
Abstract
Background:
We have previously reported that the rapid atrial swirl sign (RASS) is an accurate and safe procedure for ultrasound (US)-guided tip positioning of retrograde-tunneled hemodialysis catheters (HDCs). However, application of RASS for placement of antegrade HDCs has not been investigated yet. Therefore, we here report our first experience of applying RASS for US-guided tip positioning of antegrade-tunneled HDCs.
Methods:
We performed a cross-sectional study to assess the feasibility of applying the RASS for US-guided tip positioning of antegrade-tunneled HDCs. We included a total number of 15 antegrade-tunneled HDC insertions in 13 patients requiring placement of a HDC for the temporary or permanent treatment of ESKD in a single-center, cross-sectional pilot study.
Results:
The overall success rate of applying the RASS for US-guided tip positioning of antegrade-tunneled HDCs was 15/15 (100%) confirmed by portable anterior-posterior chest radiography, with no major adverse events after HDC insertions. In addition, this insertion technique demonstrated optimal HDC flow without any observed malfunction.
Conclusion:
This study investigated the efficacy of the RASS for US-guided tip positioning of antegrade-tunneled HDCs in patients with ESKD. Application of the RASS for US-guided tip positioning is an accurate and safe procedure for proper placement of antegrade-tunneled HDCs.
Keywords
Introduction
Chronic kidney disease (CKD) is a common medical problem in patients worldwide with an estimated global prevalence of 9.1%. 1 The prevalence of patients with end-stage kidney disease (ESKD) requiring kidney replacement therapy (KRT) is estimated to be increasing and affecting about 5.4 million people worldwide by the year 2030. 2 Tunneled hemodialysis catheters (HDCs) are preferred in patients requiring KRT for more than 2 weeks or those who develop ESKD based on a lower risk for infectious complications compared to non-tunneled HDCs. 3 Traditionally, this technique requires the use of fluoroscopic guidance to ensure correct placement and positioning of the tunneled HDC in the right atrium (RA). 3 Alternatively, the agitated bubble-enhanced visualization commonly prepared as a mixture of 9 mL of normal saline solution and 1 mL of air and has been shown to be a safe procedure for antegrade-tunneled HDC insertion without fluoroscopy. 4 However, rare events of ischemic cerebrovascular complications in patients with cardiac or intrapulmonary shunts have been reported and attributed to air bubbles.5,6 Previously, we reported that the rapid atrial swirl sign (RASS) is an accurate and safe procedure for ultrasound (US)-guided tip positioning of retrograde-tunneled HDCs by a flush injection of saline immediately after catheter positioning. 7 We here report our first experience of applying the RASS for US-guided tip positioning of antegrade-tunneled HDCs.
Materials and methods
Study population and setting
We performed a retrospective cross-sectional study to assess the feasibility of applying the RASS for US-guided tip positioning of antegrade-tunneled HDCs. We included a convenience sample of 15 antegrade-tunneled HDC insertions in 13 patients from June 2021 to January 2022 who required placement of a tunneled HDC for the temporary or permanent treatment of ESKD admitted to our Department of Nephrology and Rheumatology at the University Medical Center Göttingen, Germany (protocol number 3/6/21). Informed written consent was obtained from all subjects involved in the study for use of routinely collected data for research purposes as part of their regular medical care in the contract of the University Medical Center Göttingen, Germany.
Catheter placement procedure and material
For the placement of the antegrade-tunneled HDC, Palindrome™ Precision Symmetric Tip Dialysis Catheters (Medtronic, Minneapolis, Minnesota, USA) were used. We used 14.5 french (F)-sized HDCs that were 23 or 28 cm in length from tip to cuff, depending on the patient’s height and on the site of insertion (right or left). After obtaining informed consent by the patient, the procedure was performed by two interventionists with continuous hemodynamic monitoring in a dedicated area of our ICU to ensure maximum sterility and patient safety. The right internal jugular vein (IJV) was the preferred access site. After sterile preparation and draping, local anesthesia with 2% mepivacaine hydrochloride was applied and the IJV puncture was performed under US guidance (GE Venue US machine, General Electric Company, Boston, Massachusetts, USA) using a sterile probe cover with an out-of-plane approach. After venous cannulation, a guide wire was inserted for venous dilation and the HDC was inserted through the peel-apart introducer sheath. After tip positioning using RASS and exit site definition, the HDC was removed, and an exit site incision was performed. The HDC was tunneled from the exit site to the venotomy site under local anesthesia and inserted after peeling away the introducer sheath.
Ultrasound visualization and RASS
After placement of the antegrade-tunneled HDC, focused B-mode echocardiography using the subcostal (SC) view was used to visualize the right atrium (RA), and right ventricle (RV). Echocardiography was performed using a sector probe of a GE Venue US machine (General Electric Company, Boston, Massachusetts, USA). Immediately after HDC placement, a flush consisting of 10 mL of normal saline was injected into one of the catheter hubs by one of the interventionists, while echocardiography was performed by a third operator skilled in echographic examinations, but not directly involved in the procedure. The exam was recorded in a short video sequence on the hard disk of the US machine for later review and documentation. The appearance of the saline swirl entering the RA within 1 s of the start of the saline flush was interpreted as being indicative that the HDC tip was close to, or within, the target zone. Both onset and appearance of the turbulence were subjectively rated at the bedside. Immediate appearance of the RASS within 1 s was judged as correct placement, as previously reported.7,8
Post procedural assessment
After placement and final positioning of the antegrade-tunneled HDC, conventional anterior chest radiography was performed to document correct placement of the catheter tip and to exclude procedure-related complications. The patients were monitored for 2 h following the procedure and transferred back to the ward for observation of potential complications for at least 24 h. Post-insertion HDC performance including dialysis parameters were assessed at first treatment performed the same or next day.
Patient consent and ethics approval
The study included patients aged >18 years of age who had an indication for HDC insertion. All patients provided written informed consent for all procedures presented in this paper, which are considered standard at our center. The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of University Medical Center Göttingen (protocol number 3/6/21, approval date 25 June 2021).
Statistical analysis
Descriptive statistics with frequencies and percentages were used for the characterization of the study cohort. No prespecified hypotheses were defined due to the exploratory nature of this study. Data analyses were performed with GraphPad Prism (version 9.3.0 for MacOS, GraphPad Software, San Diego, California, USA).
Results
Clinical parameters including demographic data and etiology of ESKD in the total cohort are shown in Table 1. We included a total number of 15 antegrade-tunneled, 14.5 F-sized HDC insertions in 13 patients (two HDCs had to be replaced after the first insertion due to HDC dislocation, Figure 1). 7/15 (46.7%) of antegrade-tunneled HDC insertions were performed through the right internal jugular vein (IJV); 9/15 (60%) HDCs had a length of 23 cm (Figure 1). After placement of the antegrade-tunneled HDC, focused echocardiography to visualize the RA and RV (Figure 2(a)), RASS was performed as described previously (Figure 2(b)). 7 If the RASS appeared immediately, HDC tip positioning was considered to be adequate. If RASS visualization was delayed by more than 1 s, the HDC was inadequately positioned and repositioned. Thereafter, the HDC positioning was deemed to be in an adequate position if the tip was visualized within the RA with reconfirmed immediate RASS visualization in the apical 4C view. RASS was positive in 15/15 (100%) inserted antegrade-tunneled HDCs, the overall success rate of applying the RASS for US-guided tip positioning of antegrade-tunneled HDCs was 15/15 (100%). Proper HDC placements were confirmed by portable anterior-posterior chest radiography tip position in the RA in 10/15 (66.7%) or cavoatrial junction in 5/15 (33.3%, Table 2). After HDC insertion, there was only post-procedural bleeding in 1/15 (6.7%) HDC insertions requiring sandbag placement over the catheter insertion site and one unit of red cell transfusion. After HDC insertion, we monitored dialysis parameters at first treatment performed the same or next day without any observed malfunction, a median blood flow of 250 mL/min, median dialysate flow of 500 mL/min, a median transmembrane pressure (TMP) of 30 mmHg and median venous pressure of 70 mmHg with no differences between HDC tip position in the RA or cavoatrial junction (Table 3). In summary, we here present the feasibility and safety of applying the RASS for US-guided tip positioning of antegrade-tunneled HDCs with optimal HDC flow without any observed malfunction.
Clinical parameters in the total cohort of 13 patients.
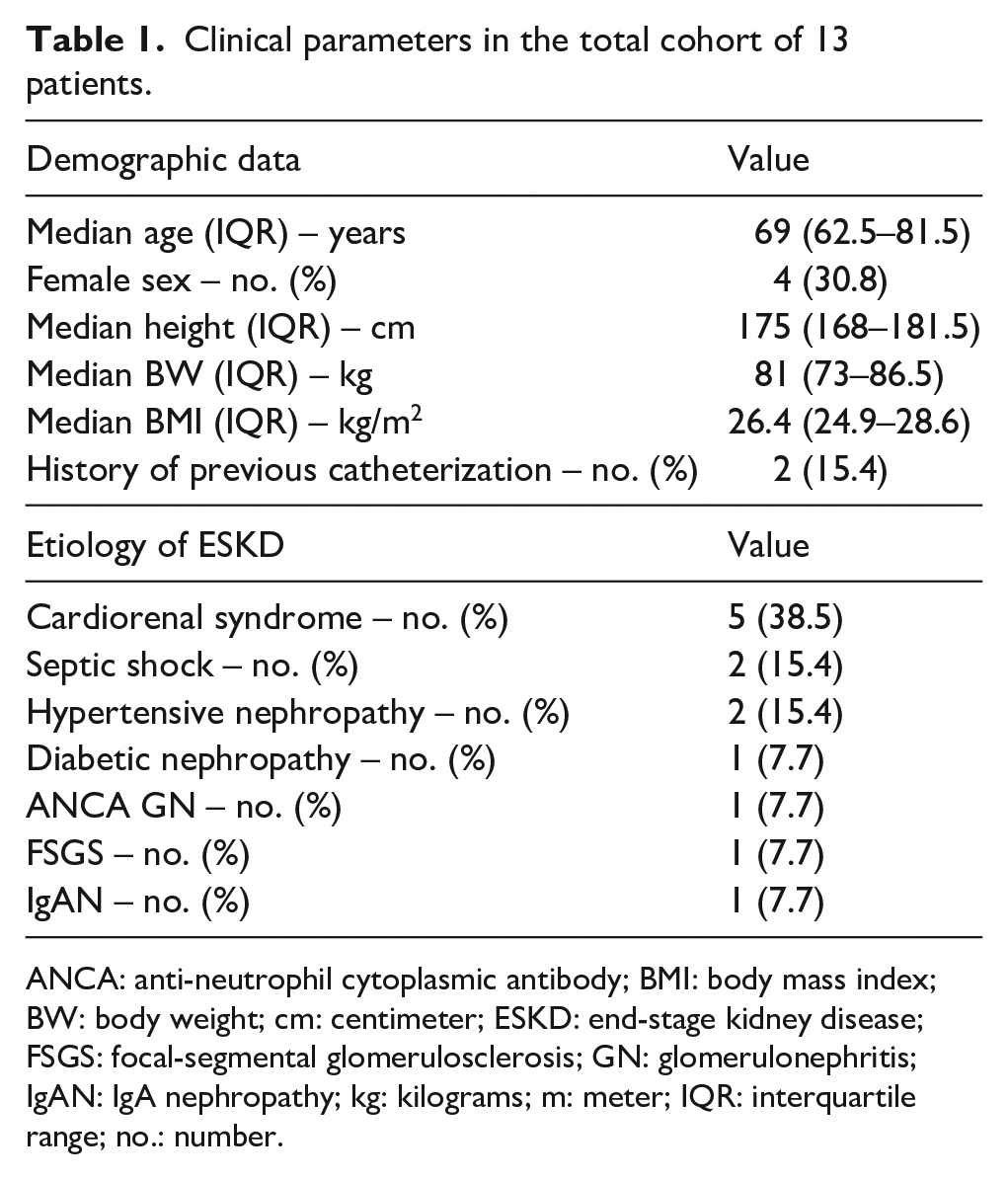
ANCA: anti-neutrophil cytoplasmic antibody; BMI: body mass index; BW: body weight; cm: centimeter; ESKD: end-stage kidney disease; FSGS: focal-segmental glomerulosclerosis; GN: glomerulonephritis; IgAN: IgA nephropathy; kg: kilograms; m: meter; IQR: interquartile range; no.: number.
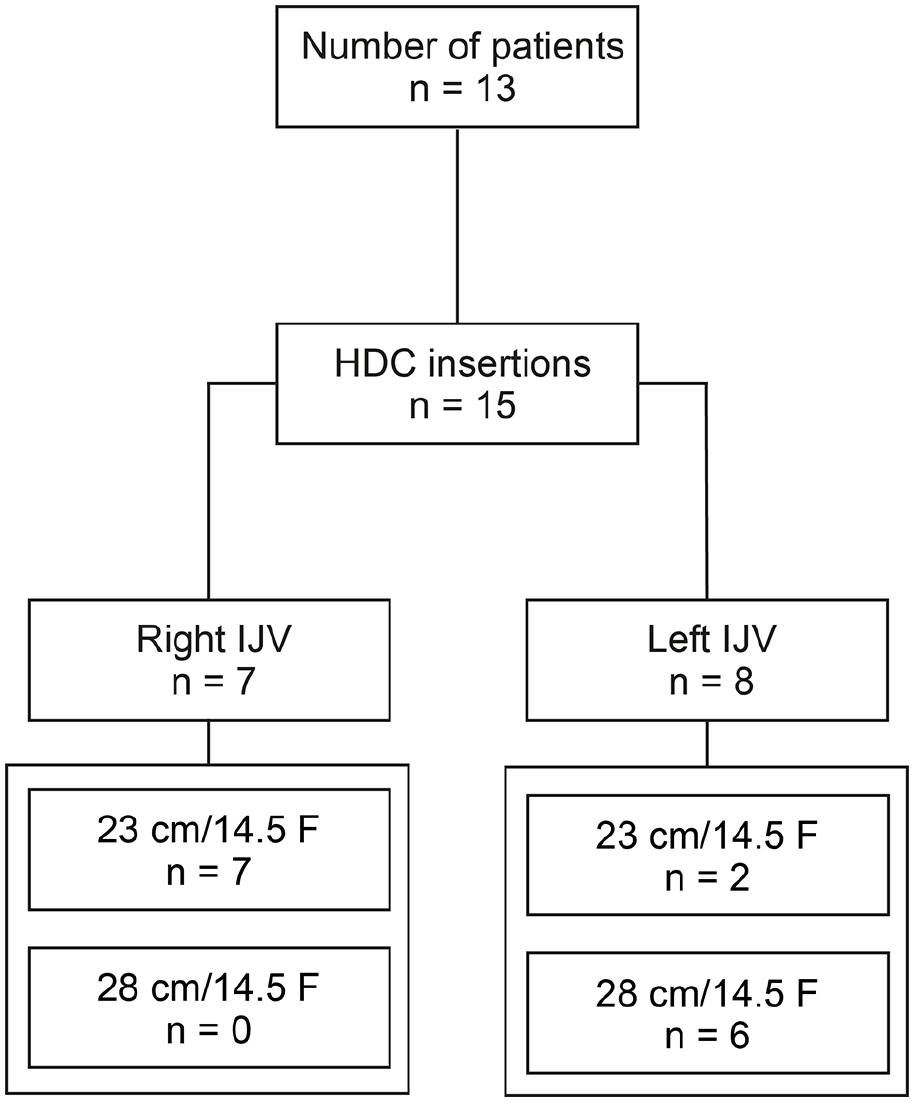
Total patient cohort. STROBE flow chart of patient disposition with indication of antegrade-tunneled HDC insertion.
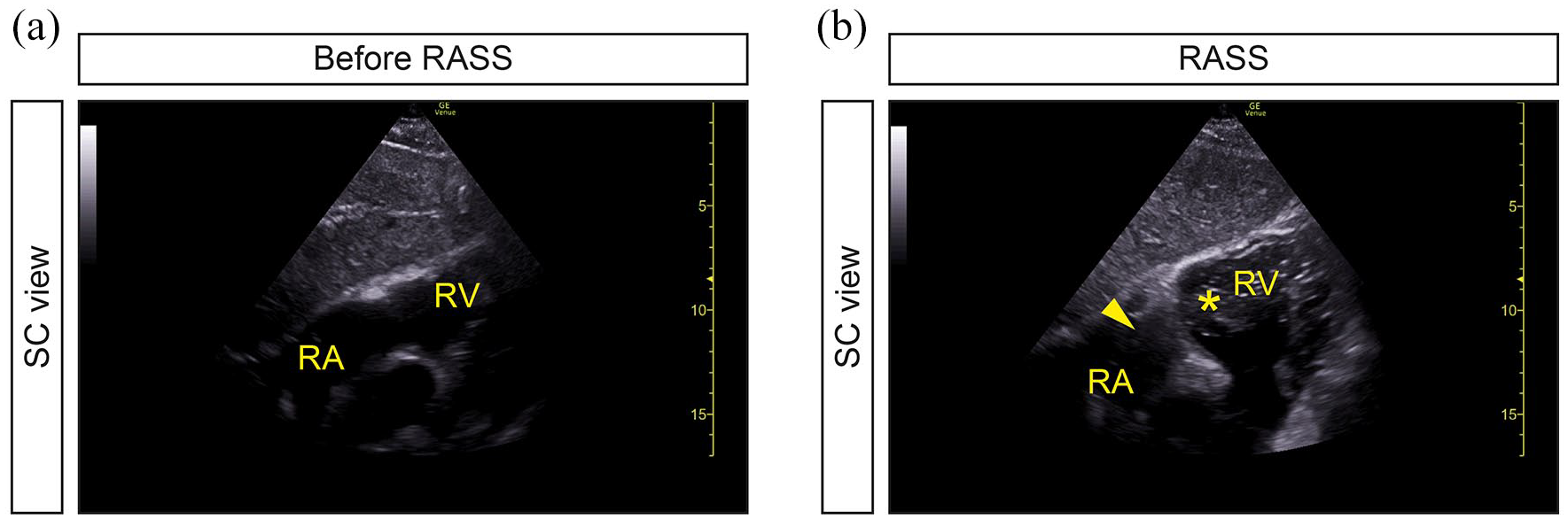
Application of the RASS for US-guided tip positioning of retrograde-tunneled HDCs: (a and b) After placement of the retrograde-tunneled HDC, focused echocardiography using a SC view to visualize the RA and RASS was performed. If the RASS appeared immediately within 1 s in the RA (arrowhead) and RV (asterisk), HDC tip positioning was considered to be adequate.
Position of antegrade-tunneled HDCs assessed by portable anterior-posterior chest radiography.

Abbreviations: no., number; HDC, hemodialysis catheter; RA, right atrium; RASS, rapid atrial swirl sign.
Antegrade-tunneled HDC performance data.
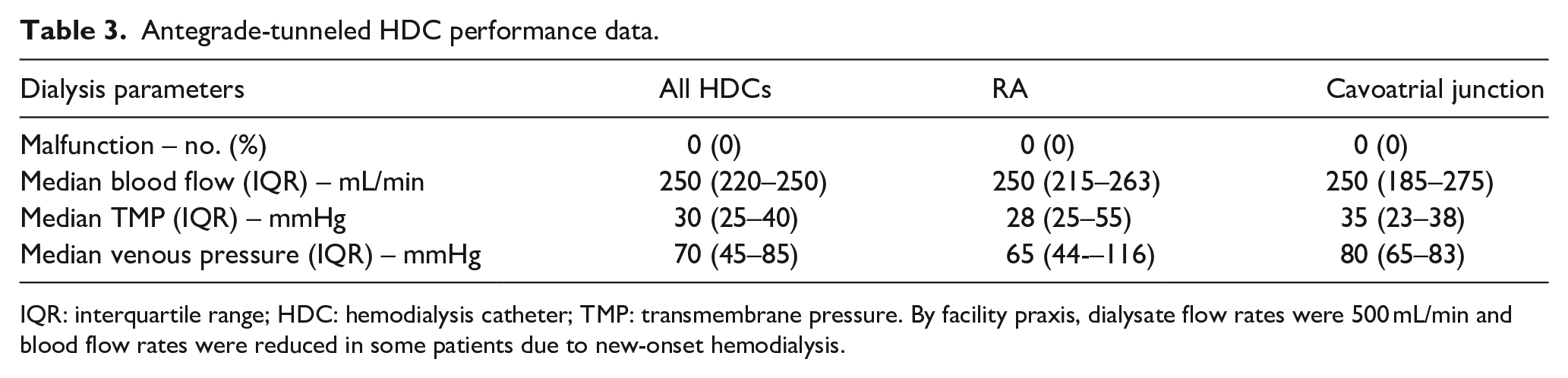
IQR: interquartile range; HDC: hemodialysis catheter; TMP: transmembrane pressure. By facility praxis, dialysate flow rates were 500 mL/min and blood flow rates were reduced in some patients due to new-onset hemodialysis.
Discussion
This cross-sectional study performed in patients requiring HDC insertion due to ESKD investigated the efficacy of the RASS for US-guided tip positioning of antegrade-tunneled HDCs. We found that the application of the RASS for US-guided tip positioning was accurate in identifying proper placement of antegrade-tunneled HDCs. Multiple studies already described the safety of US-guided tip positioning of CVCs without fluoroscopy.9,10 The advantage of US-guided tip positioning is that it provides a dynamic procedure for catheter guidance and direct visual and functional assessment of tip location. In addition, real-time fluoroscopy services are not always immediately available. In addition, real-time fluoroscopy imposes additional safety risks to patients and operators due to radiation exposure. 11 The US-guided insertion of CVCs was further improved by using different methods of flush injection and visualization of the RA, shown to be equally safe but faster and inexpensive.4,8,9 The agitated bubble-enhanced visualization has previously been shown to be a safe procedure for antegrade-tunneled HDC insertion. 4 The agitated bubble-enhanced visualization is commonly prepared as a mixture of 9 mL of normal saline solution and 1 mL of air. 4 However, rare events of ischemic cerebrovascular complications in patients with cardiac or intrapulmonary shunts have been reported and attributed to air bubbles.5,6 Previously, we reported that the RASS is an accurate and safe procedure for US-guided tip positioning of retrograde-tunneled HDCs by an opacification of the RA after flush injection of saline immediately after catheter positioning. 7 Therefore, application of the RASS without the use of air is potentially safer regarding rare side effects. 8 Here, we expand application of the RASS for US-guided tip positioning of antegrade-tunneled HDCs and show that the overall success rate was 100%, without major adverse events. In addition, we here show that this insertion technique allows optimal post-procedural HDC flow without any observed malfunction.
Despite these observations, our study has several limitations. First, this is a cross-sectional study from a single center with a limited number of antegrade-tunneled HDC insertions. Second, all HDCs were inserted through the internal jugular veins and application to different access sites (e.g. external jugular veins, subclavian veins) remains elusive. Third, our study did not intend to directly compare application of the RASS with the alternative use of fluoroscopy. Finally, this technique may have limitations in obese patients due to improper visualization of the RASS. Nevertheless, this is the first study to investigate the efficacy of the RASS for US-guided tip positioning of antegrade-tunneled HDCs as a feasible, safe and easy procedure without need for bedside fluoroscopy. Therefore, our observations require further corroboration in additional studies from other centers to define the specific benefits and risks of exclusively US-guided procedures and application of the RASS for antegrade-tunneled HDC tip positioning.
Conclusions
This study investigated the efficacy of the RASS for US-guided tip positioning of antegrade-tunneled HDCs in patients with ESKD. In line with our previous findings in retrograde-tunneled HDCs, we herein describe that the application of the RASS for US-guided tip positioning is equally accurate and safe for proper placement of antegrade-tunneled HDCs.
Footnotes
Acknowledgements
We acknowledge support by the Open Access Publication Funds of the Göttingen University, Germany.
Author contributions
BT conceived the study, collected and analyzed data, created the figures and wrote the first draft. MP, TK and BT performed surgical procedures. DT collected and analyzed data and co-wrote the manuscript. MP and TK edited the manuscript.
Data availability statement
Deidentified data are available on reasonable request from the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research is supported by georg-august-universität göttingen.
Institutional review board statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of the University Medical Center Göttingen (protocol number 3/6/21).
Informed consent statement
Informed written consent was obtained from all subjects involved in the study for use of routinely collected data for research purposes as part of their regular medical care in the contract of the University Medical Center Göttingen.