
Abstract
Commercial tobacco products are a leading contributor to health disparities for many Indigenous peoples. Mainstream interventions developed for non-Indigenous peoples have been found less effective at addressing these disparities. Meaningful engagement is needed to develop effective measures but there are limited understandings of what engagement means in practice. We conduct a scoping review of studies self-reporting engagement with Indigenous peoples; assess their engagement against ethics guidelines concerning research involving Indigenous peoples and writings of Indigenous scholars; and draw lessons for advancing practice. We found engagement of Indigenous peoples in tobacco control research is practiced in varied ways—who conducts the research, who is engaged with, for what purpose, at what research steps, and what approaches are applied. Engagement ranges from limited to deeper commitment to research as decolonizing practice. Critical reflection along five questions can advance research practice for this purpose.
Introduction
Commercial tobacco is a leading contributor to health disparities among Indigenous peoples
1
in many settler countries (Glover et al., 2013; Maddox et al., 2019). Commercial tobacco is defined as
manufactured by companies for recreational and habitual use in cigarettes, smokeless tobacco, pipe tobacco, cigars, hookahs, and other products. Commercial tobacco is mass-produced and sold for profit. It contains thousands of chemicals and produces over 7,000 chemical compounds when burned, many of which are carcinogenic, cause heart and other diseases, and premature death. (US Department of Health and Human Services, 2014)
For example, commercial tobacco (hereafter tobacco) is responsible for 23% of the gap in health burden (the total impact of disease, injury, and death) between Indigenous and non-Indigenous Australians (Australian Department of Health, 2020). In Canada, tobacco has led to about 1.5 times greater rate of population-adjusted mortality attributable to smoking among Indigenous peoples in Canada (Reading, 2015).
Tobacco control interventions for general populations have been found to be less effective in addressing health inequities from commercial tobacco use among Indigenous peoples. Evidence attributes this to their design by, and for, non-Indigenous populations (Bond et al., 2012). Interventions can thus be perceived by Indigenous peoples as culturally inappropriate, lacking in local orientation and facilitation, and insufficiently drawing on traditional knowledge, strengths and practices. As Baillie et al. (2008) write, “borrowed tobacco control initiatives are failing” in Indigenous communities in Canada. Researchers in the USA (Boudreau et al., 2016; S. Smith et al., 2014), Australia (Cosh et al., 2013) and New Zealand (Grigg et al., 2008) note a similar history of ineffective tobacco control initiatives and need for Indigenous-led solutions. For example, systematic reviews by Minichiello et al. (2016) and Palmer et al. (2017) conclude that Indigenous ownership and community engagement, and culturally appropriate measures, leads to more effective tobacco control. Health Canada’s Federal Tobacco Control Strategy (2018–2023) acknowledges the need to “recognize the unique circumstances of Indigenous populations in Canada,” and commits to “work[ing] with national and regional Indigenous organizations to co-develop distinct approaches” (Health Canada, 2018). At the global level, Article 4 of the World Health Organization (WHO) Framework Convention of Tobacco Control (FCTC) acknowledges, “the need for Indigenous individuals and communities to participate in the development, implementation and evaluation of tobacco control programs that are socially and culturally appropriate to their needs and perspectives” (WHO, 2003).
While there is recognized need for meaningful engagement with Indigenous peoples, to achieve more effective commercial tobacco control, what this means in practice varies widely. Oberly and Macedo (2004) describe a long history of public health researchers and practitioners claiming to consult with Indigenous peoples while prioritizing their own agendas and interests. As a result, “data concerning tobacco-use knowledge, attitudes, and behaviors are woefully lacking . . . due to a shortage of funds, lack of health promotion infrastructure, and the legacy, and continuing practice, of culturally inappropriate research.” More recently, Boudreau et al. (2016) write that the tobacco control community in the USA has not always dealt respectfully with Indigenous communities in the past. To continue to move beyond this legacy of colonization, tobacco control scholars and advocates need a shared understanding and practice around meaningful engagement with Indigenous peoples.
As one step towards this goal, this article presents a scoping review of peer-reviewed studies and theses which self-report engagement with Indigenous peoples. A scoping review is an “examination of a broader area to identify gaps in the research knowledge base, clarify key concepts, and report on the types of evidence that address and inform practice in the field” (Peters et al., 2015). Drawing on core values and principles set out in ethical guidelines for conducting research concerning Indigenous peoples, and writings of Indigenous scholars, we assess this research along five questions concerning different aspects of engagement. We acknowledge that existing guidelines are still emerging, alongside agreement on how to translate them into practice. As such, this review aims to scope, rather than formally evaluate, research practice to date. The article concludes by drawing lessons for supporting meaningful engagement with Indigenous peoples in commercial tobacco control research, as a precursor, to reducing tobacco-related health disparities.
Methods
To identify tobacco control research that self-reports engagement with Indigenous peoples, we searched Google Scholar and the Medline (EBSCO) academic research database (>9,000 journals across all disciplines) from inception to January 2020 without language limits. We used the search string “tobacco” AND “Indigenous” (OR “Aboriginal,” “First Nation*,” “Metis,” “Inuit,” “American Indian,” “Native,” “Maori”) AND “invol*” (OR “engag*,” “consult*,” “participat*,” “collaborat*,” “cooperat*,” “dialogue”) but NOT “India” to search title, abstract or keywords. Google Scholar yielded 231 articles and Medline provided an additional 86 articles (n=317). An additional four articles were brought to our attention during the peer review process. We then searched the ProQuest Dissertations and Theses database and Medline (EBSCO) Host Open Dissertations from inception to January 2020 (n = 97). We screened titles and abstracts for original studies against three inclusion criteria: (a) reporting primary research findings, (b) focusing on Indigenous people(s) and tobacco use and (c) involving engagement with Indigenous people(s) in some aspect of the research process. Consequently, literature reviews and commentaries were excluded, along with those that did not mention methods that included participation of Indigenous peoples in the title or abstract. We acknowledge that studies which may apply these approaches, but do not describe them in the title or abstract, may be overlooked. This resulted in 56 articles and seven dissertations (n = 63) for detailed review (Appendix 1).
The engagement by these studies with Indigenous peoples was then assessed against ethics guidelines concerning research involving Indigenous peoples in settler countries. These include the OCAP® (Ownership, Control, Access and Possession) principles (First Nations Information Governance Centre, 2019; Inter-Tribal Health Authority, 2005), TriCouncil Policy Statement Research Involving the First Nations, Inuit and Métis Peoples of Canada (Government of Canada, 2018), Guidelines for Ethical Research in Australian Indigenous Studies (AIATSIS, 2012) and Ethical Conduct in research with Aboriginal and Torres Strait Islander Peoples and communities (National Health and Medical Research Council [NHMRC], 2018a). Recognizing that existing guidelines reflect settler perspectives, vary in scope and focus, and thus are emergent as Indigenous people(s) reclaim “control over research activities and the knowledge that research produces” (L. T. Smith, 1999, p. 4), we also draw upon Indigenous scholars writing about health research practice (Boudreau et al., 2016; Castellano, 2020; Drawson et al., 2017; Oberly & Macedo, 2004; Rix et al., 2019; L. T. Smith, 1999).
We organize our scoping review, of how engagement with Indigenous peoples has been practiced to date in commercial tobacco control research, around the following five questions concerning different aspects of engagement: who conducts the research, who does the study engage with, what is the purpose of the research, what research step(s) does engagement take place and what approach is used for engagement.
We consider existing practices against core values (e.g., equity, reciprocity, respect, relevance) and principles (e.g., consent, cultural competency, cultural and intellectual property) put forth in guidelines and scholarly writings (Table 1). Given the emergent nature of these values and principles, we do not consider it appropriate to conduct a formal evaluation of these studies retrospectively. Ethical principles and standards of practice change over time. Moreover, we acknowledge that studies as reported may omit information needed to fully assess them and may thus be more aligned with core values and principles than described. For example, few studies provide details of ethics approvals or research agreements with Indigenous communities. This is not necessarily because these practices were not followed, but that they simply may not have been reported. Instead, based on the self-reported information provided, we draw lessons for meaningful engagement with Indigenous peoples in commercial tobacco control research practice.
Summary of engagement with Indigenous peoples in literature reviewed

Findings
Who conducts the study?
One long-standing criticism of much health research concerning Indigenous people(s) has been its conduct by non-Indigenous researchers. As Abimbola (2019) writes, the legacy of colonization continues to impact how research is conducted. For Indigenous peoples, the phrase “nothing about us without us” has been used to express concern about the “unidirectional gaze by non-Indigenous researchers” (Ball, 2005). For example, under the OCAP® principles, Indigenous control extends to “all aspects of research and information management processes . . . all steps of a particular research project—from start to finish” (First Nations Information Governance Centre, 2019). This includes Indigenous peoples with lived experience as researchers. As Ball (2014) describes,
[w]hile the number of Indigenous researchers is growing, most research about Indigenous people continues to be done by non-Indigenous investigators and students. Supporting the development of Indigenous research capacity and the inclusion of Indigenous students and community members on research teams, must be a priority in research involving Indigenous people.
Based on online searches of author names, 46 (73%) studies have at least one self-identified Indigenous (co)author, with 13 studies (21%) having Indigenous lead authors. Beyond authorship, at least 24 studies (38%) involve Indigenous peoples as research assistants or advisors. For example, Ivers, Castro, Parfitt, Baili, D’Abbs and Richmond (2006) and Ivers, Castro, Parfitt, Bailie, Richmond & D’Abbs (2006) employ an Indigenous research assistant to recruit participants, explain the study in the local language when needed, and facilitate informed consent. Many studies acknowledge the importance of hiring Indigenous research assistants to collect data in culturally appropriate ways. Tane et al. (2019) recruit “Cultural Mentors” who provide “oversight and guidance throughout the research, through language interpretation during qualitative interviews, cultural advice pertaining to the observance of ŋarali’ [tobacco] traditional practices and insight during analysis.” It is not possible, with the information provided by the studies, to determine the extent Indigenous (co)authors, research assistants and advisors are from the Indigenous study population. Where the study concerns a broadly defined Indigenous population, such as Aboriginal health workers in Australia (Bar-Zeev et al., 2017), the specific cultural affiliation of the Indigenous researcher may not be as important. Where the research concerns a specific community, involving community members as researchers could be important for achieving more meaningful engagement.
Who does the study engage with?
While all the studies in this review self-report engagement with Indigenous peoples, who each study actually engages with specifically varies. Indigenist and decolonizing research methodology calls for research that “fully captures and honors the voices and perspectives of Indigenous peoples but, more importantly, emanates from an Indigenous ontological and epistemological basis” (Rix et al., 2019, p. 259). Principles of ethical research involving Indigenous peoples require for example “consultation,” “negotiation,” “participation” and “informed consent” (AIATSIS, 2012). However, what these terms mean in practice lacks clarity and consensus. To move towards improved research practice to meet recognized principles, greater clarity is needed about who should be consulted and negotiated with, or invited to participate and give informed consent. The extent to which there is meaningful engagement, which enables research that genuinely reflects the perspectives of Indigenous peoples, depends on who is actually engaged with by the research.
By settler country, the distribution of studies reviewed engaged with Indigenous peoples in the USA (45%), Australia (29%), Canada (16%) and New Zealand (10%). This is perhaps reflective of the balance of tobacco control research in general being conducted in these countries. However, this may also be suggestive of the extent to which tobacco control research, being conducted in these countries, seek to engage with Indigenous peoples.
By unit of analysis, studies range from individuals selected by demographic variable (i.e., sex and gender, age, social status, expectant women) or specific behaviour (e.g., smokers, health workers) related to tobacco use, to social groups spanning single or multiple nations/tribal affiliations or other defined domain (e.g., urban, rural, online website user). We found the term “community” used in the studies reviewed to variably refer to membership by shared ethnicity, tribal affiliation or geographical location (e.g., living on reserve). Study population size ranges from a small number of key informants to nation-level population surveys.
On the approach used by each study to identify the Indigenous peoples with whom to engage with, most apply the methods of settler scholars to select subjects for focus groups, surveys or interviews. These research methods seek to enhance validity and reliability through appropriate sampling (e.g., random, purposive, convenience) to ensure an appropriate study population. Indigenist and decolonizing approaches and methods may also seek to enhance validity through the building of meaningful relationships by the researcher. As Rix et al. (2019) describe,
we do not engage in relationships, nor are we in relationships, but we are relationships. Our very being, and the nature of reality itself, is relational. We are relationships with people and communities, with the Land, with ideas, with everything. (p. 259)
As such, the researcher “is not outside of reality looking in but has entered into a different set of relationships with the people and issues that they are researching.”
The challenges faced, in applying mainstream sampling methods to a randomized control trial (RCT), in some of the studies reviewed, illustrate the difference between settler 2 and Indigenist approaches to identifying who should be engaged with (Glover et al., 2015). Lichtenstein et al.,(1995, 1996), partnering with an Indian Health Board in the northwestern USA, describe opposition to their initial RCT plans on the grounds that a “control community” contradicted the Board’s mandate to serve all tribes equally. The agreed compromise was for communities to be randomly allocated to begin the consultation immediately or be “waitlisted” until an evaluation of the first communities was completed. In seeking to conduct an RCT among Alaskan Native adolescents, Patten et al. (2014) also describe challenges in recruiting a control group. They conclude that the study design was ineffective and there is a need for innovative sampling methods to capture multiple domains (e.g., familial, social and community). The studies reviewed suggest that, when seeking to define study populations for meaningful engagement, mainstream sampling methods may be inappropriate. Rather than criteria such as representativeness, generalizability or efficiency, the significance of social relationships and cultural values held by Indigenous peoples to be engaged with may be more important considerations. A form of purposeful sampling might be conducted, for instance, in partnership with an Indigenous community in ways that align with relationships and values. For example, Margalit et al. (2013) consult community members to identify who is recognized as an elder before purposive sampling of key informants. Overall, researchers seeking to meaningfully engage with Indigenous peoples should critically reflect on how Indigenous people come to be defined as study populations in their research and, in turn, who is then chosen to engage with.
What is the purpose of the research?
A common criticism of health research involving Indigenous peoples is a lack of relevance to their lived experience, and hence priority health needs, of Indigenous peoples. This can arise for a number of reasons including inadequate representation of Indigenous perspectives among the researchers and insufficient engagement with the study population as described earlier. In addition, there can be a prioritization of benefits accruing to researchers, rather than Indigenous peoples, in the funding and design of research. More fundamentally, the epistemological and ontological starting points of settler methodologies tend to “pathologize” Indigenous people and communities, focusing on compartmentalizing and then addressing perceived deficits in the physical and mental health of individuals, Indigenous peoples’ behaviours, or the shortcomings of Indigenous societies. While seeking to improve health, mainstream research is described as too often framed and conducted in ways that are inherently biased towards maintaining systems of dispossession and oppression (Carlson, 2016; Rix et al., 2019; L. T. Smith, 1999). In contrast, Indigenous methodologies emphasize strengths-based approaches, and a holistic view of health and wellness, locating individuals within social and historical contexts, as well as “links which bind the generations together” (NHMRC, 2018a, p. 4). To address the need for research to be more relevant to Indigenous peoples, many guidelines support the value of reciprocity (First Nations Information Governance Centre, 2019; Government of Canada, 2018), and call for research outcomes that produce “specific results that respond to the needs and interests of Indigenous peoples” (AIATSIS, 2012). As Ball (2005) writes, “[p]artnerships can help to ensure that topics under investigation are priorities for Indigenous peoples, that they reinforce Indigenous values, are understood using Indigenous frames of reference, and are beneficial to Indigenous peoples.”
On study purpose, we found 43 (68%) of the studies reviewed seek to achieve individual behaviour change through measures focused on cessation and/or prevention. Twenty-eight of these studies assess the effectiveness of culturally adapted cessation and/or prevention interventions for reducing, or increasing knowledge of the health harms arising from, tobacco use as a behavioural risk factor. For example, Schinke et al. (1996) attribute the “high prevalence of cancers” among Indigenous peoples to “behavioural and lifestyle patterns,” and the fact that “[c]learly, the wisdom of cancer prevention has not found its way into the lives of most Native Americans.” Similarly, Weaver and Jackson (2010) seek to develop a culturally appropriate wellness curriculum based on the starting point that “risk factors such as poor diet, recreational tobacco use, and a sedentary lifestyle can be modified through health conscious choices.” This strong emphasis on modifying the behaviour of Indigenous peoples is consistent with commercial tobacco control research as a whole, as well as, public health efforts to address rising rates of non-communicable diseases more generally. As Lee and Crosbie (2020) argue, “mainstream approaches to tackling NCDs have so far overwhelmingly focused on so-called demand-side measures which seek to change the modifiable behaviours of consumers.” These approaches assume that “NCDs are primarily self-inflicted, and that people must simply be convinced of the error of their unhealthy ways.” This emphasis on individual behaviour is also a reflection of reductionist western approaches versus holistic Indigenous perspectives, as described earlier, which prioritize relationships and communities. For example, the Māori model of health emphasises four cornerstones of health—physical, spiritual, family and mental health (Durie, 2017).
A small number of studies seek to understand broader factors that contribute to tobacco use. Ten studies (16%) concern secondhand smoke exposure and the promotion of smokefree environments in homes, private venues (e.g., casinos) and public places. One study (1%) considers the role of sports sponsorship and is, indeed, the only study to examine the role of marketing of commercial tobacco products to Indigenous peoples. The purpose of six studies (10%) is to better understand the meanings of tobacco (commercial and traditional) from Indigenous perspectives as a precursor to developing culturally appropriate measures (Unger et al., 2006; Varcoe et al., 2010). Mutch (2011), for example, uses “a framework for Aboriginal-guided decolonizing research” to understand “the meaning of tobacco and tobacco control from the perspective of Metis people.” As a Metis woman, the author locates tobacco misuse within “a long-standing history within Aboriginal culture,” which includes ceremonial, spiritual and cultural aspects. A study by Stevensen (2013) seeks,
to determine whether a concept of traditional and non-traditional tobacco use exists among members of Fort William First Nation; how members distinguish between traditional and non-traditional uses of tobacco; tobacco’s roles in the community; emotions that members experience in relation to tobacco; and members’ visions of best-case, future realities of tobacco use in their community.
Similarly, Margalit et al. (2013) aim “to elucidate Lakota elders’ views on traditional tobacco and commercial/addictive tobacco use,” and Ratsch et al. (2017) sets out to “understand knowledge and practices around the use of Nicotiana spp (chewing tobacco) among central Australian Aboriginal women.”
Three studies (5%) take a strengths-based approach. Lukasewich (2015) seeks to understand the extent participation in a school-based health promotion video project with Aboriginal youth led to positive perspectives on health and wellbeing; and how research participation can contribute to embarking on an empowering journey. Chan Osilla et al. (2007) aim “to fill the void in knowledge about prosocial behaviors and characteristics, essential for promoting and fostering positive youth outcomes, by discussing prosocial peer networks, future aspirations, and extracurricular activities as protective factors against regular tobacco use.” Weaver and Jackson (2010) pilot a wellness curriculum which covers physical activity, tobacco use and diet.
Overall, the majority of the studies reviewed seek to evaluate the effectiveness of standard (albeit adapted) tobacco control interventions at changing Indigenous peoples’ behaviours, rather than the structural conditions which shape those behaviours. Needs are defined largely in deficit terms as reducing commercial tobacco use, as a health harming behaviour associated with negative outcomes, largely through prevention and cessation interventions. While most studies recognize the need to adapt interventions to Indigenous cultures, only a few studies align this purpose with strengths-based approaches, and fewer yet being designed by Indigenous peoples based on their priorities.
What research step(s) does engagement take place?
When seeking to engage meaningfully with Indigenous peoples, in conducting research that supports commercial tobacco control programmes, we argue that the research step(s) when engagement takes place is meaningful. The WHO FCTC states that there is a “need for Indigenous individuals and communities to participate in the development, implementation and evaluation of tobacco control programs” (WHO, 2003). Guidelines by the Australian National Health and Medical Research Council set out “community/organisational involvement” in each of “eight steps of the research journey” (NHMRC, 2018a). To what extent has tobacco control research to date engaged Indigenous peoples across these steps?
Applying the NHMRC (2018a) guidelines to the methodologies described in each study, Table 1 shows that no studies engage Indigenous peoples across all eight research steps. Ratsch et al. (2017) engage across seven steps and, in doing so, might be described as engaging more meaningfully. Five studies (8%) engage across six steps (Anderson et al., 2019; Bovill et al., 2018; Margalit et al., 2013; Montogomery et al. 2012; Varcoe et al., 2010). In contrast, seven studies (11%) engage in one step (with Indigenous peoples involved in data collection as subjects or researchers) and, in doing so, might be described as engaging least meaningfully.
Table 2 shows the total number of studies engaging Indigenous peoples by early, middle and later steps of research. This review finds most engagement with Indigenous peoples during the middle steps of data collection (63) and data analysis (23). By virtue of the inclusion criteria for this review, all the studies engage Indigenous peoples in data collection (n = 63) as study participants or subjects. In addition, at least 46 studies (73%) involve Indigenous peoples in data collection as (co)authors and 11 studies (17%) as researchers or advisors. It is notable that 23 studies (37%) involve Indigenous peoples in data analysis to enhance the validity of findings. For example, Johnston and Thomas (2010) involve Indigenous health care workers, elders and leaders in the thematic analysis of qualitative data. After a non-Indigenous researcher codes the interview data gathered, preliminary findings are reviewed by Indigenous researchers and stakeholders who then refine the emergent themes.
Total number of tobacco control studies engaging Indigenous peoples by research step.
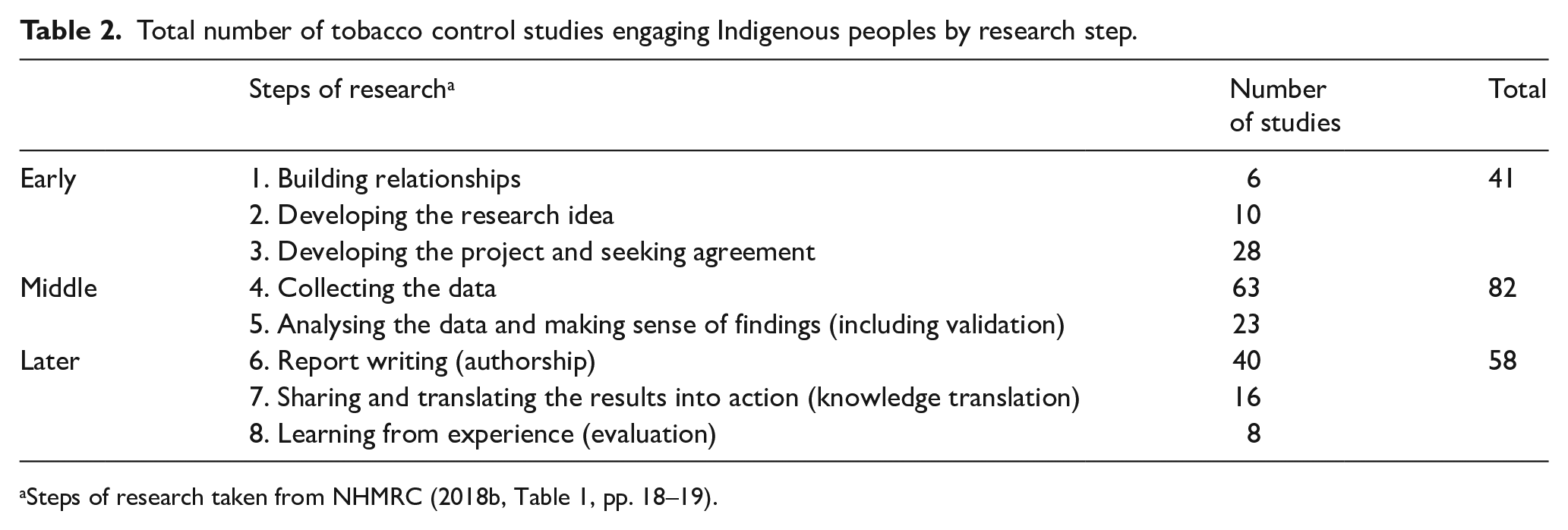
Steps of research taken from NHMRC (2018b, Table 1, pp. 18–19).
Beyond report writing (36), during the later steps of research, fewer studies engage Indigenous peoples in knowledge translation (16) and evaluation (8). One exception is Bar-Zeev et al. (2017) who carry out a “structured 4-step evaluation process” to inform “the development of a resource package to be used as part of a multi-component intervention, aimed at improving how health professionals manage smoking in Aboriginal and Torres Strait Islander pregnant women who smoke.” This is described as a
novel formative evaluation protocol [which] has never been done previously in Australia. If these resources prove effective, the methodology could be adapted for other Indigenous interventions, and culturally diverse programs. The added value of this time-consuming and costly process is yet to be justified in research, and might impact the potential adaption by other projects.
While many studies conduct evaluations, almost all involve impact (to measure short-term effect of a programme), outcome (to measure short-term effect of a programme) or evaluations (Campbell et al., 2014; D’Silva et al., 2011; Harvey et al., 2002; Hayward et al., 2007; Ivers, Castro, Parfitt, Baili, D’Abbs and Richmond, 2006). Marley et al. (2014) is notable in conducting a process evaluation of the Be Our Ally Beat Smoking (BOABS) Study to draw lessons about “how to develop and implement an integrated smoking cessation program.” As the authors write, the results of the study
demonstrated the importance of local Aboriginal ownership, commitment, participation and control. This included knowledge of local communities, the flexibility to adapt interventions to local communities and circumstances, and taking sufficient time to allow this to occur. Short-term project funding undermines community control and ownership, and program development and delivery [29,30]. Researchers, including ourselves, can also be optimistic and/or naïve in anticipating unrealistic timeframes for completing research projects in settings characterised by significant structural barriers and competing community priorities.
Similarly, relatively few studies engage Indigenous peoples from the study community or engage in the study as participants at the earliest steps of research, notably building relationships (4) and developing the research ideas (10). This is consistent with the observation by Boudreau et al. (2016) that “public health groups have not made efforts to build relationships with our [Indigenous] leaders and have even supported efforts to restrict tribal decision-making.” The exceptions in this review include Margalit et al. (2013) who describe engagement with Lakota community leaders to define the goals of the project which consequently focused on collection and preservation of oral history, and data for cessation efforts. More common is engagement with Indigenous people to provide input on research design. Lichtenstein et al. (1995, 1996) describe a “consultative intervention” with tribes in Washington, Idaho and Oregon as the basis of developing and then evaluating culturally appropriate tobacco control policies. Bar-Zeev et al. (2017) work with Indigenous leaders and community members to develop and evaluate educational materials related to tobacco use. Campbell et al. (2014) report on a social marketing campaign designed by Aboriginal communities. Bowen et al. (2012) conduct a feasibility study of a web-based intervention designed through consultation with Indigenous youth. Báezconde-Garbanati et al. (2007) mobilize the capacity of American Indian communities to develop locally relevant tobacco control policies.
Overall, engagement by step of research reveals substantial variation across the studies reviewed, from limited engagement of Indigenous peoples as the subject of study, to efforts to engage Indigenous peoples across selected steps. The average number of research steps that Indigenous peoples were engaged is 2.87 steps which suggest much scope for improvement. Our findings also suggest that perceptions of what meaningful engagement means may be changing over time, with studies conducted prior to 2005 having a lower breadth of engagement. Schinke et al. (1996), for example, write that “[t]he collaborative nature of the[ir] study . . . embodies a cultural sensitivity not often seen in preventive intervention and health programs,” and that “the study and the approaches to cancer risk reduction that it is testing are pioneer steps in health education for an important, yet underserved and underresearched, population.” While the study was perhaps pioneering in the mid 1990s, when few tobacco control studies collaborated with Indigenous peoples, core principles and values set out by research guidelines and Indigenous scholars since have raised expectations of what meaningful engagement means in practice. The five studies which engage with Indigenous peoples across six steps of research have been conducted since 2010, suggesting a possible shift towards increasing engagement earlier and later in the research process. Weaver and Jackson (2010) describe their study as having “Native American involvement at every step and level with culture as an important backdrop rather than an ‘add on’ feature.” However, such studies remain relatively few in number. The concentration of engagement during the middle steps indicate that there remains scope to achieve more meaningful engagement by involving Indigenous peoples across the full breadth of research practice.
What approach and methods are used for engagement?
What approaches and associated methods might be advanced to make engagement with Indigenous peoples in commercial tobacco control research more meaningful? Guidelines set out core values, such as respect, and principles such as consent, but do not set out specific approaches to inform practice. In the studies reviewed, we found 19 studies (30%) pre and post test pre-selected interventions (many culturally adapted) for their efficacy at achieving behavioural change or increasing knowledge of commercial tobacco use. These include seven RCTs and 11 studies (17%) which do not identify a specific approach. The latter describe the methods for developing and implementing an intervention, and assessing the degree of their effectiveness, but do not set out broader assumptions which inform the selection of methods.
In contrast, community-based participatory research (CBPR) and participatory action research (PAR) approaches are adopted in 20 studies (32%) as starting points. These approaches are described as particularly apt for enhancing control and ownership by Indigenous peoples, acknowledging power inequities between researchers and participants, and fostering local capacities. For example, Blanchard et al. (2015) describe CBPR as an “approach that reinforces the importance of power sharing and promotes the idea that collaborative partnerships give prominent roles to community partners in the ownership and control of project outcomes.” Similarly, Choi et al. (2011) describe the principles of CBPR as: “1) tailoring to meet the needs of individuals and communities; and 2) providing the opportunity for the people for whom the program is developed to participate in the development, implementation, and evaluation.” Sabesan et al. (2015) write that the PAR approach “seeks to bring about positive change and is based on equal and collaborative involvement with the affected community.”
Four studies (6%) explicitly adopt reflexive approaches which recognizes research as a relational process requiring, not only the creation of opportunities for Indigenous participation, but also a willingness by settler researchers to locate their privileged position within a context of colonization. As a result, these studies seek to challenge, not only what is researched and who carries it out, but how the research is conceived, designed and conducted. Bottorff et al. (2009) and Varcoe et al. (2010), for example, adopt a decolonizing approach by reframing commercial tobacco use through Indigenous epistemologies and methodologies. Daley et al. (2006) apply a critical anthropology framework to understand the meaning of tobacco use and related illnesses within the context of colonization. The approach and methods adopted by Bosma et al. (2014) begin with recognition of the need for researchers to honour Indigenous sovereignty. All four studies reflect on how historical and ongoing colonization impacts Indigenous health, including structuring relationships between researchers and Indigenous peoples. Four further studies (8%) incorporate Indigenous ways of knowing into their research. By honouring Indigenous knowledge positions, and Indigenous peoples as experts, these studies facilitate understanding of research in Indigenous terms. For example, Glover, Kira and Smith (2016) ground their approach—to develop programmes for reducing smoking by pregnant women—in Te Whare Tapa Wha, a model for understanding Māori health based on the four interdependent cornerstones of tinana (physical realm), hinengaro (emotional and mental aspects), whānau (family and social environments) and wairua (the spiritual realm). By applying an Indigenous knowledge framework, they are able to recognize that previous interventions relied on individual action without considering the importance of smokers’ relationships with others and their environment. Together with the community, they then develop an intervention based on the whānau component by engaging “aunties” as community health workers connected with pregnant women.
Overall, this review suggests that more meaningful engagement of Indigenous peoples in commercial tobacco control research should begin with careful reflection about philosophical assumptions and the positionality of the researchers in the context of colonization. Research approach, in turn, shapes decisions about research design and methods. Where researchers critically acknowledge the role of mainstream health research, as a construct of ongoing colonization, the studies engage Indigenous peoples across more steps of research (see above). This suggests choices about approaches and methods are integral to achieving more meaningful engagement, involving Indigenous peoples in designing how the research is conducted from start to finish.
Discussion: lessons for advancing meaningful engagement with Indigenous peoples in commercial tobacco control research
This article conducts a scoping review of 63 studies of commercial tobacco control which self-describe research engagement with Indigenous peoples. While there is now broad commitment, within the health research community in settler countries, to comply with recognized guidelines and Indigenous scholarship setting out core principles and values on the ethical conduct of research involving Indigenous peoples, there remains limited guidance of how to put these into practice. Our review suggests that there is wide-ranging and evolving practices based on differing interpretations of what constitutes meaningful engagement. As a contribution towards informing better practice, this scoping review assesses the identified studies around five questions concerning different aspects of engagement.
There are a number of lessons arising from the findings of this review. First, the studies suggest that meaningful engagement begins with the involvement of Indigenous peoples in conducting research, ideally as principal investigators and lead authors, but also as co-authors, researchers and advisors. At least 46 studies (73%) involve an Indigenous (co)author, 13 (21%) as lead authors, all but four published since 2009. This suggests a positive trend perhaps towards increasing Indigenous research capacity, a trend that could be supported by increasing recruitment and training of Indigenous peoples, including community members from study settings. Moreover, capacity building of non-Indigenous researchers, to conduct research with Indigenous peoples in ways that uphold core principles and values, is needed. An important lesson, for deepening commitment to meaningful engagement, is thus the need to integrate mutual learning and capacity building, in ways that enable knowledge production and dissemination to be genuinely collaborative and shared.
Second, meaningfulness of engagement can be reflected in how a study population is defined and selected. Who is deemed appropriate for researchers to engage with varies substantially between settler and Indigenous ways of knowing. Mainstream sampling methods, to optimize efficiency, scientific validity or generalizability, should recognize Indigenous world views which value social relationships, respect towards key knowledge holders, and benefits sharing. This requires acknowledgement of a major difference between reductionist western methods focused on the individual, and Indigenous approaches which prioritize relationships and communities. An understanding of these latter approaches, and integration into research design, requires genuine consultation with Indigenous peoples.
Third, this review suggests that the purpose of commercial tobacco control research has been largely defined by settler researchers rather than Indigenous peoples. While many studies seek to adapt interventions (most often prevention and cessation) to be culturally appropriate, and then test their effectiveness among Indigenous peoples, the purpose of such studies are generally framed in deficit or problem-based terms. This, in part, reflects a strong emphasis in commercial tobacco control research on modifying lifestyles behaviours as risk factors. An important lesson from this review is the need to critically reflect on how the purpose of commercial tobacco control research is framed in these ways and by whom. The need to understand the societal factors that shape individual decisions, supported by the development of strengths based approaches, are important alternatives to the mainstream interventions that have been less effective at improving health and wellness among Indigenous peoples.
Fourth, engagement of Indigenous peoples in commercial tobacco control research tends to take place during the middle steps of research. Self-reported engagement is most often in the form of Indigenous peoples as study subjects during data gathering and, to a lesser extent, as contributors to the actual research process during specific steps. There is limited engagement during early steps, when critical decisions are made about the research purpose and design, and the later steps when the resulting knowledge is articulated, shared and evaluated. This includes essential processes for achieving ongoing consent from Indigenous peoples. An important lesson from this review is that researchers should consider how they might extend engagement, as far as possible, across all eight steps of research to make it more meaningful. The planning of research should span from relationship building to the need for reflective practice to evaluate the research process. On the latter, the development of an agreed framework to carry out process evaluations of research involving Indigenous peoples is recommended. As well as encouraging critical reflection on how a specific study has been conducted, cumulative process evaluations can lead to lessons to support better practice in Indigenous health research more broadly.
Finally, 16 (25%) of the studies reviewed adopt CBPR and PAR approaches, as a starting point for establishing collaborative relationships with Indigenous peoples, and potentially addressing inequities in power between researcher and subject. An additional eight studies (13%) adopt approaches which are reflexive or based on Indigenous ways of knowing. As Rix et al. (2019) write, “[r]eflexive practice is essential for any researcher in examining their motivations and intent in working with Indigenous people.” The majority of studies, however, either do not explicitly identify their philosophical assumptions and positionality, or adopt mainstream approaches that lead to limited engagement with Indigenous peoples. These approaches are based on public health research paradigms which favour positivist, hypothesis-driven epistemology which are then tested against settler-defined world views (Carlson, 2016). This contrasts with grounded approaches which iteratively engage with Indigenous peoples in the conceptualization and design of research. The research thus emerges from engagement, rather than set out a priori, with engagement ongoing and embedded in the research approach. An important lesson emerging from this review is that researchers, funders, peer reviewers and publishers must prioritizes meaningful engagement.
Conclusion
To improve the relevance and effectiveness of public health efforts, to reduce the health disparities arising from higher rates of commercial tobacco use among Indigenous peoples, tobacco control research needs to strengthen engagement with Indigenous peoples. This scoping review finds increasing commitment to engagement based on recognition of the ineffectiveness of mainstream interventions. This commitment is also aligned with evolving guidelines and Indigenous scholarship which set out core principles and values for conducting research involving Indigenous peoples. However, reviewing the nature of engagement to date in commercial tobacco control research, we find varying practices. Meaningful engagement of Indigenous peoples can be advanced by critical reflection on who conducts the research, whom is engaged with, for what purpose, at what steps of the research, and using what approaches. In this way, we argue that commercial tobacco control research is more likely to contribute to improved health and wellness.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been conducted as part of the Promoting Indigenous Led Approaches to Respecting (PILAR) Tobacco Project funded by CIHR Project Grant FRN# 379337 and the First Nations Health Authority Respecting Tobacco Program.