
Abstract
Introduction:
The hemodialysis population is aging, worldwide. In Israel, more than half of the dialysis population is older than 68 years. The policy for vascular access among this population is still a matter of debate, with several studies demonstrating conflicting results. This study compared vascular access outcomes across age groups (<65, 65–75, >75 years) in a single hemodialysis center in Israel.
Methods:
This was a retrospective, single center analysis of all vascular accesses created in adult hemodialysis patients in our institution, from January 1, 2006, through December 31, 2012. Patient characteristics, primary and secondary access failure, and complications were collected from electronic medical records. Follow-up was until death or up to 5 years.
Results:
A total of 612 vascular accesses created among maintenance hemodialysis patients were included, of which 196 were in patients >75 years, 184 in patients 65–75 years, and 232 in patients <65 years. Mean age of the >75 years group was 80.5 ± 4.3 years and 60.7% were men. Vascular access site was the most important predicator for primary access failure (odds ratio for primary failure of radiocephalic arteriovenous fistula was 3.5 (95% CI 2.1–6), whereas age did not affect the primary failure rate (odds ratio 1.5, p = 0.648). Radiocephalic fistulas were more prone to secondary failure than other vascular access sites were. Complications were slightly more common in the oldest group. Eight percent of the patients >75 years died before access was used.
Conclusions:
In our cohort, age did not affect vascular outcomes, whereas VA site seemed to be the most important parameter in primary and secondary VA failures. Our results support considering VA on an individual basis and supply valuable information regarding complication and failure rates of VA among patients >75 years.
Introduction
With the population in western countries aging, the number of people ⩾65 years old reaching End Stage Renal Disease (ESRD) is steadily rising. Between 1990 and 2010, the average age of the dialysis population in Israel increased by 10 years. 1 The prevalence of patients on dialysis ages 75–84 years, rose 4.8-fold and currently, it is the largest age group on dialysis in Israel. 2
Older dialysis patients present a unique management challenge, due to large variations in comorbidities, functional abilities, frailty and life expectancy. This causes difficulty when deciding treatment measures, such as creating vascular access (VA). Recent publications, including a meta-analysis, demonstrated a higher risk of primary and secondary AVF failure among the older population, when compared to younger patients.3,4 However, the best choice of access type and location is still a matter of debate. Misskey et al. 5 reported poorer VA outcomes related to patency and fistula maturation with increasing age, as well as better results with brachiocephalic (BC) fistula compared to radiocephalic (RC). Olasha et al. 6 and Renaud et al. 7 suggested that age should not disqualify patients for fistula creation.
Considering these controversial results, the policy for VA in elderly patients is unclear. The current study evaluated VA outcomes of patients on maintenance hemodialysis (HD) across three different age groups.
Materials and methods
This retrospective, single center study included all VA created from January 1, 2006 through December 31, 2012 in our institution, including patients referred for VA creation before initiating dialysis, as well as after dialysis onset. All patients were assessed by a vascular surgeon before surgery. Vascular ultrasound mapping was performed according to the surgeon’s recommendation. Based on the patients’ ages at the time of VA creation, the study population was divided into three age groups: less than 65 years, 65–75 years, and older than 75 years. The study included patients who had more than one VA created. VA site, primary and secondary failure rates, and relevant demographic and clinical data were recorded during 60-months of follow-up. Demographic and clinical data when the VA was created were recorded for each patient from the electronic medical records.
Results are reported according to the STROBE statement guidelines.
Study outcomes
The primary endpoints were primary and secondary failure of the VA. Primary failure was defined as permanent failure of VA before it was suitable for HD. This included non-maturation, thrombosis, and failure of first and subsequent cannulations, that prevented initiating HD through the VA.
Secondary failure was defined as permanent failure of the VA after it met dialysis suitability criteria and was subsequently abandoned. In our institution, the therapeutic strategies toward thrombosed AVF and AVG differ. Whereas, thrombosed AVG will undergo fistulography for declotting the access, AVF do not. All other maintenance measures (routine pressure measurements and Doppler studies) are the same.
Secondary endpoints were all-cause mortality, post-operative complications, assisted maturation, and complications related to creating VA (including arterial steal syndrome and post-operative infections). Post-operative infections were recorded if they resulted in VA removal.
Ethical considerations
The study was approved by the Institutional Ethics Committee, in keeping with the principles of the Declaration of Helsinki. In accordance with Ministry of Health regulations, the Institutional Ethics Committee did not require written informed consent because data were collected anonymously from the electronic medical records without active patient participation.
Statistical analysis
Data are expressed as mean ± standard deviation (SD) for continuous variables and as numbers and percentage for non-metric parameters. Metric data were checked for normality with the Shapiro-Wilk test. As some of the variables were not normally distributed, t-test and Mann-Whitney nonparametric tests were used to compare the three groups for the different variables. ANOVA was used to compare continuous variables among the three groups. Chi-squared or Fisher’s Exact test was used to compare categorical parameters. Univariate and multivariate logistic regression models were applied to estimate predictors of primary and secondary failures. Survival curves of VA (“time to secondary failure”) were obtained using the Kaplan-Meier method and compared using two-sided log rank statistics. A p < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS Version 27 (IBM Corporation, Armonk, NY, USA).
Results
The study cohort consisted of 612 patients, including 196 (32%) who were older than 75 (mean age 80.5 ± 4.3) years at the time of VA creation; 60.7% were men. Clinical and demographic characteristics of the study population according to age groups are summarized in Table 1. The most common causes for ESRD were diabetic nephropathy and hypertensive renal disease. More than half of the hemodialysis patients in each age group had diabetes.
Baseline characteristics of the study population by age group.
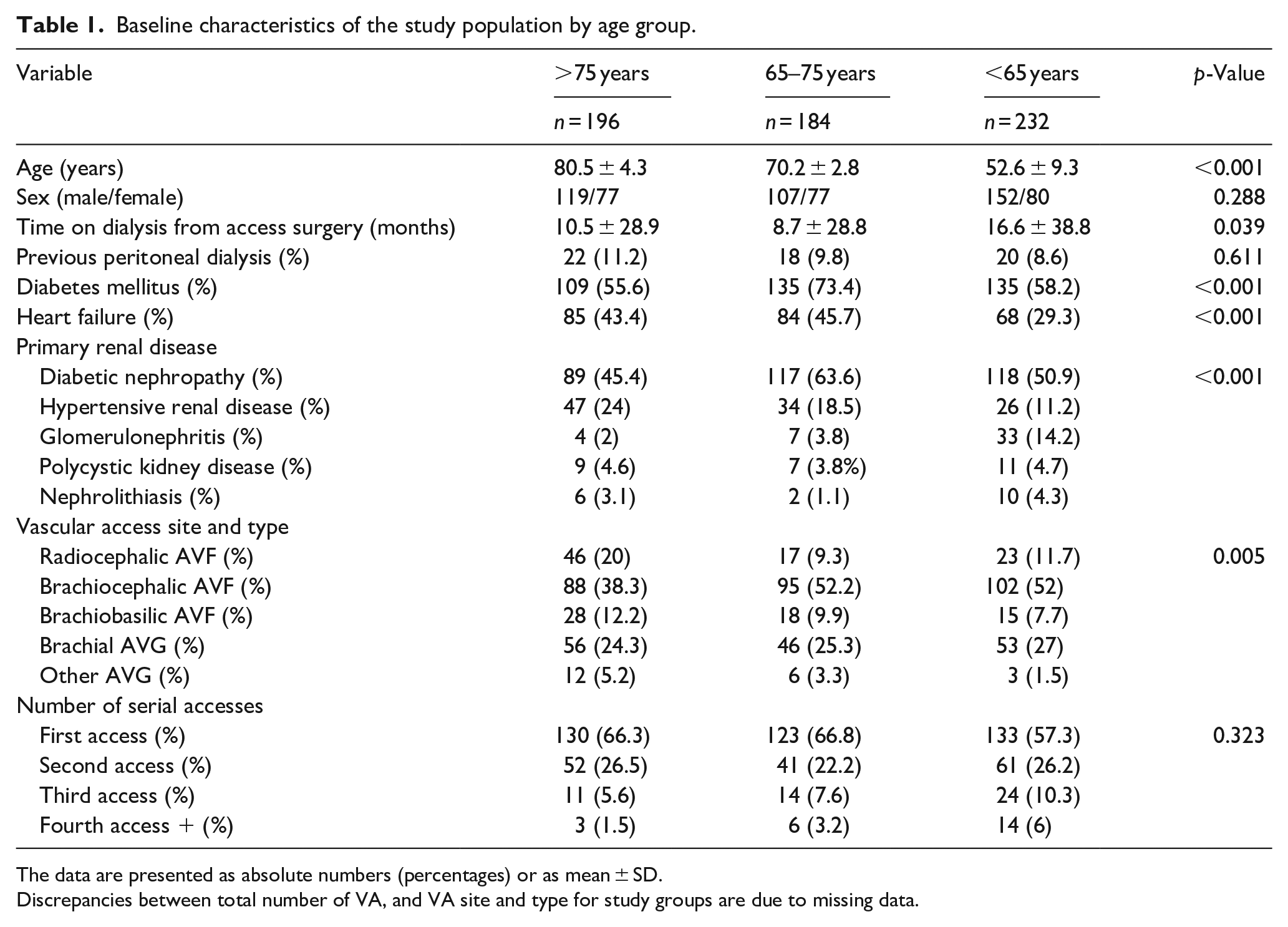
The data are presented as absolute numbers (percentages) or as mean ± SD.
Discrepancies between total number of VA, and VA site and type for study groups are due to missing data.
Most of the VA were created after dialysis initiation: 147/232 (63%) in patients <65 years, 108/184 (59%) in 65–75 years, and 111/196 (57%) in those >75 years; p = 0.556).
Among the >75 years group, 71.4% (140/196) of VA were AVF and 27% (53/196) were brachial AVG (Table 1). A RC fistula was created more often in the youngest group compared to patients ⩾65 years (p = 0.005). No other significant difference was found in VA location in the three age groups. No significant difference in the number of previous accesses created in the age groups was found.
Vascular ultrasound mapping was performed in only 36.4% of the study cohort (223 patients). Access type and site, as well as number of previous vascular access procedures, were significantly different between patients who underwent mapping, compared with patients who did not (data not shown). Based on this observation, we could not assess the effect of pre-operative vascular mapping on our results.
Primary failure
Primary failure was defined as an access that could not be used for hemodialysis. Among 196 accesses created in the group >75 years, 29 (14.8%) were not suitable for HD, as compared to 28/232 (12.1%) in the group <65 years. Odds ratio (OR) for primary failure in patients >75 years was 1.5 (0.85–2.76), p = 0.648.
The overall incidence of primary failure in the entire study cohort was 30.2% in RC AVF vs. 10.9% in all other VA (p < 0.001). OR for primary failure in RC AVF was 3.5 (95% CI 2.1–6). The prevalence of primary failure of RC fistula across age groups was: <65, 12/46 (26%); 65–75, 6/17 (35%); >75 8/23 (35%), p = 0.668. In all three age groups, RC AVF was a significant predictor of primary failure. Multivariate analysis of primary failure demonstrated age, congestive heart failure, diabetes mellitus, and anti-platelet therapy were not predictive of primary failure. However, female sex, as well as VA site had a significant effect on primary failure (Table 2).
Multivariate analysis of predictors of primary failure.
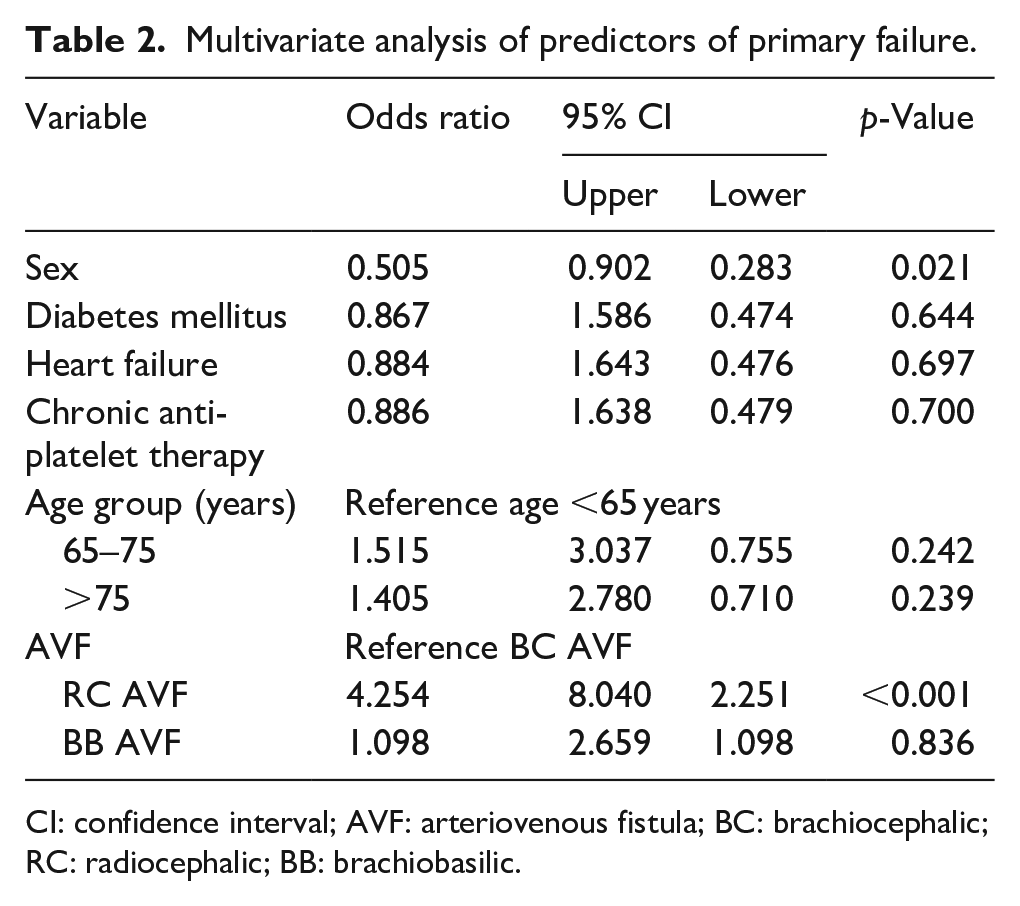
CI: confidence interval; AVF: arteriovenous fistula; BC: brachiocephalic; RC: radiocephalic; BB: brachiobasilic.
Among 612 VA, 61 (10%) required angiographic intervention (“assisted maturation”) before they were suitable for HD. There was no significant difference in the incidence of assisted maturation between the oldest and youngest groups (21/196 vs 22/232, p = 0.673). There was no significant difference in time from VA creation to first intervention among age groups: 12.5 ± 12.8 months among those <65 years, 15 ± 16 in 65–74 years, and 11.3 ± 14.7 in >75 years old (p = 0.143).
Secondary failure
Secondary failure was defined as permanent failure of the VA after it met dialysis suitability criteria, but was subsequently abandoned. Patients with primary failure were excluded from this analysis. Fewer patients in the oldest group, 23.5% (46/196) had secondary failure compared with 34.5% (80/232) in the youngest group (p = 0.015). The mean interval to secondary failure (22.9 ± 17 vs 23.9 ± 20 months) in the oldest compared to the youngest groups was not significantly different (p = 0.765).
Time to secondary failure between AVF and AVG was not significantly different (p = 0.539; Table 3). Although the oldest patients with RC fistula had a relatively high primary failure rate (35%), the survival of RC AVF was similar to that of the younger groups, with mean of 18.8 ± 5.7 months in patients >75 years versus 23.4 ± 4.2 months in the youngest group (p = 0.401). The intervals to secondary failure of the most frequent VA in our study, RC AVF, BC AVF, and Brachial AVG across the three age groups are shown in Figure 1(a)–(c).
Time (months) to secondary failure according to access type.
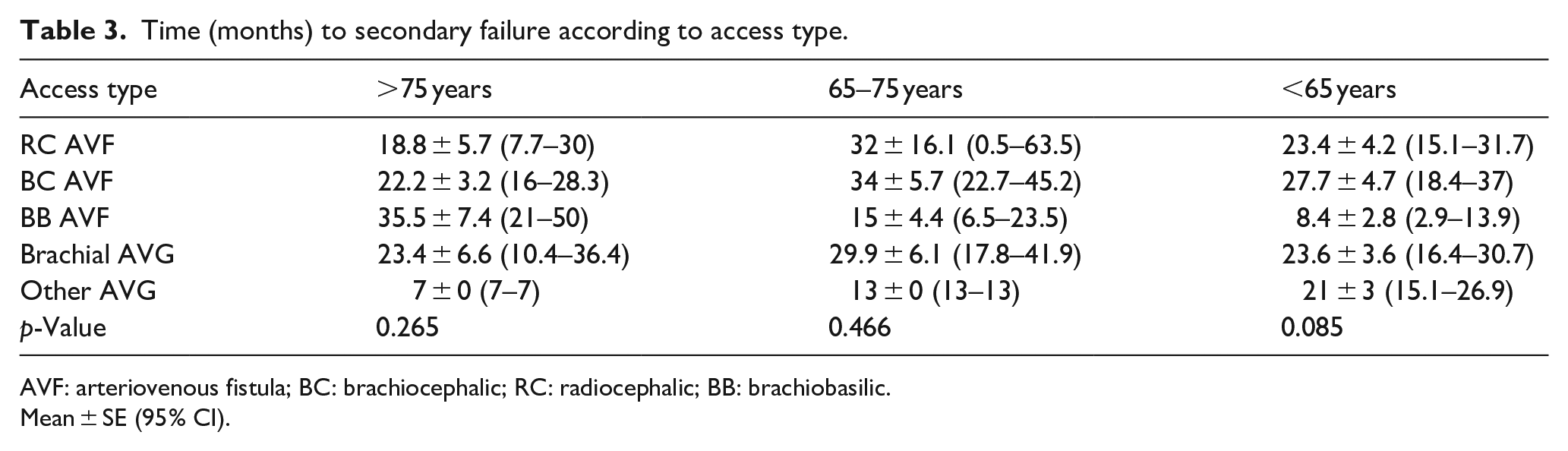
AVF: arteriovenous fistula; BC: brachiocephalic; RC: radiocephalic; BB: brachiobasilic.
Mean ± SE (95% CI).
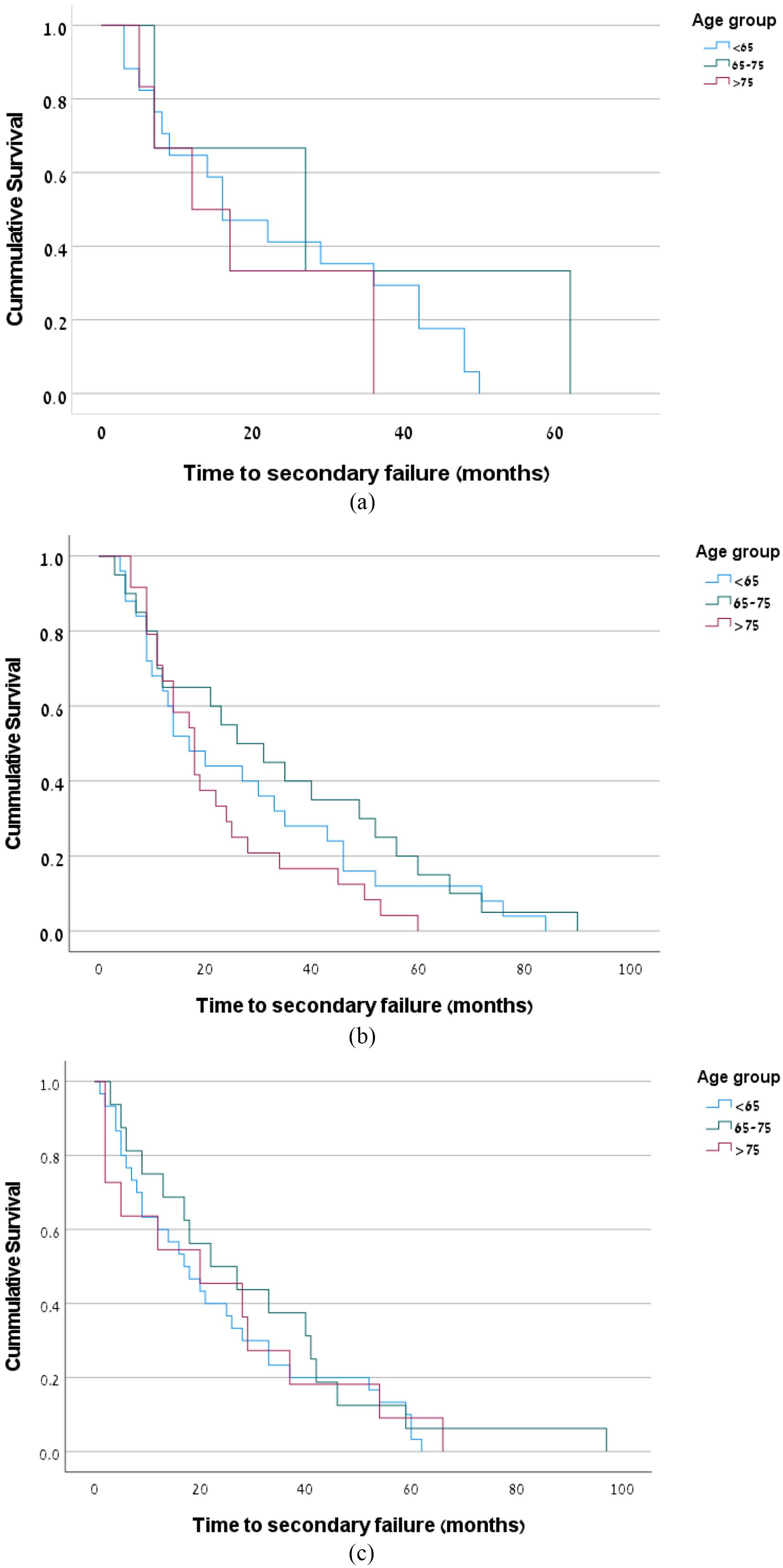
Time to secondary failure: (a) time to secondary failure in RC AVF across the three age groups (p = 0.401), (b) time to secondary failure in BC AVF across the three age groups (p = 0.191), and (c) time to secondary failure in brachial AVG across the three age groups (p = 0.727).
Post-operative complications
Steal syndrome requiring access closure occurred in 13 VA (6.6%) created in the oldest group, as compared to 8 VA in each of the other two groups (4.3% and 3.4%, respectively; p = 0.290) (OR 1.106, 95% CI 0.5–2.6, p = 0.814). Among the oldest group, steal syndrome was seeing in 11 AVF compared to only 2 in AVG (p = 0.312).
Severe post-operative infections that led to VA removal were relatively low in all age groups: 3 (1.5%), 7 (3.8%), and 12 (5.2%) in >75, 65–75, and <65 years, respectively (p = 0.129). The risk of infection was higher in AVG versus AVF in all age groups, OR = 5.8 with 95% CI 1.95–17.3, p < 0.001 in the entire study population and OR = 1.1 with 95% CI 1–1.13, p = 0.05 in the oldest group. Multivariate analysis of all severe infections resulting in VA closure showed that VA type (AVG vs AVF) was the most important predictor (p = 0.001, OR = 6,and 95% CI 2–18.1).
Mortality
Mean survival from VA surgery to death among the oldest patients was 30.6 ± 25.4 months, compared to 49.2 ± 32.5 in the youngest group, (p < 0.01). Overall, 32 of 612 VA (5.2%) were not used due to patient’s death before suitable VA was achieved. Distribution across age groups differed significantly: 16/196 (8.1%) in >75 years group, 12/184 (6.5%) in 65–75 years, and 4/232 (1.7%) in <65 years (p = 0.008). The OR for death before use was 5.1 (95% CI 1.7–15.4, p = 0.002) in older patients compared to the youngest group. Most of these patients were already on chronic HD when the VA was created (p = 0.022).
Discussion
The current study evaluated the outcomes of 612 VA created in a single institution across three different age groups. The study found no age effect related to primary and secondary failures, or to assisted maturation and complications. Mean duration of access usage was almost 2 years in the oldest group (>75 years), and only 8% of these patients died with an unused VA.
Over the last two decades, since the establishment of a “fistula first” policy, there is growing evidence that fistula maturation and patency may be compromised in older dialysis patients.4,5,8–10 However, studies that assessed the effect of age on VA outcomes had conflicting results. Lok et al. 11 who assessed first VA outcome in pre-dialysis patients younger and older than 65 years found no effect of age group. Similar findings were reported in two studies that focused on patients older than 80 years, which reported similar outcomes in younger patients.6,7 The recently updated KDOQI guidelines for vascular access suggest using a “tailored approach” for VA creation according to age, co-morbidities and patient’s preference. However, the guideline did not provide a clear recommendation for VA preference according to age group. 12 This vast amount of conflicting information poses a major challenge when deciding which VA to create among older patients.
Our study cohort was heterogenous, with more than 50% of patients on HD for an average of 10 months at the time of VA creation. It is well-known that the mortality rate in the HD population peaks in the first 2–3 months of treatment, especially in the oldest population, and slowly declines over 4–12 months, to levels similar to those seen in the first month. 13 The nature of our study population, as well as the study design, which censored mortality before VA creation led to selection bias that favored superior outcomes of VA among the older group. Mean survival after surgery among the oldest patients was 30 months, with only 8% mortality before VA was used. A study that assessed VA outcomes among HD patients ⩾70 years reported significantly higher mortality rates. The average time from surgery to death was 13 months, with up to 50% mortality within 18 months, and 65% of patients died with an unused VA. 9 These findings are significantly different from ours and might suggest fundamental differences between the two cohorts. Our findings strengthen the idea that creating VA within the first year of dialysis therapy is an acceptable option and could lead to favorable results. Ko et al. 14 assessed mortality among incident hemodialysis patients ⩾80 years had found no difference in mortality rates between patients who started dialysis with AVF/AVG, as compared with those who started with CVC, which was switched to AVF within the first year of treatment. However, patients who started with CVC but were switched to AVG or stayed with CVC had poorer survival. 14
The current study demonstrated the superior outcomes with BC fistula patency, as compared to RC fistula in all age groups, including the older population. This finding is consistent with previous studies5,8,9 that reported superiority of BC AVF over RC AVF for primary and secondary patency.
This study had several limitations; First, it was retrospective, with a heterogeneous population of incident and prevalent HD patients. Second, we did not have mortality data for patients who did not undergo VA surgery. Third, there was a mixture of primary, as well as repeated, created VA. Finally, vascular mapping was done in a small proportion of patients with significant differences related to access type and site, across all age groups. Therefore, the ability to draw conclusions regarding its effect on VA outcome could not be determined.
In conclusion, our results suggest that patient age did not affect primary or secondary VA failure, but it resulted in a non-significant increase in complication risks. This study adds to previous reports that underscored that creation of VA in older patients would not necessarily yield inferior results.
Footnotes
Acknowledgements
We thank Dr. Simone Fajer and Dr. Alli Shnacker from the Department of Vascular Surgery, Meir Medical Center, for performing the surgeries including in this analysis, Dr. Naomi Nacasch, head of the hemodialysis units, Meir Medical Center, who permitted data collection and Faye Schreiber, MS for editing the manuscript. She is an employee of Meir Medical Center.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.