
Abstract
Background and objectives:
The recent advent of a device to create a proximal radial artery arteriovenous fistula using an endovascular approach to create the anastomosis represents a significant advance in dialysis access creation. This endovascular arteriovenous fistula offers the beneficial attributes of the proximal radial artery arteriovenous fistula while adding the advantages of avoiding a surgical procedure. The endovascular arteriovenous fistula can be created safely, functions well, has excellent patency, and has a high degree of patient satisfaction. The purpose of this study is to report the 2-year cumulative patency rate for a large multicenter cohort of endovascular arteriovenous fistula cases.
Design:
An endovascular arteriovenous fistula was created in 105 patients using either local or regional anesthesia and conscious sedation. Patient data were obtained from each program’s electronic health record system. Data collection was truncated at 2 years postprocedure and used to calculate cumulative patency. Post-access creation patient satisfaction was assessed.
Results:
A physiologically mature arteriovenous fistula (blood flow ⩾500 mL/min and a target vein internal diameter ⩾4 mm) was obtained in 98%. A clinically functional arteriovenous fistula (supporting two-needle dialysis according to the patient’s dialysis prescription) was demonstrated in 95%. Access failure resulting in the loss of access occurred in eight cases during the study period. The cumulative patency rate at 6, 12, 18, and 24 months was 97.1%, 93.9%, 93.9%, and 92.7%, respectively. The post-procedure patient evaluation emphasized a high level of patient satisfaction.
Conclusion:
The proximal radial artery arteriovenous fistula created using an endovascular approach for the anastomosis is associated with excellent 2-year cumulative patency and is associated with a high level of patient satisfaction.
Keywords
Introduction
The goal of a dialysis vascular access is to provide reliable access to the circulation suitable for sustained clinical use with minimal complications associated with either its creation or its use. Of the alternatives available, an arteriovenous fistula (AVF) represents the best choice for most patients. The mature, clinically functional AVF is associated with lower morbidity and mortality, better patency rates, and a higher level of patient satisfaction and quality of life than other alternatives. 1
Traditional dialysis access planning generally evaluates the possible creation of one of three AVF configurations: radial-cephalic, brachial-cephalic, or brachial-basilic. Patient selection is important because each of these have associated disadvantages. When several choices are possible based upon vascular mapping and physical examination, preference is given to using the forearm over the upper arm. 2 Unfortunately, the forearm radial-cephalic AVF has a higher primary failure rate and shorter duration of patency than an AVF created in the upper arm, especially in the elderly patient.1,3 However, the incidence of dialysis access steal syndrome (DASS) and high-output cardiac failure is higher with an upper arm AVF.4,5 This increased incidence is attributed to the use of the brachial artery and the associated higher blood flow rate.
In order to increase the opportunities for the creation of an AVF, a variety of other configurations have been described. 6 One of these is the proximal radial artery (PRA)-AVF. Although first described in 1977, 7 until recent years, the PRA-AVF has been infrequently used, a problem likely due to unfamiliarity with this access option and its non-inclusion in common guidelines. Experience with the PRA-AVF has shown it to have a lower complication rate and a primary, assisted primary, and cumulative patency rates that are superior to the radial-cephalic AVF especially in elderly 8 as well as pediatric patients. 9 In addition, by using radial artery AVF inflow rather than from the brachial artery, there are lower risks of DASS, arm edema, high-output cardiac failure, the development of a “mega-fistula,” and idiopathic monomelic neuropathy.8,10–13 As a result, some surgeons have adopted this configuration as the first alternative in a patient in whom a radial-cephalic AVF is not feasible or where marginal vessels suggest a high likelihood of failure. 14
The recent advent of a device to create an endovascular AVF (enAVF) represents a significant advance in dialysis access creation. Although viewed as a new type of AVF, it is in reality a PRA-AVF in which the anastomosis is created in a unique manner using a novel endovascular device. 15 As such, the enAVF has the beneficial attributes of the PRA-AVF10,11,16–20 while adding the advantages of avoiding the trauma of surgery by allowing a percutaneous approach performed under local/regional anesthesia. In addition, the location of the anastomosis and lack of an incision significantly expands the cannulation zone of the access in many patients.
Previous reports have documented the safety of this technique for creating an anastomosis resulting in a functional dialysis access with excellent primary and cumulative patency rates and a high degree of patient satisfaction.21–24 The purpose of this study is to report the 2-year cumulative patency rate for a large multicenter cohort of enAVF cases. In addition, patient satisfaction with this approach to creation of an access was further examined.
Methods
This was a retrospective analysis of data generated by five vascular access programs in the United States. This study obtained prior approval from the institutional review board and was in accordance with the Declaration of Helsinki. Individual informed consent was not required by the institutional review board since this was a retrospective study.
After a vascular evaluation for suitability, all patients had an enAVF created using the using the Ellipsys® Vascular Access System (Avenu Medical, San Juan Capistrano, CA) as has been previously described.21,22 This is a thermal resistance device consisting of a single venous access catheter. Using either local or regional anesthesia and conscious sedation, the catheter was introduced retrograde over a guide wire through a single cannulation of either the cephalic or median cubital vein at the elbow. The device was then advanced through the deep communicating vein and into the adjacent PRA. The Ellipsys enAVF procedures were completed using only ultrasound guidance without radiation exposure. An anastomosis was created using the device to apply pressure and heat to securely fuse the deep communicating vein and PRA in the antecubital fossa where these two anatomic structures are adjacent. Following the creation of the anastomosis, it and the deep communicating vein were dilated with a 5 mm angioplasty balloon under ultrasound guidance as a planned secondary procedure.21–24 Currently, the balloon dilatation of the anastomosis is completed immediately as a routine part of the primary procedure.21–24 The definition for a physiologically mature AVF used in this study was a brachial artery blood flow ⩾500 mL/min and a target vein internal diameter ⩾4 mm. 21 A clinically functional AVF was defined as an access capable of supporting two-needle dialysis according to the patient’s dialysis prescription.
Patient data were obtained from each program’s electronic health record system using a specially created data collection form. Random audits were conducted to assure complete and accurate retrieval of data. The electronic medical record contained patient data entered by the facility creating the access as well as that entered at the dialysis treatment facility by the facility staff. Data collection was truncated at 2 years postprocedure (730 days).
A post-access creation patient satisfaction assessment survey was developed by a trained research assistant/patient advocate and mailed to each patient 2 years (plus or minus 30 days) after enAVF creation.
This included a five-level Likert-type scale with 1 being “Excellent” and 5 being “Poor” as well as questions that could be answered yes or no. At the end of the study period, the survey was mailed to all patients still active in the study. In addition, a patient engagement focus group which included patients who were from 1½ to 2½ years after enAVF creation was convened and led by an experienced facilitator to further explore patient satisfaction.
Summary statistics for continuous variables were reported as a mean, 95% confidence interval (CI), and a range. The cumulative patency rate was determined using Kaplan–Meier life table analysis according to standard definitions. Transplantation, loss to follow-up, and patient death were considered to be censored events. MedCalc Statistical Software version 16.8 (MedCalc Software bvba, Ostend, Belgium; https://www.medcalc.org; 2016) was used for all analyses.
Results
A total of 105 patients were entered into this study. This number included all cases of an enAVF created at these five centers during a time period that would allow for a 2-year follow-up. Patient demographics are shown in Table 1. The mean age of the cohort was 56.2 years with the range of 30–80 years. Almost three-fourths were male, and the majority of the patients were at least moderately obese (median body mass index (BMI) = 30.1). Patient demographics other than those reported were not collected.
Patient demographics.
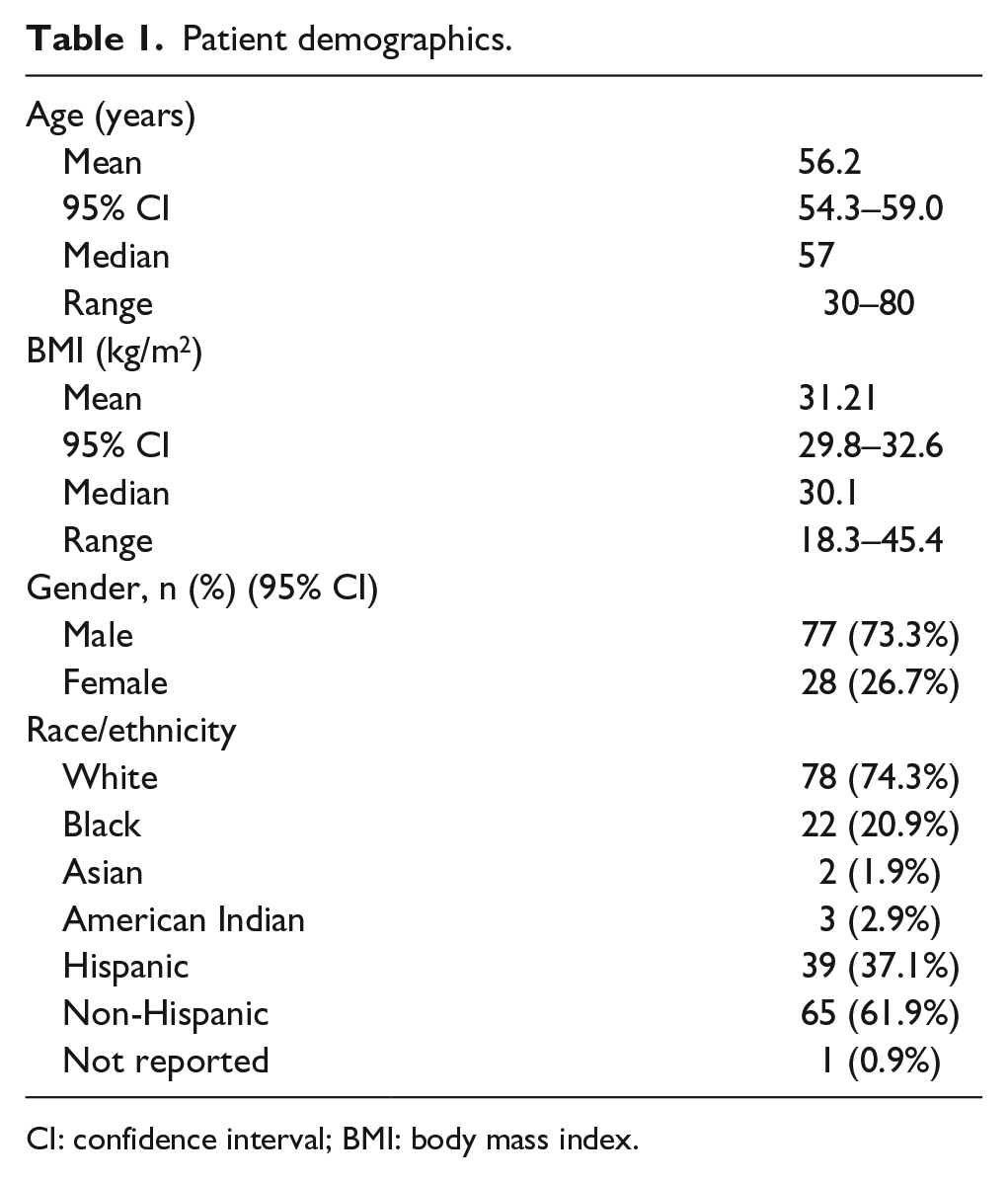
CI: confidence interval; BMI: body mass index.
The criteria for use of the enAVF (physiologically functional AVF) was met in 103 patients and was used to provide two-needle dialysis in all except three of these cases. In one case, the patient did not reach the point of requiring renal replacement therapy during the study period. In two cases, the patients were receiving peritoneal dialysis and the arteriovenous access was created as a backup. Each of these three individuals had a physiologically functional AVF.
Access failure resulting in the loss of access occurred in eight cases during the study period. There were two cases (1.9%) of primary failure and six instances (5.7%) of late failure occurring at a mean of 317 days (95% CI = 120–514, range = 35–603) following creation of the enAVF. A total of 18 patients (17%) died with a functioning AVF during the course of the observation period from causes unrelated to the access procedure. The duration of function in these 18 cases had a mean of 353 days (95% CI = 252–453, range = 28–669). Six patients (5.7%) received a renal transplant. The enAVF was functioning at the time of the transplant procedure at a mean of 201 days (95% CI = 75–327, range = 79–381). In most of these cases, the access was not ligated after transplantation. It was felt that ligation was not necessary because of the absence of high blood flow. The cumulative patency rate for the total cohort at 3, 6, 9, 12, 15, 18, 21, and 24 months was 96.1%, 96.1%, 95%, 92.8%, 92.8%, 92.8%, 91.6%, and 91.6%, respectively (Figure 1).
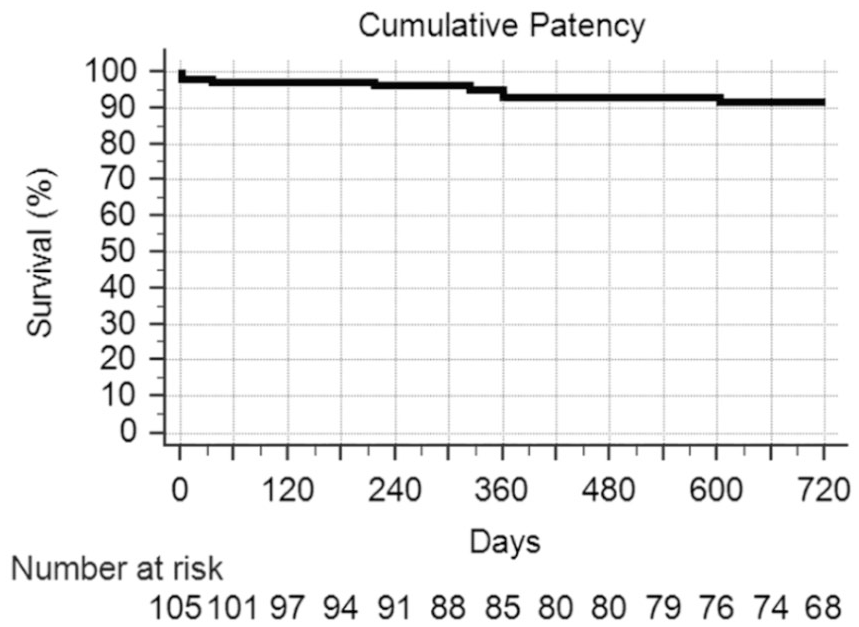
Cumulative patency for study group.
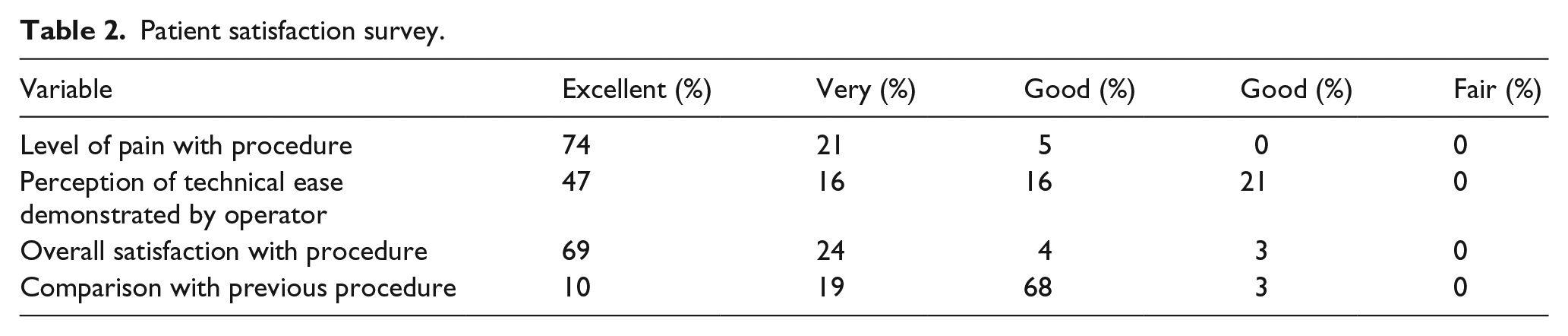
The post-access creation patient satisfaction assessment survey mail-out received a 39% response rate. The results obtained from the five-level Likert-type scale portion of the questionnaire are shown in Table 2. Patient responses indicated a high level of satisfaction with the procedure. A lack of pain perceived by the patient was rated at excellent or very good in 95% of cases. The overall satisfaction with the procedure was rated as excellent or very good in 93% of cases. Only one-third of the responders had a previous dialysis access procedure. These patients were asked to compare the enAVF procedure with their previous experience as either much better, better, same, or worse. Their responses were 10%, 19%, 68%, and 3%, respectively.
Patient satisfaction survey.
Information gained from the focus group emphasized a high level of patient satisfaction that an open surgical procedure was not required. An improved body image impression in comparison with other patients with an AVF in the dialysis facility was expressed. No opinions were expressed on issues related to cost, infection, and avoidance or decreased use of a dialysis catheter use due to a lack of patient information on these issues. Difficulty in cannulation was mentioned as a problem and attributed by the patient’s to unfamiliarity of the dialysis facility staff with the enAVF.
Discussion
The optimal vascular access for dialysis is a clinically functional AVF.1,25 However, the key term is clinically functional. Unfortunately, a large percentage of surgically created AVFs experience either primary failure or failure to mature (FTM).26,27 Although many of these cases can be salvaged,28–30 between primary surgical failures and maturation failures, 39% of AVF placed between June 2014 and May 2016 in the United States were unsuccessful. 31 Many of these early AVF failures are ultimately salvaged, but frequently require more than one procedure to become clinically usable. 32 In addition, the AVF successfully treated for FTM has been shown to have a shortened primary patency rate in comparison to an AVF that matures without intervention making repetitive interventions necessary for continued clinical use.33–35 In addition, failure of AVF function results in an escalating cost. 36
The most common lesion resulting in FTM is stenosis of the juxta-anastomotic segment of the AVF with an overall incidence ranging from 43% to 55%. It has been reported to occur in 54%–77% of dysfunctional forearm AVFs and 46%–56% of those in the upper arm. 37 Although it seems apparent that there is an association with either the way the anastomosis is created or its configuration that results in vascular injury culminating in juxta-anastomotic stenosis, the exact etiology is not clear. Possible mediators of vascular injury in this setting include (1) direct hemodynamic injury due to non-laminar flow and oscillatory wall shear stress related to the anatomical configuration of the anastomosis, (2) surgical injury from surgical site inflammatory process, and (3) angulation and spiraling of the peri-anastomotic venous segment at the time of surgical AVF creation.38–41
These data make it clear that there is a need for innovation in AVF creation. It has been proposed that surgical techniques that minimize venous dissection might improve fistula maturation and access patency.39,41,42 These techniques have dealt primarily with variations in the configuration of either the vein 39 or the artery 41 used in creating the anastomosis and have shown a significant decrease in FTM and an improvement in AVF maturation. This study demonstrates that using this novel technique to create the anastomosis which avoids surgical trauma and vessel manipulation can result in a marked enhancement in the creation of a clinically functional dialysis access with the attributes of a PRA-AVF. The enAVF creates an anastomosis between the adjacent deep communicating vein and PRA, avoiding vessel mobilization, rotation of vein to artery, and the opportunity for technical misadventure. The vessels remain in their native position. Moderate flow and lower pressure produced by these PRA enAVFs also avoid the substantial risks associated with a brachial artery anastomosis.8,10–13
Although an AVF is the optimal vascular access, not all AVFs are equal. In a meta-analysis involving 200 studies reporting on 875,269 vascular accesses, 1 an upper arm AVF (brachial-basilic or brachial-cephalic) had the best primary patency. The primary patency for a radial-cephalic AVF was only slightly better than an arteriovenous graft (AVG) in males and not as good as an AVG in females. The PRA-AVF was not included in these studies. In spite of multiple reports of successful outcomes with the PR-AVF,10,11,16–20 this option for AVF configuration is frequently overlooked as an alternative. The brachial-cephalic AVF (BCAVF) is often the first option recommended for a patient in whom a radial-cephalic AVF is not possible. However, in a systematic review of 10 studies involving 1,310 patients with a PRA-AVF, 11 the primary failure rate, primary patency, and cumulative patency at 1 and 2 years were better than was reported in a large series of cases for either the standard forearm or upper arm AVF. 43 In a study which compared 56 cases of BCAVF with 50 patients having a PRA-AVF with a mean follow-up period of 1.8 years, 20 no differences in the percentage of the two access types being successfully used for dialysis treatment were noted and primary, primary assisted, and cumulative patency rates were similar between the two groups. However, complications such as arm swelling, DASS, and the development of aneurysms were significantly less common in the PRA-AVF group. It was suggested that the prevalence of these complications was less after creation of a PRA-AVF because the radial artery provides a lower blood flow rate. This is a particularly attractive characteristic of this access, especially in the elderly patient. 44
In previous reports, patency advantages of the enAVF in comparison to a surgical AVF have been documented.21–23 In the Pivotal Multicenter Ellipsys trial, 21 a primary failure rate of 5% was reported and cumulative patency for 107 cases was 92.3%; however, because some patients had not yet required renal replacement therapy at the end of the study period, only 88% of cases were using the access for dialysis. In another study involving 34 cases, 22 the primary failure rate was 3% (1 case). At 6 weeks, all fistulas had been used or were ready for use by clinical or ultrasound examination (vein diameter ⩾6 mm for a 10 cm length and blood flow ⩾600 mL/min). Access blood flow (measured at the brachial artery) at a mean of 669 mL/min immediately after access creation and 946 mL/min (range of 645–1486 mL/min) at the patient’s last follow-up visit in the study period (range of 53–229 days; average of 141 days). Based upon the time of the follow-up period, the primary patency, assisted primary, and cumulative patency rates were 82%, 94%, and 94%, respectively. In a third study involving 34 patients, 23 a primary failure rate of 3% was recorded. Successful two-needle cannulation within 10 days to 6 weeks after access creation was achieved in 82% of cases. 23 The average blood flow measured at the brachial artery, before the first cannulation was 850 mL/min. These Ellipsys PRA enAVF flow rates are well below the level noted to offer increased cardiac risk5,12 and support the findings of fewer complications when compared to brachial artery inflow AVF procedures.11,14,20
As is the case with many new procedures, the conduct of anastomosis creation using this technique has evolved with time. In the Pivotal Multicenter Ellipsys trial, 21 maturation procedures were required. These included anastomotic balloon dilatation in 72%, brachial vein embolization in 32%, cubital vein ligation in 31%, and surgical transposition in 26%. Recent modifications in the procedure which have included immediate angioplasty of the anastomosis and adjacent vessels have represented a significant improvement in the technique. 21 This change has eliminated the need for brachial vein coiling or venous branch ligation. Utilization of both the cephalic and median cubital veins for cannulation combined with the absence of a surgical incision has increased the AVF cannulation zone considerably, reducing the need for basilic vein transposition substantially.
The level of access blood flow obtained immediately following access creation has made early cannulation of the enAVF possible. In a study of 14 cases in which early cannulation was necessitated in order to either avoid catheter insertion or catheter exchange, 45 the time to first cannulation ranged from 1 to 12 days with a mean of 8 days. In six cases, time to first cannulation was 7 days or less. Immediately after access creation, access blood flow ranged from 491 to 1169 mL/min (mean = 772 mL/min). Successful dialysis was achieved in 100% of cases. Primary patency at 3, 6, and 12 months was 76%, 76%, and 66%, respectively. Assisted primary patency for the same intervals was 100%, 100%, and 91%, respectively. Cumulative patency was 100% at all three-time intervals.
Although patients with a functioning AVF report a better quality of life than those with other types of vascular access, a significant number of patients refuse to have an AVF created. 46 Patient satisfaction and their perception of quality of life are important. Body image related to disfigurement associated with a surgically created AVF, pain associated with surgery and failure of maturation requiring additional interventions have been noted as important factors in the patient’s perception of their vascular access.47–49 Patient experience with the enAVF reflected a positive response to these issues. The survey conducted to gauge patient’s response to the procedure indicated a high level of satisfaction with the procedure and the degree of pain associated with it (Table 2). These perceptions were reinforced in the focus group discussion as well as an appreciation of the avoidance a visible scar for aesthetic reasons related to body image an observation also made by other investigators. 23
Footnotes
Author contributions
G.A.B. complied the initial draft and analyzed the data. T.L. collected and collated the data, and also edited the manuscript. W.C.J. analyzed the data and edited the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: T.L. is a patient advocate for Avenu Medical, W.C.J. received a consulting fee as stock options.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.