
Abstract
Background:
MicroBubbles Time test (MBT), consisting in the rapid infusion of saline with addition of air microbubbles, visualized by B-mode echocardiography, represents a potential alternative to Intracavitary ECG (IC-ECG) and chest X-ray for central venous catheters (CVCs) tip location. Even if promising, this technique lacks of standardization: a clear time cut-off between bubble infusion and their detection in heart’s right chambers hasn’t been yet established. At these regard, microbubbles could be also detected as microembolic signals (MES) with an alternative ultrasound technique: the pulse wave Doppler (PW).
Objective and methods:
The first aim of this pilot study is to establish agreement of MBT with PW test (MBT-PW) compared with reference standard IC-ECG and normal MBT for tip location on CVCs. Corrected tip’s position was established through reference standard IC-ECG, afterward MBT-PW was performed, with the sample volume placed at tricuspid valve to detect MES simultaneously with micro-bubbles injection in CVCs. The second aim was to evaluate inter-observer variability for MES detection and grading.
Results:
Eight patients were enrolled; we obtained three records for each patients (24 with MBT and 24 with MBT-PW, the two techniques were acquired simultaneously). Inter-methods agreement through reference standard IC-ECG versus MBT-PW and MBT versus MBT-PW methodic was satisfying (Cohen’s kappa value = 1). MBT-PW and MBT signals were recorded within the first heart beat after microbubble infusion in all patients. Mean time delay thorough MBT-PW and MBT was 0.76 ±0.07 and 0.78 ± 0.07 s respectively; Intraclass correlation coefficient was 0.992 (95% CI: 0.981–0.996) suggesting excellent correlation. Inter-observer variability for positive MBT-PW evaluation was optimal (Cohen’s kappa value was 1), while indicated substantial agreement for MES grade evaluation (Fleiss’ Kappa value was 0.704; 95% CI: 0.328–1.000).
Conclusions:
Our study supports agreement between MBT-PW and reference standard IC-ECG for tip location. Satisfactory agreement was observed also for MBT-PW and MBT.
Keywords
Introduction
Assessment of vein flow through contrast enhanced ultrasound represents an alternative to intracavitary ECG and chest X-ray (CXR) to evaluate tip location for central venous catheters (CVCs).1–4 In particular, this test consists in the injection of agitated saline solution into the CVC and subsequent ultrasound B-mode detection of microbubbles in right heart atrium (RA): the delay between infusion and microbubbles detection is called MicroBubbles Time test (MBT) (Figure 1). A MBT lower than 2 s identifies a correct tip location. 5 Recently, the GAVeCeLT Working Group for Vascular Access in COVID-19 6 suggested the use of bedside transthoracic echocardiography (TTE) for tip location by using convex or sectorial probes, adopting the microbubbles test technique.
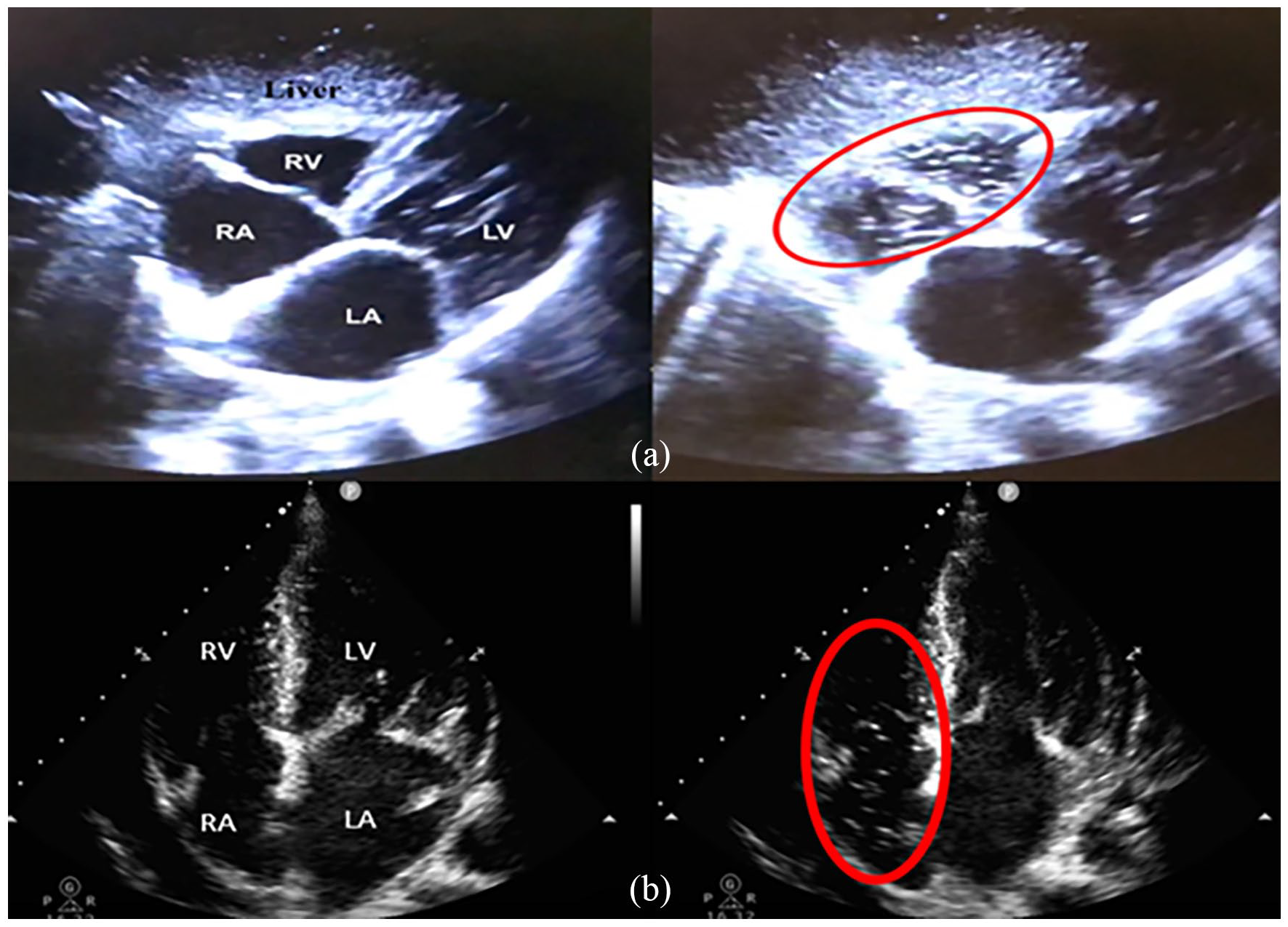
Transthoracic echography of the heart (subcostal four-chamber (a); apical four-chamber (b)) which shows the transit of microbubbles through the right chambers, after the infusion of agitated saline solution in the catheter.
When the microbubbles test is applied to central catheters, a 2 s cut-off is routinely used to confirm a correct tip location 7 (RA—superior vena cava junction). However, a recent paper evaluating peripheral midline catheters, 8 measured a MBT < 2 s in 29.4% of patients, implying that 2 s may not represent a suitable cut-off to confirm the CVC correct tip location. Such finding is in line with the studies published by Meggiolaro et al. 9 and Iacobone et al. 5 that suggest a MBT much lower than 2 s (respectively 500–1000 ms) for CVC correct location. Although sensitivity and specificity of this cut-off seems satisfactory (100%–99%), the measurement of such a small time interval requires an appropriate device. For this reason, standardization of this technique is hard and no clear time cut-off is yet established, because the probable most suitable cut-off (500 ms) is not recordable by a single human operator.
In this setting, we hypothesize to use pulse Doppler (PW) technique performed at tricuspid valve to detect the passage of microembolic signals (MES) after microbubbles injection. The MES are defined as typical, visible, high intensity signals of short duration in the Doppler spectrum. In the current clinical practice these signals are searched in the middle cerebral artery during the Transcranial Color Doppler examination after microbubbles infusion in a peripheral vein in order to diagnose right-left shunts. The detection of MES by means of PW is easier than microbubble B-mode visualization, and time delay between infusion and MES detection is objectively measurable on the PW spectrum, even after test conclusion by means of recorded frames, as previous established also in standard MBT.5–9
The first aim of this pilot study is to establish agreement of MBT with PW test (MBT-PW) compared with reference standard IC-ECG and standard MBT for tip location. Ultrasound tip location through MBT and MBT PW were performed after that the correct catheter’s position was confirmed with reference standard IC-ECG.
The second aim is to evaluate inter-observer variability of MBT-PW and MES grading.
This pilot and feasibility case series would lead to larger prospective study on MBT-PW.
Methods
In this case series we consecutively enrolled patients for whom a Peripherally Inserted Central Catheter (PICC) catheter was implanted for clinical reasons in Sacco hospital from December 23st 2020 to April 27st 2021. In those patients, tip location certified by reference standard IC-ECG was compared to MBT-PW, afterward normal MBT was compared to MBT-PW.
The study was conducted basing on the CONSORT checklist for pilot studies 10 and Practical Guide to Assess the Reproducibility of Echocardiographic Measurements. 11
The Institutional Review Board of our University Hospital (Luigi Sacco Hospital, University of Milan, Italy) approved the study protocol (BUbble test nei CAteteri Venosi ad Inserzione Periferica “BUCAVIP”; July 7, 2021). All the enrolled patients expressed and signed an informed consent.
The devices have been positioned following the protocol “Safe insertion of PICCs (SIP).” 12
PICCs (PowerPICC®, BD Franklin Lake, NJ, USA FR 4 single lumen) were the devices used.
IC-ECG with Pilot system (Vygon) was performed before MBT to verify the PICC’s tip location at the cavo-atrial junction, 13 and was used as the reference standard in sinusal rhythm as well as in atrial fibrillation according to Calabrese et al. 14 If a mid-thigh femorally inserted central catheters (FICC) was implanted, Xiao et al. 15 IC-ECG positioning technique was used to locate the catheter’s tip above the diaphragm, near the right atrium.
A “Philips CX50 CompactXtreme ultrasound system” ultrasound machine was used during the study. Subcostal view (Figure 1(a)) was considered the first choice for RA visualization, apical four-chamber view (Figure 1(b)) was used as a second option when subcostal view was not feasible. Subcostal view and apical four-chambers view were acquired according to American Society of Echocardiography (ASE) guidelines 16 ; pictures of subcostal and apical four-chamber views were included in Figure 1.
For each patient three clips were recorded both for MBT and for MBT-PW (acquired simultaneously); two different operators evaluated recorded clips of both MBT and MBT-PW in a blind modality. To obtain a uniform computation of MBT-PW across two different operators, a series of training videos produced by the principal investigator was shared in anticipation of the study beginning. The operator evaluation was double blinded (no information about the patients and the evaluation of the second physician).
A positive MBT was defined if Bubble were detected in right atrium within the first second after microbubble infusion.
A positive MBT-PW required two conditions:
(1) MES registration within the first second from the beginning of record, concomitant with injection starting, to MES visualization (first vertical spike) in the PW spectrum.
(2) At least MES 2 grade of four possible (grade 1: no microbubbles; Grade 2: 1–10 microbubbles; Grade 3: >10 microbubbles but no curtain effect; Grade 4: curtain effect, defined as shower of microbubbles that does not allow to distinguish and count them 17 ).
The time delay and the number of heart cycles from the beginning of record, concomitant with injection, to MES visualization (first vertical spike) in the PW spectrum were evaluated. Pulse Doppler wave is synchronous with cardiac flow and heart rate. Similarly, to what happens with the mitral valve, tricuspid pulse Doppler is represented by the E wave due to peak velocity blood flow from left ventricular relaxation in early diastole and the A wave due to peak velocity flow in late diastole caused by atrial contraction (Figure 2), which is absent if patient presents atrial fibrillation. In patients with atrial fibrillation E wave (due to peak velocity blood flow from left ventricular relaxation in early diastole) was used to establish heart cycle.
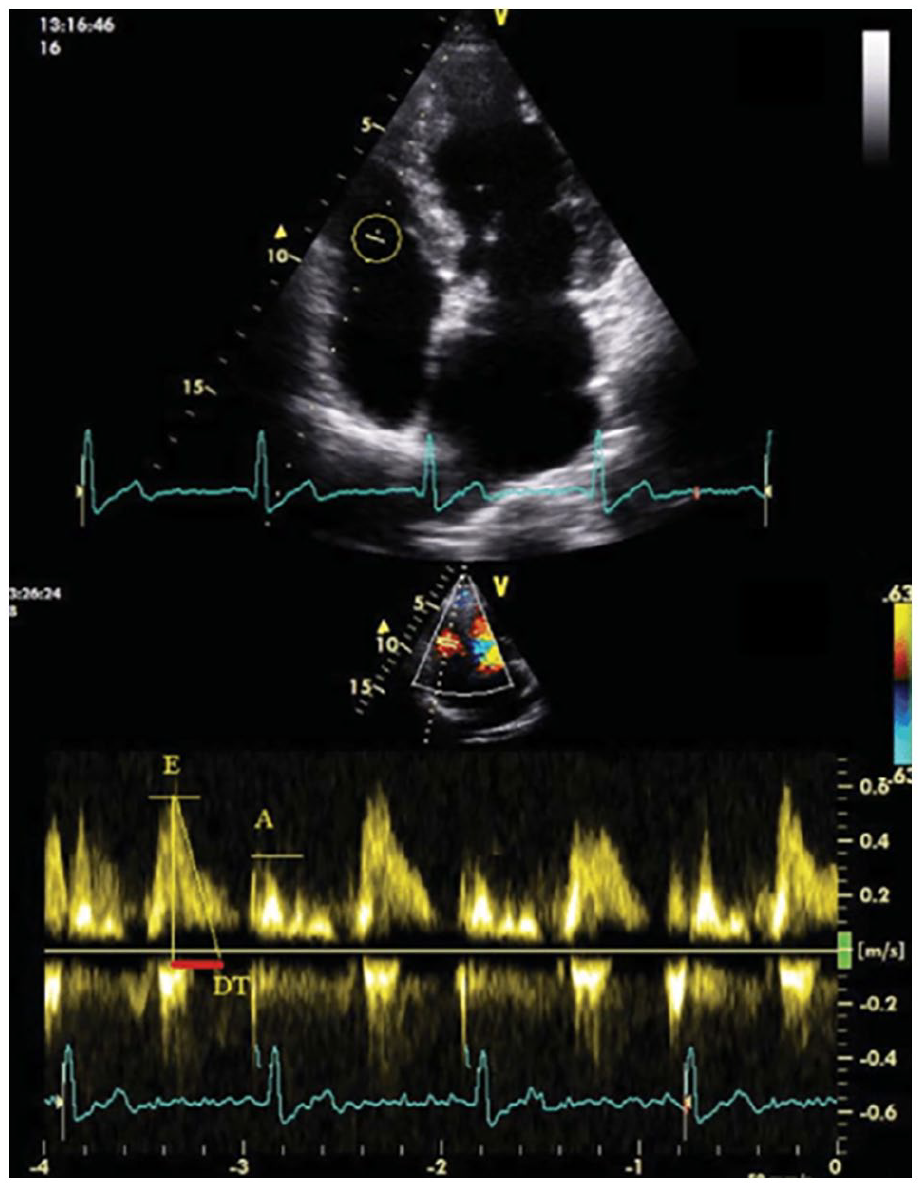
Example of tricuspid pulse Doppler in apical four-chamber: The E wave is due to peak velocity blood flow from left ventricular relaxation in early diastole; the A wave is due to peak velocity flow in late diastole caused by atrial contraction.
Technique
Exploration of the venous structures: Rapid Peripheral Vein Assessment protocol (RaPeVA), 12 Rapid Central Vein Assessment (RaCeVA) protocol, 18 and Rapid Femoral Vein Assessment (RaFeVA) protocol. 19
After administrating 1 mL of 2% lidocaine, the vessel is punctured and the guide is inserted.
Anthropometric measures are collected from the exit site to the ipsilateral clavicle–sternal articulation then adding 10 cm for the PICC inserted in the right arm and 15 cm for those inserted in the left arm (Ocado Technique) 20 ; plus 2 cm for subcutaneous anchoring device (Securacath® Interrad Medical Plymouth USA); from the puncture site to the low margin of sternum for FICC.
The catheter is cut to the anthropometric measures.
A subsequent bolus of lidocaine is deposited in the subcutaneous tissues in the area where the exit site of the catheter will be created, which will then be incised with a scalpel to facilitate the entry of the micro introducer.
The micro introducer is positioned.
The catheter is inserted into the micro-introducer and pushed until the optimal position is reached.
A reference standard technique (IC-ECG) confirms the correct tip position.
The MTB-PW is performed: First press of the pulse Doppler button activates cursor; the operator places the Doppler sample at the tips of the tricuspid valve leaflets.
With a second press the Doppler starts his registration and pop up pulse Doppler wave under 2D images in a duplex modality that allows both B-mode and PW spectrum visualization (Figure 3). Simultaneously the same operator that presses pulse Doppler, begins injection of 5 mL of a contrast agent compounded by 90% saline and 10% air, mixed with a three-way stopcock by exchange of saline/air mixture between the syringes.
The MTB-PW and MBT is repeated three times.
The micro introducer is removed.
Normal site dressing procedure: application of a subcutaneous device (Securacath® Interrad Medical Plymouth USA), using of glue (cyanoacrylate) on the exit site and covering with transparent semipermeable bordered membrane.
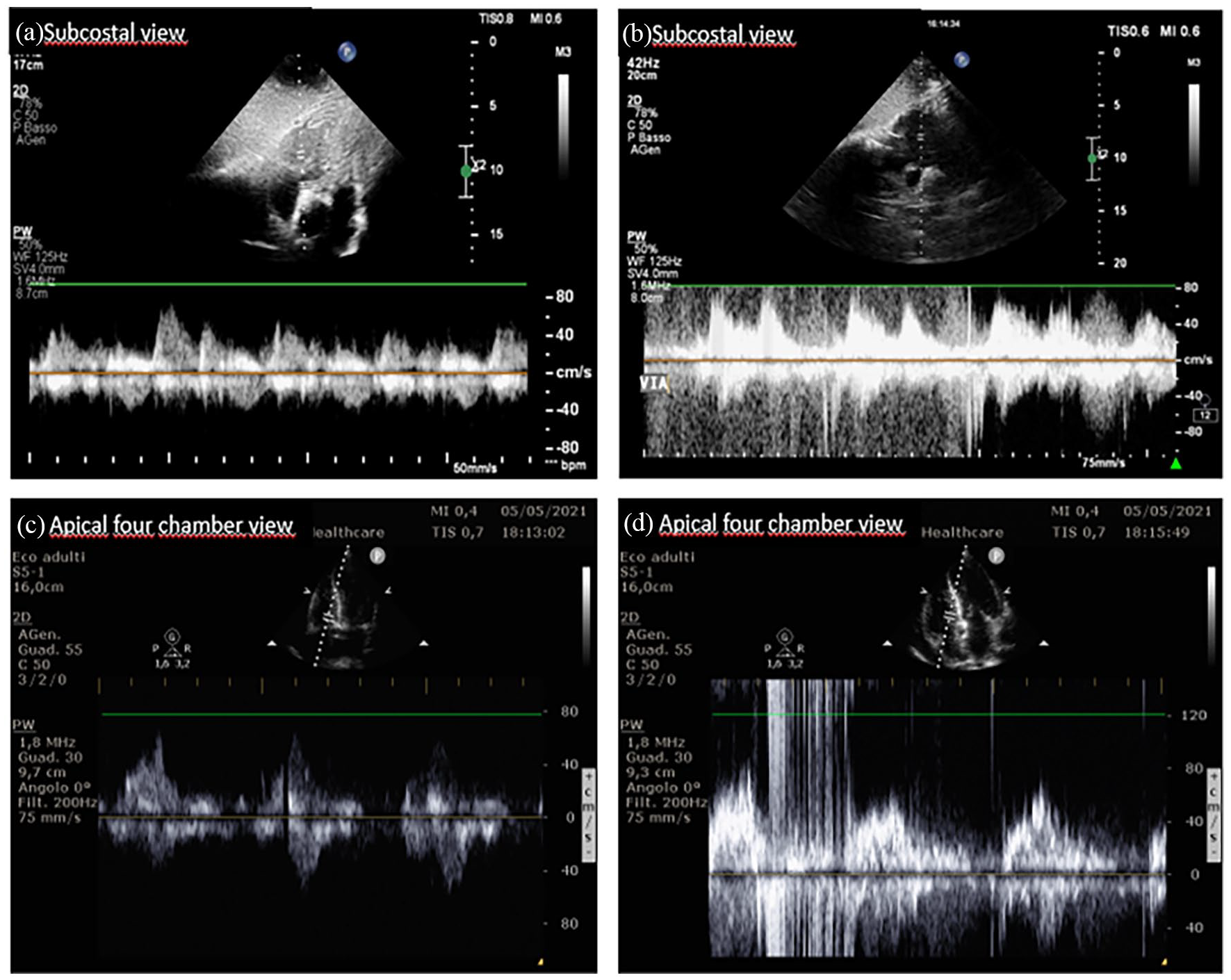
Example of MBT with pulse Doppler: (a) subcostal view; tricuspidal Pulse Doppler before microbubble injection, (b) subcostal view; tricuspidal Pulse Doppler during microbubble injection: MES appear immediately after the injection, (c) apical four chamber view; tricuspidal Pulse Doppler before microbubble injection, and (d) apical four chamber view; tricuspidal Pulse Doppler during microbubble injection: MES appear immediately after the injection.
Statistical analysis
Agreement of MBT-PW was assessed through Cohen’s kappa statistic to evaluate
(1) Inter methods agreement through reference standard IC-ECG and MBT-PW for a positive result.
(2) Inter methods agreement through MBT-PW and MBT for a positive result.
Intraclass correlation coefficient was used to compare association of measure’s time delay and number of heart cycle in MBT and MBT-PW.
Inter-observer variability was evaluated with two items:
(1) Agreement for positive MBT and MBT-PW was assessed through Cohen’s kappa statistic measures.
(2) Agreement for MES grade evaluation was assessed through Fleiss’ Kappa statistic measures.
Kolmogorov-Smirnov test was done to evaluate the normality of distribution of data. Quantitative data were expressed as mean, standard deviation, median, and interquartile range. Student-T test and Mann-Whitney test (for non-parametric data) were used for comparison of time delay between MBT and MBT-PW. p-Value less than 0.05 was considered statistically significant.
Results
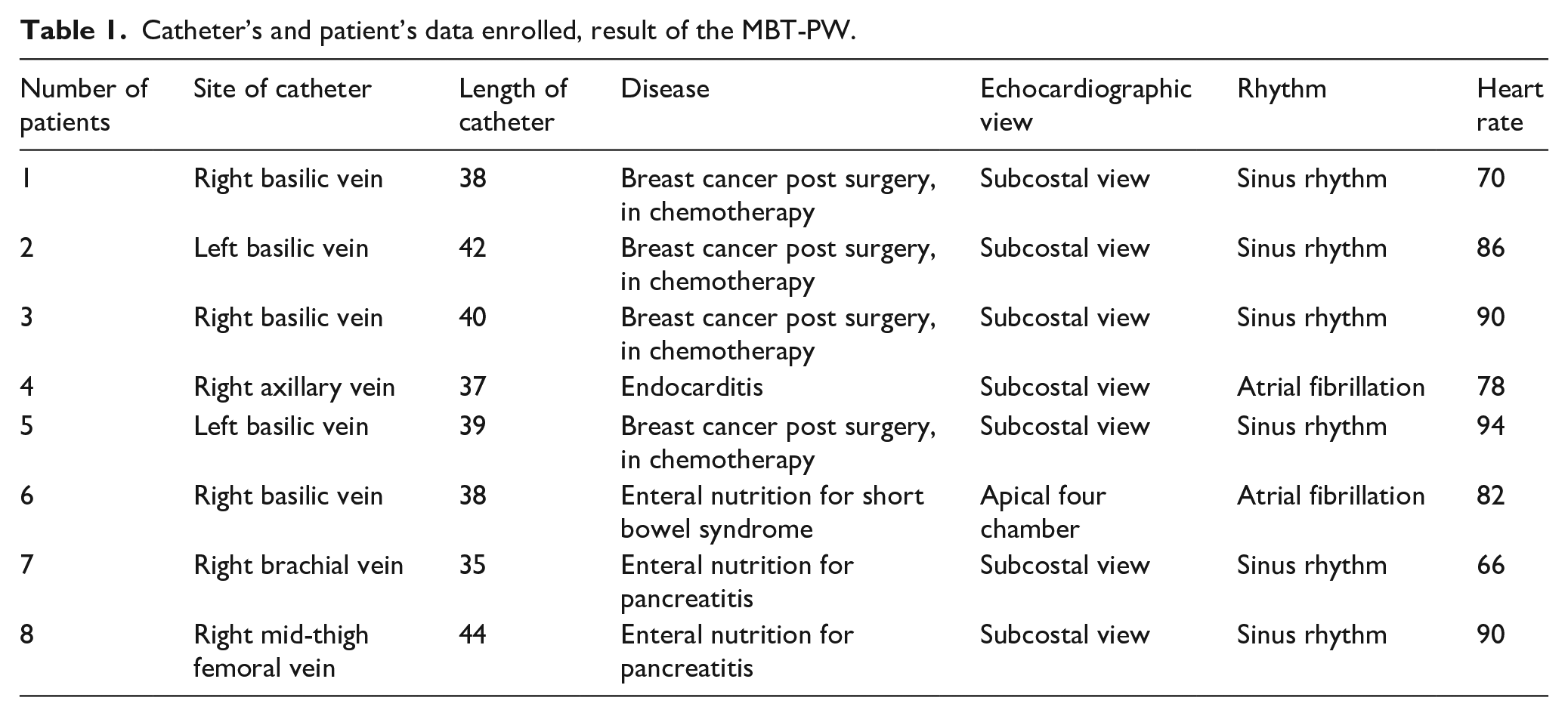
Eight patients were analyzed in this case series; MBT-PW was feasible in all patients. Six patients were in sinus rhythm, two in atrial fibrillation (Table 1). In seven patients a subcostal view was used, in one an apical four-chambers view was preferred. One patient received mid-thigh FICC while the rest received PICC.
Catheter’s and patient’s data enrolled, result of the MBT-PW.
From the eight patients enrolled, we obtained 48 videos (24 for MBT and 24 for MBT-PW). After video training education, both the Inter methods agreement through reference standard IC-ECG and MBT-PW and the two ultrasound methodic (MBT vs MBT-PW) was satisfying (Cohen’s kappa value was 1).
MBT-PW was recorded within the first heart beat after microbubble infusion in all patients, with a measured time lapse between infusion and MES detection lower than 1 s. Intraclass correlation coefficient of 1 for number of heart cycle in MBT and MBT-PW suggest excellent correlation.
Mean time delay thorough MBT-PW and MBT was 0.76 ±0.07 and 0.78 ± 0.07 s respectively; Intraclass correlation coefficient of 0.992 (95% CI 0.981–0.996) for time delay in MBT and MBT-PW suggests excellent correlation.
Inter-observer variability for positive MBT-PW evaluation was optimal (Cohen’s kappa value was 1), while for MES grade evaluation indicates substantial agreement (Fleiss’ Kappa value was 0.704; 95% CI: 0.328–1.000). MES grading for all MBT-PW clip evaluated was greater than grade 3.
Discussion
The result of our study supports adequate agreement between reference standard IC-ECG versus MBT-PW and MBT versus MBT-PW for a positive result (MES detection within the first second after infusion). Intraclass correlation coefficient suggests an excellent correlation of measure’s time delay and number of heart cycles in MBT and MBT-PW. This pilot study elucidates the interchangeability between MBT-PW and standard MBT. We hope that future larger studies will clarify if MBT-PW can perform even better than MBT thanks of his peculiar characteristics.
Literature show that the use of pulse Doppler both in transcranial color Doppler 17 and Carotid Doppler 21 Ultrasound with microbubbles injection is well established in the setting of right-left shunt detection. A right-left cardiac shunt is diagnosed with PW in the presence of ⩾1 microembolic signals (MESs) in middle cerebral artery or carotid artery after microbubbles injection. The possibility to detect only one microbubble could be useful during MBT to improve test sensibility and specificity.
Time between start of the infusion and the signal appearance in the cardiac chambers is probably better defined compared to usual MBT, because the operator can focus the attention on a single vertical line signal (MES) on the PW spectrum instead of scan the entire atrium looking for white points (the bubbles) in the B-mode.
Moreover, during MBT-PW there is not only a visual feedback of MESs, but it is also produced a typical sound due to the alteration of PW wave, that can help the operator to better perceive passage of bubbles through heart chambers.
Another vantage is that pulse Doppler wave is synchronous with cardiac flow and hearth rate. With PW technique we can replace time measurement with cardiac cycle, whose length is easy to establish (60 pulse/min = 1 s/cardiac cycle; 120 pulse/min = 0.5 s/cardiac cycle). For patients in atrial fibrillation we considered the mean frequency to estimate cardiac cycle length. In this way if the operator that injects microbubbles at the same time pushes Doppler button, we can measure cardiac pace instead of time and establish a pace cut-off instead of a time one. Moreover, time from registration starts and MES appearance is measurable on the PW spectrum. Thus, the tip may be correctly positioned if MES are recorded between the first cardiac cycle if the patient rate is 60 pulse/min or at least before the second if rate is 120 pulse/min.
As already known for MBT the concordance between two operators for a positive MBT-PW is high. Even MES evaluation indicates substantial agreement between observers. Arellano et al. 22 have underlined that the MBT is an easy technique even for novice operators and our study seems to confirm this statement also in MBT-PW.
The study presents some limitations. First it is monocentric; we hope one day the reproducibility of MBT-PW will be tested in more hospitals for both the registration and the evaluation of videos. The sample size is smaller than those suggested for pilot “feasibility” studies (at least 12 patients). In order to obtain a larger sample, we registered three MBT-PW for each patient, but this expedient reduced the heterogeneity. We can affirm that our findings have to be confirmed in a larger cohort in the future.
Our operators retain a high expertise in bedside echocardiographic exam and PICC and FICC implantation, thus the feasibility with operators with lower echocardiographic skills need to be investigated. A key point of MBT-PW is to coordinate both hands (one injects the contrast agent and one presses PW button) and this skill may not be easy to obtain.
A possible different delay in PW wave start, after PW button pressure, could be considered if different ultrasound machine were used for MBT-PW.
Conclusion
Our study supports an optimal agreement between reference standard IC-ECG versus MBT-PW and MBT versus MBT-PW for a positive result. As for the already known MBT technique, MBT-PW is applicable even in the presence of atrial fibrillation, and for both superior and inferior limbs catheters. It allows the measurement of MES delay by heart pace rather than by a timer.
These findings have to be confirmed in larger prospective studies on MBT-PW to establish specificity and sensitivity of MBT-PW and to elaborate the pace and time cut-off.
Footnotes
Data availability statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.