many of whom were children—from their communities under the residential schools system or for the screening and treatment of tuberculosis (Hick, 2019). This disconnect between community services and hospitals is an example of the dichotomy between healthcare for settler Canadians and Indigenous People. It ignores aspects of Indigenous health and healing that do not fit into the status quo of the healthcare system, and is consistent with a recent scoping review that found many barriers to cancer care for Indigenous people are embedded within political, social, and economic structures of the healthcare system, but are framed as individual issues of the patient or practitioner (Horrill et al., 2019). The framing of structural barriers as individual problems suggests a lack of understanding of the link between systemic racism and discrimination in the healthcare system with access to culturally safe care and services as was described by participants in our study.
The grief, trauma, and losses Indigenous People experience through cancer have a complex impact on both people with cancer and their community members. Described as trauma-informed bereavement, participants emphasized that a diagnosis of cancer, sickness, or death from cancer can trigger other forms of trauma accumulated from colonial practices including the Sixties Scoop (Sinclair & Dainard, 2016) and residential schools (Larocque et al., 2021). L. T. Smith (2012) described how colonial governments “established systems of rule and forms of social relations which governed interactions with the indigenous peoples. . . . The moral justifications . . . continued ill-treatment of indigenous peoples even today” (p. 27). The cumulative effect of intergenerational trauma is powerful and influences the experience of cancer care for Indigenous People. Trauma-informed bereavement builds upon approaches such as trauma-informed care, which includes understanding the intersectional nature of colonial violence and inequity, and the devastating effects this has had on Indigenous People (Horrill et al., 2020).
The questions we ask can either reify or challenge the settler colonial project. For example, contextualizing Indigenous health outcomes in terms of improving quantitative metrics or cost savings perpetuates the colonial emphasis on a market economy and efficiency; in other words, it still conceptualizes Indigenous Peoples as a problem that needs fixing. While hospitals are beginning to incorporate Indigenous cultural practices at a systems level, cultural safety demands transforming the physical structures, values, beliefs, and discourses that have prevailed in healthcare since colonization (Gifford et al., 2022). Simply recognizing Indigenous People as a diverse group within a settler healthcare system furthers colonialism by reinforcing the idea of the white saviour, or what Tuck and Yang (2012) describe as settler moves to innocence. White saviourship is the theoretical flipside of white guilt; settlers feel white saviourship when they start to understand the conditions the colonial state has created for Indigenous People. Moves to innocence denotes how despite efforts to adopt decolonizing rhetoric, this rhetoric often strips away the deeper meaning of decolonization, reducing it to tokenism—for example, smudging in a hospital—and undermining authentic relationships, instead attempting to “reconcile settler guilt and complicity, and rescue settler futurity” (Tuck and Yang, 2012, p. 3). Therefore, it is important to emphasize culturally safe care is not about amplifying the precise traditional practices and ways of life of Indigenous People. Rather, it involves turning inwards and examining our practices to deconstruct and change them at both the individual and systems levels. It means shifting from recognizing healthcare professionals as the sole holders of legitimate knowledge about health and healing and being willing to give up the privilege inherent in being a settler. Only then can a new way of understanding and envisioning the world emerge.
Strengths and limitations
A strength of this study was that knowledge was co-created in a deeply collaborative partnership process with community members and represents views grounded in their lived experiences. Therefore, while some findings can be extrapolated to other First Nations communities in Canada, one of the limitations is that results cannot be generalized without further research. A second limitation is that research partners from Pikwakanagan health team recruited participants, potentially resulting in selection bias; however, the large diverse sample helped to mitigate this. Last, as a team of Indigenous and non-Indigenous researchers, we recognize our research processes were not based in Indigenous epistemology per se. However, our Indigenous community partners were instrumental in every stage of the knowledge creation process and their perspectives were privileged analysing and interpreting the data.
Conclusion
Culturally safe care has emerged as a solution to address the problem of racism and inappropriate healthcare for Indigenous Peoples in Canada. Our study revealed the meaning of culturally safe care for Algonquins of Pikwakanagan First Nation and has important implications for reimagining how care is conceived and operationalized in the current healthcare system. While the concept of culturally safe care has largely focused on individual interactions between patients and non-Indigenous healthcare providers, the discussion must extend to the broader political, social, and economic issues that continue to perpetuate inequalities in health and healthcare. Although our study is grounded in the expertise of community members, it is unclear how this knowledge can be integrated—or not—into a healthcare system founded on racism, discrimination, and genocide. Further research is needed for health system change to dismantle the systemic and structural factors that make cancer care unsafe and continue to harm Indigenous People today.
Footnotes
Acknowledgements
We acknowledge the valuable contribution of our community partner organization, the Pikwakanagan Health Services and Family Health Team (Minopimàdiz-i Gamik), as well as the members of the Pikwakanagan community who participated in this study and generously shared their stories with us. We also acknowledge the work of Danielle Rolfe and Kublacom Pictures Inc who video-recorded and developed the documentary film portion of this study.
Authors’ note
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This study was funded by the Ontario Ministry of Health and Long-term Care Health System Research Fund Call for Targeted Research in Nursing, Grant #417.
Glossary
Algonquin First Nations People from Eastern Canada
chaga a moss found on the Birch bark tree, from which a tea of the same name is made
Māori Indigenous People of New Zealand
Pikwakanagan an Algonquin community in Renfrew County, Ontario, Canada
Minopimàdiz-i Gamik Healing House; the Algonquin name for the Pikwakanagan Health Services and Family Health Team