
Abstract
Introduction:
Maintaining optimal central venous catheter tip position requires reliable catheter securement. A vital decision about the choice of engineered securement device is often made by what is conveniently available in the insertion kit or default clinical routine. The importance of continuous securement for oncology patients prompted the need for an evaluation of securement options currently available. This study aimed to assess the effectiveness of two engineered securement devices to assist the oncology patient in reaching the end of their catheter need.
Methods:
A retrospective study was conducted to assess patients’ ability to finish their therapy with one peripherally inserted central catheter. Implant and explant data for adult oncology patients was evaluated spanning 2007–2021. All patients received a PICC with either an adhesive securement device or a subcutaneous anchor securement system.
Results:
Partial or complete dislodgement causing the unplanned removal of the PICC occurred at 12% for ASD and 0.4% for SASS (p < 0.0001). The probability of reaching the end of need with one PICC, regardless of the reason for premature removal, at 2 years for patients with an adhesive securement device was 68% (n = 944). For patients with a subcutaneous anchored securement device, it was over 95% (n = 8313). The difference in the probability of reaching the end of the need with one PICC between the two securement devices was calculated at (p < 0.0001).
Conclusion:
With over 9200 patients and more than a million catheter days, the results of this retrospective study demonstrate the SASS’s superiority in assisting the patient to reach the end of need with a single PICC.
Keywords
Introduction
Many tests, medications, and procedures often follow a cancer diagnosis. Patients may have a peripherally inserted central catheter (PICC) placed to receive chemotherapy, nutrition, or retrieve atraumatic blood samples. 1 The tip of the PICC must remain securely in the target location until the end of the patient’s need for treatment.1,2 Accomplishing the goal of reaching the end of need with one vascular access device requires expert placement and reliable continuous securement.
Adhesive-based securement devices rely entirely upon adhering to the surface of the skin, which is subject to moisture, irritation, infection, sloughing, and injury.3,4 In addition, all the adhesive-based securement devices must be reapplied weekly during dressing changes and leave the catheter without securement during this procedure.1,2 Additionally, the adhesive-based securement repeated removal and replacement places the patient at risk for medical adhesive-related skin injury (MARSI) along with the risk of catheter movement.5 –8
Depending on the individual’s habitus, the average adult’s target area in the SVC may only be 2–3 cm in length. 9 Therefore, an incremental retraction of only a centimeter with each dressing change or incidental tug on the line will dislodge the catheter tip from the optimal position. 10 Partial or complete dislodgement of a PICC may place the oncology patient at risk for vessel damage caused by inadequate dilution of chemotherapeutics, increased risk of thrombus, catheter occlusion, and catheter replacement.1,2
In practice, the seemingly inconsequential choice of securing the catheter at the end of a procedure is as crucial as achieving the initial optimal catheter tip location. Therefore, this study was conducted to assess the effectiveness of two engineered securement devices (ESD) in assisting the oncology patient in reaching the end of their catheter need with one PICC.
Methods
Study design
The design for this research was a retrospective observational dual cohort study that analyzed data collected from 2007 through 2021. Research Ethics Committee approval was sought and granted for this study.
Setting
The Clatterbridge Cancer Centre (CCC) is one of three specialized cancer treatment centers in England, covering a 2.4 million population across Cheshire and Merseyside. Annually, 35,000 patients are treated with over 380,000 patient contacts. 11
Subjects
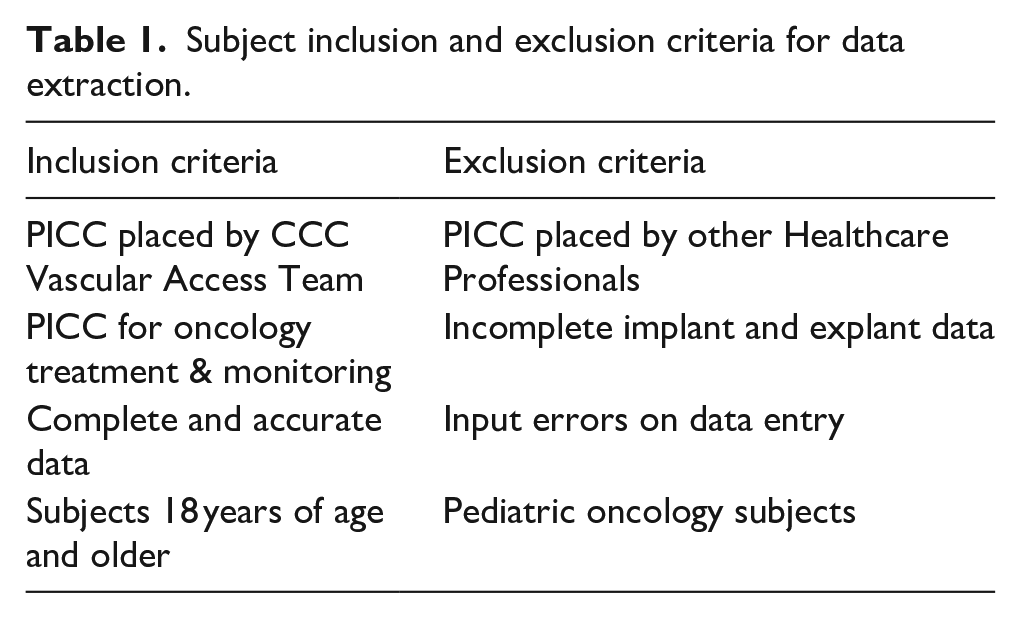
The subjects for this retrospective study were gleaned from a master database spanning from 2007 to 2021. The inclusion and exclusion criteria can be found in Table 1. All subjects received part or all of their cancer treatment from CCC. Age and gender were not a part of the master database. The primary data recorded for each qualified subject by year included; securement type, vein cannulated, insertion date, removal date, dwell time, and reason for catheter removal. Those subjects with an unknown reason for removal were excluded from the study.
Subject inclusion and exclusion criteria for data extraction.
Variables
The independent variable in this study was the type of engineered securement device (ESD) used to secure the PICC, either ASD or SASS. The dependent variables recorded were the reason for the PICC removal, including partial or complete dislodgement, reaching the end of need (EON) with one PICC, and other removal reasons. Additional data recorded by the team, but excluded from the study, varied in reliability and clarity; these included thrombus, occlusion, central line-associated bloodstream infection, and skin irritation or infection and often did not distinguish between suspected or confirmed issues.
The primary end-point for this study was assessing the patient’s likelihood of reaching the end of the need for the catheter with one PICC. The only outcomes the team sought during the data entry period were decreasing catheter replacement and improving patient outcomes, regardless of which ESD design proved superior. Bias related to outcomes according to securement was unlikely based on the initial trial period in 2012. However, the nature of retrospective studies does not support control over the cohorts and may have intrinsic bias.
Study size
The study size was not predetermined or limited. All qualified subjects with complete data from 2007 through 2021 were considered for inclusion. 2007–2011, when only ASD was utilized, totalled 571 patients. Minimal subjects with complete data were available for 2007 and 2008. By 2009 the VAT was consistently entering data on the reason for the PICC removal on every patient.
The SASS became available in 2012. 12 At the time of this study, a majority of the subjects with PICCs placed in 2021 were still in use, and therefore, this year was not included. From 2012 through 2020, ASD and SASS were used simultaneously. The inclusion flow diagram can be found in Figure 1. During the period of 2009–2020, a total of 9257 qualified subjects and 1,125,613 total catheter days were included. The two cohorts were divided into ASD cohort = 944, and the SASS cohort = 8313.
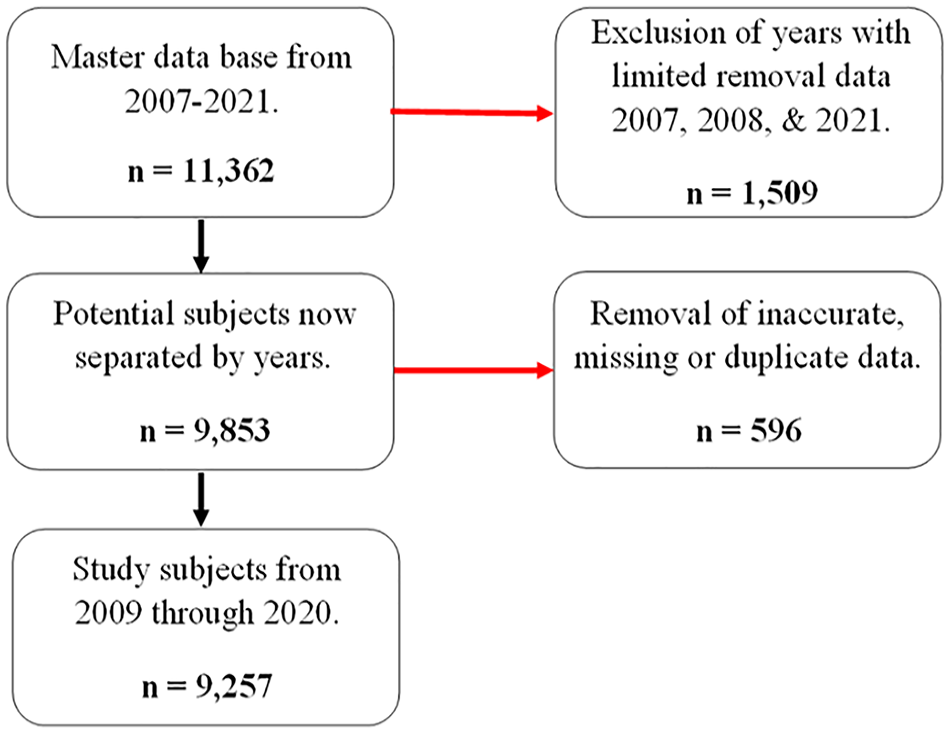
Subject inclusion flow diagram.
Statistical methods
Initial analysis and database cleaning was completed by the lead author and included computation of the years between 2007 and 2021 for incidence of the specific data points regarding the reason for removal; EON, partial or complete dislodgement, or other removal reasons. After the initial analysis, an independent biostatistician assessed the data for accuracy and provided further analysis of the two engineered securement devices’ relationship to the primary endpoint of reaching the end of need with one PICC.
Descriptive statistics were employed for dwell time median and interquartile range (IRQ). In addition, Kaplan-Meier curves were constructed for each engineered securement device, and the Wilcoxon test was used to assess statistical evidence of a difference between the survival curves. The Ghan-Breslow, generalized Wilcoxon test was chosen because it weights earlier times heavier as there was an extreme disparity between the number of SASSs and ASDs recorded over the 10-year study period.
Results
Table 2 shows data accumulated before SASS was available. This information of failure to reach the end of need with one PICC prompted the need to search for another securement option. The cumulative probability of patients reaching EON with one PICC during this period was 77%.
Adhesive securement devices 2007–2011 (n = 667).
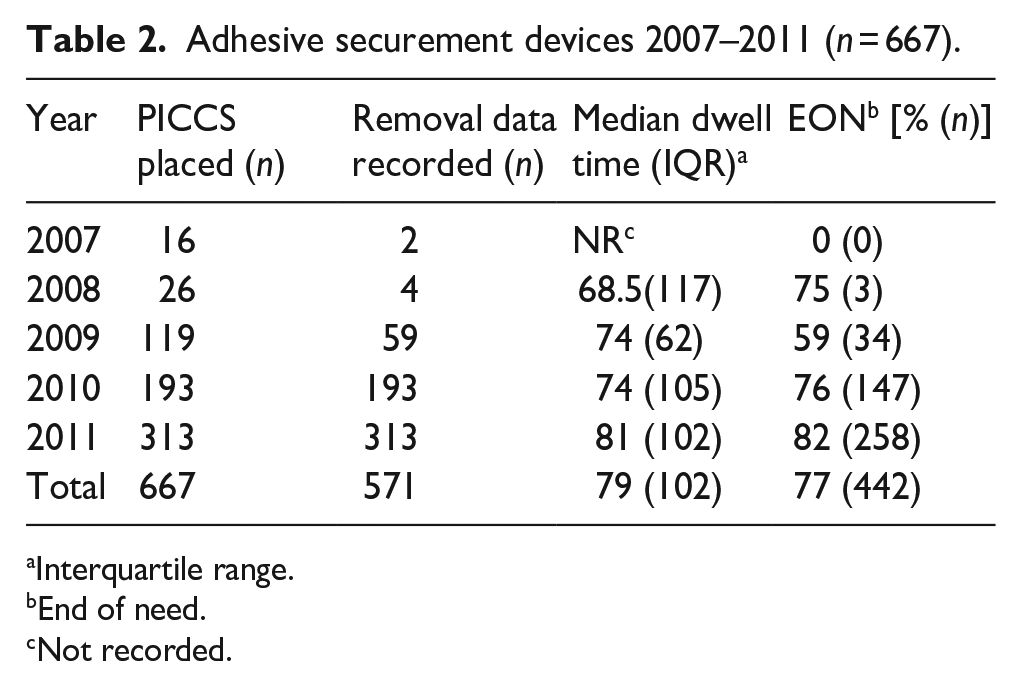
Interquartile range.
End of need.
Not recorded.
Table 3, shows the incidence of PICC removals caused directly by partial or complete dislodgement requiring replacement with another PICC, unplanned escalation to an implanted vascular access device (IVAD), or premature discontinuation of infusion therapy. The SASS achieved a less than 1% chance of migration or dislodgement every year from 2012 to 2020. The incidence of removal secondary to partial or complete dislodgement for ASD averaged over 12% for the cumulative years from 2009 to 2020. The risk ratio between ASD and SASS showed a 36 times greater risk of partial or complete dislodgement if using ASD rather than SASS. The use of ASD declined quickly after the initial trial period in 2012.
PICC removals related to partial or complete dislodgement 2009–2020.
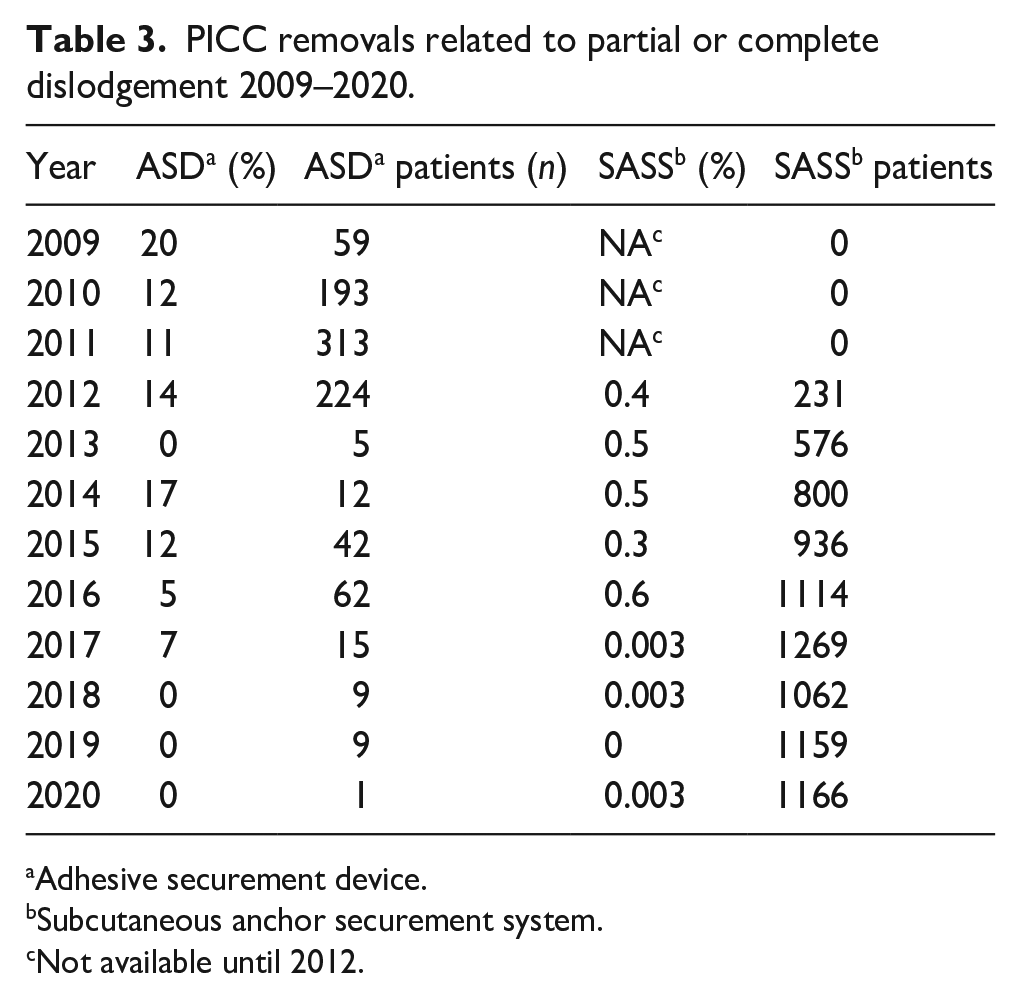
Adhesive securement device.
Subcutaneous anchor securement system.
Not available until 2012.
This study aimed to assess the effectiveness of two engineered securement devices in assisting the oncology patient in reaching the end of their catheter need with one PICC. Table 4 shows the number of patients reaching the end of need by completing their therapy, electively moving to an IVAD, or succumbing to cancer. All recorded reasons for removal are included in this table in addition to partial or complete dislodgement. By 2018 the patients using a SASS to secure their PICC had a 99% or greater chance of reaching the end of need with one PICC.
Patients reaching the end of need with a single PICC 2009–2020.
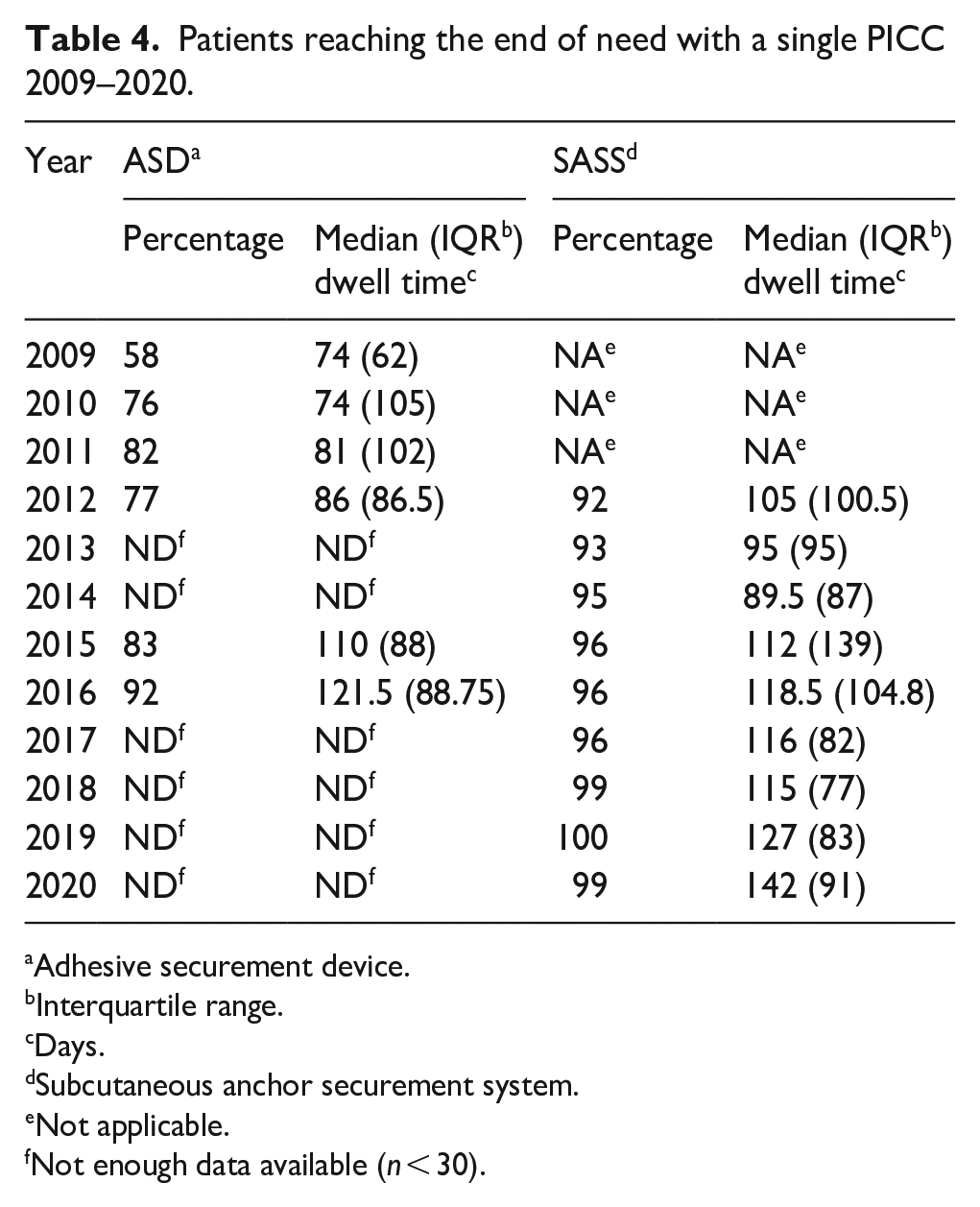
Adhesive securement device.
Interquartile range.
Days.
Subcutaneous anchor securement system.
Not applicable.
Not enough data available (n < 30).
Figure 2 shows the Kaplan-Meier survival plot of the two securement devices. Patients with SASS are much more successful in reaching the EON than those with ASD. The plot illustrates that the probability of reaching the EON with SASS is 95%–99% based on dwell time. According to survival data, ASDs secured the PICC in a range of 70% to less than 99%, depending on the duration. There is statistical evidence of a difference in the probability of reaching the EON between SASS and ASD at (p < 0.0001).
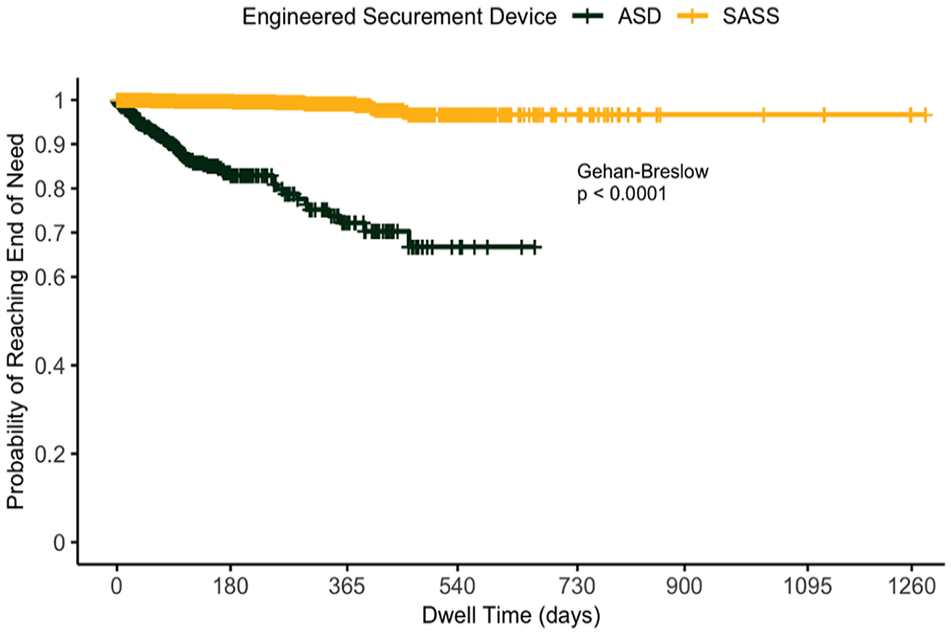
Kaplan-Meier plot of the probability of the end of need with a single PICC with an adhesive securement device (ASD) or subcutaneous anchor securement system (SASS), 2009–2020.
Discussion
In 2021 a consensus statement on SASS and venous access devices stated, “Subcutaneously anchored securement is a very promising strategy to avoid dislodgement.” 13 The results of this retrospective study seem to demonstrate that using SASS to avoid dislodgement of PICCs in oncology patients, is an appropriate strategy employ.
In a single-center prospective study by Zerla, the safety, efficacy, and cost-effectiveness of using SASS to secure long-term PICCs was assessed. The study found no episodes of dislodgement through 4963 total days and over 700 dressing changes. 14 Dressing changes with an ASD leave the PICC temporarily without securement.13,14
The highest dwell time recorded in this CCC retrospective study for ASD was 663 days. Considering this form of securement requires replacement at least every 7 days, this patient had the ASD removed and reapplied 95 times at a minimum throughout treatment. Of the recorded dwell times for SASS, the highest was 1282 day. During the 3½ years this PICC was in place, the original implanted SASS secured the PICC through more than 183 dressing changes. Additionally, no securement-related adhesive was removed and replaced, decreasing the risk of catheter dislodgement, medical adhesive-related skin injury (MARSI) and replacement costs.8,15
In a systematic review of the safety and efficacy of securement, the rate of central vascular access device partial or complete dislodgement ranged from 4.17% to 9.69% for all adhesive-based securement and 1.76% for SASS. 16 A study by McParlan, 15 described a cross-sectional comparison of ASD and SASS and reported that 6% of 1111 PICCs inserted required replacement secondary to partial or complete dislodgement if secured by ASD.
The CCC vascular access team observed the problem of patients failing to reach the end of need at a rate of 18%–41% through 2011 with ASD, see Table 2. The introduction of SASS in 2012 immediately decreased the probability of failing to reach the EON to 8%. By 2020 a patient with their PICC secured by a SASS had a 99% chance of completing the required therapy with one catheter. In addition, partial or complete dislodgement fell to less than 1% when securing the catheter with a SASS, see Table 3.
The clinician inserting the PICC often chooses securement based on what is conveniently available in the procedural kit or what they have always done. For example, in most PICC procedural trays, the available securement option is adhesive-based.17,18 Discovering issues caused by securement failure on the day of treatment will cause delays in vital testing, critically timed chemotherapy, and overall care. Securing the PICC in the optimal position is a vital clinical decision that may impact the likelihood of the patient reaching the end of need with one PICC and completing the necessary therapy. 19
Limitations
This retrospective study was conducted by analyzing over 14 years of patient data. The lack of randomization and control of groups is an inherent limit of retrospective studies. Patient information was entered into the database for tracking purposes with limited standardization of terminology. Some data were removed if the information was unclear to avoid fouling the data by speculating what information the team member meant to convey. The most consistent removal data focused on partial or complete dislodgement and EON. Additional endpoints of interest would have been CLABSI, thrombus, and skin injury. However, the entered information was vague or possibly left out if it was not the primary reason for removal.
Conclusion
Partial or complete dislodgement causing the unplanned removal of the PICC occurred at 12% for ASD and 0.4% for SASS (p < 0.0001). The probability of reaching the end of need with one PICC, regardless of the reason for premature removal, at 2 years for patients with an adhesive securement device was 68% (n = 944). For patients with a subcutaneous anchored securement device, it was over 95% (n = 8313). The difference in the probability of reaching the end of the need with one PICC between the two securement devices was calculated at (p < 0.0001).
With over 9200 patients and more than a million catheter days, the results of this retrospective study seem to demonstrate the SASS’s superiority in assisting the patient to reach the EON with a single PICC. Relying on convenient or traditional securement is not a clinically sound decision but rather a default action with potentially significant consequences for the patient.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Michelle L. Hawes: Independent research consultant, Carol A. McCormick: Staff RN, Clatterbridge Cancer Center Liverpool, Gregory E. Gilbert: Independent biostatistician.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The lead author was reimbursed for time spent on authorship and publication of this article. Gregory Gilbert was reimbursed for his statistical analysis.