
Abstract
Background:
Creating Vascular Access Teams (VAT) provides an expert nursing role that contributes to the training and continuous improvement of healthcare personnel. They can offer greater clinical safety, reducing complications and costs. Peripherally inserted central catheters (PICCs) and midline catheters (ML) can be safe and cost-effective alternatives to other types of venous access (VA). The aim of the study was to analyse our centre’s VAT first 12 months of activity. The primary outcome was reported complications. Secondary outcomes were cause of catheter removal, consultancy activity and economic impact of VAT implantation.
Methodology:
A longitudinal, descriptive study was carried out from March 2019 to March 2020. Using consecutive sampling, all VA inserted, and all consults received were included. Patients under 18 years of age were excluded.
Results:
The VAT inserted 1257 catheters into 1056 patients (291 MLs, 966 PICCs). The mean dwell time was 14.9 days for MLs and 59.07 days for PICCs. The main reason for removing VA was end of treatment (80.7%). During VA follow-up confirmed infection was detected in 1 ML (0.3%) and nine PICCs (0.9%). Symptomatic thrombosis was reported in 2 MLs (0.7%) and 16 PICCs (1.7%). The VAT received 367 consultations, and the main reason for consultation was to resolve doubts regarding the management of VA (80.9%). The insertion of ML and PICC catheters represented annual estimated economic savings of €867,688.44€.
Conclusions:
Our study provides a detailed analysis of VAT’s activity, its relevance to clinical safety, and to efficient resource management within our hospital. It demonstrates how VAT establishment can be a safe and efficient intervention that enhances care quality.
Keywords
Introduction
The management and care of venous access (VA) falls within nurses’ responsibilities. Nurses must constantly update themselves to maintain technical competence 1 and reduce potential complications associated with the insertion and management of VA. The continuous evolution of intravenous therapy has led to the creation of the role of VA expert nurses.2–4
Vascular Access Teams (VAT) assess, insert, manage, perform surveillance, analyse their service data, solve clinical concerns and where possible remove unnecessary VADs.5,6 They also educate nursing staff and physicians in VAD care 6 . VATs may help to standardise VA care 7 and increase adherence to evidence-based practices, 4 helping ensure the use of the most appropriate device considering evidence-based guidelines and clinical evaluation. VAT could reduce the waiting time for central VA placement and catheter-related bloodstream infection (CRBSI).5,7,8,9
In recent years, midline catheters (MLs) and peripherally inserted central catheters (PICCs) have been postulated as a safe and economical alternative to centrally inserted central venous catheters (CICCs).10,11 This has meant a reduction in CRBSI and the disappearance of iatrogenic pneumothorax.8,10,12 They can be inserted at the bedside, providing greater comfort to the patient whilst respecting insertion clinical safety.11,13
The adaptability of PICCs allows for the administration of medium- to long-term treatments. Being central, they can also administer irritant and vesicant treatments, and parenteral nutrition (PN). 13 PICCs have a low complication profile, are cost-effective 14 and easy to remove. However, they are not exempt from complications, especially thrombosis, CRBSI, obstruction and accidental removal.15–17
MLs are recommended for treatments up to 1–4 weeks. They are adequate for patients with difficult venous access and may represent an economic benefit when considering their early insertion. 10 Since MLs are not a central access, they are not recommended for the administration of vesicant therapy, Parental Nutrition (PN) or infusions with pH <5 or >9, or osmolarity <750–850 mOsm/l.18,19 Despite not being central, they are also not exempt from complications, such as thrombosis.20–22
To the best of our knowledge, there are no randomised studies assessing the matter, but many pre-experimental and observational studies consistently argue that establishing a VAT could be beneficial by decreasing the incidence of CRBSI and reducing costs.23–25 VAT implementation appears to be feasible, safe and cost-effective.14,25 In 2011, our centre created an exclusive VAT for onco-haematological patients. In 2019, the centre’s management implemented a transversal intravenous therapy programme, with a VAT aimed at placement, monitoring, incident resolution and VA training, structured within a scientific evidence framework.
Most of the published studies that have analysed the implementation of a VAT have focused on critically ill patients or those with onco-haematological malignancies.26–29 In this study, we analyse the VAT activity of a tertiary hospital during its first year of implementation in three medical and surgical clinical specialities.
Our aim was to analyse the VAT’s activity for 12 months since its implementation in March 2019 in three medical and surgical specialities of a tertiary hospital. The primary outcome was reported complications. Secondary outcomes were cause of catheter removal, consultancy activity and economic impact of VAT implantation.
Methods
Description of the intervention
The main objective of VAT is the adequate management of the venous capital of hospitalised patients. It aims to promote a culture of VA care that guarantees patient safety, quality of care, cost reduction, resource efficiency and the creation of an expert and up-to-date group on VA, a reference for all professionals at our centre.
To this end, a mandatory 7-h theoretical-practical training programme was developed for nurses, alongside informative sessions for physicians. A VAT comprising two nurses was created, with timetables from 8:00 a.m. to 3:00 p.m., Monday to Friday. Both nurses were part of the specific VAT for patients with onco-haematological malignancies and, therefore, had extensive training and experience.
The functions of our centre’s VAT are synthetised in Figure 1.

Functions of the VAT.
The VA insertion was performed at the patient’s bed or the VAT consultation room, after receiving informed consent from the patient. Inserted catheters were 4 Fr 1 lumen MLs (Midclavicular tip positioning), 4 Fr 1 lumen PICCs or 5 Fr 2 lumen PICCs. No catheters occupying more than 45% of the vein diameter were inserted. 18 An ultrasound-guided technique was used, maintaining maximum barrier protections and applying 2% alcoholic chlorhexidine as a skin disinfectant. The catheters were secured with the StatLock® fixation system. The location of the PICC tip was confirmed with either a chest X-ray or IC-ECG system. Maintenance of the inserted VA was carried out by the nursing team responsible for the patient, who could consult the VAT, if necessary.
Study design, setting and dates
A longitudinal, descriptive study was conducted between March 2019 and March 2020.
The study was carried out in a tertiary-level public university hospital. The patients who required the insertion of a VA by the VAT were hospitalised, receiving at-home hospitalisation or outpatient care in three pilot clinical specialities: gastroenterology and metabolic medical specialities, a liver ICU; traumatology and orthopaedics, otorhinolaryngology, maxillofacial surgery, general and gastrointestinal surgery; medical and radiation oncology, and haematology. On exceptional occasions, VA placement was requested by other services.
Participants
Through consecutive sampling, all VA inserted by the VAT (PICCs and MLs) and all consultations received were included. We excluded patients under 18 years of age.
Variables and variable measurement
The demographic data of the patients, the reason for placement of the VA, the savings gained by its insertion, the characteristics of the VA and the appearance of complications during insertion were collected prospectively.
The consultations made to the VAT by the rest of the nursing professionals, as well as the reason and interventions carried out, were also collected prospectively. The analysis of this activity made it possible to record all VA-associated complications (having been placed or not by the VAT) reported to the VAT.
In the event of removal of the VA due to suspicion of infection, the microbiology service assessed whether CRBSI criteria were met. CRBSI was defined as the presence of at least one positive blood culture obtained peripherally in a patient with a VA and clinical signs of infection, and with no other identifiable focus of infection. At least one of the following criteria also had to be met: the obtention of positive catheter culture 2 h before the peripheral culture, or significant isolation of the same microorganism in the catheter tip culture, or 3:1 ratio of colony-forming units (CFU) per millilitre in catheter culture. 31
For the economic analysis, prices were provided by the economic management of the hospital. These included material and labour costs. The cost reduction was calculated by subtracting the price of the implanted catheters (PICC or ML) from the avoided catheters (CICC or Implanted Central Venous Access Port (IVAP)). At-home hospitalisation day costs were subtracted from general hospitalisation costs and multiplied by the specific number of avoided inpatient days.
Data sources
Since the VAT implementation, all consultations received and VA inserted were recorded in an Access database. Subsequently, the VAT monitored the VA inserted to determine dwell time and reason for removal. Associated complications were recorded whenever the VAT was informed of their presence.
Bias
It is plausible that certain complications were not notified to the VAT and were resolved independently by nursing staff, therefore not being registered. Consequently, the results from follow-up complications should be carefully analysed and interpreted.
Statistical analysis
Qualitative variables were described with absolute frequencies and percentages. Quantitative variables were described by mean and standard deviation. Comparisons of categorical variables were made using the chi-squared test, and the t-student test for independent samples was used for continuous variables. Values of p < 0.05 were considered statistically significant. Statistical analysis was performed using the statistical programme R version 4.1.0. for Windows.
Ethical considerations
The study protocol was approved by the centre’s Ethics Committee. The study was carried out in compliance with the Declaration of Helsinki (version in force; currently Fortaleza, Brazil, October 2013) and in accordance with Law 14/2007 of July 3 on Biomedical Research. Personal data were pseudonymised, preserving their relationship with the original patient in a separate document.
Results
During the 12-month study period, the VAT inserted 1257 catheters in 1056 patients (291 ML, 23.2% and 966 PICC, 76.8%). Mean waiting time for placement was 0.13 days (range 0–4 days). The mean dwell time for MLs was 14.9 days (SD 19.9) and 59.1 days (SD 68.3) for PICCs, respectively. Demographic and clinical patient data, and characteristics of the inserted catheters are synthesised in Table 1.
Descriptive analysis of the sample.
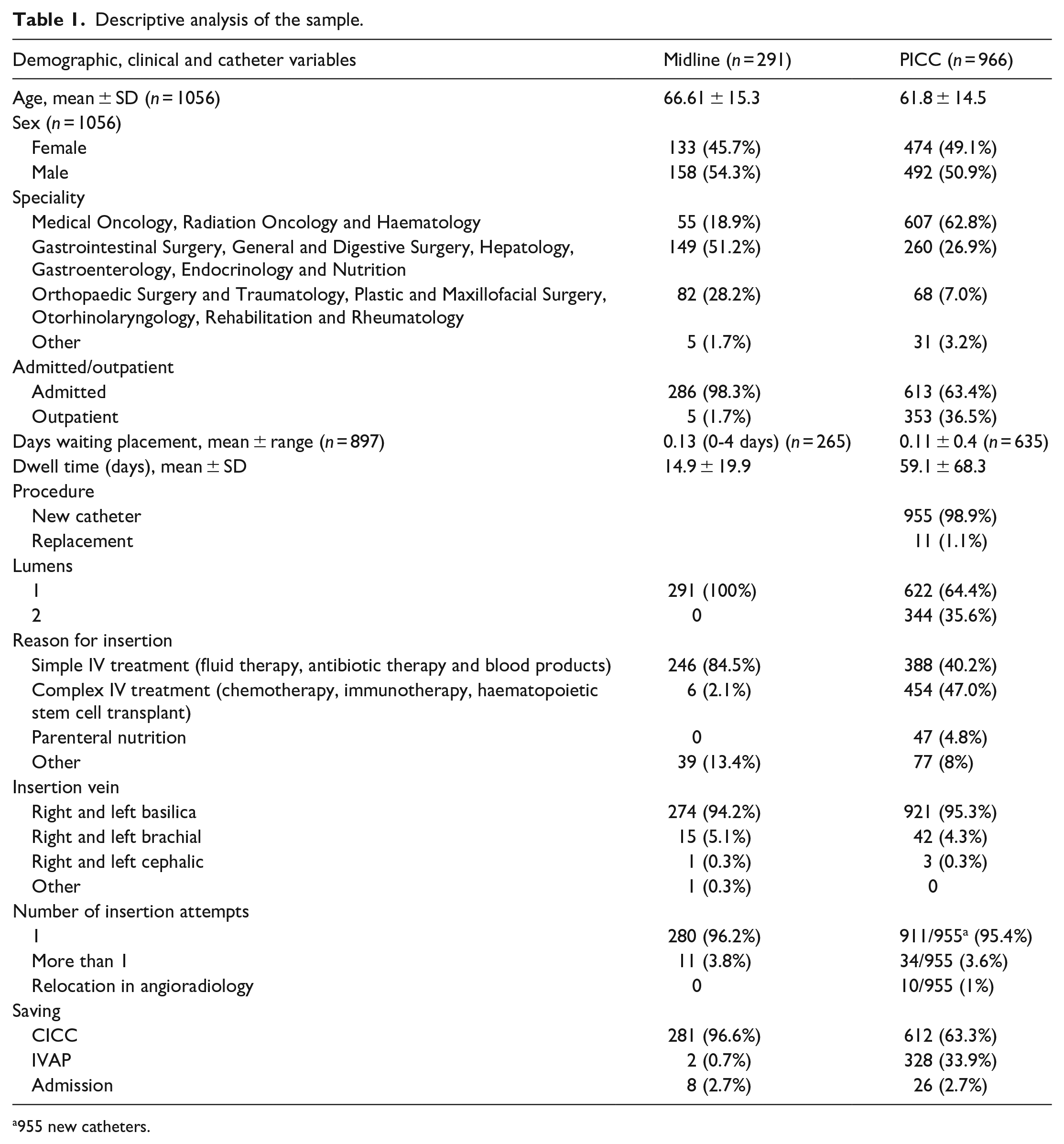
955 new catheters.
Fifty-nine PICCs could not be inserted: 15 due to non-progression of the catheter; four due to a vein of insufficient calibre or an inability to maintain the vein/catheter ratio <45%; 17 due to clinical reasons; and seven due to patient rejection. Of the 16 MLs not inserted, seven were for clinical reasons and three due to patient rejection.
Reasons for removal
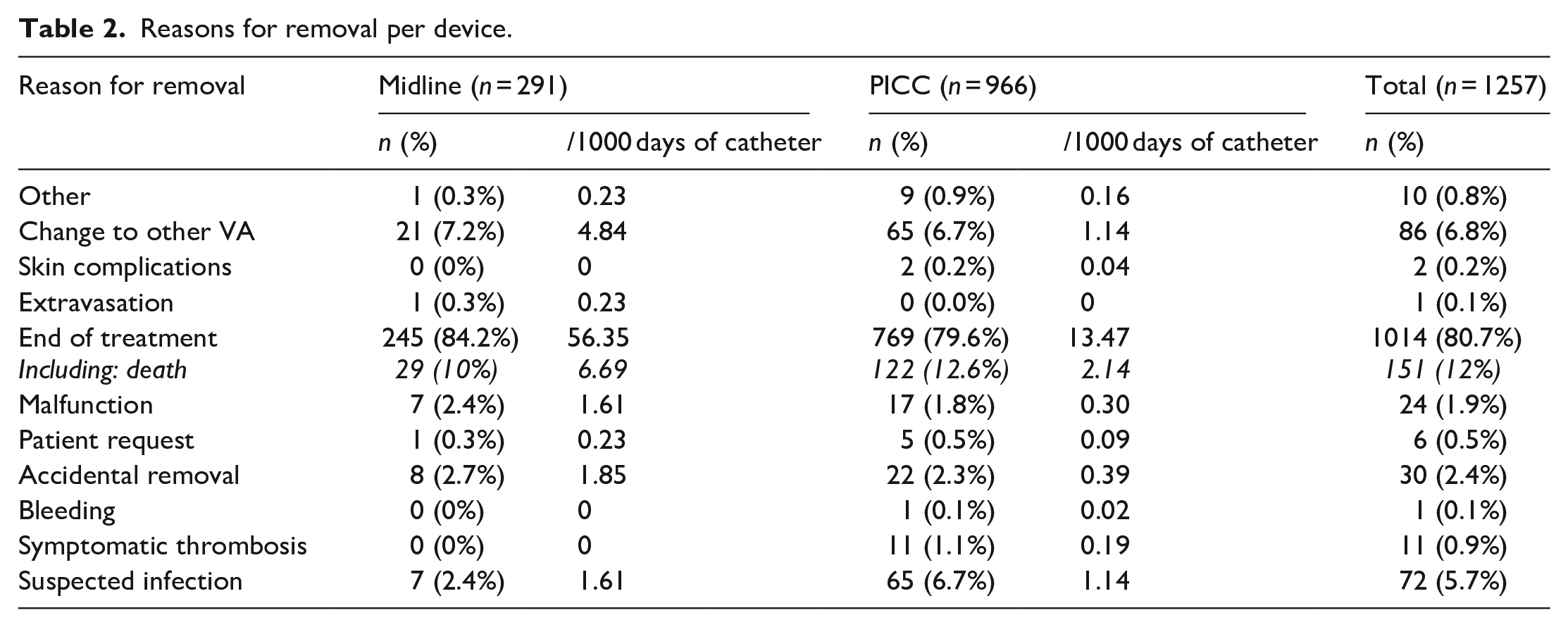
The main reasons for removal at a global level were the end of treatment (1014 – 80.7%) and the change to another VA (86 – 6.8%) (Table 2).
Reasons for removal per device.
Reported complications
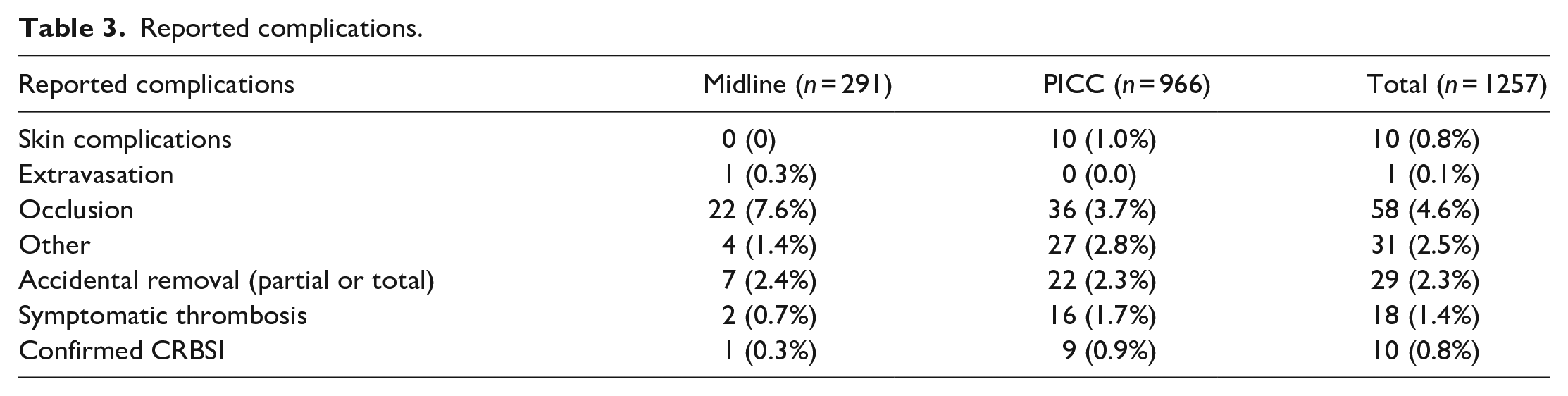
Reported complications are synthetised in Table 3. The main complication reported to the VAT was occlusion in ML’s (7.6%) and PICCs (3.7%). Of the 76 suspected infections reported, CRBSI was confirmed in one midline and nine PICCs (Table 4).
Reported complications.
Suspected versus confirmed Infection breakdown.

Cost analysis
An estimated economic saving of €867,688.44 was achieved in 1 year, including material and labour costs (Figure 2). The insertion of PICCs and MLs avoided the placement of 893 CICCs and 330 IVAPs, implying an estimated economic saving of €794,538.44. Furthermore, 34 patients (8 ML and 28 PICCs), who would have required hospitalisation, were able to receive treatment with at-home hospitalisation. 488 days of hospitalisation were avoided, meaning an estimated economic saving of €73,150.
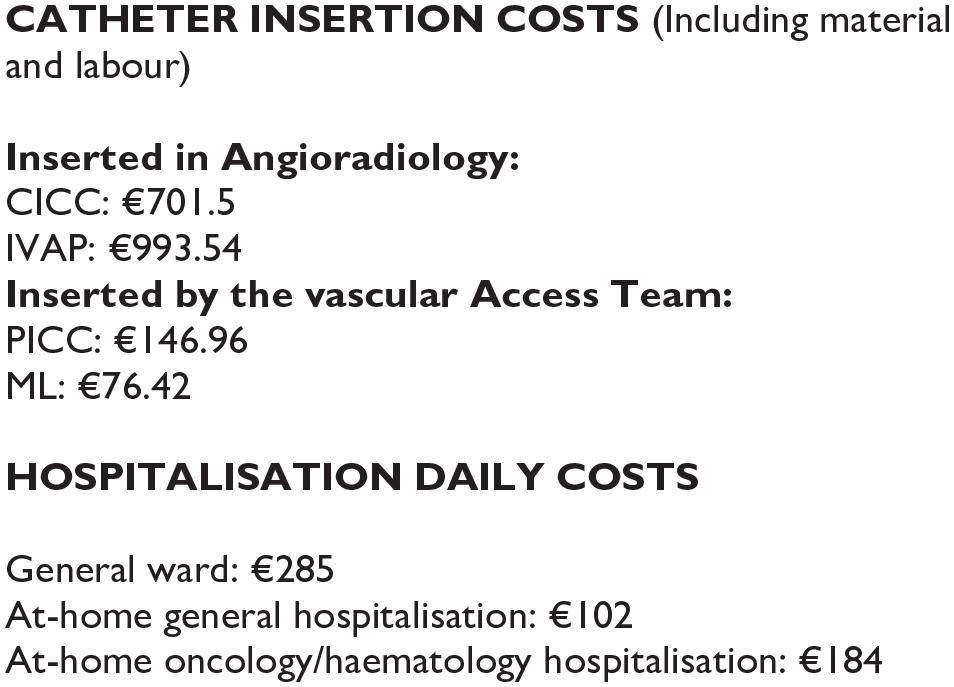
Catheter insertion and hospitalisation costs.
Consultancy activity
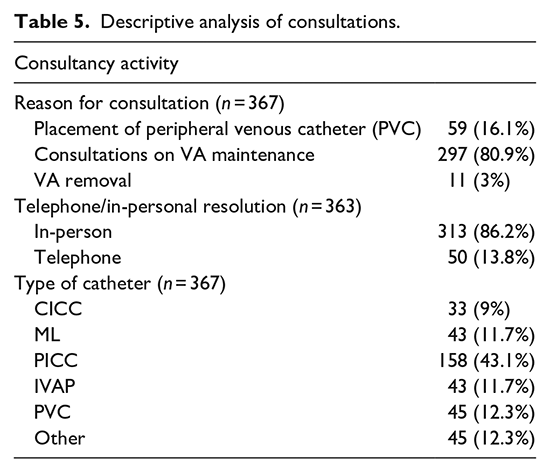
During the first year of activity, the VAT received 367 consultations, of which 86.2% (313) were resolved in person. The reasons for consultation and derived activity can be seen in Table 5. It should be emphasised that these consultations were related to the VA placed by the VAT and to other VA inserted by other professionals. The main reason for consultancy, 80.9% (297), was to resolve doubts regarding VA care or to report complications.
Descriptive analysis of consultations.
Through the prospective analysis of the consultations, it has been possible to describe the main complications detected in the VA follow-up (provided in Table 6). The main reason for consultancy was the request to recover the permeability of VAs.
Complications detected through consultations.
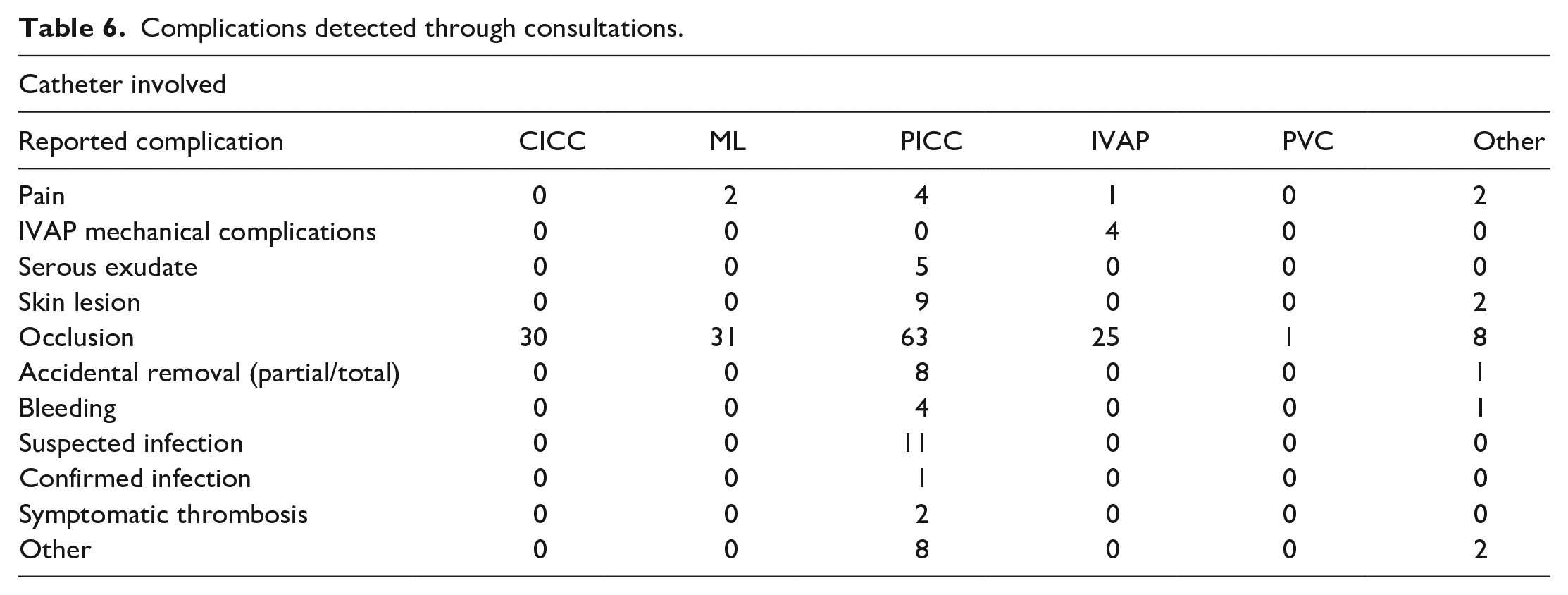
Of the 11 suspected infections reported in PICCs, bacteraemia was confirmed in one case.
Of all the consultations received, referral to angioradiology was required in 25 of 297 cases (8.41%). The reasons were IVAP placement (12, 48%); PICC revision, replacement or repositioning (3, 12%); and IVAP revision (10, 40%).
Discussion
Implementing an Intravenous Therapy Programme with a specialised VAT in our centre has appeared to be feasible and safe, in accordance with scientific evidence.8,29,32,33 The success of executing a programme of these characteristics may be based on having a team of trained nurses who are experts in VA insertion and care. In our experience, a 95.6% insertion success rate is observed in the first cannulation attempt, higher than that published in other studies.14,25,29,33 At the same time, as has been concluded in other contexts,3,7,8 the availability of the VAT could enable the insertion of the necessary and most appropriate device for the patient 6 without a waiting list and at the bedside, while reducing overall complications. 29 Given the high VAT service demand once integrated throughout the hospital, VAT hours were increased by 6.5 h to cover until 9.30 h pm. Furthermore, reduction in catheter insertion costs and avoidance of 488 days of stay made it possible to achieve an estimated economic saving of €867,688.44. In other contexts, significant cost reduction has also been observed when introducing VATs.34,35
The main reason for removal was the end of treatment (84.2% in ML, 79.6% in PICC). Although there was suspicion of infection in 8 MLs and 68 PICCs, bacteraemia was confirmed in only 1 ML (0.3%, 0.23/1000 CD) and in 9 PICCs (0.9%, 0.16/1000 CD). These results represent an improvement over previous published experiences, with some authors reporting 5.8% (0.43/1000 CD) 36 or 4.4% (1.69/1000 CD) 37 PICC related bloodstream infection (BSI) rates. Chopra et al. 38 updated integrative review indicated a global 2.25% infection incidence for PICCs and 0.67% for MLs. Nevertheless, there is still room for improvement, as other centres have published even more promising results.14,25 Considering the relevance of the health and economic implications of CRBSIs, it is essential to continue directing efforts to reduce infection rates further and increase training in the evidence-based management of suspected catheter infections in clinical teams. These efforts would prevent unnecessary removals and promote healthcare sustainability and clinical safety.
Symptomatic thrombosis was reported in 2 MLs (0.7%) and 16 PICCs (1.7%), leading to removal in 11 PICCs (1.1%, 0.19/1000 CD). These results are similar or lower to those reported by previous studies.14,16,17,25,33 We must consider that it is plausible that not all thromboses were reported to the VAT and that they were managed independently by the clinical teams responsible for the patient. Recent research20–22 indicated that thrombosis rates in MLs can be high, but, as Nickel 39 recommends, in our centre we are conservative in ML use, carefully assessing drug compatibility and expected time of use, in order to reduce its complications. This may explain our low rate of ML symptomatic thrombosis, when comparing with other recent evidence.20–22 The accidental removal rate is lower than that published in other contexts, globally being 2.4% (1.85/1000 days of catheter in MLs and 0.39/1000 days of catheter in PICCs).25,33
Finally, our study provides an analysis of one of the main functions of VAT: the follow-up and expert advice offered to other professionals in relation to VA care, which may affect the incidence of catheter complications. 3 When analysing the reasons for consultation, the necessity of this function raises attention, since 80.9% were aimed at resolving doubts.
The most frequent reason for consultation was to resolve VA occlusion, aligning with problematic reported in other contexts. 25 Systematic monitoring of complications is one of the benefits of having a VAT, 6 making them potentially more aware of complications and therefore able to address them. Consequently, the VAT carried out important training work on flushing techniques for nursing personnel.40–42
Limitations of the study
This is a descriptive and single-centre study, a fact that limits the generalisation of the results. It is plausible that some consultations carried out face-to-face during daily care practice were not recorded in the VAT database, and certain complications might have been resolved independently by the healthcare teams. Even so, we consider the analysis of the consultations to be of great interest to value the need of care professionals to receive VAT support and continuous training. Finally, considering the latest evidence, it is plausible that some occlusions were actual cases of thrombosis.20,22,39
Applicability
The main strength of this study is the joint analysis of both inpatients and outpatients across a range of medical and surgical specialities, including onco-haematological and critical patients, providing valuable insights into the daily clinical practice of a VAT in highly specialised university hospitals.
In addition, implementing the VAT at the transversal level in our centre allowed the standardisation concerning the insertion, maintenance and prevention of complications of VA. The study results enabled the promotion of targeted strategies to enhance quality of care and patient safety.
Conclusions
Implementing a VAT has enabled the insertion of 1257 catheters during its first year of activity. The mean reason for removing VA was end of treatment (80.7%). Confirmed infection was detected in 0.3% MLs and 0.9% PICCs. Symptomatic thrombosis was reported in 0.7% MLs and 1.7% PICCs. The analysis of consultancy activity highlighted the necessity for this service, with 80.9% of consults regarding doubts on VA management. The economic analysis revealed an annual estimated saving of €867,688.44. Our study provides a detailed analysis of VAT’s activity and functions as well as its relevance to clinical safety and the efficient management of resources within our hospital centre. The findings of this study have enabled the integration of the VAT throughout the hospital to ensure effective, safe and expert VA to all patients.
Footnotes
Acknowledgements
We would like to thank the healthcare nurses from the different specialities who have participated in the study. We would also like to thank the microbiology, nursing and quality departments of the hospital.
Author contributions
The corresponding author certifies that all authors meet the authorship criteria. All contributing authors consent to the submission of this manuscript for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been supported by Becton and Dickinson through a research grant. The company has not been involved with the development of the study or the content of this article, and the authors have retained full control of the data.
Ethical approval
The study protocol was approved by the centre’s Ethics Committee. The study was carried out in compliance with the Declaration of Helsinki (version in force; currently Fortaleza, Brazil, October 2013) and in accordance with Law 14/2007 of July 3 on Biomedical Research. Personal data were pseudonymised, preserving their relationship with the original patient in a separate document.