
Abstract
This article is informed by an outcome from a doctoral study that explored spirituality and collective wellbeing within Indigenous and Western healthcare practices in an Indigenous South African community. The study context consists of four communities in rural Bomvanaland, in the Eastern Cape of South Africa. The study is qualitative, utilising an ethnographic case study approach, with n = 52 participants. A two-level thematic, analytical strategy of theoretical propositions and connecting strategy was used to analyse the data. Results reveal current tensions within the community due to the conflicted understandings and approaches to healthcare and wellbeing practices between traditional practitioners and Western healthcare professionals that exist in their context. Participant narratives indicate the need for a contextual, holistic, collaborative process to inform healthcare practices within their community.
The whole person should be the practitioner’s focus . . . . We argue that by addressing the whole person and engaging both body and soul as an integrated organism, medicine could be reinfused with a sense of wonder and awe. Medicine, indeed, could be re-enchanted “in such a way that the mysteries of the soul are attended to even as the mysteries of the body are controlled.”
Introduction
In this article, we discuss an outcome from a doctoral study that explored spirituality and collective wellbeing within Indigenous and Western healthcare practices in an Indigenous South African community. Indigenous African communities for the most part, conceptualise and practice healthcare in a different way from the traditional Western healthcare systems, (Campbell-Hall et al., 2010) and colonial policies have sought to displace Indigenous healing and replace it with Western healing ideologies (Kahn & Kelly, 2001) which has caused much tension related to the practice of these two knowledge systems. Despite this, there are now calls for pathways of possible collaboration to be forged between the two knowledge systems.
The deliberation regarding the integration of biomedical and traditional medicine (TM) has been ongoing for over 30 years (Kaboru et al., 2006a). In a bid to drive Primary Healthcare (PHC) provision, the World Health Organization (WHO) has in 1977 and again in 1978, as aligned with the Alma Ata Declaration, advocated for the inclusion of traditional, complementary, and alternative medicine within public health, identifying them as a resource for healthcare service provision (Kaboru et al., 2006a). WHO endorsed TM as contextually and culturally sensitive, highlighting the value of TM and traditional healers (THs) to not only the communities they serve, but as key contributors to the delivery of PHC. Studies done regarding possible collaboration, have mostly focused on the feasibility of such collaborations, or from a policy angle (Kaboru et al., 2006b). There is a dearth need of research that is focused on what this collaboration between the two healthcare knowledge systems might be like. Even more scarce within the literature are the voices of Indigenous communities’ response and expectations regarding any proposed collaboration.
A study carried out in Zambia, which focused on the perspectives of Indigenous communities regarding healthcare collaboration, indicated five critical areas of focus linked to collaboration with healthcare practitioners. These include the need for compensating THs for their work and further education of all healthcare professionals regarding cultural awareness, respect for secrecy regarding the practice of TM, monitoring for good practice, and community involvement (Kaboru et al., 2006a, 2006b). Challenges were also identified regarding this collaboration between the two health systems. These include the feasibility of the state’s capacity to regulate a culturally imbued and spiritual healthcare system like Indigenous healthcare. Another challenge is that within the African Indigenous cosmos, the explanatory model of illness involves spirituality (Campbell-Hall et al., 2010), the patient’s belief system regarding the cause of illness impact on their experience of healthcare treatment. While the biomedical approach leans more towards physiological and psychological causes of illness (Campbell-Hall et al., 2010), wellbeing within the African Indigenous cosmos is about connection and balanced relationships between people, nature, and the divine (Ohajunwa, 2019). The big question is how can these two lenses coexist without one marginalising the other? (Campbell-Hall et al., 2010).
The South African context
In South Africa, the South African Health Act of 1974 banned all THs not registered with the South African Medical and Dental Council from carrying out any act deemed as medical. Despite this it is estimated that approximately 80% of Black South Africans still consult THs before going to the hospital (Pinkoane et al., 2005; Setswe, 1999), especially in the area of HIV/Aids and mental health (Moshabela et al., 2016). The current dispensation in South Africa has recognised THs and introduced the Traditional Health Practitioners Bill in South Africa (Department of Health, 2003). Since the passing of this Bill, various collaborative measures have been sought and initiated without much success, and the perspectives of Indigenous practitioners on these provisions are very minimal (Campbell-Hall et al., 2010; Kaboru et al., 2006b). The Traditional Health Practitioners Bill of 2003 has been replaced with the Traditional Health Practitioners Act No22 of 2007 in a bid to enhance engagement with THs.
Various modes of engagement between the two knowledge systems have been researched in South Africa. Three possible approaches suggested among others are incorporation, cooperation, collaboration, or total integration (Freeman & Motsei, 1992). Research with various stakeholders indicates a preference for collaboration. Collaboration would support both Western healthcare practitioners and THs to practice separately from each other, running dual systems. They would both regulate themselves and cooperate mainly through mutual referral of patients. This option although viable, still does not explore or clearly represent what the face of the proposed collaboration might look like, and even more, how sustainable this might be from the viewpoint of Indigenous practitioners. This study aims to address this gap by presenting the amaBomvane prerequisites and model for healthcare collaboration within their context, but first we will introduce the Bomvana context below.
Context of study and methodology
The context of the study is an Indigenous community in southern Elliotdale in the Eastern Cape Province of South Africa (Figure 1). The people of this area are called amaBomvane, they are part of the Nguni group that speak Xhosa, which is a Bantu language (Jansen, 1973). The community consists of nine village clusters. The study was conducted across four of the village clusters. To ensure a good representation across the different socio-cultural contexts, one village cluster from the start, two village clusters from the middle, and one village cluster from the most rural part of their community were selected. Ethics approval was received for the study from the University of Stellenbosch, Faculty of Medicine and Health Sciences Health Research Evaluation Committee with approval number: - S16/04/078.

The hilly landscape of Bomvanaland with the sea running alongside the communities. Their medicinal herbs are located in the valleys (Photo by Damiana Ohajunwa).
Ubuntu, which is an Indigenous African philosophical framework (Boogaard & van Norren, 2021), and resilience theory, which is a Western framework (Ungar, 2012), influenced the study. The study is a qualitative study, utilising an ethnographic case study approach. This supported a more holistic process that allowed for multiple data collection. Interviews, focus groups, reflexive journaling, photography, and observations were utilised for a total of N = 52 across the four study contexts (Chilisa, 2012; Denzin & Lincoln, 2012; Yin, 2009;). Data analysis was informed by a two-level analysis. First, is an analytical strategy of theoretical propositions which is the first level of analysis and participant driven. The second level of analysis is a connecting strategy which is researcher driven. Here, interpretations of the participant narratives occur within a higher level of abstraction (Yin, 2009) until the final theme emerges. Detailed discussion of the research methodology and the influencing framework has been published in a separate article (Ohajunwa & Mji, 2021)
Results
Understanding of spirituality
The Bomvana cosmos inform their understanding of the world around them. To amaBomvane, the spiritual control the physical (Ohajunwa, 2019). This understanding of spirituality as a grounding philosophy informs the basis of all Bomvana engagements with themselves and the outside world, including their healthcare system. Spirituality is referred to in the Bomvana Indigenous language as umoya. Umoya is a lived spirituality, involving the spoken and unspoken, experiential and observed, implicit and explicit understandings and behaviours that guide one through life (Ohajunwa, 2019). The understanding of spirituality is anchored across three equally crucial and relevant aspects of beingness, which are humans living and non-living, nature, and the divine. Umoya as connectedness, and relational is key to how their spirituality is expressed. They refer to this spiritual connectedness as ubuntu.
To be seen as human within the Bomvana cosmos, one must recognise this shared existence and connectedness to other humans living and non-living, nature, and the divine. A person is perceived to be human when they are empathetic, benevolent, and kind to all about them. This is the Bomvana core value. This core positive moral guiding philosophy—ubuntu, is referred to as the community spirit by study participants: [Ubuntu is] the community spirit. (THS CA, 68)
Ubuntu is seen as an inherent spiritual concept within a person, but at the same time it also exists outside of a person and resides within the community. Ubuntu is a philosophy that connects the seen to the unseen. This is their spirituality, identity, morality, and their divine heritage all in one: Ubuntu is written, not on a piece of paper but in your face. A person with no ubuntu can be easily distinguished. (EM CA, 105) You cannot take ubuntu from a person as you cannot take the spirit. They go hand in hand. (HCP CA, 126)
Ubuntu is respect for humanity and acceptable differences. When someone does not have these attributes, they are seen as lacking in humanity, so they do not have Ubuntu: Being able to know and accept a person as a human being. I need to acknowledge the fact that they have their own beliefs and respect them. That is ubuntu. (HCP CA, 71)
The Bomvana people believe that the Western healthcare practitioners in their context do not have or show ubuntu. This is because their Indigenous belief systems are cast aside, and their healers disrespected and not recognised within the formal healthcare system. This impact on the wellbeing of their communities, as ubuntu is perceived to have the capacity to heal even before medicine is given: Kakulu! I think ubuntu can heal a person without any tangible, without anything that is given to that person. (SEW1 CB, 61) Even before giving the medication ask the patient to feel at ease, the smile, the way we handle our people, the person will get cured even before getting the medication. (HCP CB, 297)
Ubuntu is also a practical strategy for living and giving assistance to each other. Within Ubuntu’s ethos of care, the focus is not only on the health of humanity but also on the health of all nature and animals. This is reflected in their understanding of ubuntu as a community spirit as stated earlier. This is a connection beyond humans to all that is life: Ubuntu has a huge impact. Let me make an example, in this community, you live in this community, it is not like there are no orphans. There are and there are a lot. But because of ubuntu you will never see an orphan sleeping on the street like in the city. That is what we call ubuntu. It has kept us going and is working for us in the rural areas and we like it. (CLP CB, 131)
This attribute of holistic spiritual and physical care embedded within the understanding and practice of ubuntu informs the Bomvana belief that both the Western and Indigenous healing systems must find a space for collaboration. They insist that both healing systems have a role to play within their communities and besides, the concept of spirituality is not so estranged within Western healthcare practice itself: No, the medicines work in two ways, there is something in a human that will need a Xhosa medicine and there is also that which will need the English medicine. One can get sick and be cured with a Xhosa herb, or one can get sick for the medicine of doctors. It is like that. (FGCH CB, 100)
Discussion
Ubuntu is an African philosophy that upholds egalitarian connectedness. It enshrines the individual as existing within a collective, situated within a reciprocal connection with other people, and espousing a holistic, spiritual approach that sees all of the divine and nature as one (Masango, 2006; Metz, 2007; Townsend, 1997).
Ubuntu although named differently based on the context, is quite universal within the African context. The Akan adinkra cosmology from Ghana in the Western part of the continent, for instance, uses the term sankofa to denote a reconnection to humanity, empathy, and sharedness. This concept of a shared humanity is so strongly held that peoples’ validation come from being embedded and participating within their communities. This belief influences care in such a way that if people are denied participation, they become dehumanised in a sense (C. Akpom, personal communication, March 30, 2005). Hence being human is a communal philosophy grounded in ubuntu. Communal meaning people, nature, and the divine within a caring spiritual relationship (Gianan, 2011).
One of the biggest challenges to collaboration between Western and African Indigenous communities is the inclusion of Indigenous spirituality and the secrecy that often enshroud it into the formal healthcare space (Agrawal, 1995; Campbell-Hall et al., 2010) as evidenced in amaBomvane. The participants of this study proposed a way forward regarding this gridlock, which we refer to as The African Indigenous Transcultural Spirituality Framework (AITS) (Figure 2).
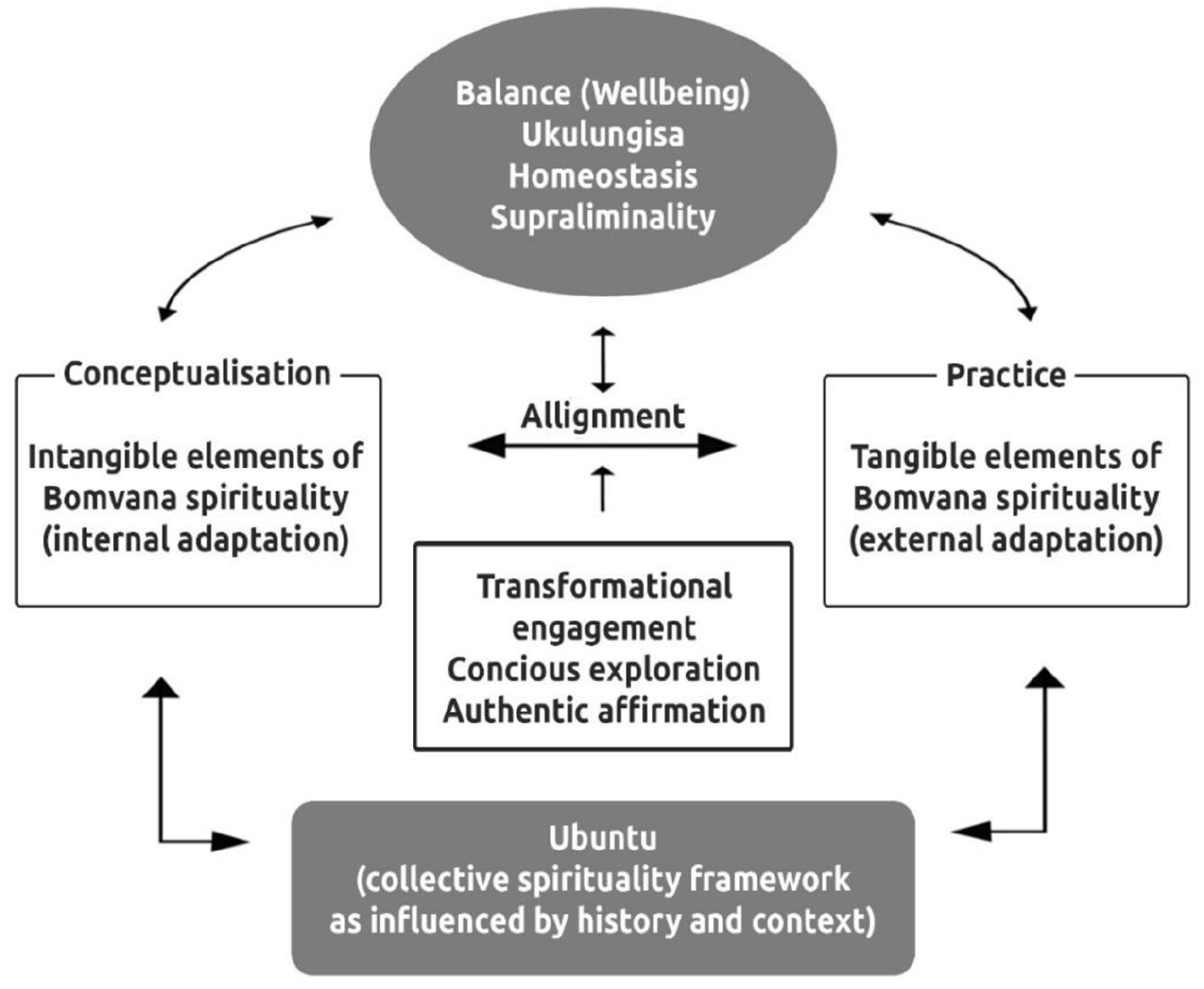
The modified African Indigenous Transcultural Spirituality framework (AITS) Ohajunwa (2019).
Ubuntu as depicted above is presented as a collective spiritual philosophical platform and undergirding factor of AITS. The concept of ubuntu acknowledges and foregrounds the shared humanity between Western and Indigenous healthcare practitioners while recognising the different healthcare narratives and worldviews that both practitioners carry that influence their practices (Ohajunwa, 2019). The transcendence within ubuntu integrates specific aspects of the two knowledge systems while leaving their core belief systems untouched (Jansen, 1973).
Ubuntu is a spiritual cultural resource that contains both tangible and intangible attributes, which we have grouped under Conceptualisation and Practice accordingly within healthcare. Alignment between these two factors provide balance. AmaBomvane believe that when a person achieves balance, then they reside in wellbeing. When there is a misalignment between the tangible and intangible aspects of ubuntu, then ill health or a loss of wellbeing is experienced.
Within the African Indigenous setting, the intangible—spiritual interpretations of illness and wellbeing for instance—is seen as more important while the Western healthcare system prioritises the tangible—such as the provision and staffing of structures like hospitals and clinics—more than the intangibles. These issues impact on long-term sustainable outcomes through a consideration of history, context and culture which inform practice.
AITS embodies past, present, and future and is an African cultural logic that advocates for a two-pronged approach that focuses on not only healthcare delivery, but how it is delivered. It takes cognisance of and engages with any pre-existing healthcare knowledge (Iwata & Hoskins, 2018), acknowledging the impact of context and history on its trajectory and human engagement within the Bomvana context. AITS is about a shared pathway and alliance to healthcare delivery within the Indigenous community that it serves within a transcultural approach (Afshar, 2005; Jansen, 1973; Leininger, 2002; Ohajunwa, 2019).
Transculturality supports collaboration between contrasting belief systems (Campbell-Hall et al., 2010; Jansen, 1973; Kourie, 2006). Although within healthcare the normative transcultural discourse is geared towards enhancing culturally congruent care, it has not adequately considered the unique historical positioning and contextual experiences of the Indigenous African community. This positioning is facilitated by the problematic way a perceived sense of superiority and systemic privilege is ascribed to Western knowledge as alluded to by the Bomvana (Ohajunwa, 2019). Neither has the transcultural discourse sufficiently addressed the implications inherent in the positioning of African Indigenous knowledge as inferior. AmaBomvane argue that these historical and contextual contexts and positioning cannot be ignored within AITS. Therefore, AITS positions Transculturality as the “merging of cultural diversity, ethnohistories in multifarious societies, identifying and working with similarities and differences among cultures and world views” (Leininger, 2002, p. 190). AITS advocates that any collaboration must not undermine beingness, but exist as a part of it, guided by ubuntu.
Tenets of AITS
There are three main attributes of AITS which the study participants have expressed as key to this collaboration within their context. We have conflated these attributes into three main tenets. These are Transformational engagement; Conscious exploration; and Authentic affirmation.
Transformational engagement
This concept connotes sharedness of identity. It depicts a transition from I to We and is facilitated by the building of reciprocal relationships. Western healthcare practitioners and Indigenous practitioners currently operate from the Us and Them paradigm, even though the tenets of both vocations centre care. Care of self, care of the other. Transformational engagement seeks a space to create one holistic system of reciprocal care. This is achieved by a transcultural movement between the past and the present, between Western and African Indigenous practices to facilitate what healthcare knowledge and practices are viable and which are not. AmaBomvane insist that rather than eschew all that is related to their African Indigenous health practices and belief system, there is a need to engage with their history and context, unearthing these knowledge and practices with the aim of exploring their relevance for the present time. The focus of transformational engagement is not about a health knowledge that is better than, but the realisation of sustainable health knowledge and practices that facilitate a shared sense of our humanity and contribute to collective wellbeing.
Conscious exploration
This concept is about sharedness in terms of common goals and motives, while coordinating activities to sync with these expected outcomes (Metz, 2007). The intentions of both Western and Indigenous healthcare practitioners towards amaBomvane is to support wellbeing. This is already a shared intent. AmaBomvane locate both Western biomedical and Indigenous healing as part of a larger belief system (Shai-Mahoko, 1996) that informs different practices. Western medicine can be perceived as simply folk medicine that has withstood certain scientific investigations (Marks, 2006). AmaBomvane notes the value of Western healthcare practices but asserts that their Indigenous knowledges must be unearthed and consciously explored, to influence their collaboration with Western healthcare practitioners. This conscious exploration of imminent possibilities must be community led so the Bomvana can define what wellbeing is to them within their multidimensional existentialism. This ensures that sustainable outcomes and narratives are accorded the right interpretation and actions taken are meaningful to the communities. One area where this exploration can begin is related to the identification of what healthcare practices are customary and which are traditional as understood by the Bomvana people. Participants indicate that while a customary practice could be negotiated, traditional practices must be carried out at a specific time, in a specific manner. Initial collaborations could begin from this customary viewpoint.
Authentic affirmation
This is about acceptable difference and goodwill (Metz, 2007). AmaBomvane realise that although the intended outcomes of both healthcare practitioners and Indigenous practitioners are similar, each retain unique differences in their approach to the conceptualisation and implementation of their health knowledges. Within authentic affirmation, these differences are positioned as a strength developed through the building of trust (Kurt et al., 2016) mutual respect, openness and a genuine need to affirm and accord benefit to the other.
Adherence to culture is a grounding factor of Bomvana spirituality and understanding of health and wellbeing (Ohajunwa & Mji, 2018). This is their resilience, context, identity, and wellbeing. Biomedicine on the contrary has focused more on physiology which equally has been very beneficial within the African context. The one challenge is that wherever biomedicine enters within African Indigenous communities, it seeks to eliminate the existing knowledge rather than collaborate with it. Evidence from the Regional Office for South East-Asia, World Health Organization (2007) shows that the ratio of TH to patient in sub-Saharan Africa is 1:500, while for the Western doctor the ratio is 1:40,000, emphasising the crucial need for collaboration. Familial and community support are important domains for a responsive health system (Basu, 2018). AITS align to a responsive health system through acknowledging shared commonalities, differences, and autonomy of each knowledge system to retain their originality and impact. The African Indigenous realities must be taken into cognisance to ensure authentic collaboration, collective wellbeing, and sustainable outcomes, all embedded within ubuntu.
Conclusion
Studies have shown the relevance of collaboration between Western healthcare and African Indigenous knowledge (Ohajunwa & Mji, 2018), engaging with their history and context. AmaBomvane have acknowledged the benefit of Western biomedical healthcare practices within their communities but insist that the practice of Western healthcare is not informed by their values, which makes it unsustainable for them. AmaBomvane insist that any meaningful collaboration must be community led and guided by the concepts of Transformational engagement, Conscious exploration, and Authentic affirmation within a transdisciplinary collaborative approach imbued with their Indigenous philosophy of wellbeing.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and publication of this article: The authors hereby acknowledge the financial assistance of the National Research Foundation (NRF) Grant Holder Linked Bursary towards this research.