
Abstract
Indigenous populations in Canada are disproportionately affected by early childhood caries. The Healthy Smile, Happy Child initiative utilizes a community development approach to encourage community uptake of evidence-based early childhood oral health promotion strategies. Sharing circles and focus groups elicited First Nations and Metis (Indigenous peoples of mixed Indigenous-European, primarily French, ancestry) views on the challenges of keeping children caries-free. We share participants’ experiences and viewpoints on implementation research strategies, principles and protocols that are sensitive to Indigenous community-based contexts.
Introduction
The future of Canada’s First Nations (FN) and Metis communities depends on the health of its children. FN and Metis peoples are committed to ensuring the best possible health for their children, including oral health. Healthy children are seen as the key to a better future (Greenwood et al., 2018). Indigenous children’s overall health and well-being affect the opportunities they can access, and the achievements that could influence the future of their communities. The oral health of Canada’s Indigenous children is less optimal than that of the general population (Mathu-Muju et al., 2016; Schroth, Moore, et al., 2005). Early childhood caries (ECC) is prevalent among FN children (Irvine et al., 2011; Peressini et al., 2004; Schroth, 2006; Schroth et al., 2008, 2013; Schroth, Harrison, & Moffatt, 2009; Schroth & Moffatt, 2005; Schroth, Moore, et al., 2005). While it is anecdotally known and observable that Metis children also have poorer oral health, little is documented (Findlay & Janz, 2012). Schroth, Harrison, and Moffatt (2009) have argued that ECC affects children’s overall health and well-being, a position that is also supported by others (The First Nations Information Governance Centre, 2012; Frohlich et al., 2006; Health Canada, 2009; Kandelman et al., 2008). Broad determinants of health also contribute to ECC in Indigenous populations (Power, 2008; Salehyar et al., 2015; Schroth, Smith, et al., 2005). For example, it is known that good nutrition is a factor in preventing ECC (Angelopoulou et al., 2018; Power, 2008). Yet in some provinces, including Manitoba, remote FN (Burnett et al., 2017) and rural and northern Metis (Sanguins et al., 2013, 2014) communities face difficulties accessing and affording nutritious foods (Burnett et al., 2017), a factor that negatively affects oral health. Other influences such as parent and caregiver knowledge and behaviours affect whether or not a child will develop ECC over time (Amin & Harrison, 2009; Gopal et al., 2016; Ozen et al., 2016). Amin and Harrison (2009) have argued that parents are more likely to implement positive oral health behaviours to prevent ECC when they know and value such behaviours.
Interventions to reduce ECC among Indigenous populations have included workshops targeting oral health workers (Macintosh et al., 2010) and leveraging available social resources to generate and sustain interest in oral health (Salehyar et al., 2015), also providing information and resources to promote and encourage uptake of oral hygiene practices as well as increasing clinical interventions such as topical fluoride varnish applications (Dooley et al., 2016). Oral health promotion programmes have also encouraged uptake and reintegration of good traditional child-rearing practices by pregnant women (Cidro et al., 2014, 2017). The aim has been to reduce parental risk-related practices, and to support health-promoting behaviours associated with ECC. Some of the practices include the use of traditional willow cradles to soothe children rather than baby bottles filled with sugary drinks, or the use of traditional diets of wild meats, fish, berries and the like instead of processed and sugary food options. Recruiting and training healthcare providers from Indigenous communities and the training of non-Indigenous healthcare providers on the specific contexts and needs of Indigenous communities are other effective practices (Lawrence, 2010).
Concerted efforts must continue towards reversing ECC prevalence among Indigenous children. Indigenous people taking the lead on their well-being is key to success. The United Nations Declaration on the Rights of Indigenous Peoples (UNDRIP, 2008) recognizes the rights of Indigenous families and communities to maintain responsibility for the continued well-being of their children, consistent with the rights of the child as a key precursor to community well-being. Similarly, the Canadian Truth and Reconciliation Commission (TRC, 2015) Calls to Action have mandated partnerships with Indigenous peoples to ensure culturally appropriate action towards closing existing health gaps for adults and children. The Healthy Smile, Happy Child (HSHC) initiative responds to the Call to Action in its oral health promotion work with Indigenous peoples and communities.
The HSHC initiative is a well-established, multidisciplinary partnership to improve Early Childhood Oral Health (ECOH) in Manitoba, Canada (Robert J. Schroth, Harrison & Moffatt et al., 2009). The partnership includes the University of Manitoba, Regional Health Authorities (RHAs), the Public Health Agency of Canada, First Nations and Inuit Health (FNIH), decision-makers, First Nations and Metis communities, service providers, and professional groups, such as the Manitoba Dental Association and Manitoba Dental Hygienists Association, among others. These partners collaborate to address the problem of ECC, which is prevalent and persistent in Indigenous populations and communities (Irvine et al., 2011). Partners also work collaboratively with the Manitoba Metis Federation (MMF) and First Nations Health and the Social Secretariat of Manitoba (FNHSSM), who provide official political representation for all Metis and FN communities, respectively.
The HSHC initiative utilizes a community engagement and development approach to enhance and increase communities’ understanding of the need to prevent ECC in Manitoba. It works with existing programmes, services, service providers and community leaders to support ECOH promotion, targeting preschool children and their caregivers. This approach is effective in improving caregiver knowledge, attitudes and behaviours towards ECOH (Schroth et al., 2015). The HSHC initiative also has a multi-directional knowledge exchange component that strives to increase the knowledge of all stakeholders to foster community-based prevention strategies, disseminate current evidence and develop the best-practice guidelines (Robert J. Schroth et al., 2009). Embedded research, evaluation and quality improvement components aim on an ongoing basis, to determine the impact of ECOH promotion on knowledge, attitudes, skills, acceptance and behaviours of all stakeholders, and to monitor the effectiveness of community-based oral health promotion strategies and activities on the prevalence of ECC (Figure 1).
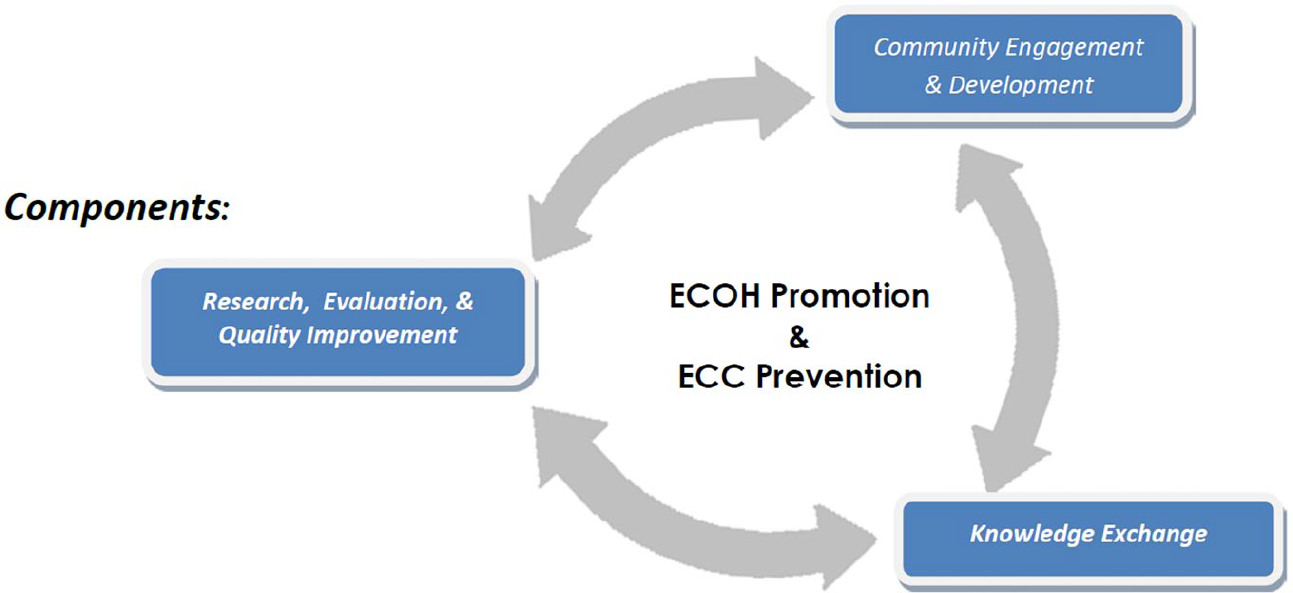
The HSHC logic model.
The key objectives of the HSHC initiative are to (1) promote the initiative and gain community awareness and acceptance of the importance of ECOH; (2) use existing early childhood and family focused community-based programmes, services and activities to deliver oral health promotion and ECC prevention activities; (3) recruit and train local leaders, including service providers; (4) assist in programme development and to deliver the ECC prevention programme on an ongoing basis; (5) scale-up capacity within existing programmes and communities to assist in the sustainability of the promotional and educational programme and finally; and (6) determine the impact all preceding objectives would have on preschool oral health and the knowledge and attitudes of parents regarding existing oral health services and healthcare providers (Robert J. Schroth et al., 2009).
A community development approach employed by the HSHC initiative is especially useful in achieving the stated programme goal of promoting young children’s oral health, by focusing on, engaging and enabling communities to identify strategies develop resources and determine teaching tools to prevent ECC in their particular contexts (Schroth et al., 2015). The approach also favours training service providers and community members to disseminate key oral health messages in recognition that community members have knowledge of the community, which researchers or external health promoters may not have. Community members and community-based service providers might best be able to identify areas of real need and to move research evidence and knowledge into action in the communities. Thus, using capacity-building strategies, community members receive relevant knowledge, tools and resources to develop or enhance their ability to support the dental health of preschool children in their localities. This process helps sustain the efforts initiated by the programme, positioning workers and community members to apply evidence on an ongoing basis.
This article discusses the key steps in engaging FN and Metis communities to understand factors facilitating or inhibiting ECOH. We outline our process of engaging FN and Metis parents, caregivers and community members in bi-directional learning of the causes and drivers of ECC, and in co-creating oral health promotion information and resources for parents and caregivers.
Method
The partnership
In keeping with the principles of community-based participatory research (CBPR) with Indigenous communities, steps were taken to build and maintain trust throughout the research relationship, part of which was respecting community ethics and protocols, and encouraging community ownership of the research process to create culturally grounded interventions (Christopher et al., 2008; Kyoon-Achan et al., 2018; Walters et al., 2020). This study occurred in collaboration with members of FNHSSM and MMF, who assisted in every phase of the project from development of the proposal, selecting the study sites, through recruiting participants, and analysing and interpreting the data. Community members on the research team also reviewed the preliminary abstracts and articles, and assisted in dissemination of results in the community. The initial proposal development was a particularly time-intensive, iterative but relationship building process. It helped bring the university-based and community-based team together to define a mutually strengthening research relationship in which the study could be directly beneficial to the communities involved as well as serving the research agenda. The research team includes FN and Metis academics and policymakers, HSHC programme coordinators, researchers, knowledge users and data collectors. Knowledge is triangulated between the FNHSSM and the MMF, and the HSHC initiative based at the University of Manitoba with input from participating communities.
Ethics approval
Ethics approval was obtained from the University of Manitoba’s Health Research Ethics Board. The process was guided by First Nations Ownership, Control, Access and Possession (The First Nations Information Governance Centre, 2014) and the MMF’s Ownership, Control, Access and Stewardship principles (The First Nations Information Governance Centre, 2014; University of Manitoba, 2015). The participating communities were contacted to obtain free, informed and prior consent to participate in the study (Ermine et al., 2004). The study was also explained to all participants and each individual was informed of the voluntary nature of the study and understood that they could choose to participate or not and could withdraw consent at any given time in the course of data collection. They were informed at the start of focus groups, of their freedom to decline responding to any question for any reason if they choose not to respond. Participants were purposively recruited, targeting parents, grandparents and caregivers of children below 6 years (<72 months) in three rural communities and various groups in an urban community. In the rural communities, a community-based research assistant contacted and invited potential participants to the sharing circle locations, which were community centres. The HSHC programme coordinator and oral health promoter contacted community programme coordinators at selected programmes to have them recruit participants who normally attended clinic and activities at drop-in centres in the inner city of Winnipeg, Manitoba.
Participants
A total of eight groups participated in focus groups or sharing circles. Four groups were conducted in an urban community and four were in rural communities. Of the eight groups, two comprised FN participants, two were primarily Metis participants and four groups were mixed FN and Metis groups. Fifty-nine community members—parents and grandparents—attended either a traditional focus group or an Indigenous modelled sharing circle.
Focus groups and sharing circles
Information was gathered from participants in two ways: focus groups for Metis communities and sharing circles with some FN participants. Focus groups are a well-known and often used qualitative method in health research, used to collect individual perspectives within a safe group context (Kitzinger, 1995; Krueger & Casey, 2009). Sharing circles resemble focus groups and build on oral traditions familiar to many FN. They are seen as a respectful and inclusive method to share information and stories (Berthelette, 2001). Sharing circles were used in two participating communities; one was in a rural FN community and the other with an urban group of FN and Metis participants. The sharing circle that took place in the rural community was conducted in a boardroom and the other took place in a community health centre.
The second sharing circle was the urban community took place in a ceremonial round room located within the premises of a local clinic. The room is part of a programme that works with Indigenous women and mothers to support them and their young children’s health and well-being. Semi-structured questions encouraged storytelling and mutual interaction, which are suitable for both data gathering and knowledge sharing with the FN and Metis communities that participated in the study. Participants spoke directly to the questions being asked, or provided any context they wished, if that helped them respond more fully to the questions. This process, in some Indigenous contexts, has been referred to as “yarning” and is an informal conversational communication that precedes and defines a mutually engaged conversation within and outside a formal research environment (Bessarab & Ng’andu, 2010). When conversations happen organically, it facilitates a more open and relaxed interaction within the formal research sessions, generating rich discussion and data (Bessarab & Ng’andu, 2010). In the FN groups, sessions opened with prayers and an eagle feather was used to guide the communication so that only the person holding the feather could speak at any time. This encouraged respect for each speaker and ensured that no one was interrupted as she or he shared their knowledge in responding to questions. Everyone had the opportunity to speak her or his thoughts fully without being rushed or interrupted. The eagle feather was passed on from one person to the next in a systematic manner so that everyone had a fair chance to contribute. No participant was under any pressure to speak; individuals could simply take the feather and say that they wanted to “pass” or that they needed more time to think about the question before responding.
For the Metis communities the research team was advised that while oral traditions were also valued and recognized within the culture, Metis citizens do not use sharing circles as a model for structuring communication. Rather, CBPR work that has involved Metis citizens in Manitoba has employed focus groups (Sanguins et al., 2013, 2014). Thus, facilitated focus groups were held in Metis communities following written informed consent obtained from participants. The same interview questions were used in all sessions, although prompts changed the more researchers learned from preceding groups.
The research environment
Knowledge sharing began after all participants were comfortably seated on flat cushions in a circle or on chairs in a circular arrangement. Only the facilitator and note-takers remained standing. Introductions were not done to respect confidentiality and maintain anonymity with the focus group facilitator who would be transcribing and analysing the data. Participants did not say their names throughout the focus group or sharing circle session. The focus groups facilitator took a systematic approach to inviting responses, in which participants took numbers and responded in descending or ascending order. Participants could choose to pass and not respond to a question if they so preferred. This made for easier transcription and enhanced an unbiased reflection on the data in the analysis phase. Written notes were taken during each session. Note-takers wrote key discussion points on wall-hanging flip charts, so that all participants could see what ideas were gaining salience in real time during the sessions. The notes helped participants and facilitators alike to visually interact with each others’ ideas, viewpoints and follow the progression of the various thoughts and questions being discussed. At the start of the session, the facilitator informed the group of this process and let participants know that they could comment on the notes at any stage. They could also make any additions or corrections if they felt that the note-taker had not correctly noted what was said.
Data analysis
All focus groups and sharing circle sessions were audio-recorded and transcribed verbatim. The analysis process began with open manual coding of data to generate an initial general understanding of that data. Further coding was completed using NVivo 12™. Thematic analysis was completed with the goal of understanding the oral health knowledge and unique experiences of Indigenous children and their parents or caregivers in general. Data were analysed separately to determine circumstances that may be unique to either the FN or Metis communities specifically. Quotes indicate FN or Metis identity to indicate distinction of thought on converging responses.
Results
A total of 59 FN and Metis community members participated in the focus groups and sharing circles. Participants included 11 males and 48 females. The age range was 21 to 71 years. A good number (44%) were employed at the time, but only 20% reported having employer-sponsored dental insurance. Some FN participants said they had non-insured health benefit (NIHB) coverage and 35% reported not having any insurance coverage.
The NIHB programme provides registered FN and recognized Inuit with coverage for a range of medically necessary health benefits. The benefits include prescription drugs and over-the-counter (OTC) medications, dental and vision care, medical supplies and equipment, mental health counselling and transportation to access medically required health services that are not available on reserve or in the community of residence (Government of Canada, 2019).
The majority (88%) of participants had children; others were grandparents whose children had young children. About 50% were married or living in common-law relationships. The actual numbers in all categories are shown in Table 1.
Participant characteristics.
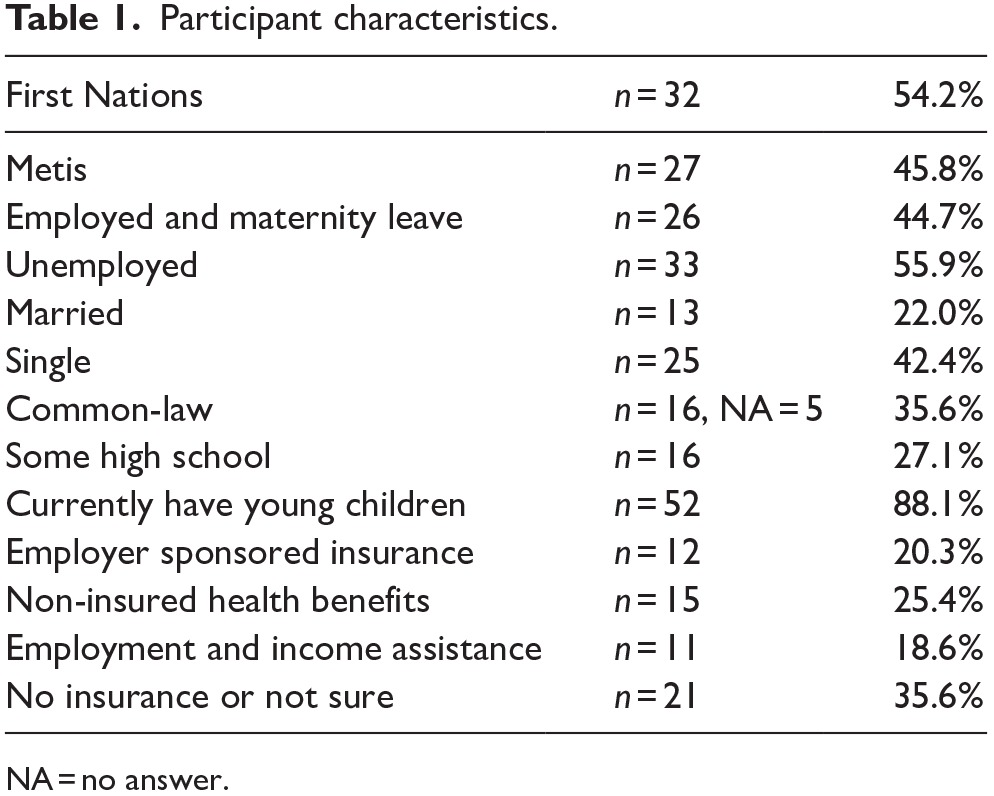
NA = no answer.
Seven themes emerged, including usefulness of the study, research as intervention, cultural relevance, and relationships, avoid assumptions, building trust and traditional health knowledge as important ingredients in research partnerships with the FN and Metis communities. We outline and discuss these themes here. In addition, however, the researchers observed and learned through the community engagement process. These perspectives are elaborated in the “Discussion” section of this article.
Usefulness of the study
The participants wanted to know whether the study would yield tangible and useful outcomes for them and their communities: Is it something that is going to come back to [our community] or are you just using us to look for answers? Will we get anything out of [the study] or is it [oral healthcare] something that you are going to bring to us? I’m looking forward to seeing what comes out of it. (FN participant)
Research as part of the intervention
While the study sought information from participants, some reported that discussions in the focus groups and sharing circles were informative to them as parents and grandparents and so had the immediate effect of encouraging change in the oral health behaviours of parents: I have my four kids [and] yeah I had my kids go under [general anesthesia for surgery]. I did it before I heard about the stories [in the session]. But this one [pointing to her child], I’m going to watch his beautiful teeth. (Mixed group urban participant)
Cultural relevance
Participants wanted researchers to consider parent and community backgrounds, values, geographical contexts and spiritual leanings in designing studies and healthcare initiatives, suggesting that in this way, studies can plan appropriate approaches to reach participants: I grew up in a school with lots of kids who are from different places . . . And also the parents. They like to live by their religion pretty strictly and if it is something outside the religion, they won’t touch it or even go near it. So maybe get someone from their religion or their culture to talk to them. If you can relate to them then maybe they’ll be more open to it. (Mixed group urban participant)
Relationship building
Participants said that they want health and healthcare information to be shared in ways that are positive and make that information more receptive to parents. One participant echoed others in wanting information that projects a positive image of the healthcare system and healthcare providers where possible, saying that an atmosphere thus created would encourage better uptake of healthcare services: This focus group is a good idea. . . . Like workshops like this would be very good, get people together to discuss [relational information sharing]. (First Nation participant) Nobody gave me scary stories, so I figured with [my daughter] she has never heard anything scary. I make sure that her daddy doesn’t talk about the dentist in front of her. I think definitely positive vibes help. (Mixed group urban participant)
Avoid assumptions
Participants suggested that commonly held assumptions by researchers and others could affect how people experience the healthcare system. One participant reported that she held in a lot of pain because the dentist assumed that she should have no pain. It appears that he trusted his assumption rather than what the patient was experiencing. Participants suggest dispelling commonly held assumptions and biases and seek instead to understand people: I find there’s a lot of assumptions made by healthcare providers that everybody’s covered under First Nations health. (Metis participant) I had to go to the dentist and I remembered feeling a lot of pain. A lot of pain, like they’re giving me the needle and I still felt the pain and I felt my tears coming through and it hurt. But because the dentist said, “It shouldn’t hurt anymore.” I just sucked it up and I can’t have had it worse. I never liked the dentist. (FN participant)
Building trust
Participants shared experiences that suggest distrust of some healthcare providers. They recommend communicating patiently and dealing honestly as ways to build trust with people: I hate to say it but personal experience, I kind of felt that the dentist rushed for it right away. . . . the first thing, before they could even get [anything done], like he didn’t even, he just kind of took a look in his [child’s] mouth and then right away he was like, oh he needs surgery. Like not even like 15 seconds he was in his mouth and right away, he was like, he needs surgery. . . . I was like hell no, I knew, I’m not even going to deal with this. When I talked to [a different provider], the dentist checked and even sat there with my son for like 20 minutes . . . And then that dentist told me straight up that he doesn’t need surgery. She’s like; those [teeth] are going to fall out. (FN participant)
Traditional health knowledge
Traditional health knowledge is important. Participants said that they use traditional medicines when prescription medications or interventions do not seem to work. Participants were hesitant to admit the use of traditional medicines, which may reflect the reality that traditional medicines and healing ways are not fully, appropriately recognized as existing and serving the population: I don’t know if I should say this, but I make medicine from herbs. Sometimes they have these doctor’s [prescriptions] that don’t get them anything when they take them, and the babies continue crying all night. (Metis participant)
In stating these desired qualities in health and healthcare research, participants provided direction on how to forge better partnerships and engage parents for better ECOH.
Discussion
In this segment, we build on respondents’ voices in discussing the importance of using methods and approaches that are congruent with Indigenous ways of being and worldview by researchers and practitioners alike (Hovey et al., 2017; Martin, 2012). The research partnerships encouraged embodied learning throughout the research process in which non-Indigenous researchers were also learning by interacting in communities and observing what is important in the FN and Metis community-based contexts.
Qualitative methods
Focus groups and sharing circles were selected because they can provide insights that are typically not captured by traditional questionnaires (Bourgeault et al., 2010). These approaches, by their very nature, promote values that are understood and desired by Indigenous populations (Maar et al., 2011), and capture the unique characteristics of each community. Participants in the groups felt so comfortable that they assumed they were in a workshop. We discuss our use of focus groups and sharing circles, honouring community protocols, the role of Indigenous Elders, the necessity to create a welcoming research environment, engagement, active interaction and participating in feasts as part of an Indigenous way of promoting relational engagements.
Respectful research
We learned that respect involves processes that are familiar and comfortable for the people involved in the research process and just catering to the needs of the research or researchers. Focus groups and sharing circles that employ storytelling and conversational interaction are suitable for both data gathering and knowledge sharing with Indigenous communities. Respectful research should also keep the entire process straightforward and relatable for community participants (Maar et al., 2011). As participants indicated, the study needs to be relevant, transparent and speak of the needs of the peoples concerned, understanding that many Indigenous peoples operate within a worldview that is geared towards interconnectedness and implementation (Bessarab & Ng’andu, 2010; Kovach, 2010), in which knowledge is rarely generated just for the sake of it, but should be used to advance clearly defined well-being and advancement goals.
Choosing the right approach
It is critically important that research with Indigenous peoples and communities engages participants as key stakeholders and recognizes this as a right and benefit (Kyoon-Achan et al., 2018). Participants in this study have recommended that in order for community members to participate meaningfully, health researchers must understand and adopt approaches that are of interest and beneficial to participants and their communities so that the research itself becomes a form of intervention as it provides relevant information and resources. More so, when participants can see value in the study, they will be more likely to participate and own the process and outcomes (Maar et al., 2011; University of Manitoba, 2015).
Discursive methods
Conducive to research with Indigenous populations are relational approaches that involve explorative and solutions seeking communication between researchers and participants (Kovach, 2010). Such approaches also lend themselves to open-ended conversation formats that pose the intended questions and invite participants to engage with the questions broadly in providing responses. Participants in this study have indicated how researcher or practitioners’ assumptions can affect how Indigenous peoples experiences processes and the healthcare system. Indigenous epistemologies can inoculate against assumptions and biases, as they aim to uncover knowledge by observing and promoting understanding through connectedness and storytelling (Braun et al., 2014). Storytelling in this manner has been said to be a central purpose of research (Lewis, 2011).
Participatory research
This is assuming a partnership stance in approaching issues, understanding phenomena and generating actionable results with research participants. CBPR, which functions along these lines, is used to foster meaningful collaborations that promote Indigenous ownership of the process and results (Kyoon-Achan et al., 2018; Tobias et al., 2013). CBPR frontlines the community as the primary data user and positions the researcher as a collaborator in health transformation. Thus culturally relevant research, as recommended by participants in this study, should seek to understand and incorporate the socio-cultural and spiritual milieu of the people and the community. This can affect how interview questions are developed, how data gathering is conducted and who is involved.
Honouring community protocols
In the example provided by a study participant at a dental office, a dentist approached her child, barely looked in the child’s mouth and promptly declared that the child would require surgery. This frightened the mother who felt distrust and likely suspicion towards the dentist and his approach. She later expressed appreciation for a different dentist who took the time to properly examine the child and discuss a treatment plan with her. In a similar manner, trust can and should be built in every interaction with Indigenous peoples and communities. In our particular case, this involved introducing the project and outlining the purpose to individuals in the communities who acted as liaisons in the communities. We wanted parents in the community to understand the purpose of the study, what to expect in sessions and how the study could potentially benefit them and other communities. The community partner—Health Director, programme coordinator, oral health promoter—was then responsible to create awareness of the research project in the community and respond to any questions. If the community wanted to participate in the project, then the contact person created a plan to recruit participants, determine dates, location for the focus group and discuss the schedule of activities. Before commencing a session in all cases, the facilitator approached individuals in the community to determine the appropriateness and requirements for offering tobacco to Elders to request prayers and an opening of the circle or group in a respectful way. The two predominantly FN groups identified an Elder to accept the tobacco and open the circles with prayers and a smudging ceremony. Prayers were said at the end to close the sessions with gratitude.
Elders and knowledge keepers
Elders and knowledge keepers who are seen as custodians of Indigenous knowledge, play an important role in ensuring that activities in the community are conducted with respect and recognition of the efforts of others who have gone ahead. An Elder or knowledge keepers would ideally be present to receive the tobacco and offer prayers on behalf of the group. An Elder was present at the first of the two FN groups. There was no Elder present at the second group so the tobacco was offered to one of the women who was to be a participant in the sharing circle. Another respected Indigenous woman in the programme who had been approached by the programme manager at the clinic selected her. The tobacco was received and prayers offered to open the sharing circles at the beginning and at the end. One of the FN groups offered a Christian prayer with no additional action. The other group offered an opening prayer followed by a traditional activity. The Elder conducted a smudge, a practice which involves the burning of traditional herbs such as sweet grass and sage. The smoke is then fanned towards the face and body as a cleansing aroma in spiritual preparation to engage in a ceremony. Everyone present, the research team, participants and workers, at the clinic proceeded to smudge if they wanted to. Those who did took turns at conducting fanning and cleansing motions with the smoke. The Metis communities did not observe the same protocols as the FN communities in that there were no Elders overseeing the process or offering prayers and tobacco at the start of sessions.
Active interaction
The participants talked about bringing people together to discuss issues of common importance and keeping communication positive as a way in which to protect people’s perceptions of healthcare. These ideas elicit the theme of relationships, at the centre of which is communication. Maintaining active interaction between researchers and participants helped create the quality of togetherness in addressing an issue of common import. The session was not one-sided with researchers asking questions and participants merely responding. The ambience was kept friendly, conversational, using humour and storytelling, which helps douse tensions and research-related anxiety (Hewer et al., 2019). The facilitator was also willing to reframe and clarify questions, so that participants clearly understood and would respond to what was being asked. The research team did not take for granted that everyone would understand the terms and jargon being used in the questions. Participants also made connections between questions, clarified their responses and elaborated on points and statements as they deemed fit. They could also ask any questions or seek clarifications as necessary. Researchers also committed to sharing data and results with each community on an ongoing basis through all stages of the study.
Feasts and gifts giving
Sharing food is observably a part of many Indigenous cultures. Researchers and participants enjoyed meals together; this made for lighter conversation and helped with developing warmer relationships. Gifts or giveaways were handed out to show appreciation of participants’ time and knowledge. All participants received gift cards, toothbrushes, toothpaste and dental floss in appreciation of their participation. This is not to be construed as payment because the knowledge shared is invaluable. More so, paying for knowledge goes against the fundamental value of sharing, which is so prominent in Indigenous cultures. The gift cards given to participants at the end of the sessions were in appreciation of their time and contribution.
Limitations of the study
This study has shared information that pertains to the Manitoba FN and Metis contexts, and at that, the specific communities that participated in the study. Although we believe that the perspectives shared herein could be applied elsewhere, additional research is required to further elaborate on the respectful engagement and partnership expectations of other Indigenous peoples and communities when collaborating to promote ECOH.
Conclusion
In ECOH promotion to prevent ECC, it is crucial to understand the drivers of ECOH in Indigenous communities. However, research should be implemented in ways that respect and align with Indigenous values, and honour working together to make the needed changes. In this way, research becomes a platform for learning from the FN and Metis communities in a reciprocal and respectful way and for co-creation of knowledge that is both relevant and applicable in the communities. This involves applying processes that are familiar and comfortable for Indigenous peoples, who will ultimately own and continue to implement the results. The Scaling Up initiative, in its partnership with the Manitoba FN and Metis communities, is working to ensure that the goals of the UNDRIP and TRC Calls to Action are honoured and met in ending ECC and promoting ECOH for better overall health and well-being. Research that is useful to the communities, such as respectful of collaboration, culturally relevant, relationship building, oriented to trust building, respects traditional healing ways, is contextually situated and owned by the communities, is one way to achieve this objective. Ensuring that communities understand and are taking the lead in evidence-based oral health knowledge and culturally grounded oral health promotion is the key to improving the oral health of FN and Metis children in Manitoba.
Footnotes
Acknowledgements
This study was made possible by an Implementation Research Team grant from the Canadian Institutes of Health Research for the Scaling Up the Healthy Smile Happy Child Initiative: Tailoring and Enhancing a Community Development Approach to Improve Early Childhood Oral Health for First Nations and Metis Children. Dr Schroth holds a Canadian Institutes of Health Research Embedded Clinician Researcher Salary Award in Improving Access to Oral Health Care and Oral Health Care Delivery for At-Risk Young Children in Manitoba.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Glossary
Metis Indigenous peoples of Canada and parts of the United States of mixed Indigenous-European, primarily French, ancestry.