
Abstract
To study whether allowing adolescents and young adults (AYA) with chronic or oncologic diseases admitted to tertiary or intensive care units to share decisions in choosing the insertion site for central-venous catheters (CVC) implanted for intravenous therapies or parenteral nutrition reduces central-line-associated and catheter-related bloodstream infections (CLABSI and CRBSI). Following the PRISMA guidelines, we systematically reviewed the literature by searching MEDLINE, Embase, CINAHL, CENTRAL, SCOPUS, Cochrane Library, and Web of Science up to December 2019. According to our aims, the review identified no study that could be included. This empty systematic review on healthcare teams allowing AYA with chronic or oncologic diseases admitted in tertiary or intensive care units to share decisions in choosing the site for implanting CVC prompts further research on clinical pathways on this hot-topic. By considering purportedly risk-taking behaviors in youngsters thus reducing CLABSI and CRBSI, healthcare teams should test specific strategies by engaging AYA empathetically in sharing decisions on the site for implanting CVC to improve quality in health care bundles.
Keywords
Introduction
Even though social studies have only recently included adolescents and young adults (AYA) as a specific developmental stage in life, their unique features are well recognized and documented in psychosocial literature, hence assessing their specific needs and frequently risky behaviors is a hot-topic raising concern. 1 In AYA with chronic diseases, risk-taking behaviors tend to increase.2,3 One way to reduce multiple risk behavior would be to identify AYA assets, attitudes, and strengths thus promoting resilience. 4 Although health professionals give AYA inpatients broad information on concerns about their disease, unless specifically asked in empathic trustworthy clinical conversations, AYA are reluctant to discuss sensitive issues.5,6 Many AYA concerns, such as self-injury or suicidal ideations, involve broader chronic health matters that cause morbidity and mortality.7,8 Healthcare teams, focused on AYA disease-related and clinical issues, can neglect hidden AYA concerns, thus failing to engage them in choosing appropriate therapeutic care strategies and reducing adherence to treatment regimens.1,9–12 AYA whose chronic and oncologic diseases require complex care, including parenteral nutrition, invariably need central venous catheters (CVC).10,11 After CVC insertions, AYA should also receive face-to-face and digital education in managing CVCs to reduce risk behaviors such as noncompliance potentially determining dangerous central line-associated blood stream infections (CLABSI) and catheter-related blood stream infections (CRBSI).13–15
Given that the various CVC insertion sites leave CLABSI and CRBSI rates unchanged,16–19 multidisciplinary healthcare teams should share with AYA decisions on the CVC insertion site by using empathic shared decision-making (SDM) tools (decision aids). 20 Sharing decisions on the CVC insertion site is a promising new clinical SDM pathway, guaranteeing balanced communication with AYA addressing their esthetic body image, emotional, social, spiritual assets, and cognitive status especially during the lengthy disease course.21–24 Repeated CVC insertions over the years worsen AYA’s body image, and their psychosocial development to adulthood.18,19,22–25 Over time, complex CVC treatment courses lead AYA also to changes in regular life, sport, and fitness, even changing their potential interpersonal interactions with their peers.1,26–28 Although an SDM approach received international widespread endorsement as a clinical practice standard in health care groups treating children and AYA,1,29,30 care bundles, a set packages that provide technical and professional quality elements actively surveying CLABSI and CRBSI, include no empathic SDM approaches.14,31–33 Nor do SDM strategies provide specific information on the benefits and risks of CVC devices, minimize AYA concerns on their body image, and decrease their risk-taking behaviors.14,34,35 AYA with chronic and oncologic diseases should therefore have a say in choosing the CVC insertion site. 36 To satisfy AYA, reduce their esthetic concerns and risk-taking behavior, we need tailored empathic SDM approaches allowing AYA to manage CVC better over time thus reducing CLABSI and CRBSI.34,37
We undertook a systematic review by searching multiple databases to assess the potential impact of allowing AYA, suffering from chronic diseases or cancer, to share decisions in choosing the insertion site for implanting CVCs for intravenous medium- or long-term therapies or parenteral nutrition thus reducing CLABSI and CRBSI rates.
Materials and methods
Literature search
We conducted a systematic literature search to identify all studies focused on SDM strategies in AYA with chronic diseases or cancer for choosing the CVC implantation site and reducing possible CVC associated bacteremia (CLABSI and CRBSI). We searched the following databases: the Cochrane Central Register of Controlled Tri (2019, Issue 7; 31 December 2019); PubMed (from 1966 to 31 December 2019); Embase (Elsevier, embase.com, from 1974 to 31 December 2019); CINAHL (EBSCO HOST; from 1982 to 31 December 2019); SCOPUS (from 1970 to 31 December 2019); Web of Science (from 1990 to 31 December 2019). No language limitation. See Appendix 1 for the full search strategies for each database. We followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) group guidelines. 38
Inclusion and exclusion criteria
Intervention types and comparison groups: SDM approaches with AYA suffering from chronic diseases or cancer allowing them to share decisions in choosing the implantation CVC site for complex therapies or parenteral nutrition. Outcome types: reduction in CLABSI and CRBSI. The review included all study designs except abstracts, unpublished studies, conference presentations, and editorials.
A protocol for this systematic review has been registered prospectively in the PROSPERO database [CRD42020162886] https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=162886.
Results
Through specific tailored search strategies, starting on 10 May 2018 and ending on 31 December 2019, we identified 2465 records. After removing duplicates, we obtained 1710 references. By screening titles and abstracts, we excluded 1691 papers. A total 19 eligible articles were acquired in full text and carefully read by two authors (PR and RS) for inclusion. The two authors agreed on excluding the 19 articles that failed to meet the predefined inclusion criteria (Flowchart on literature search and study selection in Figure 1).
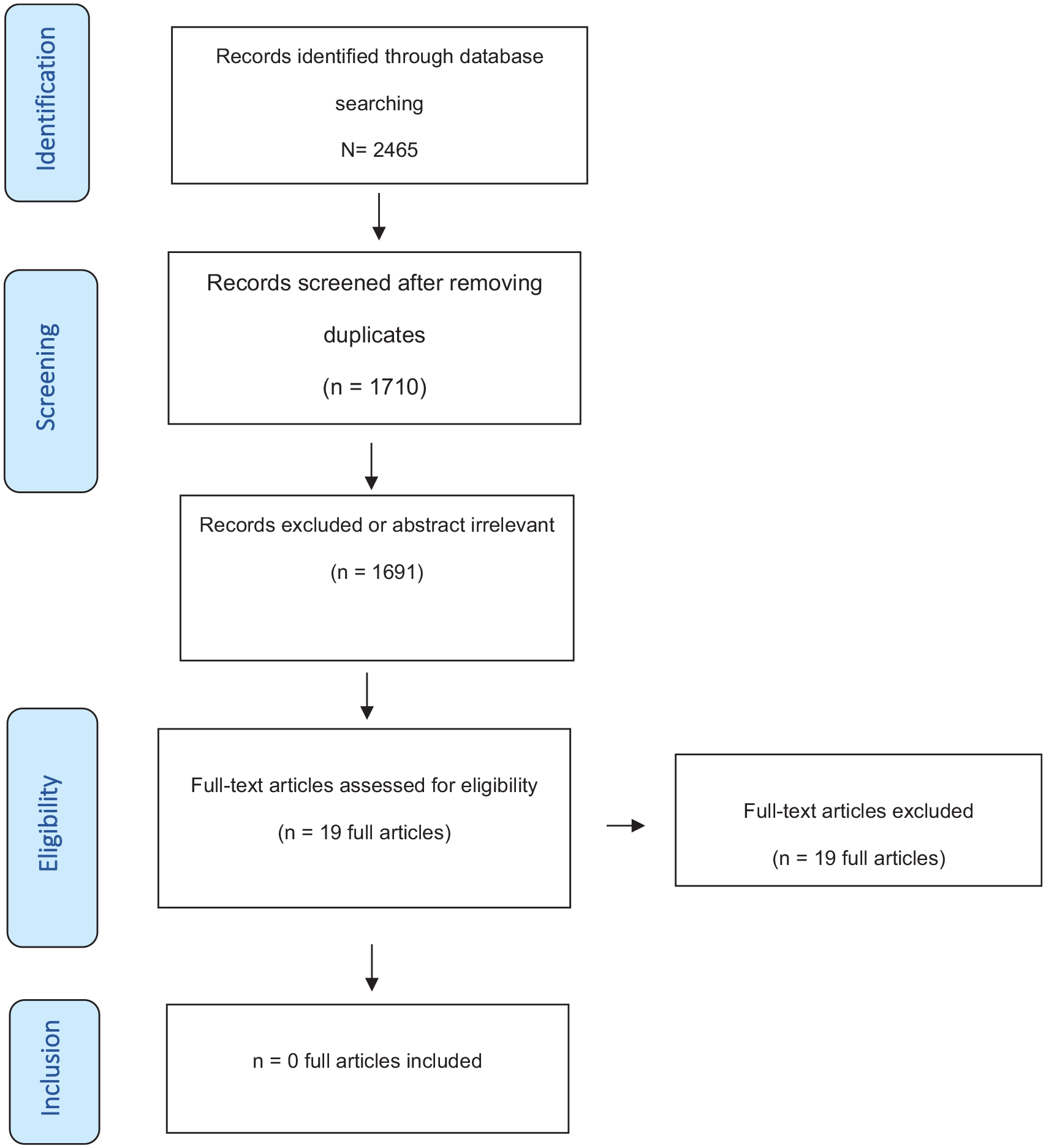
PRISMA 2020 flow diagram. PRISMA indicates preferred reported items for systematic reviews and meta-analyses. 38
Discussion
Surprisingly, although we searched systematically in several databases without limitations on study design, time, and language, our review identified no clinical studies on the potential impact of allowing AYA, suffering from chronic diseases or cancer, to share decisions in choosing the insertion site for implanting CVCs for intravenous medium- or long-term therapies or parenteral nutrition thus reducing CLABSI and CRBSI rates. We hope this empty review gives a sound standpoint on the hot-topic of engaging AYA in SDM strategies to enable them to choose the CVC insertion site thus reducing CLABSI and CRBSI rates. Empty reviews are important because they tell us why we need to search systematically on major topics highlighting the extent of evidence at a point in time. 39 Systematic reviews including clinical trials are necessary but insufficient for informing shared therapeutic decisions for individual patients and policies. 1 Our empty review therefore justifies further qualitative research on the potential harms of failing to engage AYA in quality healthcare bundles, also investigating important factors such as AYA-related assets, attitudes, needs, preferences, priorities, resources, and spiritual values. 5 Clinical research on patients’ benefits must include co-production in specific important clinical outcomes tailored in partnership with patients. 40 We agree that the current approach on providing AYA with traditional healthcare antimicrobial information is an outdated model.13,41 We need to move toward a patient-centered software system for preventing infections and controlling surveillance, starting from focusing on understanding the enablers and barriers that impact on AYA participation. 6 Recent 3.0 software conversations, including questions on Home environment, Education and employment, Eating, peer-related Activities, Drugs, Sexuality, Suicide/depression, and Safety from injury and violence (HEEADSSS 3.0) setting up the conversation, covering tricky questions, building trust, and getting difficult conversations back on track, can allow AYA to cooperate with healthcare teams in sharing decisions in choosing the CVC site.6,42 Software decision aids to standardize clinical strategies for treating AYA might restore their trust in healthcare professionals, reduce AYA risk behaviors, and increase their self-esteem.1,6 A qualitative report from three large public hospitals in Sydney provides evidence that in depth-interviews undertaken in a sample of patients and healthcare providers, re-imagined patient involvement in infection prevention and control, and assured antimicrobial stewardship. 43 This report highlights three new barriers in the current hospital landscape. First, the health system focuses on providing information as the primary strategy (generally reactive not proactive). Second, major misunderstandings exist about what patient involvement entails; and third, both healthcare workers and patients acknowledge that “everybody has a role to play in infection prevention and control,” but no one is sure which activities could work best. 43
Another barrier to engaging AYA in sharing decisions on the CVC insertion site, is the failure to refer them in healthcare bundles for surgical evaluation, and explain alternative insertion sites. 28 Whereas healthcare strategies enabling patients to choose CVC implantation sites showed that patients preferred one site over another because they perceived a lower infection risk and better associated hygiene, clinical prejudices, and interests might decide differently. 44 To reduce CLABSI and CRBSI rates, healthcare teams need to overcome clinical technical interests, and focus on engaging AYA in choosing CVC insertion sites by considering crucial AYA assets, attitudes, and perspectives.
Conclusion
Our empty review underlines the compelling need to design and conduct future studies with a high-quality clinical protocol and qualitative outcome assessment co-produced with youngsters over a long follow-up period on empathic SDM approaches by engaging AYA in choosing the site for implanting CVCs to minimize their esthetic concerns and managing CVCs better over time to decrease risk-taking behaviors thus reducing CLABSI and CRBSI. Further research could address whether these changes might apply in other age groups.
Supplemental Material
sj-pdf-1-jva-10.1177_11297298221074448 – Supplemental material for Does letting adolescent and young adult inpatients share decisions in choosing the central-line insertion site reduce central-line-associated bloodstream infections? An empty systematic review
Supplemental material, sj-pdf-1-jva-10.1177_11297298221074448 for Does letting adolescent and young adult inpatients share decisions in choosing the central-line insertion site reduce central-line-associated bloodstream infections? An empty systematic review by Paola Rosati, Alessandro Crocoli, Rosella Saulle, Laura Amato, Matilde Brancaccio, Zuzana Mitrova, Gaetano Ciliento, Marta Ciofi degli Atti and Massimiliano Raponi in The Journal of Vascular Access
Footnotes
Appendix: Search strategies to identify studies
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received a grant from the Italian Ministry of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.