
Abstract
Cultural safety is a decolonizing and transformative approach to health care aimed at achieving health care that recognizes, respects and nurtures the needs, rights and identities of Indigenous peoples. Such a transformation requires new or radically reimagined professional roles. Based on a rapid review design, this synthesis aimed to identify fundamental characteristics of cultural safety interventions that involved the creation or transformation of professional roles. The 23 included studies presented three main categories of professional roles for cultural safety. These roles were focused on (a) supporting health care system navigation, (b) providing a new or improved service offering, and (c) building organizational capacity to provide culturally safe health care. Our results demonstrate that cultural safety can be implemented by key actors playing different roles at different levels of the health care organization. These roles should be viewed as complementary to one another and be defined and implemented in partnership with Indigenous partners.
Introduction
In western-colonized countries, health systems are extensions of the colonial enterprise that reproduce and reinforce oppressive power dynamics and exclusionary processes faced by Indigenous peoples. As a reflection of the systemic racism embedded in social institutions, interactions between Indigenous patients and health care providers are often characterized by stigma, discrimination and racism (Allan & Smylie, 2015; Jacklin et al., 2017; Janzen et al., 2017; Paradies et al., 2008; C. Reading & Wien, 2009; J. Reading, 2009; Tang & Browne, 2008; Viens, 2019). Research has demonstrated that patients who experience racism and discrimination when they enter the health care system tend to anticipate interactions with health professionals, underutilize health care services and underreport their symptoms to health professionals (Allan & Smylie, 2015; Tang & Browne, 2008). These barriers contribute to a significant avoidable burden of disease, by increasing the intensity and frequency of crisis situations and delaying screening and provision of care (Allan & Smylie, 2015; Viens, 2019).
Cultural safety is a decolonizing, transformative and participatory approach to health care aimed at achieving health care that recognizes, respects and nurtures the unique needs, rights and cultural identities of Indigenous peoples (Ramsden, 1992, 1993, 2002; Smye et al., 2010). Cultural safety is a radical paradigm shift from other approaches that maintain a focus on the interactions between patients and providers − for example, cultural sensitivity, awareness and competency − because it is based on a politicized understanding of health and of power inequities underlying the health system (Brascoupé & Waters, 2009; Curtis et al., 2019; Mackean et al., 2019). Over the last decades, this concept has gained increasing recognition by professional bodies and associations in Canada and at an international level (Aboriginal Nurses Association of Canada [ANAC] et al., 2009; The Association of Faculties of Medicine of Canada, 2019; The Indigenous Physicians Association of Canada & The Royal College of Physicians and Surgeons of Canada, 2009). There is considerable diversity in the way cultural safety is defined and implemented, with many regulatory and educational organizations framing their understanding of this concept through approaches fostering self-reflection and awareness of power, privilege and biases (Gerlach, 2012; The Indigenous Physicians Association of Canada & The Royal College of Physicians and Surgeons of Canada, 2009). The earliest definition of cultural safety, developed by Ramsden in the 1990s, is built on the idea of self-reflection: “the effective nursing of a person/family from another culture by a nurse who has undertaken a process of reflection on [their] own cultural identity and recognizes the impact of the nurses’ culture on [their] own nursing practice” (Papps & Ramsden, 1996, p. 491). Along the same lines, the Indigenous Physicians Association of Canada conceives of cultural safety as
a state whereby a provider embraces the skill of self-reflection as a means to advancing a therapeutic encounter with First Nations, Inuit [Indigenous inhabitants of the Arctic and sub-Arctic region of Canada], [and] Métis [a culturally distinct group of specific mixed European and Indigenous ancestry] peoples. (The Indigenous Physicians Association of Canada & The Royal College of Physicians and Surgeons of Canada, 2009, p. 9)
Many definitions of cultural safety lead toward critical and reflective educational strategies, placing most of the responsibility for change in the hands of professionals. While critical education and training may play an important role in cultural safety, only systemic transformation of the health system with a genuine aim for decolonization will address the social inequalities of access experienced by Indigenous populations. Such a transformation will require new or radically reimagined professional roles. We make this assertion building on a concept of cultural safety that supports “the application of cultural safety within a healthcare systemic/organizational context in addition to the individual health provider-patient interface; [which would] not be limited to formal training curricula but [would] be aligned across all training/practice environments, systems, structures, and policies” (Curtis et al., 2019, p. 14).
This rapid review synthesizes data from qualitative, quantitative and mixed-method studies describing cultural safety interventions involving new professional roles for different players of the health system. We conducted this rapid review in the context of a larger study in Québec aiming to co-develop a relevant intervention model for cultural safety in the health system. The larger community-based participatory project relies on respectful and mutually enriching partnerships with three communities of the Atikamekw Nehirowisiwok (Indigenous inhabitants of the upper Saint-Maurice River valley, Québec, Canada) (Atikamekw) in Québec, the Council of the Atikamekw Nation, community leaders and Atikamekw health professionals. The Atikamekw are a First Nation of the Anishinaabe (culturally related Indigenous peoples present in the Great Lakes region of Canada and the United States) cultural area, who uphold values such as caring for extended family and community members, respect for Elders, equality between men and women, and a close connection with mother earth (Atikamekw Sipi, n.d.). Before the advent of permanent communities, the Atikamekw practiced a highly mobile, land-based economy grounded in a profound knowledge of the earth and its many inhabitants. The land and knowledge continue to support gathering, fishing and hunting practices that are physically, socially, emotionally and spiritually nourishing. Like many Indigenous peoples, the Atikamekw have unique and specific cultural health practices, traditional knowledge and perspectives on health which are central to their well-being but are often devalued or ignored by western science and medicine (Tremblay et al., 2020). Preliminary work with these partners identified a need for the development and implementation of a new intervention, based on a new set of professional responsibilities, to promote cultural safety in health care organizations where Atikamekw people seek care (Tremblay et al., 2020). This rapid review was conducted to identify similar interventions which could fuel the development of this new intervention model. Although some scoping reviews were conducted to better understand how to apply the principle of cultural safety in health care practice (Brooks-Cleator et al., 2018; Schill & Caxaj, 2019) or to differentiate the concept of cultural safety from cultural competence (Curtis et al., 2019), none have specifically focused on interventions describing the development or transformation of professional roles as a strategy for fostering cultural safety into health organizations.
Methods
Search strategy
A rapid review (Khangura et al., 2012) was chosen as the most appropriate approach for quick synthesis of descriptive information from qualitative and quantitative studies for the purpose of informing decision making within the context of our larger study. The search strategy was developed in collaboration with a librarian and is described using Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Page et al., 2021). The full search strategy is provided in Supplementary Material 1. In the search strategy, we intentionally used a large number of keywords, recognizing that some authors may not differentiate between cultural safety and other cultural approaches. However, in the selection process, we purposely included only interventions aimed at transforming the way care is delivered based on the unique needs and cultural identities of the Indigenous populations, which aligns with the concept of cultural safety.
Data sources
Titles and abstracts were searched in the databases MEDLINE (Ovid), Embase (Elsevier) and Web of Science on January 20, 2021, using a pre-defined list of keywords related to Indigenous, health services, intervention and cultural safety (Supplementary Material 1). As the objective was to obtain a quick overview of the current scientific literature, the reference works cited in the identified studies and related gray literature were not explored.
Inclusion criteria
Publications retained for review met the following criteria:
(a) published within the last 10 years (from January 2010 to December 2020);
(b) written in French or English;
(c) concerned Indigenous peoples or Indigenous populations living in Australia, the United States, Canada and New Zealand;
(d) reported on strategies or interventions aiming to improve cultural safety through creation of a new professional role, that is a new position involving a new set of responsibilities, or the transformation of an existing professional role, that is a health professional performing a new role;
(e) focus on health and social services.
The search strategy was limited to studies published from January 2010 to December 2020. Indeed, while the concept of cultural safety has been discussed in the literature since 1990, interventions to bring cultural safety into practice have only been reported in the literature recently. Furthermore, we limited our searches to studies from Australia, the United States, Canada and New Zealand as these countries share similarities in their history of colonization and health system organization, which ensures a certain transferability of the interventions identified.
Exclusion criteria
Editorials, letters to the editor and secondary data studies were excluded from this review, as were environmental scans of existing interventions, as these did not present sufficiently detailed descriptions. In addition, articles focused on training programs for future health care professionals, describing interventions aiming to improve cultural awareness or cultural competence, or describing factors limiting or facilitating access to health care were excluded from the study.
Study selection
The identified studies were imported into the systematic review software Covidence (www.covidence.org). Two reviewers (G.O.-D., L.G.) were involved throughout the selection process. First, the two reviewers independently applied the eligibility criteria to 10 randomly selected titles and abstracts to ensure that they had a common understanding of the criteria. Next, G.O.-D. selected studies based on their titles and abstracts, and L.G. randomly assessed 20% of them, with 92.2% agreement. Disagreements were discussed and resolved by consensus with a third reviewer (M.-C.T.). Once full texts were accessed, the two reviewers worked together on the reviewing process.
Data extraction
G.O.-D. and L.G. independently reviewed the selected studies and extracted data accordingly. These data were entered into an Excel spreadsheet under the following headings: authors, description of the intervention, and description of the new or transformed role. Regarding the results, in Canada, Indigenous is the accepted term used to refer collectively to the three constitutionally First Peoples of Canada: First Nations, Inuit and Metis. However, in the results, we use the terms used by the authors to refer to their intervention, for example, Aboriginal and Native.
Data synthesis
Results were summarized using a narrative synthesis (Lisy & Porritt, 2016), providing an organized portrait of the data describing the main characteristics of the intervention roles.
Results
Figure 1 provides the complete study selection process. Of the 1,923 articles initially identified, 23 articles met the inclusion criteria for this study. Supplementary Material 2 presents a summary of the data extraction sheet.
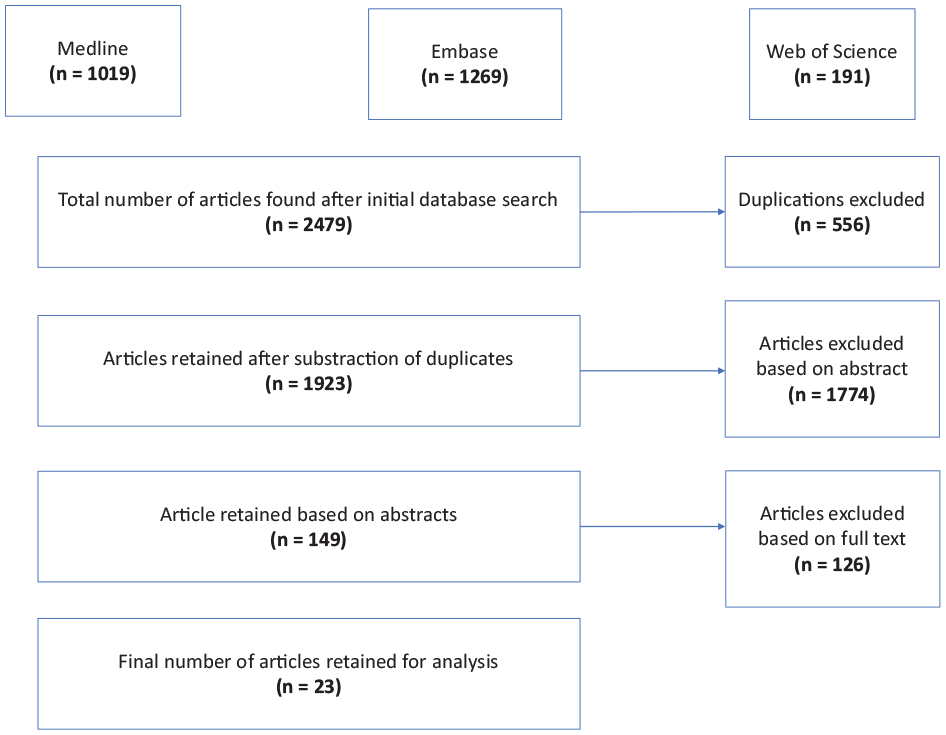
Rapid review flowchart.
From these 23 articles, three main types of professional roles for cultural safety can be identified. These roles focus on (a) supporting individuals and families in the health care system, (b) providing a new or improved service offering, and (c) building the capacity to provide culturally safe health care. Some interventions bring together components that allow them to be associated with more than one type.
Supporting Indigenous people’s access to and navigation of the health care system
We found 13 studies based on diverse designs (Bernardes et al., 2018; Cuesta-Briand et al., 2016; Grimes et al., 2017; Guadagnolo, Boylan, et al., 2011; Guadagnolo, Cina, et al., 2011; Ivers et al., 2019; McKenna et al., 2015; Middleton et al., 2017; Miyamoto et al., 2019; Reilly et al., 2018; Richer et al., 2018; Slater et al., 2016; Smith et al., 2010) describing 12 different interventions to support patient access to health services in Australia (n = 7), the United States (n = 4), Canada (n = 1) and New Zealand (n = 1). For the most part, these interventions were built around the central role of a peer facilitator, often a community member, who supports Indigenous individuals and their families in overcoming the multiple systemic and organizational barriers to health services access. Of these 12 interventions, 7 are specifically aimed at supporting health system navigation in the context of cancer care for Indigenous patients at risk of, diagnosed with, suffering from or surviving cancer (Bernardes et al., 2018; Cuesta-Briand et al., 2016; Grimes et al., 2017; Guadagnolo, Boylan, et al., 2011; Ivers et al., 2019; Reilly et al., 2018; Slater et al., 2016). Other interventions are dedicated to Indigenous families and populations with various or broader orientations, for example, maternal health, family-centered care, geriatric and palliative care, and mental health.
These interventions are largely based on the work of peers, who are identified by different titles: patient navigator (Bernardes et al., 2018; Grimes et al., 2017; Guadagnolo, Boylan, et al., 2011; Guadagnolo, Cina, et al., 2011), community health navigator (Miyamoto et al., 2019), Aboriginal Mental Health Liaison Officer (McKenna et al., 2015), Aboriginal Maternal and Infant Care worker or Aboriginal Liaison Officer (Middleton et al., 2017), family support worker (Richer et al., 2018), Yuendumu Old People’s Programme worker (Smith et al., 2010) or coordinator (Cuesta-Briand et al., 2016; Reilly et al., 2018). While bearing different titles, most of these roles share similar characteristics, and they usually involve one or more Indigenous people from local or urban communities who speak the local language and have a good knowledge of socio-economical contexts and cultural codes.
These mainly non-clinician facilitators take multiple actions to make it easier for individuals to access and use health services. The range of roles filled by facilitators includes, for example, connecting patients with health and social services (Cuesta-Briand et al., 2016; Grimes et al., 2017; Guadagnolo, Boylan, et al., 2011; Guadagnolo, Cina, et al., 2011; McKenna et al., 2015; Reilly et al., 2018; Slater et al., 2016), coordinating appointments for patients (Bernardes et al., 2018; Grimes et al., 2017; Guadagnolo, Boylan, et al., 2011; Guadagnolo, Cina, et al., 2011; Ivers et al., 2019; Reilly et al., 2018), facilitating communication between patients and clinicians (Bernardes et al., 2018; McKenna et al., 2015), resolving insurance issues, following up on test results (Guadagnolo, Boylan, et al., 2011; Guadagnolo, Cina, et al., 2011), following up on patients’ needs and wellness (Middleton et al., 2017) and delivering culturally safe outreach services in the form of home visits (Richer et al., 2018; Smith et al., 2010). In addition, health education and prevention activities (Bernardes et al., 2018; Cuesta-Briand et al., 2016; Grimes et al., 2017; Middleton et al., 2017; Slater et al., 2016), informal needs assessments (Reilly et al., 2018; Smith et al., 2010) and health referrals (Slater et al., 2016; Smith et al., 2010) are common activities put in place by facilitators while they carry out home visits, transportation, accompaniment or meetings. In some cases, facilitators can also advocate for patient rights and system changes (McKenna et al., 2015; Middleton et al., 2017; Slater et al., 2016). These kinds of interventions are put in place by different structures and organizations, such as mainstream health organizations (McKenna et al., 2015; Reilly et al., 2018), Indigenous health organizations (Ivers et al., 2019; Richer et al., 2018; Slater et al., 2016; Smith et al., 2010), partnerships between organizations (Bernardes et al., 2018; Grimes et al., 2017; Guadagnolo, Boylan, et al., 2011; Guadagnolo, Cina, et al., 2011; Middleton et al., 2017; Miyamoto et al., 2019) and community health action networks (Cuesta-Briand et al., 2016).
Providing a new or improved service offering that meets the needs of Indigenous peoples
We identified two interventions providing new services or improving a service offering that involved the transformation or creation of new professional roles. These interventions took place in Australia (Caffery et al., 2018) and in Canada (Drost, 2019); they were dedicated to Indigenous patients with mental health disorders (Drost, 2019) or Indigenous patients at large (Caffery et al., 2018). The new roles at the center of these interventions were an Indigenous health professional with an expanded role (Caffery et al., 2018) and an Indigenous Elder who offered spiritual guidance and enabled traditional health practices in a clinical setting (Drost, 2019). Both interventions were put in place following the establishment of partnerships between a mainstream health organization and an Indigenous health organization.
The intervention described in Caffery et al. (2018) built on telehealth to provide access to culturally appropriate consultations. Through telehealth, consultations took place in a familiar and safe environment and were facilitated by an Indigenous health professional who spoke the same language as the patient and shared the same cultural background. Part of the Indigenous health professional’s expanded role was to draw attention to the social determinants of Indigenous health so that other health professionals involved in service delivery could better address them. Resources required to put this intervention in place included infrastructure for telehealth, financial, human and logistical resources (Caffery et al., 2018).
The intervention featured in Drost (2019) focused on providing holistic health care in combination with western medicine. Traditional health practices, including spiritual rituals, were offered by an Indigenous Elder within the health organization to Indigenous patients, staff and community members. This intervention relied on specific resources for spiritual rituals, such as a ceremonial room or sacred space, as well as cultural competency training for the staff. It also involved mobilization of Elders and development of meaningful partnerships between Indigenous community leaders and institutional stakeholders (Drost, 2019).
Building capacity to provide culturally safe health care
Three studies described interventions with roles focused on building professional and organizational capacity for cultural safety in Australia (Abbott et al., 2014) and in Canada (Browne et al., 2018; Browne et al., 2016). Unlike other types of intervention roles, these roles were oriented toward the organization and its staff, rather than toward patients. The first role involved a cultural mentor who offered mentorship, cultural safety education and training to general practitioners and registrars, in order to increase their awareness of local history, patient backgrounds, community resources and networks (Abbott et al., 2014). This intervention aimed to promote cultural safety and improve communication between Aboriginal patients and non-Aboriginal staff. Cultural mentorship from Aboriginal members to non-Aboriginal health care professionals was a crucial aspect of the approach. A second intervention presented in Browne et al. (2016) consisted of integration of Indigenous Elders as part of the health care team. This intervention involved educating healthcare professionals about the pre-colonial and colonial background of the communities served, as well as fostering adaptation of health care according to the specificities and needs of the communities. Part of the role of the Elders was to encourage inclusion of Indigenous knowledge and language in health care (Browne et al., 2016). Another intervention presented in Browne et al. (2018) involved a practice consultant coordinating an employee education program over a period of 8–12 months. In association with staff training, the practice consultant supported staff and leaders in the development of an organizational integration and tailoring process. This approach aimed at enhancing organizational capacity to provide equity-oriented health care, by reducing the effects of structural inequities, the impact of multiple and intersecting forms of discrimination in relation with care services, as well as mismatches between dominant way of providing services and the needs and realities of people affected by health and social inequities.
All these interventions involved multiple strategies at different levels of action. For instance, all the capacity building interventions were comprised of training, orientation and continuing education. In addition, recruiting, supporting and retaining more Indigenous health care professionals was a core complementary strategy. These interventions followed different models but were all based on social justice ideals and collaborative models of governance. In Browne et al. (2016), the explicit commitment to equal partnerships and the development of internal structures and processes to support this commitment were presented as the starting point for organizational capacity building. A collaborative model of organizational change that promotes cultural safety in care was identified as the driver of change in Abbott et al. (2014) and Browne et al. (2016). Partnerships between health care teams and Indigenous communities were considered to be central in all of these interventions.
Mixed interventions
Five studies (Hadjipavlou et al., 2018; Hickey et al., 2019; Joe et al., 2016; Medlin et al., 2014; Taylor et al., 2020) described interventions with mixed characteristics of the different categories presented above. These interventions were conducted in Canada (Hadjipavlou et al., 2018), Australia (Hickey et al., 2019; Medlin et al., 2014; Taylor et al., 2020) and the United States (Joe et al., 2016). They aimed to provide culturally safe health services to Indigenous patients with mental health issues (Hadjipavlou et al., 2018), Indigenous mothers and their babies (Hickey et al., 2019), Indigenous patients seeking primary care (Joe et al., 2016), Indigenous children and adults with respiratory illnesses (Medlin et al., 2014) as well as cancer care patients (Taylor et al., 2020). These interventions combined service-centered roles, capacity building and navigation roles. They involved, for example, Indigenous Elders providing cultural services such as one-on-one visits, education sessions or consultations, and cultural teaching circles and ceremonies (Hadjipavlou et al., 2018); Indigenous Family Support Workers providing pre- and post-natal care and offering cultural and logistical support to patients (Hickey et al., 2019); and Indigenous health workers assisting patients and their families while providing cultural diagnostic services, ceremonies, patient education and in-service training for hospital staff (Joe et al., 2016). In these interventions, in addition to patient navigation, Indigenous staff provided new services and were fully integrated into the health services and health care teams where they were deployed. In the case documented by Hadjipavlou et al. (2018), for example, Elders worked in direct partnership with the primary care team, participated in clinical rounds and shared access to the patient’s digital medical records at the clinic. The integration of these Indigenous workers allowed the addition of traditional medicine services within existing facilities (Hadjipavlou et al., 2018; Joe et al., 2016). Another interesting, but different, intervention featured in Medlin et al. (2014) involves traveling multidisciplinary teams including Indigenous project officers, which provide respiratory outreach services in communities. The consultation strategy involves sitting in the street in the community and yarning with people walking past, performing clinical assessment with portable diagnostic tools, and providing referrals. While focused on service offer, this intervention also involves two-way learning between local Indigenous workers and multidisciplinary teams about community protocols and practices, thus building provider and team capacity. A final study (Taylor et al., 2020) describes interventions involving Indigenous Liaison Officers, managed by Indigenous Health Units, in a “whole of service” approach in the context of cancer care (p. 3). The Indigenous Liaison Officers, who act as care coordinators, are an integral part of the multidisciplinary care team. This intervention is supported by a range of strategies at the organizational level, including strong executive leadership and commitment to cultural safety, a proactive employment and recruitment strategy, professional development opportunities, and a supportive work environment characterized with respect for Indigenous cultures (Taylor et al., 2020).
Discussion
From these results, it appears that cultural safety can be articulated through different categories of roles. One such category is that of the facilitator or navigator that helps patients and their families to access existing health and social services. This role is most often assumed by an Indigenous lay navigator, but may also be performed by a health professional or a team. While allowing a change at the interface of the health system, the patient navigator model has been criticized for its mainly unidirectional focus, since it aims to reduce logistical and individual barriers to access to care − in short, to facilitate patients’ adaptation to current services − without allowing for real transformation of the system or genuine consideration of the social inequalities of access to care (Carter et al., 2018; Thorne & Truant, 2010; Wells et al., 2008). So far, there is no recognized certification program for this type of role, and the role has been carried out with varying degrees of success and efficacy (Wells et al., 2008). In addition, the performance of this type of role is often dependent on a particular individual’s profile, which may affect its sustainability over time. The development of a standardized scope of practice and the formalization of harmonized core competencies for the training and certification of health navigators are thus central issues. Moreover, in an urban context where members of different communities consult each other, this type of intervention requires multiple navigators to respond to the diversity of the clientele.
A second category of role revolves around a new or expanded service offering. These services often aim to better meet the needs of Indigenous patients by supporting a more holistic perspective of health by integrating ceremonies or facilitating traditional health practices, or by making an existing service more culturally safe and sensitive with the help of Indigenous professionals. However, it must be kept in mind that cultural safety cannot be achieved based on service add-ons alone; these transformations of health services must be accompanied by collective changes in values, mind-sets, organizational practices and health policies. Thus, this type of role raises issues related to the integration and recognition of these new practitioners within existing care teams. Beyond a broader vision of interprofessional collaboration, this requires organizations to formally recognize these individuals as professionals in their own right. In fact, cultural safety requires more than a simple adaptation of practices; rather, it calls for deep organizational change processes (Gerlach, 2012; Smye et al., 2010).
A third category of role for actualizing cultural safety focuses on building the capacity of various actors within health organizations. Thus, with the organization as the target, this type of role is radically different from those that are more patient-oriented. In this category, Indigenous mentors, Elders and consultants are engaged to provide education or in-service training to health professionals, as well as cultural mentoring or pilot processes to review organizational norms and culture. This role implies an openness and commitment to cultural safety as an organizational value, which is not always obvious as it can interfere with competing agendas and values (Oelke et al., 2013). Most of the interventions in this category involve different level strategies, a factor highlighting the positive effect of an organizational buy-in to cultural safety, as this commitment translates into an organized set of policies, practices and activities. More importantly, they are all based on a central partnership with an Indigenous organization or community.
Based on the results of the present review, it is clear that cultural safety requires the integration of key players performing roles at different levels of the health care system: first, at the interface of care, in order to support improved navigation of existing services by Indigenous individuals and families; second, at the service level, to develop services that better meet the needs of patients and communities as well as professional practices that allow for greater openness and consideration of Indigenous realities and values; and third, at the organizational level, to develop the capacity of organizational actors to implement systemic changes that support cultural safety. In turn, for these roles to be integrated into health care organizations, cultural safety is a key issue. Paraprofessionals, as they are sometimes called, are often left out of health care team, which demonstrates a misunderstanding of their roles, lack of confidence in their abilities and reproduction of power differentials underlying the health system (Oelke et al., 2013). Cultural safety implies that all the people involved in health care delivery or organization should be recognized and valued. This can be done through a process of reflection on professional cultures, recognition of difference and attention to potential power differentials among professionals. In order to achieve cultural safety, team members must actively assess inequalities within the team and find solutions through team discussions to address power differentials and colonialism in health care (Oelke et al., 2013).
Systemic transformation underpinned by cultural safety typically involves changes at the patient–provider interface, in organizations and in structures. In this review, we identified new or upgraded professional roles that enable action at different levels of the health care system in a complementary and cross-cutting way. In this sense, each of the role categories is not necessarily sufficient in itself, but taken together, they participate in a more comprehensive approach to cultural safety. This could explain why a number of identified interventions (n = 5) present a varied mix of new or improved roles.
Limitations
This review of interventions aims to describe cultural safety interventions involving new professional roles for different players of the health system. As a result, many articles included in this review, which are descriptive in nature, did not report on the outcomes of these interventions. This does not allow us to assess the effectiveness of the various roles in promoting cultural safety. Future studies would benefit from comparing and investigating the effectiveness of different roles in fostering cultural safety for Indigenous patients.
Another limitation stems from the boundaries established by our search strategy. We deliberately sought out recent interventions involving Indigenous populations in Australia, the United States, Canada and New Zealand, because we wanted to identify interventions that could inform the development of an intervention model relevant to our project. However, cultural safety is a relevant concept for thinking about the power dynamics that affect access to care for other types of marginalized populations that experience discrimination or exclusion, such as immigrants, racial minorities and gender diverse communities. This has already been pointed out by other researchers (Kellett & Fitton, 2017; Osei-Twum et al., 2019). Future reviews on this topic could be more encompassing by including other types of marginalized populations.
Conclusion
Cultural safety requires a radical paradigm shift from other approaches that maintain a focus on the interactions between patients and providers such as cultural competency, because it is based on a politicized understanding of health and of racial power inequities (Brascoupé & Waters, 2009; Curtis et al., 2019). Thus, implementation of this concept cannot rely on education alone; it involves strategies to integrate new roles at different levels of the health care organization. The results of this study demonstrate that cultural safety can be implemented by key actors playing different roles, such as (a) supporting individuals and families in navigating the health care system, (b) providing a new or improved service offering, and (c) building the organizational capacity to provide culturally safe health care. To achieve cultural safety, these three types of roles must be viewed as complementary to one another: they cannot stand alone. This highlights the importance of interprofessional collaboration, respect and understanding. Our results also highlight the importance of partnerships with Indigenous communities, organizations and actors in defining and implementing these roles. Cultural safety privileges the autonomy and self-determination of Indigenous populations in relation to their health services. As such, public institutions, actors and organizations must accept Indigenous difference, exceptionality and expertise in shaping solutions to meet their health care needs.
Supplemental Material
sj-docx-1-aln-10.1177_11771801221146787 – Supplemental material for Cultural safety involves new professional roles: a rapid review of interventions in Australia, the United States, Canada and New Zealand
Supplemental material, sj-docx-1-aln-10.1177_11771801221146787 for Cultural safety involves new professional roles: a rapid review of interventions in Australia, the United States, Canada and New Zealand by Marie-Claude Tremblay, Geneviève Olivier-D’Avignon, Laurence Garceau, Sandro Échaquan, Christopher Fletcher, Anne-Marie Leclerc, Marie-Eve Poitras, Eniko Neashish, Lara Maillet and Jean-Sébastien Paquette in AlterNative: An International Journal of Indigenous Peoples
Supplemental Material
sj-docx-2-aln-10.1177_11771801221146787 – Supplemental material for Cultural safety involves new professional roles: a rapid review of interventions in Australia, the United States, Canada and New Zealand
Supplemental material, sj-docx-2-aln-10.1177_11771801221146787 for Cultural safety involves new professional roles: a rapid review of interventions in Australia, the United States, Canada and New Zealand by Marie-Claude Tremblay, Geneviève Olivier-D’Avignon, Laurence Garceau, Sandro Échaquan, Christopher Fletcher, Anne-Marie Leclerc, Marie-Eve Poitras, Eniko Neashish, Lara Maillet and Jean-Sébastien Paquette in AlterNative: An International Journal of Indigenous Peoples
Footnotes
Acknowledgements
The authors thank the communities of Manawan, Opitciwan and Wemotaci, as well as the Conseil de la nation Atikamekw for their important contribution to the larger research project. The authors also acknowledge the work of Cherie Pyne, for her detailed edit of this manuscript.
Authors’ note
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and publication of this article: Fonds de Recherche du Québec—Santé 268417; Government of Canada; Canadian Institutes of Health Research; Institute of Indigenous Peoples’ Health 421162.
Glossary
Anishinaabe culturally related Indigenous peoples present in the Great Lakes region of Canada and the United States
Atikamekw Nehirowisiwok Indigenous inhabitants of a subnational territory in the upper Saint-Maurice River valley, Québec, Canada
Inuit Indigenous inhabitants of the Arctic and sub-Arctic region of Canada
Métis a culturally distinct group of specific mixed European and Indigenous ancestry
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.