
Abstract
Objective:
To investigate the feasibility of percutaneous arteriovenous fistula creation in consecutive patients screened for first access creation.
Methods:
Prospective study of ultrasound mapping based on the following minimal anatomic requirements: a patent proximal radial artery and adjacent elbow perforating vein with straight trajectory, each greater than or equal to 2 mm in diameter and within 1.5 mm of each other. In addition, the same population was evaluated for feasibility of a distal radiocephalic fistula established.
Results:
One hundred consecutive patients were examined between November 2018 and January 2019. Sixty-seven were male (67%) and mean age was 61 years. Sixty-three patients (63%) and a total of 100 limbs (50%) were found to be eligible for a percutaneous fistula creation with Ellipsys®. Thirty-seven percent of patients were ineligible because of the absence of both median cephalic and median cubital veins (15%), absence or inadequate elbow perforating vein and/or smaller than 2 mm proximal radial artery (14%), and/or distance greater than 1.5 mm (8%). We found suitable vessels for a surgical distal fistula creation in 91 extremities (45%), but this percentage dropped to 17% in patients over 70 years old. Among the 100 limbs eligible for percutaneous arteriovenous fistula, only 30 (30%) were eligible for radiocephalic arteriovenous fistula.
Conclusion:
More than 60% of patients were eligible for Ellipsys. The absence of veins at the elbow and a large distance between vessels were the most common limiting factors. Less than one half of the patients were candidates for surgical fistula and this percentage dropped significantly for older individuals.
Keywords
Introduction
Native arteriovenous fistulae (AVF) are known to be the preferred vascular access for hemodialysis in patients with end-stage renal disease. 1 Since the first AVF creation of a side-to-side anastomosis by Appell, Brescia, and Cimino, the number of AVF options evolved substantially over the years. 2 The success of a surgical AVF is largely dependent on reliable preoperative vessel mapping in addition to surgical skill and experience. 3 AVF creation with the use of the perforating vein of the elbow (EPV) has been described as a valuable alternative for autogenous access creation and particularly in elderly diabetic patients. 4 The Ellipsys® vascular access system (Avenu Medical San Juan Capistrano, CA, USA) allows the percutaneous creation of an AVF between the EPV and the proximal radial artery (PRA); however, a suitable candidate needs to meet specific anatomic criteria.5,6 We sought to prospectively determine the percentage of patients anatomically eligible for percutaneous arteriovenous fistula (pAVF) and/or a radiocephalic arteriovenous fistula (RcAVF) among a group of consecutive patients being evaluated for first vascular access creation.
Materials and methods
Data of both upper limbs in 100 consecutive patients referred to our vascular laboratory for preoperative duplex scan mapping before first AVF creation were prospectively collected and evaluated. Both arms were mapped to include an evaluation of the EPV and its relationship with the PRA for a pAVF creation in addition to accessing the anatomic suitability for constructing a RcAVF. The feasibility criteria used to determine pAVF eligibility were defined according to the instructions for use of the device (IFU): existence of a patent PRA and adjacent EPV with reasonably straight segments and both vessels greater than 2 mm in diameter and within 1.5 mm of each other. These criteria defined the minimal requirements for construction of a pAVF. Patients were also evaluated for feasibility of a distal RcAVF based on current standards and reported guidelines that include minimal radial artery diameter of 2 mm and cephalic vein diameter of 2.5 mm.1,7,8 A single experienced trained physician (G.F.) performed the examinations with an ARIETA 70 scanner (Hitachi-Aloka LTD, Tokyo). The compound feature and harmonic imaging was used in all cases. High-frequency linear transducer broadband design 5–18 MHz was used for near-field resolution improvement. The diameters of the artery and vein were determined by B-mode ultrasonography in a transverse and longitudinal plane from inner edge to inner edge. A Tourniquet was used for vein measurements in a room that was appropriately warm. The distance between artery and vein was measured at the location where they were closest to each other on longitudinal or transverse plane (Figure 1).
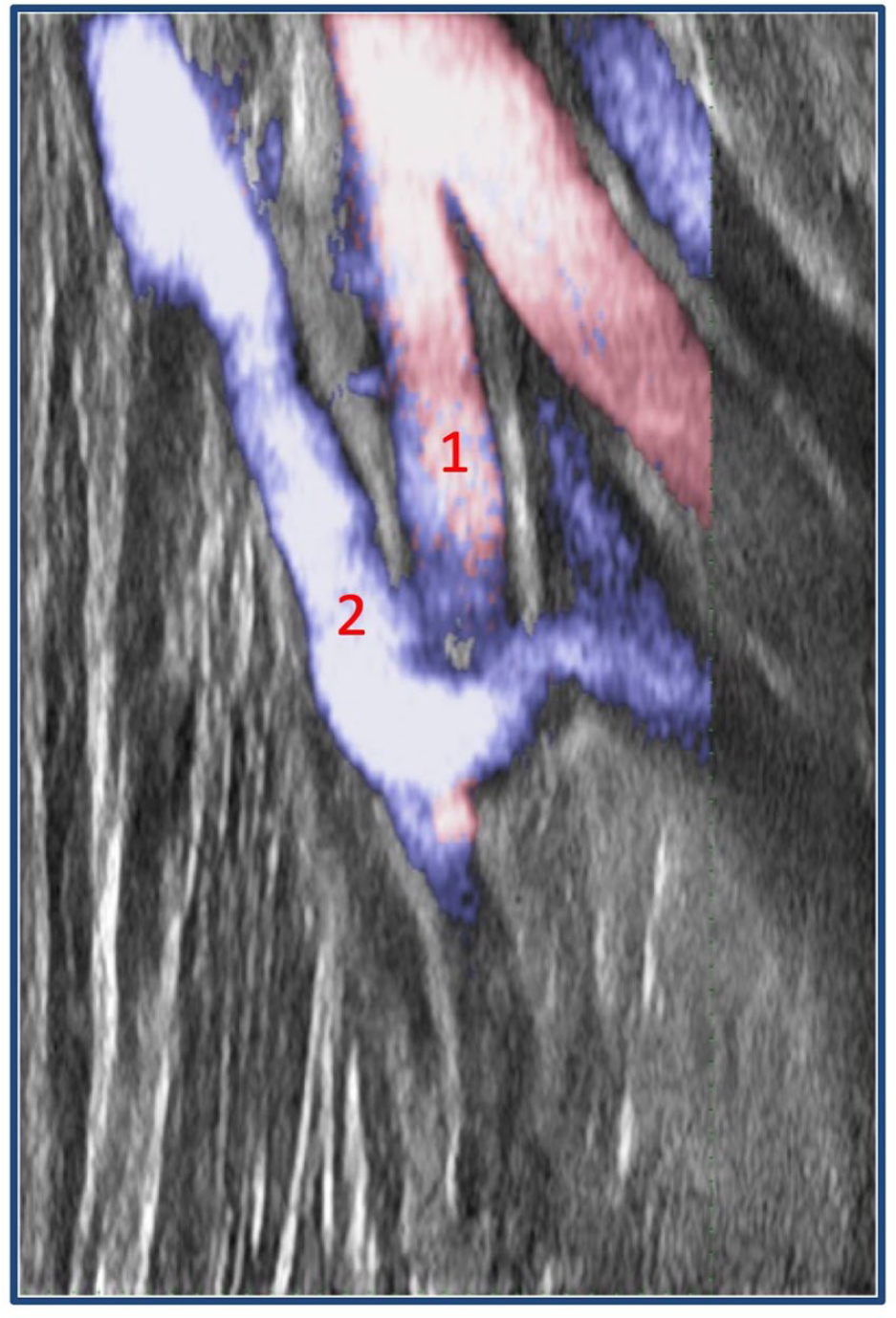
Duplex scan of antecubital fossa. Note the proximity between (1) proximal radial artery (PRA) and the (2) elbow perforating vein (EPV).
Nomenclature of the superficial veins in the forearm and in the elbow crease is highly variable in the literature. In this report, ‘median cephalic vein’ (MCV) refers to the superficial vein of the antecubital fossa that connects the median antebrachial vein (MAV) to the cephalic vein of the arm. Similarly, ‘median basilic vein’ (MBV) (often referred to as the median antecubital vein) is the superficial vein connecting the MAV to the basilic vein of the upper arm.
The study was approved by the Institutional Review Board (Comité d’Evaluation des Protocoles et d’Aide à la Recherche Protocol Evaluation and Research Assistance Committee–CEPAR) and is in accordance with the Declaration of Helsinki. Individual informed consent was obtained from all patients.
Results
Both upper limbs of 100 consecutive patients were assessed for a first AVF creation between November 2018 and January 2019. Sixty-seven were men, and mean age was 61 years (range = 21–87 years; standard deviation (SD) = 20.8 years). Sixty-three (63%) were found to be eligible for a pAVF. Fifteen patients (15%) were ineligible because they had no superficial veins at the elbow. A small PRA and/or highly tortuous EPV was the next more common contraindication (14%) while distance >1.5 mm between the two vessels was the least frequent finding (8%). Evaluation by individual limb found 62 limbs (31%) had PRA diameter smaller than 2 mm. Twenty-four limbs (12%) had distance between the PRA and adjacent EPV greater than 1.5 mm. In 32 upper extremities (16%), the EPV was smaller than 2 mm. In total, and strictly following the above-mentioned anatomic criteria, 100 arms (50%) in 63 patients (63%) met the criteria for creation of a pAVF.
In 26 patients (26%), only a unilateral pAVF was possible while in 37 (37%) a pAVF creation was possible in both arms. In 92 limbs (46%), both median cephalic and basilic veins were patent at the elbow, and 29% had only one patent vein at the antecubital fossa (18% MCV and 11% MBV only). In eligible patients, the average diameter of the EPV was 2.6 mm (range = 2–5 mm; SD = 0.77). Average diameter of PRA was 2.35 mm (range = 2–3.5 mm; SD = 0.33), and the average distance between the PRA and adjacent EPV was 1 mm (range = 0.2–1.5 mm; SD = 0.33).
Twenty-six patients (26%) had anatomical variations of the arterial network. Seven (7%) were bilateral and 19% unilateral involving 33 limbs (16.5%). Thirty-one limbs (15.5%) had a high take off of the radial artery (29 from brachial artery and 2 from axillary artery) while 2 had high take off of the ulnar artery (1%). In this group of patients, only six pAVFs (23%) would have been feasible. The limiting factors were distance >1.5 mm between EPV and the PRA (42%) and a PRA diameter <2 mm (48%) being the most common.
Creation of a distal RcAVF was possible in 91 limbs (45%); however, this percentage dropped to 17% in patients older than 70 years. Among the 100 limbs eligible for a pAVF, only 30 (30%) were eligible for a RcAVF.
Discussion
This study found 63% feasibility of pAVF with the Ellipsys vascular access system in consecutive patients screened for first fistula creation. In the same group, 45% were good candidates for creation of a surgical distal AVF while this number dropped to 17% in patients older than 70 years.
The anatomy of superficial veins of the upper extremity is highly variable. Within the antecubital fossa, the MCV and the MBV usually form a junction in a Y- or M-like shape with the ostium of the EPV usually located at the distal portion of this junction. Alternatively, 5%–10% of all patients have either a MBV or a MCV, but not both.
Perforating veins are numerous, most of them have a small diameter often less than a millimetre and represent connections between the superficial and deep veins that accompany the arteries and are also described as ‘venae comitans’. In two locations they may exist without valves allowing venous blood flow in both directions. The first is within the first intermetatarsal space on the back of the foot, and the second is the EPV in the antecubital fossa, connecting the deep system with the MCV in 70% and with the MBV in 30% of cases. In regular flow conditions where a distal AVF is not present, blood is directed from the deep towards the superficial venous system. In patients with a distal RcAVF at the wrist, flow is reversed in the EPV, draining part of the AVF flow into the deep system. Studies have confirmed the presence of other small perforators within the forearm, connecting the radial venae comitans and the superficial venous system. If functional valves are not present, a distal pAVF creation with the Ellipsys vascular access system can be created through these more distal perforators if vessel size criteria are met.9–11
Surgical AVF creation between the PRA and the EPV has been well described as a safe option for patients who are not good candidates for a distal RcAVF. Using the PRA as the inflow site for the anastomosis offers advantages when compared to the distal radial artery due to a larger diameter and freedom from severe distal radial artery calcifications encountered in some patients. Excellent patency and maturation rates are combined with lower risk for steal syndrome and excessive flow, making this an important vascular access option between distal RcAVF and brachial inflow AVFs, particularly for the elderly and/or diabetic patients increasingly encountered as hemodialysis candidates.12–19
The pAVFs created with the Ellipsys system are constructed at the same site as surgically created PRA-AVFs and may offer the same favourable advantages. The combination of a precise and limited sized anastomosis with both MCV and MBV outflow maintains the AVF in a moderate flow and low-pressure state; positive factors in terms of long-term patency and minimizing risk of complications.5,6,20 The simplicity and relative short procedure time for the Ellipsys technique, combined with local or regional anaesthesia and requiring only ultrasound guidance with a single venous puncture, makes this an appealing minimally invasive procedure when the specific anatomic criteria outlined here are present.
We found that 63% of patients have suitable anatomic criteria for a pAVF creation with the Ellipsys vascular access system. The absence of superficial veins and anatomical variations of the PRA were the most common reasons noted for lack of patient suitability for this technique. We also found that a high brachial artery bifurcation was associated with a fewer opportunities for creation of a pAVF.
To our knowledge, this is the first prospective evaluation of consecutive patients regarding the presence of anatomic criteria for pAVF creation. In a retrospective review, Hull et al. 21 reported 87.9% of the limbs suitable for pAVF creation at the level of the PRA in a study based on vein and arterial mapping data. Although our results indicate somewhat lower feasibility rates, more challenging patients may be considered by experienced operators. These may include individuals with a more tortuous EPV or a smaller PRA that could be dilated immediately before creation. In addition, the possibility of distal radial pAVF creation in selected cases with adequate distal perforators in addition to our early experience in patients without superficial vein options, creating pAVFs with radial vein outflow for subsequent brachial vein superficialization, might bring the percentage of feasibility up to 80%. Surgical PRA to radial vein outflow AVF for staged brachial vein for staged brachial vein transposition is a successful surgical strategy.22,23 A pAVF creation for brachial vein outflow and subsequent staged elevation represents a promising opportunity for an autogenous access which should be evaluated in future studies.
PRA-AVFs offer a valuable option for reliable and safe hemodialysis access in older patients.4,19 In this study, 17% of patients older than 70 years had suitable anatomy for distal RcAVF creation and only 30% of limbs where a pAVF was feasible, a RcAVF was also possible. This indicates that the two techniques are complementary, especially for the older and sicker patients.
Conclusion
More than 60% of patients meet the strict anatomical requirements for creation of a pAVF in the proximal forearm with Ellipsys. The absence of veins at the elbow and a large distance between vessels are the most common limiting factors. Less than one half of the patients were candidates for surgical RcAVF, and this percentage dropped significantly for individuals older than 70 years. Larger multicentre studies are required for confirmation of the above findings.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs Mallios and Jennings are consultants and shareholders for Avenu Medical.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.