
Abstract
Background:
Increasing options for vascular access have increased the need for more effective communication to optimize patient engagement and ensure effective consent. An advanced prototype of the mobile application (VA App) was developed over 3 years as a patient decision aid. For the first time, entry to the 2021 UK Kidney Week was opened to all professions and patients and was held online. The VA App was presented in an inter-active session. This report summarizes the findings.
Methods:
A 30-min interactive session was allocated with the session delivered in four sections: (1) demographic data was collected; (2) an overall opinion was obtained about current patient information sources and satisfaction with these; (3) the participants were asked a series of eight questions regarding the main problem areas previously identified; (4) following a 6-min demonstration video, the participants were then re-asked the same questions to determine if the VA App would improve/worsen these areas.
Results:
Completed data from 30 participants showed great variation in all demographics. The most cited source was verbal and rated the best, whilst all other sources were felt to be poor by 90%. All eight aspects of current information sources rated poorly. There was a unanimous agreement that the VA App could make this better. Interestingly, when the eight aspects were ranked by order of the worst to best, this matched the order of the benefits of the VA App.
Discussion:
This is the first report of an on-line, multi-professional co-design workshop. With a unanimous view that current systems are very limited and that better patient information systems are required, the VA App was found to be a potential solution as a patient decision aid. Interestingly, paper leaflets were widely viewed as the least used and the least effective mechanism for communicating information to patients. Funding for a commercially produced mobile application has been secured and will be further tested in the near future.
Introduction
Until relatively recently, few options for vascular access for haemodialysis meant that little patient choice was required. An AVF (arteriovenous fistula) was considered the optimal access, but high rates of tunnelled central venous catheters (TCVC) use persist. Partly this may be due to high rates of AVF that fail to mature with a default of TCVC if dialysis was needed in the interim period. 1
The last decade has led to significant changes in the provision of vascular access with the development of early-cannulation arteriovenous grafts (ecAVG) that can be used immediately thus avoiding the need for TCVC. 2 A single randomized trial showed that these were effective in reducing TCVC use, TCVC complications, overall costs and improvement in quality of life. 3 Thus, for the first time, there have been three options for vascular access: AVF, TCVC and ecAVG. This may change in the future as other approaches such as percutaneous AVF may also have differing requirements and outcomes to traditional open surgery. Each of these has very differing implications for ease and success of creation, short and long-term maintenance requirements, and local and systemic complications. As such, there is a greater need for patient involvement in the decisions regarding vascular access selection.
Optimizing patient engagement is recognized as a key element when planning treatment. To achieve this, effective communication between patients and healthcare workers is crucial – especially where there is a requirement to assimilate and process complex data on options and alternatives, the differing outcomes, and the associated risks of each. There is now recognition that both patient factors and initial choices have a significant impact on long-term experiences and outcomes. 4 Furthermore, with changes to the UK laws on consent, effective communication is a now legally and ethically mandated as a fundamental component of healthcare delivery.
Traditionally patient information has relied on paper leaflets given to patients at the time of clinical consultations. However several limitations may make this ineffective: (1) the information cannot be easily tailored to an individual patient’s situation, understanding or needs, (2) it relies on patients having the ability to read, process and interpret this information effectively, often at a time of significant illness and multi-morbidity, (3) as the patient situation changes, a fixed information method cannot adapt to the changing circumstances and (4) this information is written from a medical perspective and based on objective measures – a view that may not necessarily mirror the lived patient experience.
It has been a long-standing aim that more effective information could be achieved using digital methods with patient decision aides, particularly in the ability to tailor to widely differing needs and capabilities in assimilating complex information. A Cochrane review found that patients exposed to decision aids demonstrated greater knowledge, were better informed, and had a greater role in decision making and more accurate risk perceptions. 5 However, there is also recognition that digital applications should be designed and implemented in a way that avoids exceeding the capacity of those less digitally able. 6 Applications that are useful, useable and desirable for patients have the potential to reduce the burden of care and improve patient capacity. Although there is now considerable literature on the methodology of this process, there are few applications that have been proven to improve outcomes. 7 A prototype of a patient decision aid – a vascular access patient mobile application has been developed over 3 years with medical experts across varied fields, allied health care professionals and patients. Based on previous cycles of design and reflective workshops, a single prototype patient mobile application was developed (VA App). The UK Kidney Week allowed a unique opportunity to present this work in an online session to a multidisciplinary audience with a background in kidney disease, including feedback from patients.
The aim of this report is to summarize the findings of this multi-national, multi-profession interactive workshop on current patient information systems and the impact of the VA App to change the situation.
Methods
The VA App has been in development for a few years and undergone refinement following multi-disciplinary stakeholder feedback including surgeons, nephrologists, health informatics, nephrologists, interventional radiologists, nurses and patients. The development and progress of the VA App has been conducted within the guidelines for such PDAs and reports have been guided by the SUNDAE checklist. 7
The UK Kidney Week is the largest event for nephrology in the UK, devoted to all topics and research in all fields of nephrology. For the first time, entry to the 2021 UKKW was opened to professions other than nephrology and patients. In addition, it was held online allowing for widely varying inter-active sessions easily accessible to a broader audience. Registration was free for patients or through renal unit registration, thus minimizing the costs for attending. This allowed a unique opportunity to present and obtain feedback on a scale that would be impossible with traditional work-shop dynamics. A 30-minute online webinar session was allocated to the presentation of the VA App.
Audience recruitment: Ensuring a diverse audience was felt critical to an effective session. Several advertising strategies were employed. Firstly, direct contacts were approached through email ‘keep-the-date’ fliers 2and 3 days before the session to 150 potential participants. Secondly, social media was used to disseminate the session with Twitter feeds of organizers and UK renal charities and regional patient groups.
Session Design: An interactive session with real-time polling and feedback was run by a surgeon, a PhD student in mobile health and health informatics, and a lecturer in digital health. The first two presented the session to reduce aural fatigue whilst the third managed Zoom tasks such as launching polls, collating chat messages and formatting results from polls into presentable formats.
Initial overview: The session was delivered in four sections: firstly, demographic data was collected; secondly, an overall opinion was obtained about the types of patient information sources and satisfaction with these through the Zoom polling features; thirdly, the participants were asked a series of eight questions regarding the main problem areas with patient information systems identified from a literature review 8 (Table 1). A 6-min video demonstrating some of the features of the VA App was then shown, following which the participants were then re-asked the same questions following the demonstration to determine if in these specific areas the VA App would make it better or worse. Finally, the participants were asked if an app like that demonstrated would be useful.
Questions and the aspect each question is designed to test.
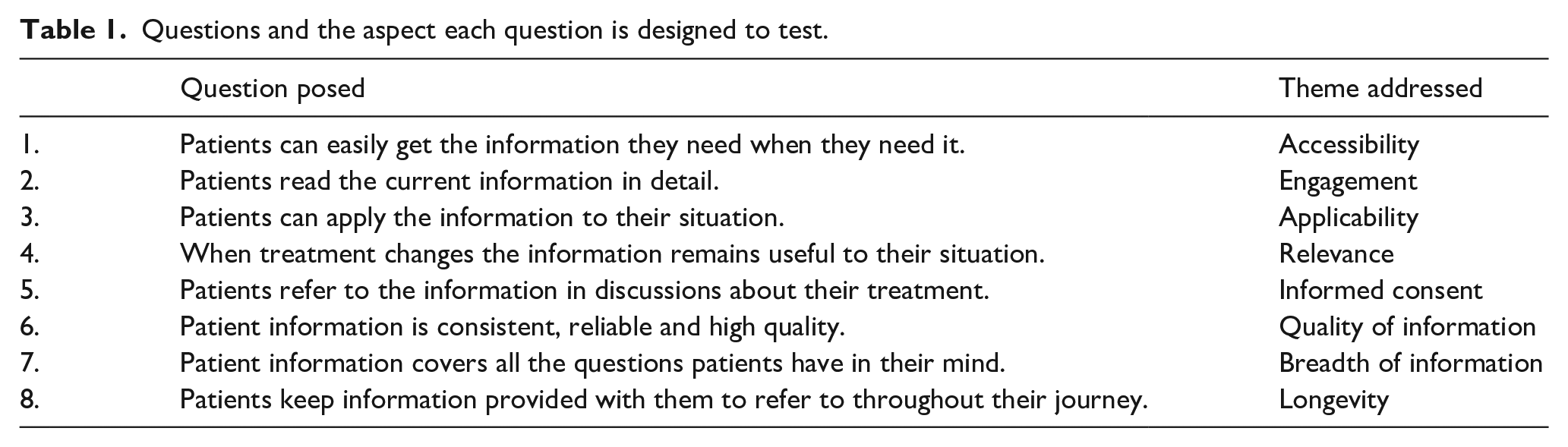
A 5-point Likert response scale was used to grade the strength of feeling to statements made (strongly agree-2; agree-1; neutral-0; disagree- −1; strongly disagree- −2).
The workshops were conducted under University of Strathclyde ethical approval.
Results
The 30 participants who completed the demographics poll showed great variation in all aspects: nephrology was the leading specialty represented (n = 14), (surgical n = 4, nursing n = 3, patients n = 2, other roles represented n = 7). The age distribution showed a predominance of ages between 31 and 50 (n = 20, 68%), with eight being older and one younger; 19 were male and 11 were female.
Sources of information + Need for new sources
‘Verbal’ was the most cited source (90%) and felt to be the best (14, 48%). All other sources were felt to be poor with less than 25% rating them satisfactory even though they were widely used: the internet was used in 80%, other patients in 75%, with paper leaflets the least used in 60%. Other than verbal, all these other sources were not highly regarded and less than 20% felt satisfactory. Only 10% ‘agreed’ and none ‘strongly agreed’ with the statement ‘current sources are satisfactory, and no other information source is needed’, with a majority (65%) either disagreeing or strongly disagreeing.
Response to initial poll on current information systems.
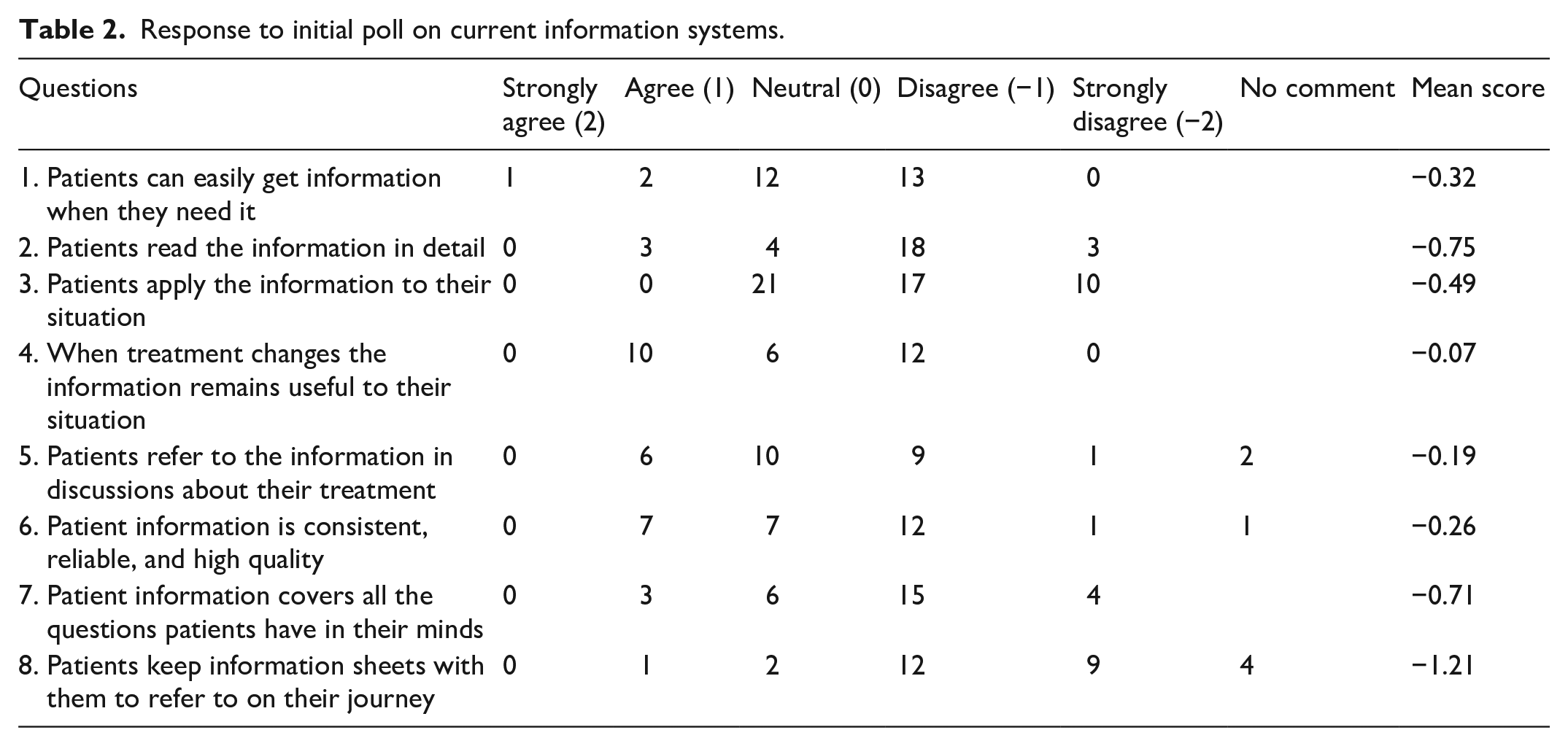
Poll Results on Current Patient Information Systems And Impact Of the Prototype – VA App.
Poll Results on Current Patient Information Systems And Impact Of the Prototype – VA App.
Response to poll on the impact of a prototype patient app.
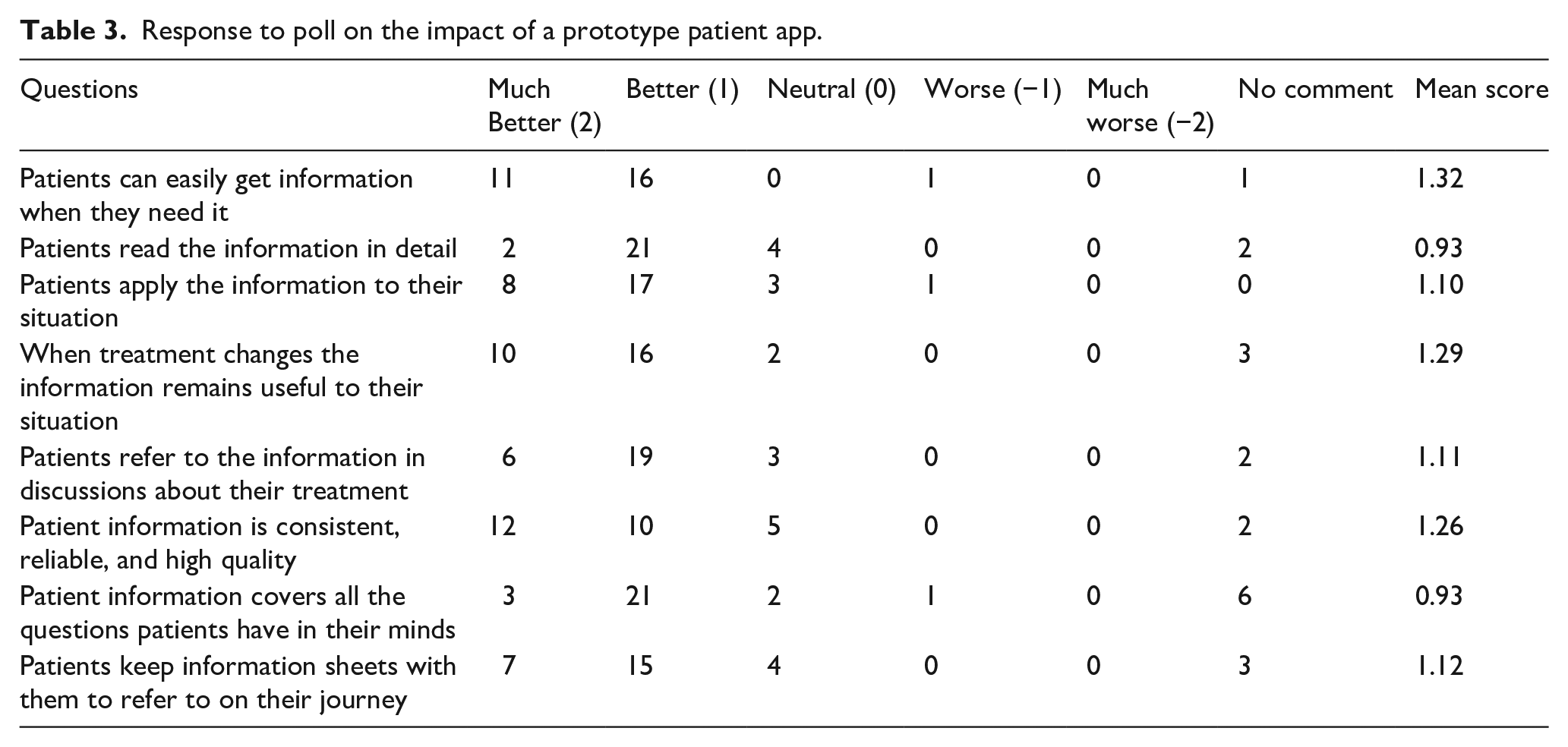
Overall, all participants agreed or strongly agreed (45% and 55%, respectively). that the VA App demonstrated would be useful.
Discussion
This is the first report of an on-line, multi-professional co-design workshop, with not only interesting data on the potential for a Patient App for vascular access (VA App) but also important practical steps for running such a process. With a unanimous view that current systems are very limited and that better patient information systems are required, the VA App was found to be a potential solution. Interestingly, paper leaflets were widely viewed as the least used and the least effective mechanism for communicating information to patients.
The online co-design workshop occurred as a function of the Covid pandemic, but the success of this establishes this format as a good method for the future. The removal of the limitations of physical space allowed a greater number of participants with a greater diversity of backgrounds. However, this may have been matched by the selection bias in requiring notification of the event through digital media, the technical ability to navigate the online platform and willingness to submit responses which may have felt less personal. Data thus obtained must therefore be further balanced and compared to a similar approach performed through traditional in person techniques when permitted.
This demonstration was the third iteration of the VA App and was based on five smaller online workshops conducted previously that were focussed on differing specialties involved in vascular access. Despite this previous experience, the technical aspects of the platform chosen required IT manipulation whilst the presentation was in progress to enable real-time voting and amalgamated responses. Several technical aspects are worth highlighting: asking participants to mute their microphones if this cannot be controlled by the moderator; to allow refinement of the voting systems the facilitator must be both host and owner of the call as some Zoom commands are restricted to a host from a different institution; ensuring one organizer is tasked with allowing room entry prevents unwanted distractions whilst presenting; ensuring that the polls were very tightly organized to draw out specific responses to considered questions; and finally ensuring that there is efficient advertising of the mechanism of attendance with codes and sites easily made accessible. A policy on use of data from partial participation should be considered in advance as participants will inevitably join and leave during the study, and even ethical approval repeated mid-way. It was unfortunate that coinciding with this session were parallel patient sessions that may have reduced the number of potential patient participants.
Overall, there was universal support for the need for improved patient data sources in keeping with many other studies. The VA App demonstrated was universally seen as a worthwhile potential solution. This information is essential in justifying investment and time to potential funders. Several design features of the app gained support: the ability to tailor information to access types; the translation of numerical probabilities to pictorial representations; the ability to input patient views and then refine the reviewer features desired; illustration was seen as important with pictures and videos. Interestingly the patient pathway – a pictorial representation of the practicalities of the forthcoming access journey was seen as confusing, perhaps partly due to the speed of presentation from time constraints that prohibited effective demonstration of this feature. As this was a key design feature previously identified as being the most difficult to effectively communicate with patients, it would be essential to determine if this criticism was presentation related or due to the feature itself.
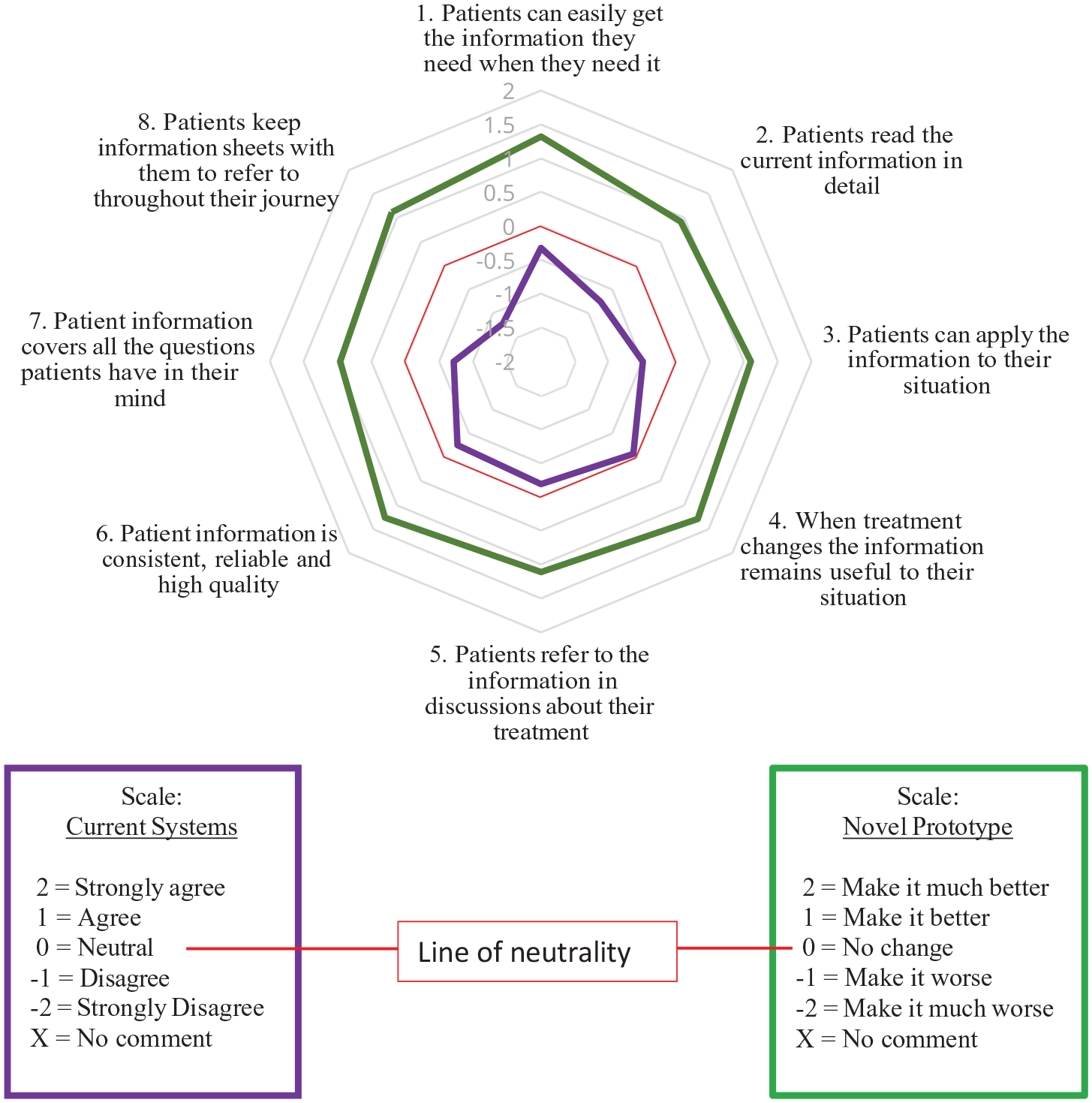
Perhaps the most interesting aspect of the data is the order or rating of the limitations of current information systems based on the scoring, which were almost completely mapped by the ranking of the benefits of the VA App demonstrated – the top seven limitations were mapped to the top six of the benefits of the VA App. This is very strong evidence that the solution derived is meeting the limitations of the current information systems correctly.
Whilst the initial impression of the VA App was supportive, it must be balanced that for impact on patient outcomes, there must be engagement of professionals looking after patients and ongoing interaction. This could only be determined by further trials. In addition, the breadth of information required by diverse groups and depth with differing capacity means that testing and further iterations will be required to take account of these factors. Funding for a commercially produced functional App has been sourced and will be available in the next months. This will allow patient group-specific workshops with variation in age, CKD stage, comorbidity and digital capacity to enable further refinement and ensure that the individual features achieve the aim of improving mutual communication and engagement between patients and health care professionals.
Footnotes
Acknowledgements
The authors would like to acknowledge the work of the Vascular Access Coordinators at the Glasgow Renal and Transplant Unit.
Author contributions
All authors designed the study; DBK, MD and RM analysed the data; D.B.K. drafted the paper; all authors revised the paper; all authors approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D.B.K., K.S.S., RK and P.C.T. have received honoraria for speaking from W.L. Gore & Associates. D.B.K. and P.C.T. have received an investigator research grant from Proteon Therapeutics. D.B.K. has received an investigator-led small research grant from W.L. Gore & Associates.
Ethical Approval
Study registered with Strathclyde University
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Investigator-led small research grant – WL Gore Ltd