
Abstract
Background
Early cannulation arteriovenous grafts (ecAVGs) are advocated as an alternative to tunnelled central venous catheters (TCVCs). A real-time observational “virtual study” and budget impact model was performed to evaluate a strategy of ecAVG as a replacement to TCVC as a bridge to definitive access creation.
Methodology
Data on complications and access-related bed days was collected prospectively for all TCVCs inserted over a six-month period (n = 101). The feasibility and acceptability of an alternative strategy (ecAVGs) was also evaluated. A budget impact model comparing the two strategies was performed. Autologous access in the form of native fistula was the goal wherever possible.
Results
We found 34.7% (n = 35) of TCVCs developed significant complications (including 17 culture-proven bacteraemia and one death from line sepsis). Patients spent an average of 11.9 days/patient/year in hospital as a result of access-related complications. The wait for TCVC insertion delayed discharge in 35 patients (median: 6 days). The ecAVGs were a practical and acceptable alternative to TCVCs in over 80% of patients. Over a 6-month period, total treatment costs per patient wereGBP5882 in the TCVC strategy and GBP4954 in the ecAVG strategy, delivering potential savings of GBP927 per patient. The ecAVGs had higher procedure and re-intervention costs (GBP3014 vs. GBP1836); however, these were offset by significant reductions in septicaemia treatment costs (GBP1322 vs. GBP2176) and in-patient waiting time bed costs (GBP619 vs. GBP1870).
Conclusions
Adopting ecAVGs as an alternative to TCVCs in patients requiring immediate access for haemodialysis may provide better individual patient care and deliver cost savings to the hospital.
Introduction
Arteriovenous fistulae (AVF) are the vascular access of choice for patients requiring haemodialysis, with tunnelled central venous catheters (TCVCs) only considered as an option of necessity (1). Unfortunately, AVF usage is often limited by the length of time required for pre-operative imaging, surgery and maturation. This necessitates creation of an AVF 3-4 months prior to the anticipated date of dialysis commencement. If haemodialysis is required before this time, or if complications arise with the initial AVF creation (25%-35% of AVF fail at an early stage), then an alternative method of dialysis, generally via TCVC, is required (2).
Dialysis via a TCVC confers significantly higher risk of infection, mortality and central venous stenosis than dialysis via an AVF. A recent national Scottish study of 2666 patients revealed a 2- to 3-fold increased risk in mortality (all-cause mortality, cardiovascular or infection related mortality) and a 7-fold increase in death from septicaemia with the use of TCVCs (3). The complications of vascular access are responsible for over 20% of all hospitalisations of patients on haemodialysis and account for one-third of all in-patient renal bed usage (4). It therefore follows that a strategy of TCVC minimisation or avoidance is likely to have significant benefits both to the individual and to the health service generally.
Arteriovenous grafts (AVGs) may provide an alternative means of achieving vascular access in patients requiring dialysis who are without a mature AVF. Traditionally, AVGs have been used only when all other native venous options have been exhausted. However, the recent development of “early cannulation” AVGs (suitable for cannulation within 24 hours of insertion) allow such grafts to be considered as an alternative to TCVC. The benefits and limitations of an AVG lie somewhere between those of a TCVC and an AVF: they require significantly more initial cost in surgical expertise, time, and price, but have rates of infection and complications lower than a TCVC. Infective rates of TCVCs are 1.77 per 1000 catheter days compared to 0.5-0.6 per 1000 dialysis days for an AVG and 0.3 per 1000 dialysis days for an AVF (5, 6). The primary patency rates for AVGs range from 40%-60% (7). However, with aggressive management of thrombosis and re-intervention, secondary patency rates of as high as 90% at 1 year have been achieved in some series (8).
Early cannulation AVGs (ecAVGs) may have a role in incident patients, in whom there has not been sufficient time to create and mature an AVF prior to the need to commence haemodialysis, or in prevalent patients whose existing AVF has failed suddenly. 30%-35% of patients needing to start haemodialysis are referred for access creation less than 90 days prior to the date that they are required to commence dialysis, leaving insufficient time for planning, surgery and maturation of an AVF (9–10–11). Only 40% of patients commence haemodialysis via an AVF (12). Given that ecAVGs will permit rapid haemodialysis, we believe that it may be possible to implant an ecAVG and avoid the need for a TCVC entirely in this population of “crash-landers”. (We do not advocate the long-term use of ecAVGs in patients in whom it would be possible to create an AVF, rather the ecAVG would provide temporary vascular access until the native option had matured adequately.)
With this in mind, we proposed a “virtual study” to answer the question of whether (outside the confines of an idealised-protected trial) ecAVGs could be a better real-world alternative to TCVC in patients requiring imminent haemodialysis. We aimed to determine if ecAVGs were a practicable, acceptable and cost-effective alternative to TCVCs.
The “virtual study” is a novel concept not previously described in the literature, permitting a “real-world” observational study of current practice and comparing it to a hypothetical model of an alternative treatment strategy based on best available evidence and data collected “real-time” about the feasibility of any change in practice. It can be used to inform cost calculations, future research and the clinical implementation of any subsequent practice change. It may be useful in situations, such as the one proposed, where the implementation of any strategy involving ecAVGs as an alternative to TCVCs would necessitate a paradigm shift in nephrology thinking and service provision.
The results of our “virtual study” and the associated health economic cost-consequence analysis are presented.
Materials and methods
Ethical approval
Formal approval from the Research Ethics Committee was not required for this observational study of standard practice. Approval for data collection was obtained from the hospital Clinical Effectiveness Department.
Setting
Data were collected from the Department of Renal Surgery, Western Infirmary, Glasgow. This is a large tertiary referral vascular access centre in the West of Scotland, serving approximately 700 prevalent haemodialysis patients. There are approximately 120 incident patients annually. Around 400 vascular access procedures, including 100 complex access procedures, are performed each year.
Study design
A prospective observational cohort study of current standard practice (TCVCs) with a hypothetical comparator group (ecAVGs) and associated budget impact analysis.
Participants
This was an inclusive study. All patients having TCVC inserted over a 6-month period between December 2012 and June 2013 were included for analysis. It was anticipated that this time period would permit recruitment of a representative proportion of our dialysis population. All referrals for TCVC insertion were managed by a dedicated vascular access coordinator who identified patients and highlighted them to the research team on the day of referral.
Data collection
Basic patient demographic data (including age, sex, cause of renal failure, duration on haemodialysis, indications for TCVC insertion) were obtained from the Scottish Electronic Renal Patient Record (SERPR) system. Prior to TCVC insertion all patients were approached by a member of the research team and the features of ecAVG explained. Patients were informed of the risks of infection and central vein stenosis of TCVC. The ecAVGs were proposed as an alternative with lower infection rates than TCVC. It was explained that ecAVG would necessitate an additional operative procedure with potential risks of steal and thrombosis described. It was explained to those patients for whom ecAVG was not intended to be the definitive management strategy, that further AVF creation was still needed. Their views and opinions regarding whether or not they would accept ecAVG in place of the TCVC, if the option were available to them, were explored. These same questions were asked to the patients after 6 months’ follow-up also to assess if their opinion had changed. Ultrasound vein mapping was performed to determine the optimal placement of ecAVG and AVF. It was assumed that the ultimate aim was to achieve autologous AVF wherever possible, with TCVC with and ecAVGs used only as an interim measure. Patients were deemed anatomically suitable for ecAVG if they had an artery measuring >2.5 mm diameter and suitable venous landing site. If no upper limb option was suitable, leg grafts were considered in patients fit for general anaesthesia. Patients who had previously had access ligated for steal or who had monophasic arterial flow were excluded from upper limb ecAVG. Finally, the practicalities of ecAVG were considered: was the patient fit for surgery? Did they have significant hyperkalaemia or pulmonary oedema necessitating temporary access for haemodialysis prior to ecAVG? Was there an operating theatre available that could be used to permit ecAVG insertion and AVF creation? What delays might be involved in this process? What was the patient's definitive vascular access and how might this be best expedited? Although no ecAVGs were implanted, the answers to these questions allowed us to assess patient suitability and waiting time in a hypothetical scenario.
Follow-up
All patients were followed-up for 6 months. Treatment delays and complications of TCVCs (wait time for TCVC insertion, bed days required as a result of vascular access complications, culture-proven bacteraemia, suspected bacteraemia, antibiotic usage, line thrombosis, urokinase infusions, new TCVCs/temporary lines/AVF other line complications) were recorded. Data were also recorded on AVF creation, maturation and suitability for cannulation for dialysis, along with what form of vascular access was used for haemodialysis at the 6-month follow-up. Data were collected prospectively, so there were no missing data points and no patients were lost to follow-up. Patients who died had death recorded, and data collated prior to death was retained for analysis.
Analysis
Patient demographics and complication rates for patients having TCVC insertion are presented as mean ± SD or as a percentage of the total patient population (n = 79). Data on the practicalities and acceptability of ecAVG are presented similarly.
These data were then used to create a model for “standard” practice of TCVC insertion, including treatment delays and complications. A similar model for ecAVGs was also created using data obtained from the real-time study (acceptability derived from patient questionnaires, theatre availability and anatomical feasibility from clinical ultrasounds) and previously published rates of graft infection and thrombosis (4, 8). These models permitted a comparison of the “real-world” current practice of TCVC insertion until definitive autologous access could be created and a hypothetical model of ecAVGs used until the AVF was mature. It must be emphasised that the ultimate aim for every patient was to achieve autologous vascular access if possible. Both TCVCs and ecAVGs were considered a “bridge” to this definitive access wherever possible.
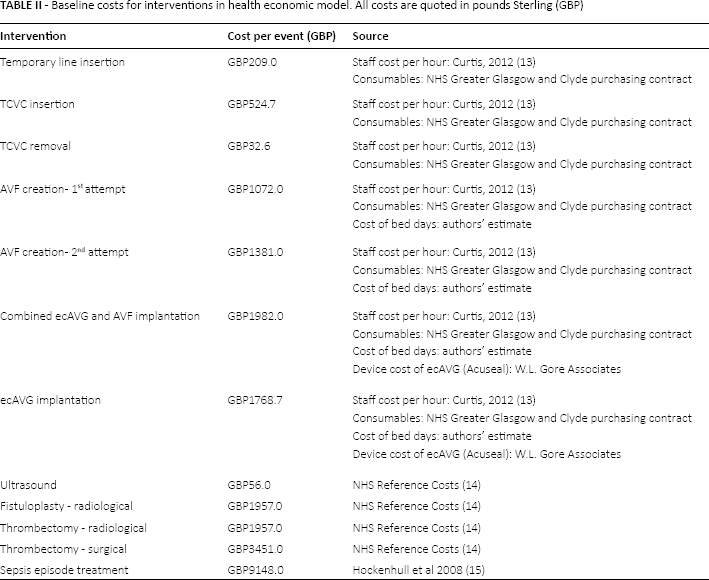
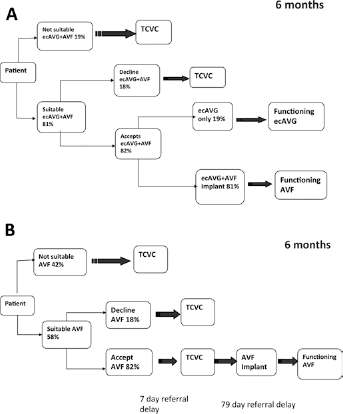
A budget impact model was used to estimate the total costs to the hospital of the two treatment strategies over a 6-month time horizon. These strategies are illustrated in Figure 1A and Figure 1B. Figure 1A reflects the current treatment pathway, where patients primarily use TCVCs as temporary vascular access while awaiting definitive AVF formation and maturation. Figure 1B represents the proposed strategy with ecAVGs replacing TCVCs where possible. To reflect real-world practice, patient suitability and acceptability for ecAVG and AVF taken from the “virtual study” was incorporated into the analysis. Clinical inputs including referral delays for treatment, complications and repeat procedures were derived directly from the observational data, internal audits and published literature. We assumed that the re-intervention and infection rates of ecAVGs were equivalent to conventional AVGs (58% secondary patency rate at 6 months (7, 8)). Access-related bacteraemia rates for TCVCs were derived from the “virtual study” data and from the published literature for AVGs and AVFs (Tab. I). The model includes costs for all initial procedures and re-interventions, in addition to treatment costs for complications including thrombosis and infection. The costs of individual procedures are listed in Table II. Resource use was based on hospital practice, and unit costs were taken from Personal Social Service Research Unit (PSSRU5) figures, NHS Reference Costs and published literature (13–14–15). All costs are quoted in pounds Sterling (GBP). A sensitivity analysis was conducted to consider varying rates for TCVC bacteraemia, referral days for TCVC insertion, and the percentage of patients using the ecAVG as their definitive access option.
Vascular access associated bacteraemia rates
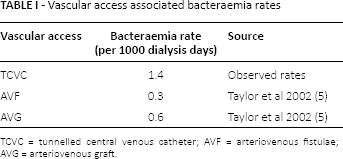
TCVC = tunnelled central venous catheter; AVF = arteriovenous fistulae; AVG = arteriovenous graft.
Baseline costs for interventions in health economic model. All costs are quoted in pounds Sterling (GBP)
(
Results
Demographics
Seventy-nine patients were assessed prior to TCVC insertion (mean age: 62.8 ± 13.1 years; 51.4% male) requiring 101 TCVCs and 40 temporary lines over 6 months. Table III outlines basic patient demographics. Reasons for TCVC usage were as follows: problems with existing AVF (22.7%), problems with existing TCVC (48.5%) and need to commence HD without functioning AVF (28.7%) (Fig. 2).
Demographics of patients having TCVC inserted
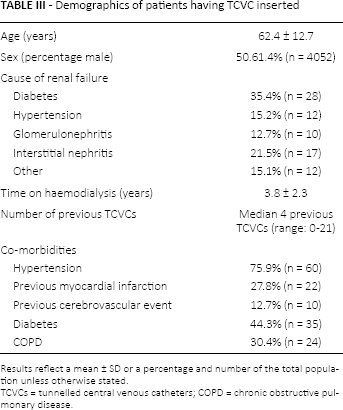
Results reflect a mean ± SD or a percentage and number of the total population unless otherwise stated.
TCVCs = tunnelled central venous catheters; COPD = chronic obstructive pulmonary disease.
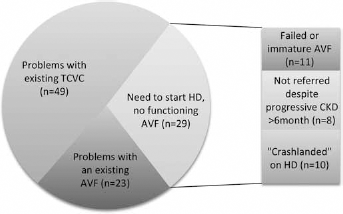
Indications for TCVC insertion. The majority of patients requiring TCVC insertion were already on haemodialysis (most having problems with an existing TCVC with a smaller number having problems with an AVF). 28.7% of patients needing TCVC were incident haemodialysis patients (who were either referred late for vascular access creation or “crash-landed” onto dialysis).
Delays and complications associated with TCVCs
Patients had a median delay of 7 days in hospital for TCVC implantation (range: 0-27). Thirty-five had discharge delayed solely due to delays in TCVC insertion (median time: 6 days). We saw 34.7% of TCVCs (n = 35) with significant complications (including 17 episodes of culture-proven bacteraemia and 13 flow-related problems) during the 6-month follow-up period. Culture-proven bacteraemia rate was 1.4 per 1000 catheter days. All episodes of suspected or proven line sepsis resulted in line replacement. This resulted in an additional 357 hospital days for line complications in 6 months. Table IV outlines TCVC complications.
Complications of TCVCs
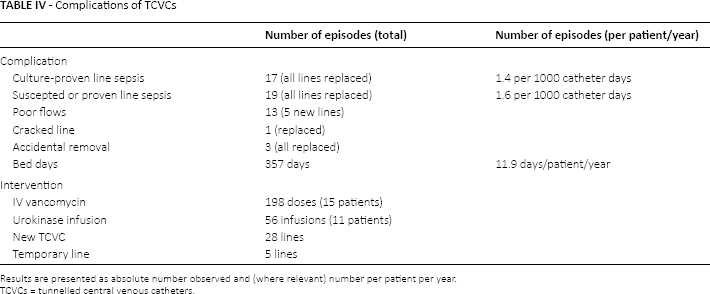
Results are presented as absolute number observed and (where relevant) number per patient per year.
TCVCs = tunnelled central venous catheters.
Definitive access
Fifty-six AVF access creation procedures were performed during the first 6 months after TCVC insertion. Median time from referral to actual AVF procedure was 79 days and 57 days thereafter for AVF maturation (until first successful cannulation). Seven patients (8.8%) died during the follow-up period and were removed from the analysis at the time of their death. One death was the result of proven line sepsis. Thirty-one patients successfully dialysed through their AVF at some point during the first 6 months, but many failed early, and only 16 patients had a functioning AVF capable of giving sustained dialysis at 6 months’ follow-up.
Acceptability and practicality of an alternative ecAVG strategy
In 66 of the 79 patients (83.5%) ecAVGs were a clinically suitable alternative to TCVC. Sixty-four patients (81%) would have been suitable for a strategy of ecAVG and AVF. A total of 13 patients were not clinically suitable for ecAVG for the following reasons: acute illness which would have precluded ecAVG (n = 5); chronically too frail or unfit for ecAVG (n = 11). Twelve (11.8%) would have required temporary access to permit haemodialysis for hyperkalaemia or fluid overload prior to ecAVG insertion.
Fifty-three patients would have accepted ecAVG as an alternative to TCVC. Thirteen patients declined ecAVGs (the majority also declined an AVF) at initial and 6-month interviews; however, these were different sets of patients. This meant that 81% of patients were anatomically suitable for an ecAVG± - AVF, and 72% of these patients would have accepted this as a treatment option (Fig. 1B). Table V outlines the acceptability of ecAVGs to patients at outset and at 6-month follow-up.
Reasons for ecAVG refusal at initial interview and after a 6-month follow-up. Thirteen of 66 patients (19.7%) declined ecAVG at each time point; however, these were not the same 13 patients and opinions were affected by experience with TCVC. Patients who had TCVC for a short period of time with rapid AVF maturation felt that ecAVG may have been unnecessary, while patients who initially would not have wished ecAVG but then experienced complications of TCVC usage, subsequently wished for ecAVG instead
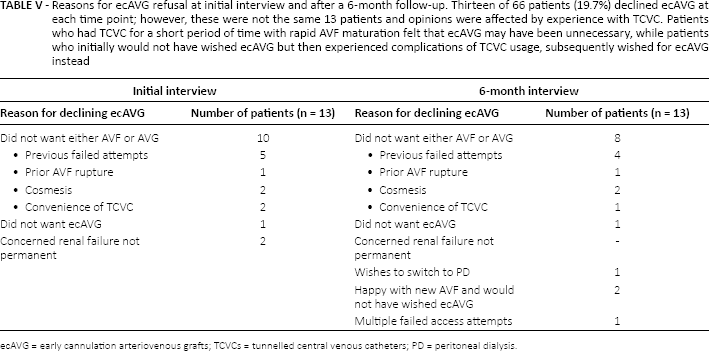
ecAVG = early cannulation arteriovenous grafts; TCVCs = tunnelled central venous catheters; PD = peritoneal dialysis.
In all but two cases, the emergency Confidential Enquiry into Perioperative Deaths (CEPOD) theatre was available within 4 hours. In these two cases a theatre slot would have been available within 24 hours and there would have been no need for additional temporary access.
There would have been 21.2% of ecAVG sited in the forearm, 69.7% in the upper arm and 9.1% in the thigh, and ecAVGs would have been the final definitive access option in 23.4%.
Budget impact analysis
Over a 6-month period, total treatment costs per patient were GBP5882 in the TCVC strategy and GBP4954 in the ecAVG strategy, delivering potential savings of GBP927 per patient in the ecAVG arm. Although ecAVGs had higher procedure and re-intervention costs reflecting longer procedure time and device costs (GBP3014 vs. GBP1836), these were offset by significant reductions in septicaemia treatment costs (GBP1322 vs. GBP2176) and in-patient waiting time bed costs (GBP619 vs. GBP1870) (Tab. VI).
Health economic analysis highlighting relative intervention and complication costs of standard practice (TCVCs) and the novel strategy of ecAVG. All costs are quoted in pounds Sterling (GBP)
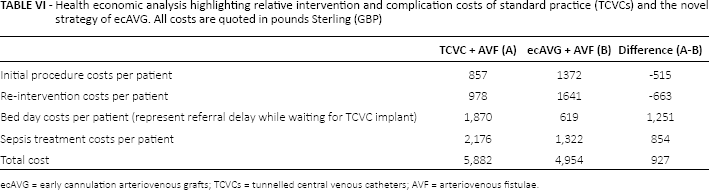
ecAVG = early cannulation arteriovenous grafts; TCVCs = tunnelled central venous catheters; AVF = arteriovenous fistulae.
Figures 3, 4 and 5 are graphical models demonstrating how the overall cost savings (or otherwise) of an ecAVG strategy may change if various factors in the model (TCVC bacteraemia rate, delay for TCVC insertion or proportion of patients using ecAVG as their definitive access option) changed. For example, the observed bacteraemia rate for TCVCs was 1.4 per 1000 catheter days. At this rate, the estimated cost savings of an ecAVG strategy are GBP927 per patient at 6 months’ follow-up. Figure 3 illustrates that if the TCVC-associated bacteraemia rate were to reduce to 1.0 per 1000 catheter days, ecAVGs would continue to derive a lesser cost saving of GBP548 per patient. Similarly Figure 4 demonstrates a lesser cost saving of GBP228 per patient if the delay waiting for TCVC insertion reduced from 7 to 3 days, while Figure 5 demonstrates greater cost savings with the ecAVG strategy if the proportion of patients using ecAVG as their definitive access option were to increase.
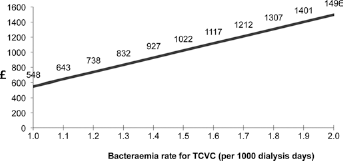
Graphical model reflecting changing cost savings if bacteraemia rate amongst TCVC patients were to change. For example, the observed bacteraemia rate for TCVCs was 1.4 per 1000 catheter days. At this rate, the estimated cost savings of an ecAVG strategy are GBP927. If the TCVC-associated bacteraemia rate were to reduce to 1.0 per 1000 catheter days, ecAVGs would continue to derive a lesser cost saving of GBP548. All costs are in pounds Sterling (GBP).
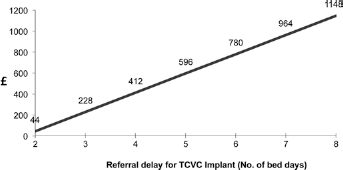
Graphical model reflecting changing cost savings if delays associated with TCVC insertion were to change. For example, the observed delay for TCVC insertion was seven days. At this rate, the estimated cost savings of an ecAVG strategy are GBP927. If the delay for TCVC insertion were to reduce to three days, ecAVGs would continue to derive a lesser cost saving of GBP228. All costs are in pounds Sterling (GBP).
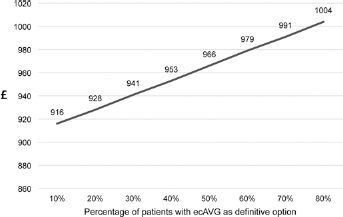
Graphical model reflecting changing cost savings if the percentage of patients using ecAVGs as their definitive access option were to change. For example, the observed proportion of patients using ecAVGs as their definitive option was 21%. At this rate, the estimated cost savings of an ecAVG strategy are GBP927. If this proportion were to increase to 40%, estimated cost savings would be higher at GBP953. All costs are in pounds Sterling (GBP).
Discussion
This study demonstrates that ecAVGs may provide a viable alternative to TCVCs in patients requiring urgent vascular access for haemodialysis. It has been demonstrated that ecAVGs are acceptable to patients and practical to insert within the confines of our busy NHS practice. Moreover, when offset against delays and complications (particularly infective) associated with current TCVC usage, ecAVGs have been shown to have cost-savings of nearly GBP1000 at 6 months over TCVCs.
A strategy of “line avoidance” has proven the holy grail of vascular access. Both short-term risks of infection and long-term risks of central venous stenosis associated with TCVC usage are associated with access loss, morbidity and mortality for patients on haemodialysis (3, 6, 16). Despite efforts to decrease TCVC usage, it has not been possible to reduce prevalent TCVC usage below 30%-35% in most units (17, 18). With “Fistula First” in the USA and governmental tariffs in England and Wales, there are now financial incentives to minimise TCVC usage (18–19–20). This study demonstrates that there may be cost savings to be derived from the policy of TCVC replacement with ecAVG itself.
Clinically, early cannulation grafts have been used for a number of years; however, published literature on their use, and indications for their use, is sparse (21, 22). In most cases they continue to be used in situations analogous to conventional AVGs, where there are no alternative autologous options. Our group has recently published information on our successful use of ecAVGs as a “bridge” to autologous AVF maturation or transplantation in selected patients (23). However, this is the first study to propose the use of ecAVG as an alternative to TCVCs for the entire dialysis population. Such a change would necessitate a paradigm shift in current nephrology thinking and resource allocation.
The approach adopted in this study is one of autologous primacy, with both ecAVG and TCVC used, wherever possible, only as a stop-gap until native AVF maturation. We advocate this approach due the well-recognised lower infection and better long-term patency rates provided by native AVF (3, 6). It should be noted however that only 16 patients had autologous access at 6 months’ follow-up. This seems low and, given the 30%-35% primary failure rate quoted in most studies of de novo AVF (4, 24) could be seen to limit the generalisability of our results. However, we believe this observation is representative of “real-world” practice and is probably comparable to other studies trying to achieve vascular access in prevalent patients (4, 10). One recent multicentre study found that more than 60% of AVFs were not suitable for cannulation at 4-5 months (24). Furthermore, dialysis via a TCVC is recognised as a risk factor for early AVF failure (4) with Weber and colleagues achieving 81% primary patency in patients who had AVF created prior to commencing dialysis, compared to only 44% in patients who had AVF created after commencing on haemodialysis (25). This highlights that the concept of short-term TCVC (or ecAVG) for only 6-8 weeks to permit AVF maturation, may be flawed and a slightly more robust, albeit temporary, vascular access may have benefits.
This work utilises the novel concept of a “virtual study” to compare “real-world” prospective data collected on standard practice (the TCVC cohort) to an innovative, but as yet unproven, hypothetical new treatment strategy arm (ecAVG). It allows real-time assessment of the practicality, feasibility and acceptability of the proposed new management strategy and can inform a health economic analysis. The model could be adapted to permit cost-analyses for business cases prior to implementation of a new treatment plan or, in our case, has been used to inform cost calculations for a future randomised controlled trial (RCT). The real-time data collection in the standard practice cohort, allows very accurate figures, often lacking from other health-economic analyses, and modelling that allows manipulation of variables such as bacteraemia rates and waiting time for TCVCs provides generalisability to other centres, which may have differing baseline rates for these factors.
The “virtual study” model uses real-life data to inform cost-analysis in the TCVC arm; however, data in the ecAVG arm are extrapolated from the literature. We intend to use data collected from this “virtual study” to inform a future RCT comparing TCVCs versus ecAVGs (26), and propose that similar studies could be used to support the conduct of other RCTs (either to demonstrate potential cost savings to sponsors, or to assist in grant applications). This study has informed the power calculation for our subsequent study, which is unique in the fact that it could be manipulated and modelled to take into account changes in practice which might occur over time or between units. The “virtual study” can also inform potential recruitment to subsequent RCTs by assessing acceptability of the novel intervention and likely refusal rates or eligibility criteria for future RCTs. This is particularly relevant in trials of heterogeneous patient groups, such as those on dialysis, where strict inclusion criteria may necessitate large numbers of patients to be screened to determine eligibility. For example, a recent New England Journal of Medicine study evaluating tissue plasminogen activator (tPA) in dialysis catheter malfunction, failed to recruit the intended 380 participants despite screening nearly 2500 patients (27). The “virtual study” has allowed us to assess likely uptake to an RCT prior to beginning recruitment. Finally, the results from our “virtual study” have been used to support our application to our NHS trust sponsor for conducting an RCT, indicating that the study will, at a minimum, be cost-neutral to the hospital. This has allowed our research to progress without the need to seek additional research funding. In an era where research costs can often be prohibitive and charitable funding is limited, demonstrating potential cost-savings achievable from conducting the research itself has proven very valuable in this case.
In conclusion, the “virtual study” is a novel research methodology that can be used to compare current standard practice to an alternative management strategy and model potential outcomes. We have used it to demonstrate that ecAVGs could provide a practical, acceptable and cost-effective alternative to TCVCs in patients requiring urgent vascular access for haemodialysis.
Footnotes
Acknowledgement
We would like to thank Belinda Mohr, Health Economist at W.L. Gore Associates for her assistance in preparing this manuscript.
Financial support: No financial support was received for this study. EAs salary was funded by Darlinda's Charity for Renal Research.
Conflict of interest: EA and DBK receive an investigator-led small research grant from W.L. Gore Associates.