
Abstract
Background:
The concept of calcar-guided short-stem THA (ssTHA) has largely emerged over the last decade, especially in Europe, and today modern calcar-guided short stems are among the most successful primary femoral implants in terms of complications and revision rates as indicated by multiple registry data. The philosophy originally comprised an individualised reconstruction of the hip anatomy by following the calcar of the femoral neck providing bone- and soft-tissue-sparing characteristics. However, as the stem design allows either metaphyseal fixation alone or additional diaphyseal anchoring, depending on the stem alignment and indication, distinct knowledge is required regarding the implantation technique, the broad variation of positioning and fixation and its potential clinical consequences.
Aim:
To report on and highlight the characteristics of different ways of performing calcar-guided ssTHA as well as to introduce a classification in order to systematically account for the variety of strategies and the respective implications on the type of fixation.
Surgical technique:
Already when templating preoperatively, surgeons need to weigh up the different fixation types taking into account a number of patient-related factors. Intraoperatively, by individually controlling the level of osteotomy, the intended type of anchorage can be implemented. Intraoperative radiography to confirm the result, is mandatory.
Results:
Despite numerous options of stem alignment, depending on the patient’s anatomy, the bone quality or the indication for operation, a total of 4 categories were identified to characterise different fixation strategies in calcar-guided ssTHA.
Conclusions:
The classification system should be used for the preoperative determination of the intended type of anchorage. Whenever a short-stem philosophy with metaphyseal fixation (Type I (M)) is possible, it should be pursued.
Introduction
Short stems have become increasingly popular in recent years. Short-stem THA (ssTHA) aims to preserve bone, prevent stress shielding, and provide favourable conditions for revision without altering the basic concepts of conventional THA. Most short-stem designs on the market focus on metaphyseal fixation.
The concept of modern calcar-guided short stems in THA aims for the precise reconstruction of the individual, anatomic hip geometry, using a bone- and soft-tissue sparing implantation technique, following the calcar of the femoral neck, associated with a physiological loading in the meta-diaphysis to conserve proximal bone stock over the long term. 1
The results of several national registries indicate that calcar-guided short stems are among the most successful implants in terms of early-stage survivorship. For example, in the German national joint registry (EPRD), calcar-guided short stems, such as the optimys stem (Mathys Ltd., Bettlach, Switzerland) and the A2 stem (Artiqo, Lüdinghausen, Germany), have been associated with excellent implant survival. 2 These results are strongly supported by findings from the Australian (AOANJRR) and the Swiss (SIRIS) national registries, which provided similar results for these implant designs.3,4
Calcar-guided short stems can follow a valgus anatomy into a valgus position or a varus anatomy into a varus position. The positioning must be accomplished by the surgeon, through the intraoperative selection of an individualised, adjusted level of resection, according to the preoperative plan. 1
This stem design allows for many ways of varying the fixation, such as either pronounced metaphyseal anchorage alone or with additional diaphyseal anchorage, depending on the stem alignment and indication.5,6
Thus, distinct knowledge is required regarding the implantation technique, the broad variation of positioning and fixation and its potential clinical consequences.
Changing the type of anchorage through the addition of a diaphyseal anchorage will potentially result in negative effects on proximal bone remodelling and stress shielding compared with metaphyseal anchorage alone.6,7 On the other hand, the option of additional individualised fixation types potentially increases the indications for the safe use of a short stem. Additionally, a number of biomechanical investigations have suggested a cemented version of this stem design may also be beneficial, 8 and a calcar-guided short stem with cemented fixation has recently entered the market.
The classification of this stem design, however, is challenging.
The purpose of this study was to report on and highlight the characteristics of different ways of performing calcar-guided ssTHA as well as to introduce a classification in order to systematically account for the variety of strategies and the respective implications on the type of fixation. Additionally, guidelines regarding indications will be provided in effort to support surgeons during their learning curve.
Surgical technique
The newest generation of calcar-guided short stems is mainly represented by the optimys stem, the A2 stem and the MiniHip stem (Corin, Cirencester, UK) (Figure 1(a–c)).
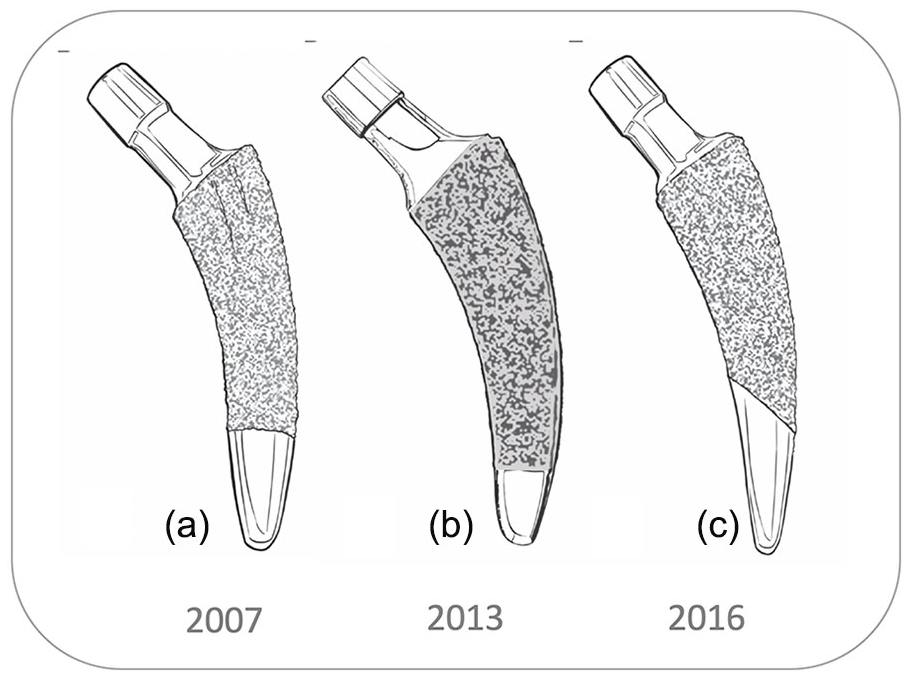
New-generation calcar-guided short stems (a) MiniHip (Corin) since 2007 (b) optimys, (Mathys) since 2013 (c) A2 (Artiqo) since 2016).
In new-generation, calcar-guided ssTHA, in addition to individualised positioning, the anchoring type can be individualised. For example, when using the stem in a varus position as well as in cases of good bone quality, a classical 3-point anchoring approach with metaphyseal fixation should be attempted (Figure 2(a)). In the neutral and valgus position, as well as in cases with compromised bone quality, an additional diaphyseal anchorage is possible (Figure 2(b) and (c)). In varus hips, the high level of the osteotomy proximal wedging combined with the three-point anchoring approach is typically sufficient, whereas in valgus hips, due to the low resection level, the stems may require an additional diaphyseal anchorage to achieve primary stability. 7 Most calcar-guided stem designs offer a lateralised offset version besides the standard offset version to account for the variation of anatomy and type of fixation (Figure 2(c)). When facing osteoporotic bone or a Dorr type C femur, cemented fixation should be chosen. 9
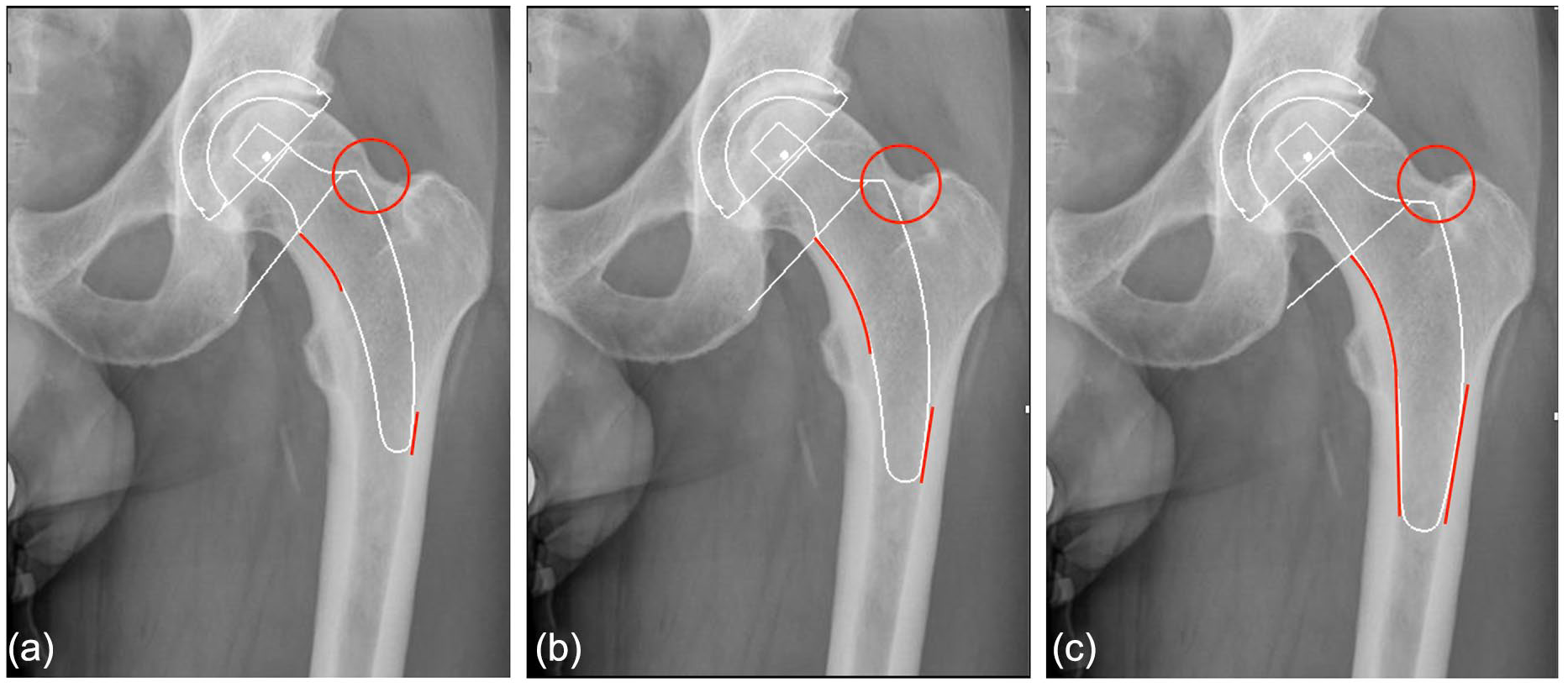
Different preoperative templating strategies in the identical patient (a) High osteotomy, varus alignment, shoulder superior to fossa, lateral point load (b) Intermediate osteotomy, varus or neutral alignment, same-level to fossa, lateral area load (c) Low osteotomy, neutral or valgus alignment, shoulder inferior to fossa, distal fit-and-fill.
Already when templating preoperatively, surgeons need to weigh up the different fixation types taking into account a number of patient-related factors (Figure 2(a–c)). Intraoperatively, by individually controlling the level of osteotomy, the determination of the entry point into the femoral neck and the final height of the implant shoulder as well as the choice of the standard or lateral offset, the intended type of anchorage can be implemented. Intraoperative radiography to confirm the result, is mandatory. In cases of malalignment, insufficient cortical contact or undersizing, adjustments have to be made.10,11
The alignment strategy and the intended type of anchorage require an individual approach for each patient and each case. Therefore, a new classification system in calcar-guided ssTHA is introduced.
Classification of calcar-guided ssTHA
The most relevant classification system for short stems to date, described by Khanuja et al. 12 , was introduced in 2014. This system categorises all short-stem designs into 4 groups. The group of calcar-guided stems (Group 2) comprises the group of calcar-loading stems. A subclassification method was added, dividing calcar-loading stems into trapezoidal, rounded, threaded, and thrust-plate designs. Modern calcar-guided short stems are almost exclusively classified as trapezoidal, rounded, calcar-loading stems according to the system defined by Khanuja et al. 12 (Groups 2A and 2B).
To account for differences in the individualised positioning and anchorage of calcar-guided short stems, a second subclassification method was suggested earlier, distinguishing metaphyseal anchorage (for example Group 2B(M)) from meta-diaphyseal anchorage (Group 2B(MD)). However, the previous attempts to provide a systematic classification in calcar-guided ssTHA were insufficient. 13
Thus, this is the introduction of a new systematic classification system in calcar-guided ssTHA.
There are 4 categories of individualised fixation strategies. Those are classified type I through IV (Figure 3(a–d)).

Classification system in calcar-guided ssTHA (a) Type I (M), metaphyseal anchorage (b) Type II (MD), meta-diaphyseal anchorage (c) Type III (D), diaphyseal anchorage (d) Type IV (C), cemented fixation.
Type I (M): metaphyseal anchorage
In type I category, only metaphyseal fixation is accomplished (M). This may be considered the original “short stem philosophy”. Characteristics are a high level of osteotomy, varus or neutral stem alignment, implant shoulder superior to the fossa piriformis and point loading at the distal lateral cortex. In almost all cases, a standard offset version is sufficient in reconstructing the lateral femoral offset. In this category, Dorr type A is mandatory (Figure 3(a)).
Type II (MD): meta-diaphyseal anchorage
In type II category, in addition to the metaphyseal fixation, there is also partial diaphyseal anchoring (MD). Characteristics are an intermediate level of osteotomy, varus, neutral or valgus alignment, implant shoulder same-level to the fossa piriformis and area loading at the distal lateral cortex. In most cases, a standard offset version is sufficient in reconstructing the lateral femoral offset. In this category, Dorr type A and B are suitable (Figure 3(b)).
Type III (D): diaphyseal anchorage
In type III category, a large diaphyseal fixation is accomplished (D). This may be considered the “mid-size stem philosophy”. Characteristics are a low level of osteotomy, neutral or valgus alignment, implant shoulder inferior to the fossa piriformis and fit-and-fill in the proximal diaphysis. In most cases, a lateralised offset version is needed to reconstruct the lateral femoral offset. In cases of reduced bone quality this philosophy may be pursued (Figure 3(c)).
Type IV (C): cemented fixation
In type IV category, cemented fixation is accomplished. Cementation may be done in line-to-line technique. Predominantly, the “mid-size philosophy” should be pursued. Predominantly, indications are age >75 years and Dorr type B or Dorr type C. To date, cemented calcar-guided short stems are available only with a lateralised offset version (Figure 3(d)).
Indication recommendations and guidelines
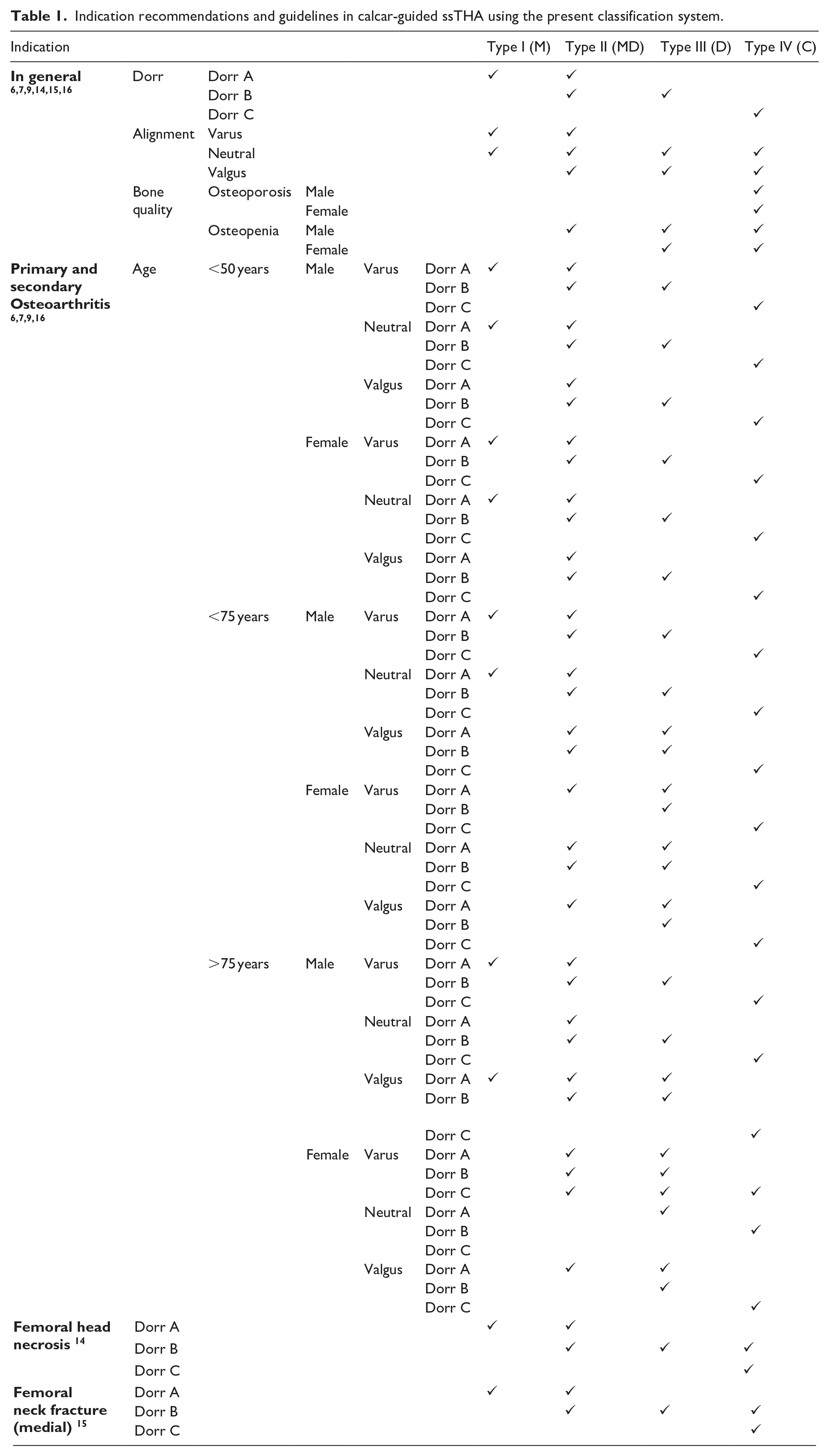
According to the present classification system, different indications for calcar-guided ssTHA can be assigned to the various types of fixation strategies.Table 1 contains recommendations based on current literature and may serve as indication guidelines.
Indication recommendations and guidelines in calcar-guided ssTHA using the present classification system.
Case presentations
Case 1
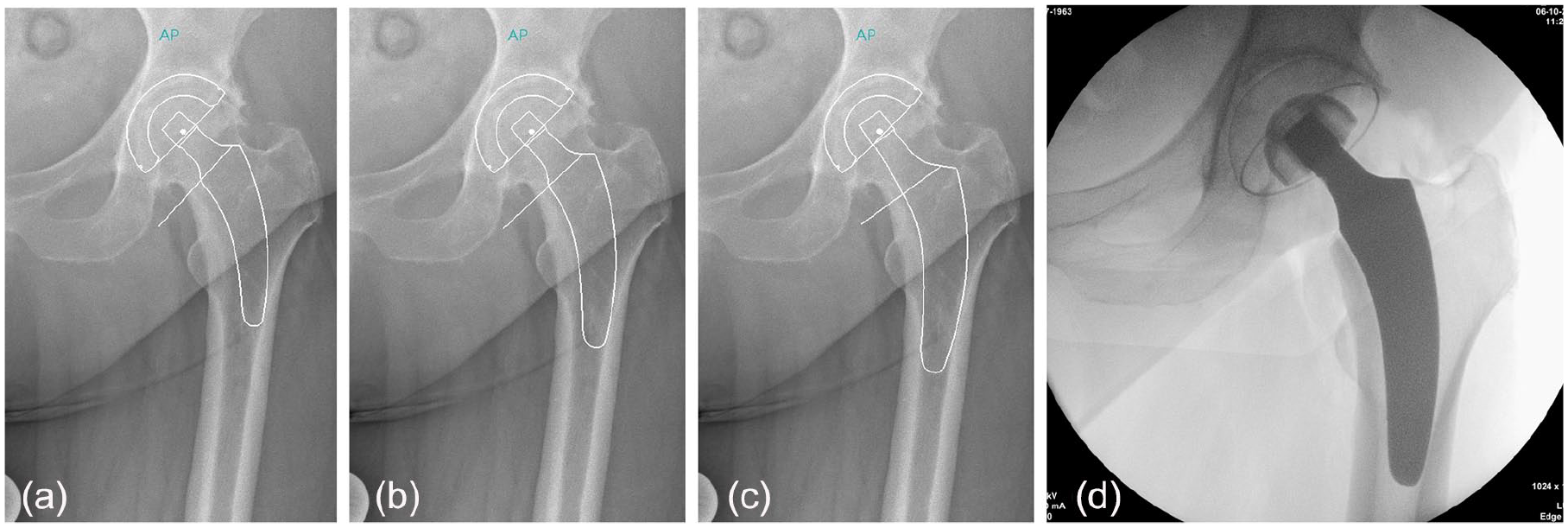
A 62-year-old man with a 3-year history of left hip pain presented for total hip arthroplasty. On examination he was found to have a significant reduction of range of motion and x-ray revealed pronounced arthritis of the left hip. The bone quality was rated very good according to the x-ray and the femur was classified Dorr type A. Provided a CCD-angle of 123°, the femur showed a varus alignment (group A according to Kutzner et al. 6 ). Preoperative templating was performed using various options. The strategies were classified according to the introduced classification system. A type I (M) fixation was predefined and implemented intraoperatively. Intraoperative radiography confirmed the result (Figure 4(a–d).
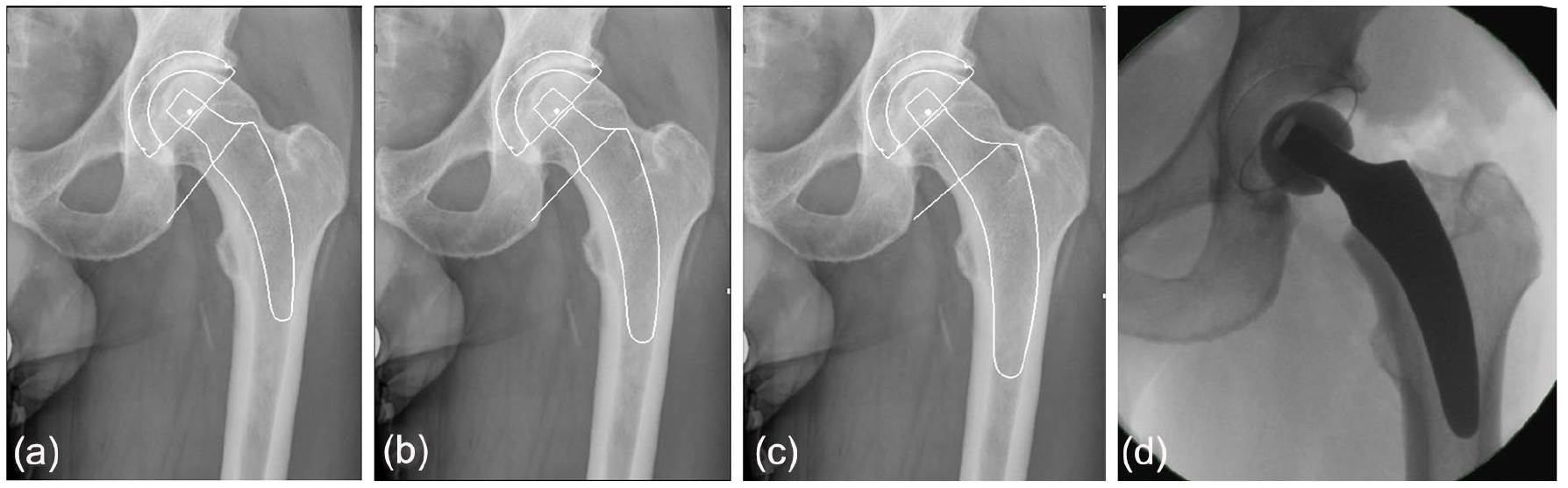
Case of a 62-year-old man with left hip pain (a–c) Preoperative templating of different fixation strategies according to the present classification (d) Intraoperative radiograph shows a type I (M) procedure).
Case 2
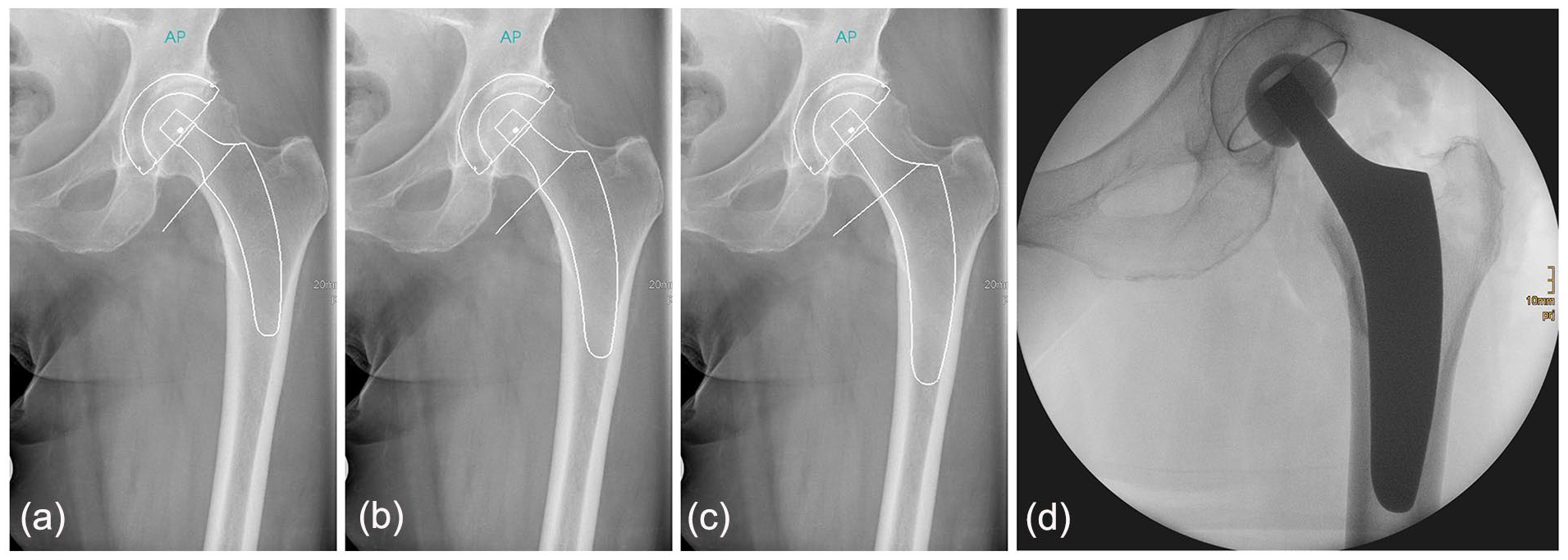
A 74-year-old woman with a 4-year history of left hip pain presented for total hip arthroplasty. On examination she was found to have a significant reduction of range of motion and x-ray revealed pronounced arthritis of the left hip. The bone quality was rated good according to the x-ray and the femur was classified Dorr type A. Provided a CCD-angle of 132°, the femur showed a neutral alignment (group C according to Kutzner et al. 6 ). Preoperative templating was performed using various options. The strategies were classified according to the introduced classification system. A type II (MD) fixation was predefined and implemented intraoperatively. Intraoperative radiography confirmed the result (Figure 5(a–d)).
Case of a 74-year-old woman with left hip pain (a–c) Preoperative templating of different fixation strategies according to the present classification (d) Intraoperative radiograph shows a type II (MD) procedure.
Case 3
An 88-years-old woman with a 12-year history of left hip pain presented for total hip arthroplasty. On examination she was found to have a significant reduction of range of motion and x-ray revealed pronounced arthritis of the left hip. The bone quality was reduced, a preoperative DXA analysis resulted in a femoral T-score of – 1,9. The femur was classified Dorr type B. Provided a CCD-angle of 126°, the femur showed a varus alignment (group B according to Kutzner et al. 6 ). Preoperative templating was performed using various options. The strategies were classified according to the introduced classification system. A type III (D) fixation was predefined and implemented intraoperatively. Intraoperative radiography confirmed the result (Figure 6(a–d)).
Case of an 88-year-old woman with left hip pain (a–c) Preoperative templating of different fixation strategies according to the present classification (d) intraoperative radiograph shows a type III (D) procedure.
Discussion
The design features of calcar-guided short stems, including the ability to apply individualised meta-diaphyseal anchorages, may account for advantages of this stem type compared with earlier short-stem designs in terms of indications for use, including reduced quality of bone, osteonecrosis of the femoral head (ONFH), and femoral neck fractures.14,15 In those cases, a diaphyseal fixation can be pursued. However, when operating on young patients with sufficient bone quality, a metaphyseal anchorage should be aimed for, in order to achieve the best result for the patient in the long-term. The present classification system provides a method of differentiation and should be used in the determination of the individually intended alignment and fixation.
A recent dual-energy x-ray absorptiometry (DEXA) study reported by Hochreiter et al. 17 evaluated bone remodeling around the calcar-guided optimys stem. Bone mineral density increased primarily in the lateral region (Gruen zones 2 and 3) and the distal-medial region (Gruen zone 5), suggesting lateral loading. Thus, stress-shielding was limited, and periprosthetic bone loss was minimised when using this stem design.
However, it is to be expected that the application of diaphyseal anchorage, also for this stem design, will compromise the positive effects on stress-shielding. Thus, it should be avoided and a metaphyseal anchorage should be pursued in those cases where possible.
Studies investigating the migration patterns of modern short stems using EBRA-FCA (Ein-Bild-Roentgen-Analyse; femoral component analysis) have suggested an initial, pronounced settlement into the metaphyseal bone upon the initiation of full weight-bearing, followed by a subsequent stabilisation.16 –20 In a recent investigation, most of the investigated stems showed delayed settlement during the first 2 years after surgery, suggesting that these new-generation stems are likely to display different migration patterns from conventional stems. 7 Male patients and heavy-weight patients have been shown to be at higher risk of subsidence, as are stems with valgus alignment.6,16
A securely achieved cortical contact with the distal lateral cortex appears to be crucial to provide sufficient primary stability. 10 The use of intraoperative imaging to identify the potential “undersizing” of calcar-guided short stems is highly recommended, especially with regard to individualised positioning.1,11
Cemented ssTHA may represent a potential alternative for patients with poor bone quality, such as Dorr type C femora. Recently, one of the new-generation short stems emerged on the market with cemented fixation. Additionally, using prototypes of the optimys stem fabricated using polished steel, recent in vitro biomechanical studies demonstrated that cemented short stems are a promising alternative for use in osteoporotic bone and may, therefore, further expand the range of indications in the future. 8
Conclusion
The individualised implantation technique requires distinct knowledge of the characteristics associated with different types of anchoring, resulting in a significant learning curve for surgeons new to this technique. In sufficient bone quality the short-stem philosophy with metaphyseal anchorage (type I (M) and type II (MD) should be pursued. Range of indications can be extended by applying diaphyseal anchorage. Contraindications for the cementless use of these implants should be respected. Improving education and collecting further clinical evidence will be crucial determinants of a successful future of calcar-guided ssTHA.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KPK: medical advisor for Mathys Ltd. No further conflicts of interest have been declared.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.