
Abstract
Background:
Although several reports have examined the association between preoperative function and postoperative outcomes in patients undergoing total hip arthroplasty (THA), it is unclear whether the ability of the affected or non-affected side particularly impacts on outcomes. We aimed to investigate the association between affected and non-affected side ability and walking independence.
Methods:
We prospectively enrolled 721 consecutive patients who underwent THA. Preoperatively, quadriceps isometric strength (QIS) and one-leg standing time (OLST) were measured. The endpoints were walking independence within 3, 5, 7, 10, and 14 days postoperatively. The associations between preoperative abilities and outcomes were examined using multivariate Cox hazard model, and the area under the curves (AUCs) for outcomes were compared.
Results:
We analysed 540 patients after excluding patients who met the exclusion criteria. Both affected and non-affected QIS predicted walking independence within 3 (p = 0.006 and 0.001, respectively), 5, 7, 10, and 14 (both p < 0.001) days postoperatively. For OLST, only the affected side did not predict walking independence within 3 days postoperatively (p = 0.154 and 0.012, respectively), and both sides did at days 5 (p = 0.019 and <0.001, respectively), 7, 10, and 14 (both p < 0.001). The AUCs of the non-affected side ability for walking independence were significantly greater than those of the affected side on postoperative days 3 (0.66 vs. 0.73; p = 0.021) and 5 (0.67 vs. 0.71; p = 0.040), with no significant difference after day 7.
Conclusions:
Both sides abilities were associated with walking independence after THA, but non-affected side was found to be particularly crucial for early walking independence.
Keywords
Introduction
Total hip arthroplasty (THA) reduces pain and improves the quality of life (QOL) of patients with hip diseases, including osteoarthritis (OA), 1 and physical function. 2 However, physical function recovery, including walking independence, is often delayed. Several factors lead to delayed physical function recovery.3–7 Walking ability and muscle strength are closely related, 8 and we reported the importance of preoperative quadriceps strength for early walking independence in older patients undergoing THA. 9 Furthermore, balance skills, including one-leg standing time (OLST), are known as good indicators of walking ability and are important for evaluating lower limb ability. 10 However, previous reports have not examined whether preoperative affected side or non-affected side performance was more important for postoperative walking ability. Only Ohmori et al. 11 reported that preoperative non-affected side ability affected walking speed 1 year after THA, but it is unclear whether non-affected side ability is also important in early postoperative walking independence. The knowledge of which side function is more important for early postoperative walking independence has been shown to be important for planning pre- and postoperative management and rehabilitation in our institution.5,7,9,12 Therefore, we hypothesised that the preoperative non-affected lower limb performance is also important for early postoperative gait independence, and the purpose of this study was to determine the impact of both lower limbs’ abilities on postoperative walking independence. We further examined the differences in effects on walking independence between both the sides.
Methods
Study population
We prospectively analysed an initial population of 721 consecutive patients who underwent THA at our hospital between September 2018 and January 2022. The exclusion criteria were as follows: preoperative unable to walk >50 m continuously; revision THA; simultaneous bilateral surgery; and unexpected events (e.g., severe deep vein thrombosis, fracture, and infection) in the perioperative and postoperative periods. The study protocol was approved by the Ethics Committee of our hospital and performed in accordance with the Declaration of Helsinki. Informed consent was obtained from all the included participants.
Postoperative rehabilitation
All patients underwent acute rehabilitation supervised by physical therapists. On postoperative day 1, the patients were transferred to wheelchairs, and they started walking on postoperative day 2. Depending on the patients’ physical function, physical therapists determined the walking distance, walking aid use, and ability to walk independently. According to the postoperative clinical pathway in our hospital, sutures were removed on the 10th postoperative day and patients were discharged home on the 11th day if they were walking and climbing stairs independently at this point, but if they needed assistance with these activities, they were transferred to a rehabilitation facility.5,7
Data collection
Patient characteristics, including age, sex, body mass index (BMI), comorbidities, American Society of Anesthesiologists physical status (ASA-PS) score, 13 and controlling nutritional status (CONUT) score, 14 were obtained from electronic medical records within 2 weeks of admission for surgery. We also assessed hip pain at rest and during walking using the visual analogue scale (VAS). 15 Additionally, the number of days taken to achieve walking independence was followed up for a maximum of 14 postoperative days.
Preoperative affected and non-affected lower limb ability
For affected and non-affected side lower limb function, we measured quadriceps isometric strength (QIS) and OLST for both the sides. The QIS was measured using a handheld dynamometer (μ-Tas; ANIMA, Tokyo, Japan) fixed to a rigid bar. With the patient sitting on a bench, 5-s maximal isometric voluntary contractions of the quadriceps were recorded 3times successively for both legs, with the knee joints fixed at 90° flexion and hip joints at approximately 90° flexion. 16 The pressure sensor’s lower end was placed on the 2 lateral fingers from the lateral malleolus and installed on the front of the lower thigh. The right and left quadriceps were consecutively tested. The greatest strength values on the both sides were expressed as absolute values (kg) and percentage body mass (%BM). 17
In the assessment of OLST, the patients wore their shoes and were required to stand on 1 leg for up to 30 seconds with the hands placed on the hips and the eyes open. The floor was smooth and level, and the room was well-lit. A digital stopwatch was used to determine OLST and was stopped if the patients made contact with any part of the room with any part of the body other than the supporting foot, began to hop around, or moved their hand off the hip. The patients performed the test twice for both the affected and non-affected sides, and the best time obtained in the 2 trials was recorded.
We assessed these lower limb functions as part of routine clinical practice in an outpatient setting within 2 weeks of admission.
Outcome
The primary outcome of the study was walking independence after THA. The number of days to walking independence was set at 5 points: within 3, 5, 7, 10 and 14 days after surgery. The definition of walking independence was defined as the ability to walk 50 m without assistance regardless of the use of walking aids, based on the FIM definition.18,19
Treatment of missing data
Missing-data proportions for all variables were as follows: the affected side’s visual analogue scale (VAS) score at rest (1.1%), affected side’s VAS score during walking (1.1%), non-affected side’s VAS score at rest (1.1%), and non-affected side’s VAS score during walking (1.1%).
Assuming that the analysed data were missing at random, we performed multiple imputations using the chained equations method, with linear regression performed for all missing data. The imputation used all the analytic models’ variables. The results from 20 imputed datasets were combined for analysis using Rubin’s formula. 20
Statistical analyses
Continuous-variable results were expressed as median values (interquartile range [IQR]). Categorical variables were expressed as numbers and percentages.
Operative and nonoperative QIS and OLST cut-off values for walking independence at each time point were calculated using receiver operating characteristic (ROC) curves and the Youden index. To examine the association between preoperative both side lower limbs’ abilities and independent walking within 3, 5, 7, 10, and 14 days after THA, the subjects were divided into 4 groups according to the cut-off values of QIS and OLST for each lower limb, and we used the Kaplan-Meier method with the log-rank test. Additionally, we estimated the hazard ratio (HR) of independent walking and its 95% confidence interval (CI) using Cox proportional hazard model for each lower limb, adjusting for age, sex, BMI, preoperative hip-pain VAS score, ASA-PS, previous THA on non-affected side, and controlling nutritional status (CONUT) score. Moreover, to address selection bias because of a history of non-affected side surgery, we performed a sensitivity analysis with multiple imputations except for patients with a history of non-affected side surgery.
Furthermore, to compare the effect of affected and non-affected ability on postoperative walking independence, we constructed a logistic model for walking independence at each postoperative day using affected side ability and non-affected side ability. ROC curves were constructed using these models and compared the area under the curves (AUCs) according to the method developed by DeLong et al. 21
Analyses were performed using Stata (version 15.0; StataCorp LP, College Station, TX, USA), and R (version 2.7-1; R Foundation for Statistical Computing, Vienna, Austria). In all analyses, a 2-tailed p < 0.05, was considered statistically significant.
Results
Study population
A consort diagram of the subjects is shown in Figure 1. After excluding patients who were unable to walk before surgery (n = 36), had undergone revision THA (n = 63) or simultaneous bilateral surgery (n = 65), and experienced unexpected events during hospitalisation (n = 17), 540 patients were included in this study. Table 1 shows the patients’ baseline characteristics. The patients’ median age was 65.5 years, and 80% were women. The median preoperative QIS of affected and non-affected side were 29.1% BM and 35% BM, and preoperative OLST was 15.5 sec and 30.0 sec, respectively.
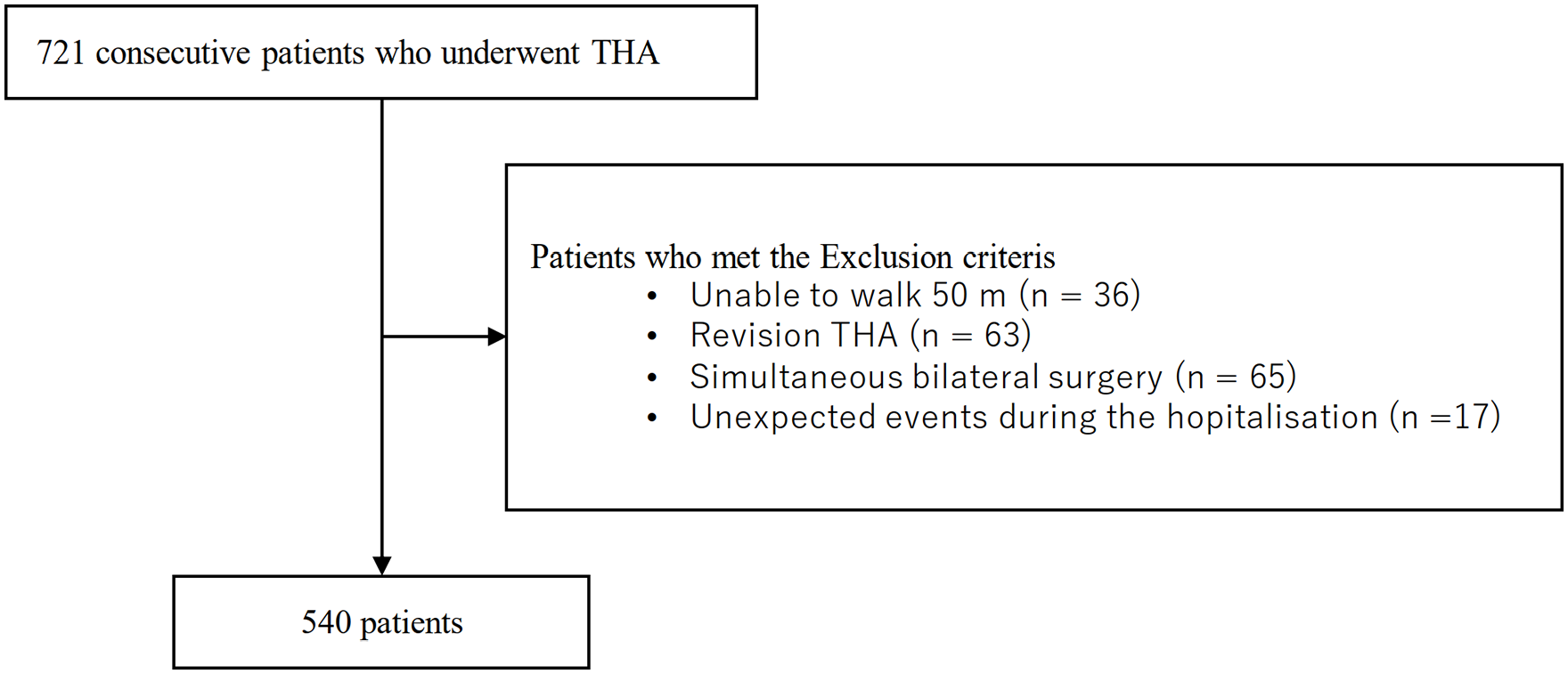
Consort diagram of the subject.
Patients’ characteristics.
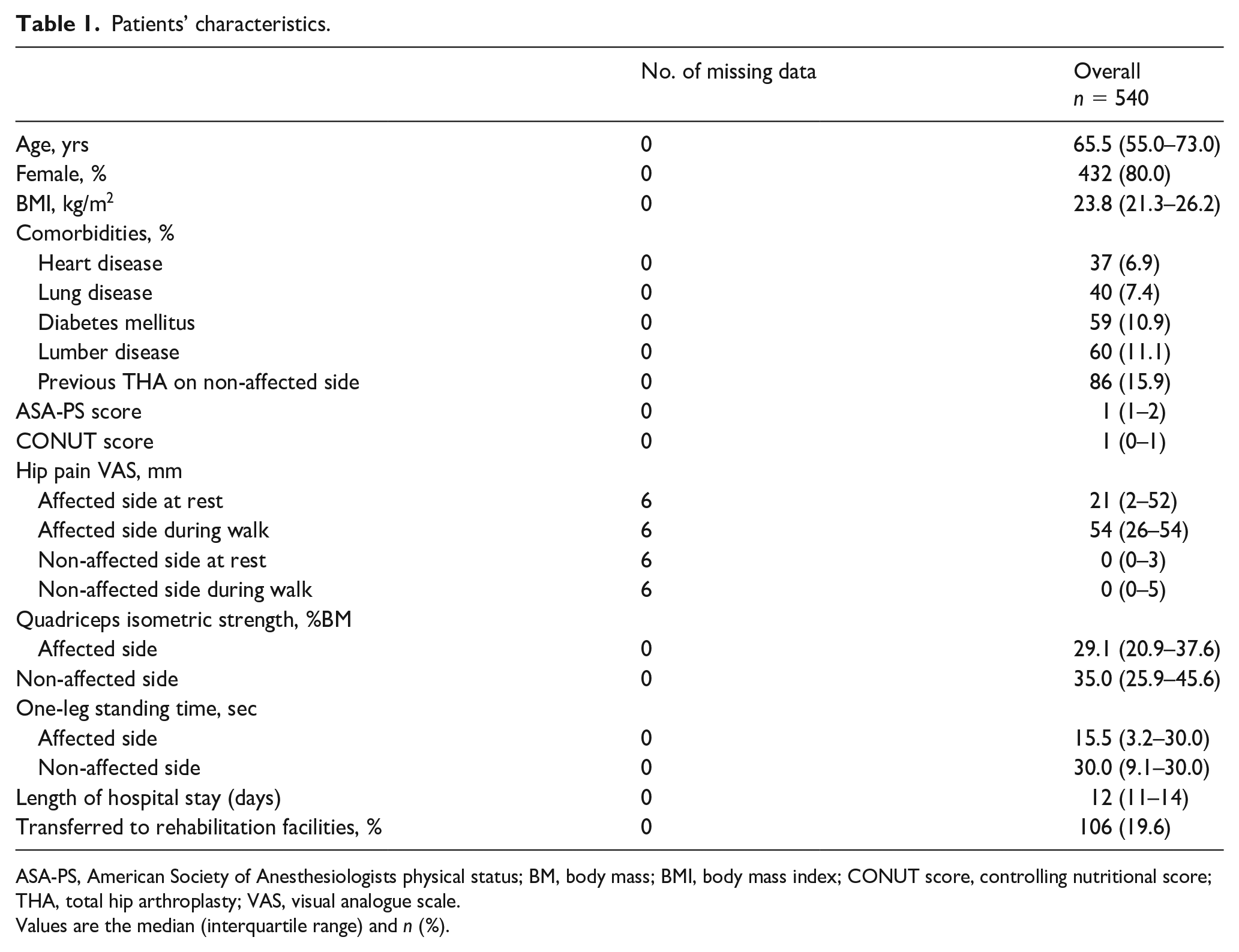
ASA-PS, American Society of Anesthesiologists physical status; BM, body mass; BMI, body mass index; CONUT score, controlling nutritional score; THA, total hip arthroplasty; VAS, visual analogue scale.
Values are the median (interquartile range) and n (%).
Cut-off values of QIS and OLST for walking independence
Cut-off values for walking independence within 3, 5, 7, 10, and 14 days postoperatively are shown in Table 2. Regarding QIS, the required strength was slightly lower on the affected side than on the non-affected side for all postoperative days. Additionally, the preoperative QIS requirements decreased as more days passed since surgery. The time required to perform OLST was also less on the non-affected side than on the affected side. Additionally, the more days passed since surgery, the shorter the OLST cut-off value for walking independence was observed.
Cut-off values of affected and non-affected side abilities for walking independence within 3, 5, 7, 10, and 14 days postoperative.
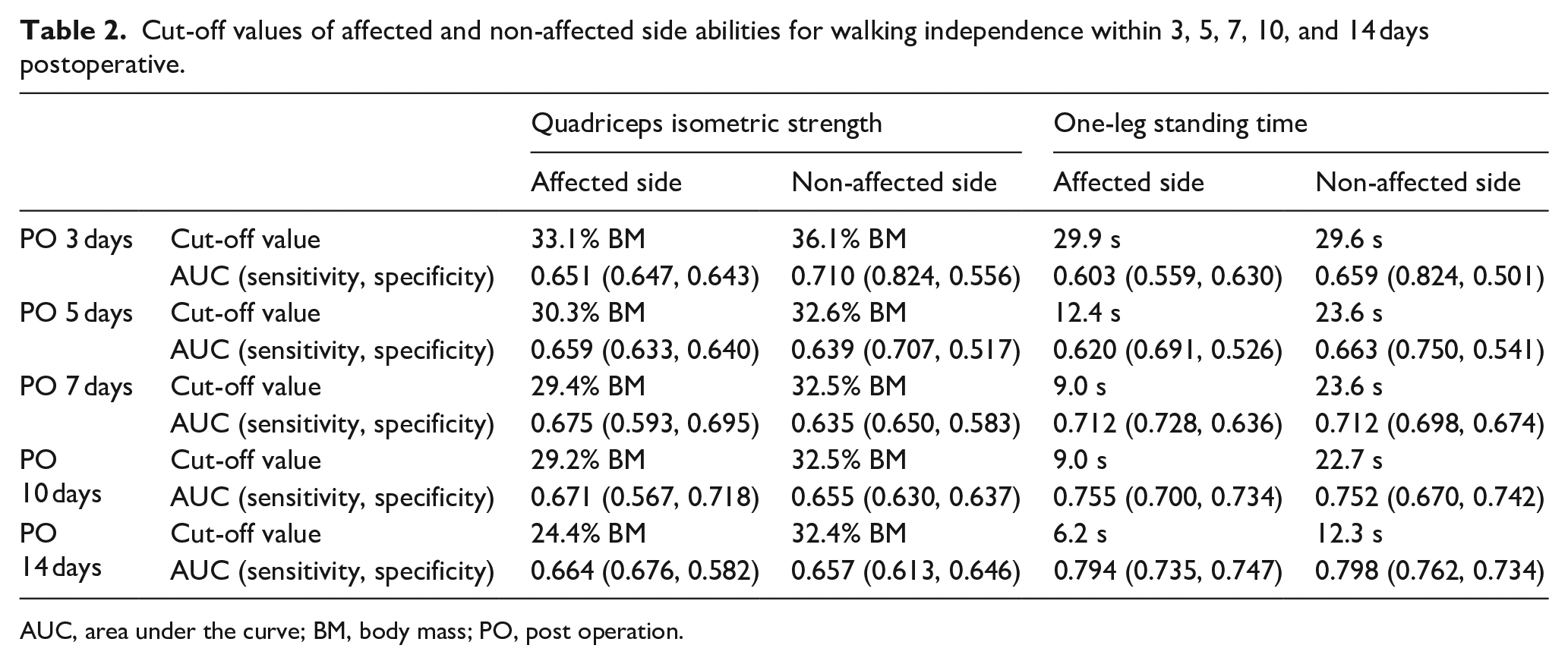
AUC, area under the curve; BM, body mass; PO, post operation.
Association between both side ability and walking independence
Of all subjects, 34 (6.3%), 191 (35.4%), 342 (63.3%), 408 (75.6%), and 453 (83.9%) patients achieved walking independence within 3, 5, 7, 10, and 14 days after surgery, respectively. The Kaplan-Meier survival curve followed by the log-rank test is shown in Figure 2. The results indicated that significantly lower rate of patients achieved walking independence when either 1 or both of QIS and OLST were below the cut-off values compared to patients with both above the cut-off values on both the affected and non-affected sides (all p < 0.001, respectively). Table 3 shows the hazard ratio for walking independence within 3, 5, 7, 10, and 14 days postoperatively. Although no significant association between OLST of affected side and walking independence within 3 days postoperatively (p = 0.154) was observed, QIS and OLST predicted the walking independence in each postoperative day on both the affected and non-affected sides (all p < 0.05). Additionally, sensitivity analysis, excluding patients with a history of THA on the nonoperative side, did not noticeably affect the estimated association between the ability of both sides and postoperative walking independence (Supplemental Table 1).
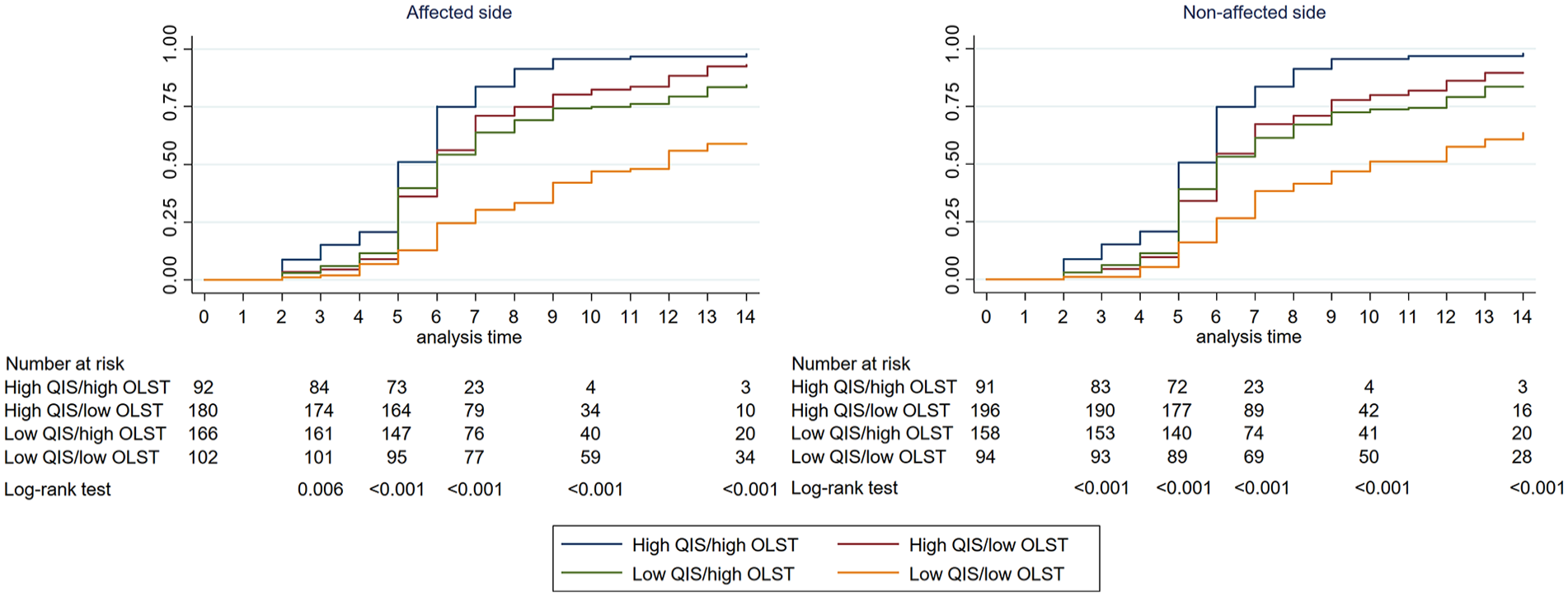
Kaplan–Meier curve for walking independence according to affected and non-affected side abilities.
Results of the Poisson regression models with robust estimators for walking independence at each time point.
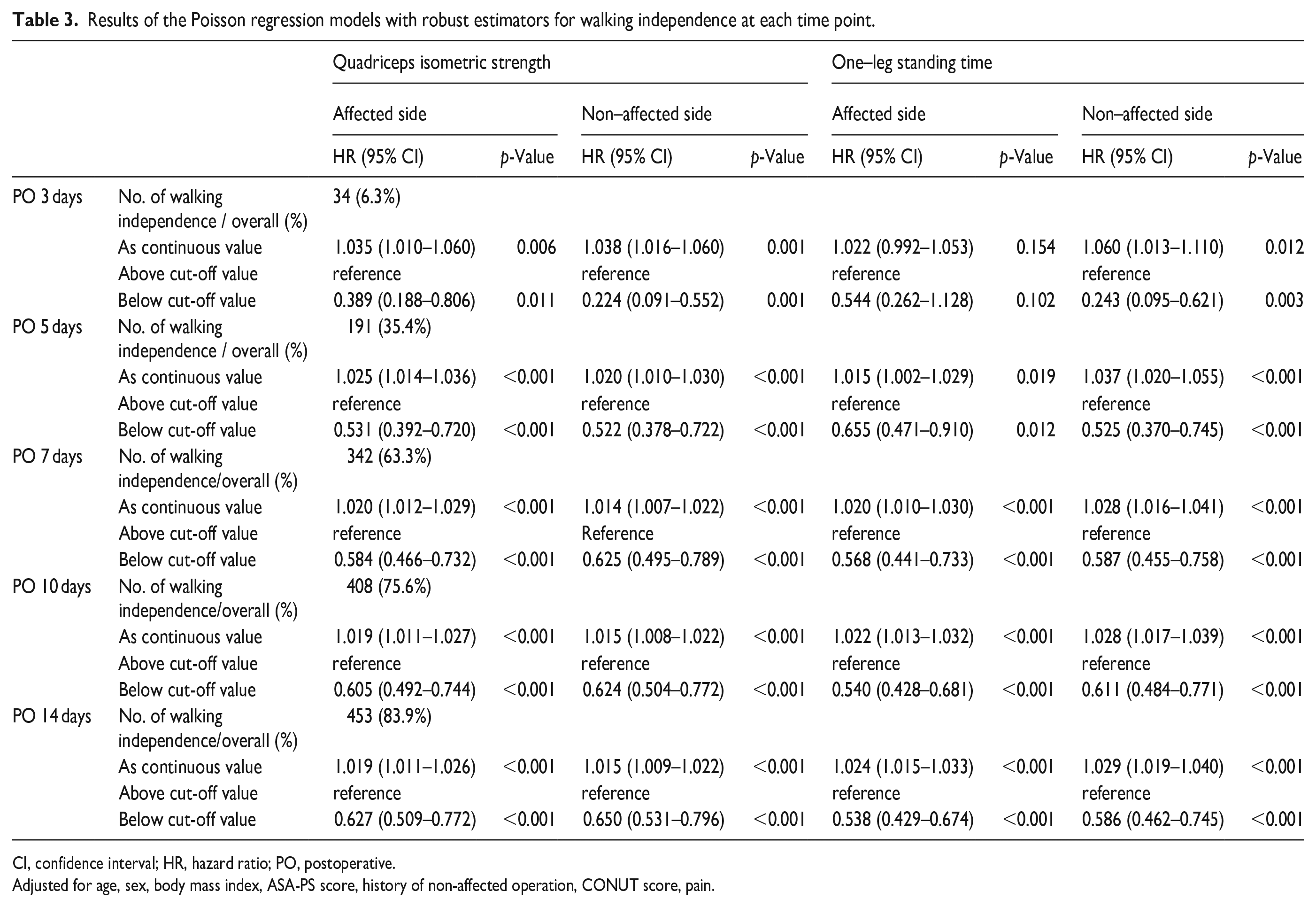
CI, confidence interval; HR, hazard ratio; PO, postoperative.
Adjusted for age, sex, body mass index, ASA-PS score, history of non-affected operation, CONUT score, pain.
Comparison of AUCs of affected and non-affected side ability for walking independence
The AUCs of affected and non-affected side ability for walking independence were shown in Table 4. The AUCs of the non-affected side ability for walking independence were significantly greater than those of the affected side on postoperative days 3 (p = 0.021) and 5 (p = 0.040), with no significant difference after day 7.
Comparison of AUCs of affected and non-affected side ability for walking independence.
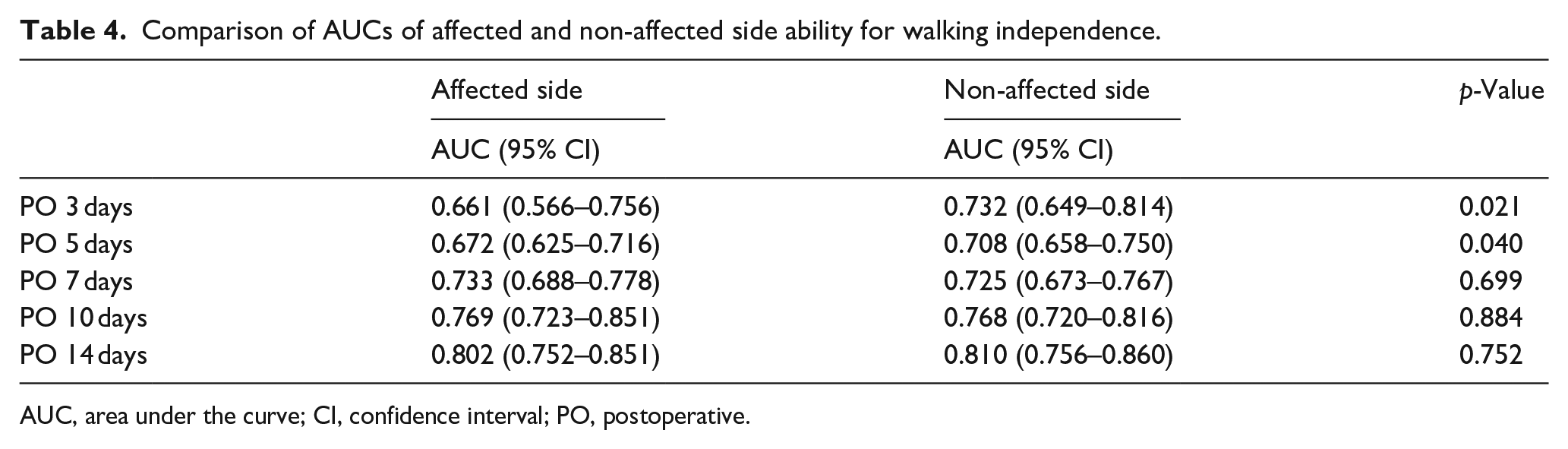
AUC, area under the curve; CI, confidence interval; PO, postoperative.
Discussion
This is the first report to investigate the association of preoperative affected and non-affected side abilities with walking independence after THA. Our study’s primary findings were as follows: (1) the cut-off values for postoperative walking independence were lower on the affected side than non-affected side, and decreased as the number of days since surgery passed; (2) high preoperative QIS and OLST, on both the affected and non-affected sides, were associated with the achievement of postoperative gait independence; (3) non-affected side ability was more important than affected side ability for walking independence within 3 and 5 days postoperatively, but there was no difference between both the limbs in terms of impact on walking independence at 7, 10, and 14 days. These results suggest the importance of a careful preoperative assessment of the abilities of both the lower limbs for postoperative risk stratification.
Previous studies examined the postoperative physical function prediction using preoperative information. In these reports, older age, female sex, and poor nutritional status delayed postoperative physical function.3,5,22 Rega-rding physical abilities, the preoperative timed up and go (TUG) test and walking speed are reportedly associated with postoperative function.6,7 Although this is a useful information, other predictors are necessary because patients with osteoarthritis experience more pain when walking and have a higher fall risk.23,24 We recently reported that pre-THA summary muscle weakness is associated with postoperative walking independence. 9 However, muscle strength is defined as the average of both the lower limbs, and the relationship between affected and non-affected side abilities independently as well as walking independence for preoperative management and postoperative planning may be known. Additionally, QIS and OLST have the advantage that these can be measured in a small office space, in fact, have proven to be simple to measure from our reports. 25 Therefore, these tests are highly applicable and easily usable in our daily clinical practice.
In a report focusing on affected and non-affected side function in patients undergoing THA, Ohmori et al. 11 investigated the association between preoperative ability and walking speed 1 year after the surgery. They concluded that non-affected side ability was associated with favourable gait speed 1 year postoperatively, whereas affected side ability showed no significant association. Our results showed that the non-affected side had better predictive ability up to the postoperative day 5, but similarly predicted walking independence after the postoperative day 7. Their findings on the importance of non-affected side ability differ slightly from ours, possibly because we did not define walking speed as a measure of walking independence and focused on walking ability in the early postoperative phase.
The present study showed that preoperative non-affected side ability is important for walking independence, especially as early as within 5 days postoperatively, according to the results of AUCs. This may be because the importance of preoperative ability is relatively low because of the surgical wound pain and psychologic reasons, including confused body image.26,27 Which limits the performance of operative side in the early postoperative phase. 28 It is likely that these improvements and postoperative factors such as rehabilitation are related to the disappearance of the difference between the two groups in the predictive ability of walking independence after 7 days;29,30 however, the mechanism cannot be clarified in this study. Nevertheless, it should be noted that the number of patients who achieved walking independence within 3 or 5 days postoperatively was small and might not be statistically significant. This may be because the walking-independence criterion was set at 50 m, which is a slightly longer distance. Also, in our postoperative path, most patients were hospitalised for >10 days. In fact, only 6.3% of patients were able to walk independently 3 days postoperatively. However, according to a meta-analysis by Zhu et al., 31 , the average post-THA length of hospital stay is 2–13 days, and other reports have demonstrated that predicting walking independence at and within 5 days postoperatively is important in shortening hospital stay.7,32 Furthermore, the addition of non-affected side ability to the models for predicting walking independence including affected side ability at all postoperative phases improved predictive capability, and therefore, preoperative evaluation of non-affected side ability is necessary and valuable in the clinical practice.
Our results showed that 80% of all subjects were women, a higher proportion than in many previous studies, and a lower BMI of 23.8. As for the high number of women, it may be partly due to the high number of Asians with congenital dysplasia of the acetabulum. 33 Particularly in Japan, it has been reported that many patients have acetabular dysplasia, suggesting a possible transition to hip osteoarthritis. 34 Indeed, our results are similar to the gender ratios of reports performed using national data in Japan. 35 Regarding BMI, it has been shown that BMI is lower in Asians compared to Europeans and Americans living in the community and those with various diseases. In fact, most data from Asia, including Japan, report a BMI around 22–25 kg/m2,36–38 and our data are in this range. Considering sex ratio and BMI specificity, it may not be certain whether our results apply to Westerners as well. In addition, among the complications, lumbar spine disease was more common in patients in the study. Although it has been reported that patients with hip disease can develop lumbar spine disease, 39 in our study, patients with preoperative inability to walk >50 m were excluded, and it is unlikely that walking independence was delayed due to symptoms caused by lumbar spine disease, such as paralysis or intermittent claudication.
To our knowledge, this study is 1 of the few epidemiologic studies to focus on affected and non-affected side ability and investigate its association with postoperative walking independence. The results of the present study have important public health implications and may be particularly useful for preoperative risk stratification and postoperative management planning. A major strength of our prospective observational study is the study design and that we were able to include consecutive cases, which reduced selection bias. Additionally, although pre-THA rehabilitation effects have been controversial,40–44 our results suggest that exercise therapy for the nonoperative side may hasten postoperative functional recovery.
The present study had certain limitations. First, this single-centre study incorporated a small sample size. In addition, the study was validated only in Japan, and it is unknown whether the results of the study can be referred to clinical practice when postoperative hospital stays are shorter and postoperative clinical pathways are different. A multicentre, multinational cohort would have the potential to validate the findings of the present study. In particular, cut-off values would be more accurate if calculated for each of the various subgroups with increased number of subjects. Second, indicators associated with postoperative functional recovery were not included, such as TUG and cognitive function.45,46 Therefore, it is necessary to assess whether non-affected side ability could be useful for early walking independence after surgery even after adjusting for these values. Finally, the definition of walking independence is defined as only being able to walk 50 metres unaided with or without the use of a walking aid. Because it is considered possible to live without the ability to walk 50 m depending on the situation, further research using different criteria or activities of daily living battery such as the Barthel Index as an outcome would be clinically meaningful. 47
In conclusion, both side abilities were associated with walking independence after THA, but non-affected side was found to be particularly crucial for early walking independence. Our results suggest that assessing preoperatively non-affected side ability may be of interest with respect to postoperative risk stratification.
Supplemental Material
sj-pdf-1-hpi-10.1177_11207000231199169 – Supplemental material for Association of affected and non-affected side ability with postoperative outcomes in patients undergoing total hip arthroplasty
Supplemental material, sj-pdf-1-hpi-10.1177_11207000231199169 for Association of affected and non-affected side ability with postoperative outcomes in patients undergoing total hip arthroplasty by Kohei Nozaki, Yuta Nanri, Masashi Kawabata, Manaka Shibuya, Manami Nihei, Takehiro Shirota, Hiroyoshi Masuma, Takuya Maeda, Kensuke Fukushima, Katsufumi Uchiyama, Naonobu Takahira and Masashi Takaso in HIP International
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.