
Abstract
Background:
Haemodialysis requires a permanent vascular access and relies on cannulation with two large bore needles. Point Of Care Ultrasound (POCUS) is a tool that may assist nursing staff with visualising cannula placement and prevent miscannulation. This can be particularly useful in regional hospitals with limited access to vascular access specialists.
Aims:
To examine the impact of POCUS provision and education for nursing staff on confidence in cannulation and to understand the patient experience at three regional hospital haemodialysis units in South Australia.
Methods:
A POCUS machine and dedicated nursing education were provided at each of the three sites. A pre-test post-test model was used to assess the individual nurses perceived competency before and after the delivery of a series of online ultrasound education modules and face to face training. Patient reported outcome measures (PROMs) were collected to understand the use of POCUS from the client perspective.
Results:
There was a shift towards ‘agree’ or ‘strongly agree’ for all nursing surveys in regard to perceived competency (n = 15). This was statistically significant (p ⩽ 0.05) for all questions other than question 1 ‘I am confident in my ability to physically assess vascular access’ (p = 0.06). The patients that completed the PROMs (n = 17) overall supported the ease and use of POCUS for haemodialysis cannulation and felt that it contributed to the nursing staff competency in cannulation.
Conclusion:
POCUS has the potential to be a valuable tool in regional haemodialysis units to support vascular access cannulation and potentially avoid metropolitan transfer due to cannulation difficulties. The non-significant change post intervention for question 1 likely reflects the haemodialysis nurses inherent pre-existing capacity to assess vascular access without the use of POCUS using the standard process of visual inspection, the use of a stethoscope and palpation (‘look, listen and feel’).
Introduction
The burden of kidney failure requiring therapy such as haemodialysis (HD) continues to grow in Australia and is complicated by the increasing age of the average HD patient and the high prevalence of comorbid conditions. 1 A functioning long-term vascular access (VA) is required for HD therapy and cannulation of an arteriovenous fistula (AVF) or arteriovenous graft (AVG) is a critical component of a successful HD treatment. Our previous research has demonstrated that early miscannulation in HD is high 2 as is cannulation fear. 3 Formal ultrasound studies have demonstrated that over 80% of HD needles in use for the treatment are sub-optimally placed 4 and the use of point of care ultrasound (POCUS) to assess VA may improve cannulation success rates and optimise cannula placement.5,6 POCUS is used at the bedside to scan the length of the VA and to identify the most suitable areas for cannulation and can be used effectively for both AVF and AVG.
The use of POCUS is not widespread clinical practice in regional HD units due to the lack of equipment and the availability of nursing training. In conjunction with the introduction of units in three regional dialysis locations and a dedicated training programme, we examined the impact on nurse-and patient-reported measures of competence and confidence in cannulation.
Method
We performed a prospective evaluation of the implementation of POCUS HD nurse education and training on VA cannulation outcomes. This involved 15 staff reporting their perceived knowledge and confidence in POCUS before and after dedicated POCUS education using a competency based evaluation tool in matched pre/post pairs. 7 Although de-identified the staff placed a code on the survey pre and post so they could be analysed as a matched pair. The staff to patient ratio in HD units in SA is 1:3, staff experience in cannulation of VA varied widely from currently training in the unit to several years of experience with the service and included several Enrolled Nurses as well as Registered Nurses. Staff in two units had never used POCUS previously and the third unit had some experience with a hospital wide shared POCUS machine. We also collated data on cannulation outcomes before and after the educational intervention for prevalent patients within all three services. Patient reported outcome measures (PROMS) were also collected after the implementation of POCUS at the three sites.
Eligibility criteria
Inclusion criteria for both nursing staff and adult patients alike, were being permanently based in one of the three regional HD sites and willing to complete the survey. Patients with cognitive impairment unable to understand the purpose and intent of the study or those unable to understand and read English were excluded.
Intervention
The training programme (Table 1) was an interactive four module workshop for clinical staff in the use of ultrasound imaging techniques. The programme content was designed by a Registered Vascular Technologist, Accredited Medical Sonographer (Vascular Speciality). Modules 1–3 were delivered in an online lecture format and recorded. Module 4 was delivered face to face with interactive tasks across two site visits to each regional hospital on two occasions 4 months apart by two members of the research team (who are trained HD nurses) and an Accredited Medical Sonographer.
Outline of training programme.
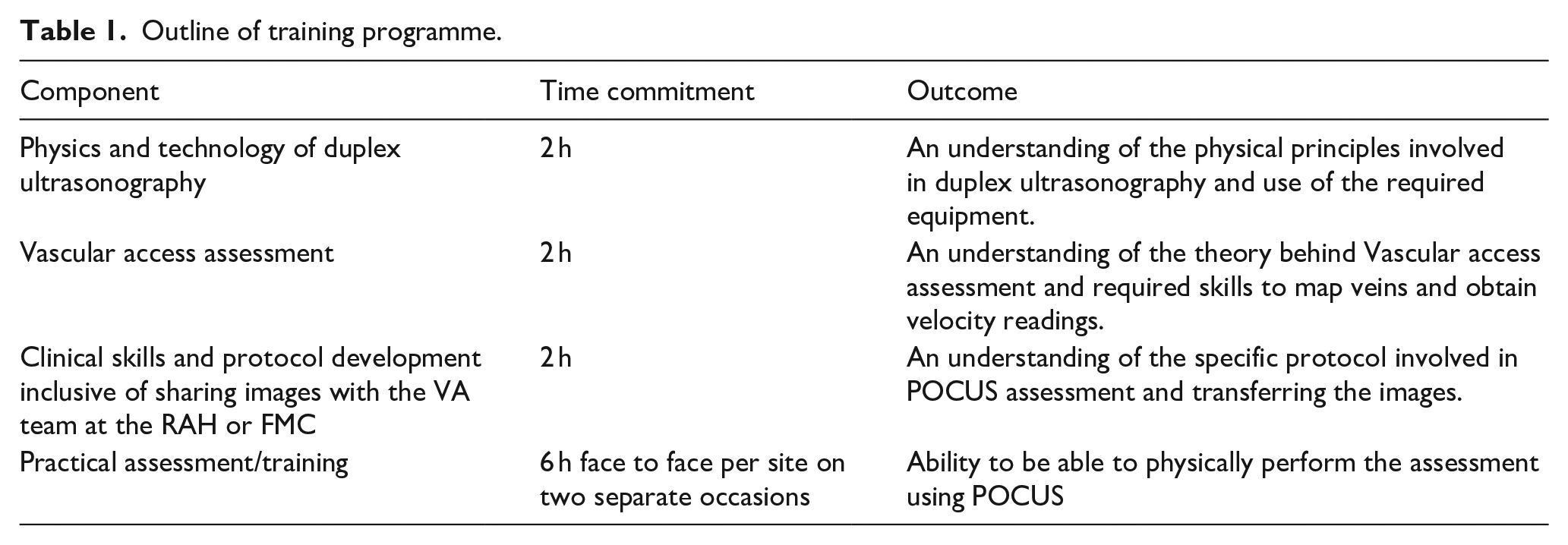
The GE Logiq V2 POCUS system was used. This produces high quality images across a broad range of applications. For data management and sending images across from regional sites to the parent hospital the assessment information can be exported in DICOM and PC formats. This allows the regional health sites to communicate their vascular access assessments easily with the vascular access team at the parent hospital.
Ethical considerations
The research proposal was reviewed by the Central Adelaide Local Health Network Research Services and granted exemption from formal ethical approval as it was deemed a quality improvement project. All nursing staff undertaking study surveys did this anonymously and voluntarily and patients gave oral consent to complete the PROM’s survey without any identifying information.
Data collection
Cannulation data
Data regarding cannulation difficulties was recorded electronically at each dialysis unit as part of routine care on the Oacis™ electronic health record platform as a HD problem. The baseline data and post intervention data collected over a 2-month period respectively reflects over 3500 needle placements as two needles are placed per treatment, treatment is performed three times a week and data was collected on n = 40 pre n = 54 post prevalent patients who were cannulated for HD across the three sites during the study time frame. In respect to VA type, South Australia has an AVF/AVG ratio of 95%/5% respectively. 2
Nursing education survey
Nurses at each site responsible for VA cannulation completed a validated POCUS competency survey pre and post the educational intervention (Appendix 1).
PROMs
Patients were asked to complete a mixed quantitative and qualitative open-ended survey to describe their experiences of cannulation, the use of POCUS and their opinions on cannulation anxiety and pain. The quantitative component utilised the validated dialysis fear of injections tool along with some open-ended questions regarding the use of POCUS for AVF assessment and cannulation (Appendix 2).
Analysis
The data pertaining to miscannulations, missed treatments, single needle treatments and VA interventions was reported descriptively. Statistical analysis of the nursing pre and post intervention survey data 5-point Likert scale used a paired t-test sample comparison. Analysis of the PROMs involved both frequencies and a qualitative thematic analysis which will underpin the future development of a quantitative survey tool specific to this population.
Results
POCUS education
The face-to-face POCUS education with sonographer support provided nursing staff the opportunity to correlate multiple ultrasound images with anatomy of a VA and the common complications encountered during cannulation. Nursing staff were able to identify the difference between a AVF and AVG, vein and artery, trauma due to needle infiltration, haematoma above and below the vessel, a thrombosis within the vessel and a false aneurysm. In addition, staff were able to locate the inserted needle within the vessel, determine if this location was optimal and manipulate if not satisfied with needle placement. Across the three sites a mixture of senior Registered Nurses (RN’s), junior RN’s and Enrolled Nurses participated in the face-to-face training across two shifts for each visit as well as several staff not rostered on duty who elected to attend in their own time.
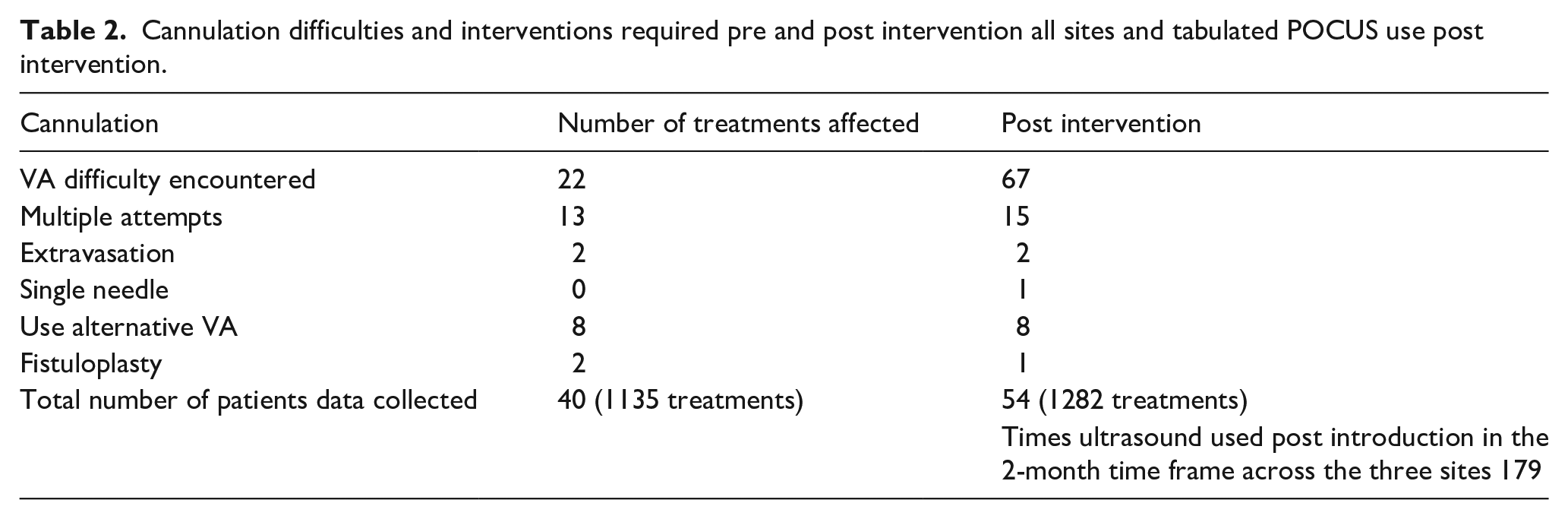
Table 2 describes the prevalence of cannulation difficulties both before and after the implementation of the nursing staff training. Table 2 also describes collated data on ultrasound use post intervention demonstrating good uptake in a short time frame.
Cannulation difficulties and interventions required pre and post intervention all sites and tabulated POCUS use post intervention.
Nursing staff questionnaires pre and post intervention
Figure 1 describes nurses perceived confidence in the use of POCUS both pre-intervention and post intervention. There was a unanimous shift on the questionnaire Likert scale from neutral, disagree or strongly agree (3, 4 and 5) with perceived POCUS confidence towards agree or strongly agree (1 and 2) for being confident across the POCUS competency domains for all nursing staff. Individual nurse pre and post confidence scores can be seen in Table A1 which describes nurse 1–4 answers at site 1, nurse 1–6 answers at site 2 and nurse 1–5 answers at site 3. This shift towards an increase in confidence was statistically significant (p ⩽ 0.05) for all questions other than question 1 ‘I am confident in my ability to physically assess vascular access’ (p = 0.06). The non-significant change post intervention for question 1 likely reflects the haemodialysis nurses inherent pre-existing capacity to assess vascular access without the use of POCUS using the standard process of visual inspection, the use of a stethoscope and palpation (‘look, listen and feel’).
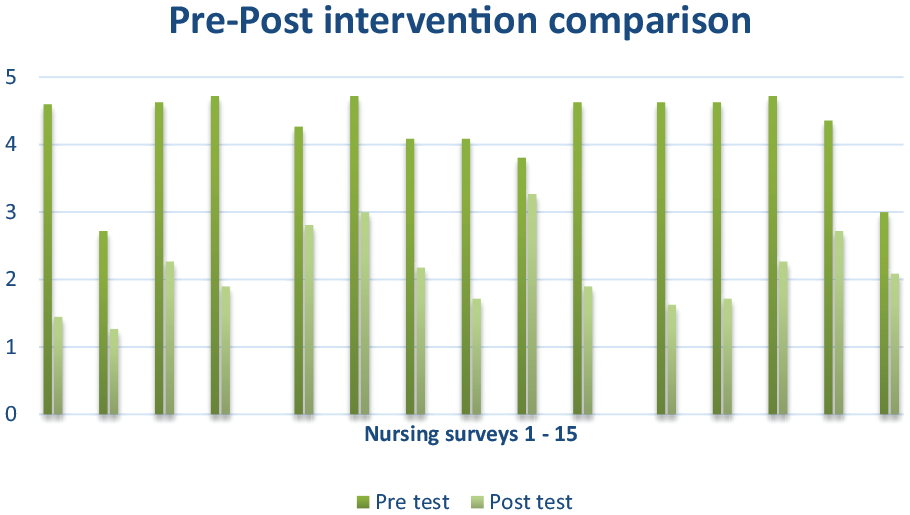
Individual nurses pre and post intervention aggregated Likert scale scores demonstrating a shift downwards towards confident (1 and 2) in the post test result.
Patient experience of POCUS
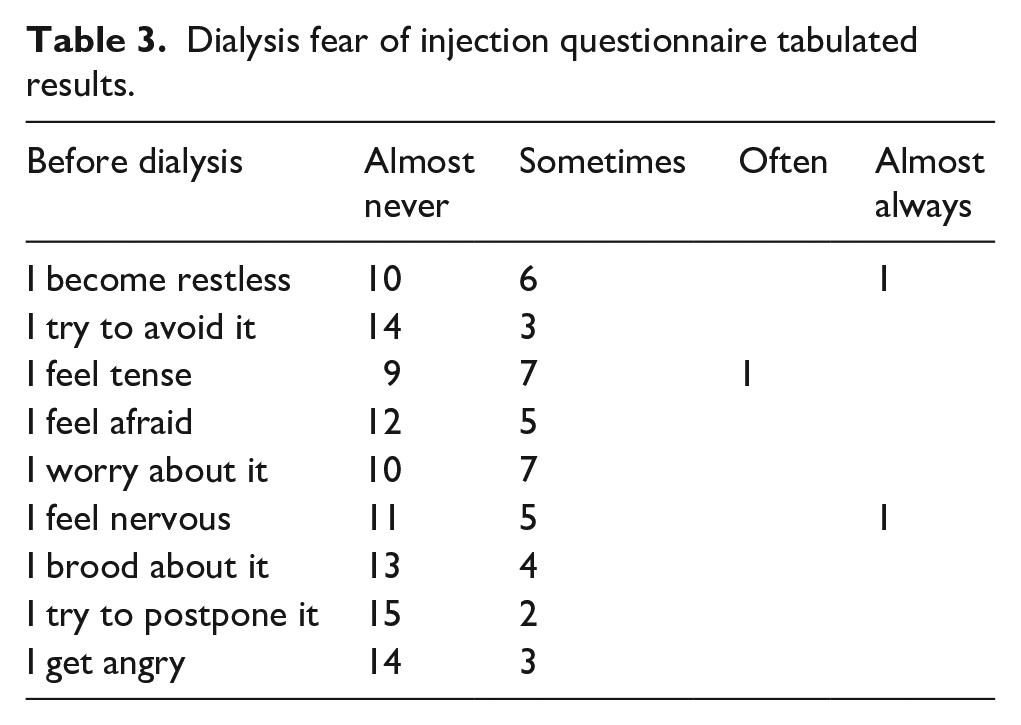
The patient PROMS provided consistent results across the three study sites with a total of 17 patients returning surveys (Table 3) which reflects all patients with an AVF or AVG that were assessed with POCUS during the second site visit (excluded patients with a CVC for HD access). In relation to needle fear before attending dialysis and the moment the nurses cannulate, some patients reported moderate levels of distress. However, patients reported this was much improved overall in comparison to when a new patient to haemodialysis, fear and anxiety was much more common at that time, particularly if cannulation difficulties were encountered. As time progressed, patients reported they became accustomed to the process, their vascular access developed and they built rapport with the nursing staff which reduced their fear and anxiety.
Dialysis fear of injection questionnaire tabulated results.
The open-ended survey questionnaire provided an important insight into cannulation (Appendix 2). When asked if needles cause pain and/or discomfort the leading responses were, ‘no’, ‘no, I use local’, ‘only when using a new spot’, ‘sometimes’ and ‘if the needle doesn’t go straight in’. When asked if patients have confidence in the nurse’s ability the answer was yes but confidence can vary between nurses, ‘newer staff or staff I don’t know often have difficulty’. The impact of POCUS on cannulation time, discomfort and confidence in needle placement was discussed. Patients reported that time taken to cannulate did increase slightly but, ‘not by much’ and if ultrasound assisted in needle placement, they ‘are happy to wait’ and ‘didn’t mind’. None of the patients reported that the ultrasound probe caused pain or discomfort when their vascular access was scanned and assessed. The resounding response to whether confidence in needle placement changed, the answer was, yes. The ultrasound, ‘helps the nurses’ which improved the patients ‘confidence in the nurse’ cannulating.
Discussion
The VA cannulation experience for HD is of concern to both patients and nurses and an aspect of care that could be further improved. This study has demonstrated an immediately visible change in practice at all sites in relation to the use of POCUS to assess VA and to find new sites to cannulate. All nurses participating in the training used POCUS on prevalent patients in their unit and in all cases identified new areas for cannulation that had not previously been used creating a change to rope ladder technique. This is an important shift in thinking, as the primary technique used when cannulating an AVF or AVG for HD is area cannulation. 8 This change is consistent with current best practice guidelines which promotes rope ladder cannulation. Identifying new sites for potential cannulation can limit the ongoing use of aneurysmal sites that can lead to weakening of the vessel walls. It is proposed that the potential benefits from the introduction of POCUS to these HD units will be best seen when used to assess the VA before the first cannulation and then ongoing in the life of the VA to identify new cannulation sites increase vessel length suitable for cannulation and reduce area cannulation and aneurysm formation. All of which could potentially increase the longevity of the AVF/AVG.
Cannulation difficulties prior to the introduction of POCUS were documented for less than 2% of treatments collated and is viewed as underreporting given the known published data on the incidence of miscannulation in HD. 2 The post POCUS implementation data demonstrates a higher cannulation difficulty rate (5%) for the treatments collated. Whilst slightly more treatment data was collected post intervention this is not thought to be the main reason for this finding. It may in part be due to the relatively short data collection period but is more likely to reflect an increase in reporting. Despite this finding, other research has found that whilst POCUS may not reduce miscannulation it does increase nursing staff confidence with cannulation and improve patient comfort by reducing pain.9,10 Pleasingly the number of times POCUS was used at each site is high suggesting immediate adaptation and change in clinical practice. In this study whilst POCUS has not had a tangible impact on reported miscannulation rates the performance aspects for nurses and patients were much improved.
The post education survey results saw a significant shift in staff confidence towards their abilities to access a VA using POCUS. The staff ‘agreed’ or ‘strongly’ agreed in their ability to identify collateral vessels, a thrombosis, use the transverse and longitudinal views and determine the difference between an artery and vein. All nursing staff felt confident to appropriately follow infection control principles to protect the patient and the ultrasound probe and document and/or refer vascular access images to the metropolitan vascular access team. The opportunity for undertaking education in each regional site was well received.
Patient reported outcome measures in relation to VA are a growing area of interest in HD and the development of a vascular access quality of life instrument (VASQol) has demonstrated a relationship between VA events for HD patients and changes in quality of life. 11 However there are currently no standardised PROMs for HD vascular access in relation to POCUS 12 and studies of vascular access in the USA did not assess the use of POCUS. 13 This study has provided some insight into the early development of PROMS for HD cannulation. Whilst the fear of injections reported by this prevalent cohort of HD patients is low, our previous work suggests a very high fear of injection prevalence of more than one-third in HD patients 3 and our previous work collating miscannulation in HD suggests a very high rate of early miscannulation. 2 A body of work that overall supports the importance of POCUS in HD units.
Study limitations
Covid-19 impacted the studies progress and caused significant time delays to the production of the education package and the delivery of the education package. This was compounded by the redeployment of research staff to frontline clinical care roles. In addition, there were no routinely collected VA PROMS to make comparisons with the data collected during this project.
Conclusion
This project has described the implementation of POCUS training for nursing staff in three regional HD unit. The results have demonstrated that when nursing staff are provided with tailored education, they can become proficient in the basic functions of POCUS to assess and cannulate HD vascular access. In addition, patient satisfaction when being cannulated using POCUS was high and it is hoped this early positive experience will translate into better VA outcomes.
Footnotes
Appendix 1: Nursing survey
Thank you for taking the time to complete this short survey regarding vascular access assessment in haemodialysis and the use of point of care ultrasound (POCUS). 7
Please tell us how confident are you on a scale of 1–5 where 1 is very confident and 5 is not confident at all in the following assessment items by circling the response that you feel most appropriate;
Appendix 2: Patient survey
Dialysis Fear of Injection Questionnaire (D-FIQ) 14
Date: __________
Please indicate to what extent dialysis needles are a cause of distress to you, by ticking or marking an ‘X’ the box that best suits your experience, in the past month.
Open ended survey questionnaire
Please make sure you have answered all questions. Thank you for completing this questionnaire.
Acknowledgements
The authors gratefully acknowledge the funding support for this project provided by The Hospital Research Foundation and the support given by Amanda Biddle and the Rural Health team in South Australia.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding was received from The Hospital Research Foundation. The University of South Australia financially supported the open access publication.