
Abstract
Autosomal dominant osteopetrosis (ADOP) is an extremely rare congenital bone disease. We report a case of a hip disorder in combination with ADOP, which was treated by total hip arthroplasty, resulting in a good recovery and a significant improvement in the patient’s ability to perform daily activities.
Keywords
Introduction
Autosomal dominant osteopetrosis (ADOP) is a rare metabolic bone disease characterized by a deficiency or functional defect in osteoclasts, which results in higher bone density and a narrowing of the bone marrow cavity. 1 Bone density abnormalities in patients with ADOP greatly increase the risks of bone fragility and fracture. 2 In addition, such patients often have comorbidities, such as hip inversion, long bone flexion deformity, osteomyelitis, osteoarthritis and fracture non-union. 3
The incidence of hip disorders in combination with ADOP and severe hip osteoarthritis is extremely low, and patients are often treated by total hip replacement. 4 Anatomical abnormalities of the hip joint in such patients render the implantation of surgical prostheses very difficult, which affects the postoperative outcomes and leads to a high incidence of complications. 5 Therefore, total hip arthroplasty in this group of patients requires a high level of operator skill. In this paper, we report the case of a patient with a hip disorder in combination with ADOP who was treated by total hip arthroplasty using a posterior-lateral approach, which was associated with good clinical results.
Case report
The patient was a 16-year-old woman who had been experiencing left hip pain for more than 1 year. The Institutional Review Board of the Ethics Committee requires investigators to seek patient consent to publish case reports, but does not require a full review or approval by the committee. Verbal consent was obtained from the patient through telephone interviews during the investigation and reporting of the case, and all the necessary patient information was collected and anonymized. We have obtained the written informed consent of the patient for publication. The reporting of this study conforms to the CARE guidelines. 6
Family history
The patient’s maternal grandmother also had ADOP.
Specialized examination
On physical examination, the patient was found to have a pronounced limp, with a lean to the left. She was 163 cm tall and had a body mass of 75 kg. Her left lower extremity was ∼6 cm shorter that her right lower extremity; and the mobility of her left hip joint was low, showing 90° forward flexion, 0° posterior extension, 10° adduction and 10° abduction.
Laboratory results
The serum concentrations of relevant substances were as follows: parathyroid hormone (PTH), 6.549 pmol/L (normal range 1.144–10.731 pmol/L); 25-hydroxy-vitamin D (25-OH Vit D), 37.69 nmol/L (normal range 74.9–249.6 nmol/L); beta-C-terminal telopeptide (β-CTX), 0.486 ng/mL (normal range 0.068–0.68 ng/mL); total procollagen type N-terminal propeptide (tPINP) 167.5 ng/mL (normal range 8.53–64.32 ng/mL).
Preoperative imaging
Hip radiographs and computed tomography showed bilateral high bone densities of the femoral heads and acetabula, and the medullary cavities were narrowed or absent. The left femoral head was flattened, the left hip joint space was narrowed, the pelvis was tilted, and the lower limbs were asymmetrical. Radiographs of the spine and upper extremities showed non-structural scoliosis (bending film <25°), thickened and dense upper and lower endplates, a loose and radiolucent mid-vertebral body, “sandwich cake-like” changes in the vertebral body, bilateral humeral cortical thickening and medullary stenosis (Figure 1). Magnetic resonance imaging of the hip joints showed bilateral osteosclerosis deep to the femoral head and acetabular joint surface, bilateral local defects of the left femoral head and narrowing of the left hip joint space. The bone mineral density (BMD) of the patient was high (left hip: neck Z = −9.8, shaft = −6.5, total = −8.5; neck BMD = 1.912, shaft = 1.965, total =1.878). Therefore, the patient was diagnosed with a hip disorder in combination with ADOP.

Preoperative images of the patient. (a) Pelvic X-ray, showing high density of the iliac and femoral bones, a pelvic tilt, a “ring-like” change on the iliac wing, flattening of the left femoral head, narrowing of the left hip joint space and stenosis of the femoral medullary cavity. (b) Hip CT, showing narrowing or absence of the medullary category. (c) Spinal X-rays, showing thickening and high density of the upper and lower endplates, laxity and central radiolucency of the vertebrae and a “sandwich cake” appearance of the vertebral bodies and (d) X-ray of the upper extremity, showing cortical thickening of the humerus and narrowing of the medullary cavity.
We obtained the patient’s consent for treatment. Pre-operative X-rays were used to develop a complete acetabular and femoral reconstruction plan.
We chose a biologic ceramic total hip prosthesis (Tri-Lock COC, DePuy Synthes, Raynham, MA, USA) and prepared the S-ROM prosthesis (DePuy Synthes Joint Reconstruction, Warsaw, IN, USA) to cope with the extremely narrow medullary cavity. After inducing satisfactory anesthesia, the patient was placed in the right lateral position, her skin was routinely disinfected with iodine and alcohol, and then a sterile sheet was placed and the surgical procedure was performed via a posterior lateral approach. Intraoperatively, the femoral head was found to be deformed, the articular cartilage was worn or absent, the bone was hard, and the acetabulum was severely ossified (Figure 2). After dislocation of the hip, the hard femoral head was removed, the acetabulum was revealed, the acetabular labrum was removed, and the remaining femoral ligamentous tissue in the acetabular fossa was removed to reveal the transverse acetabular ligament at the inferior border of the acetabulum. The acetabular component was inserted at an angle of 45° relative to the sagittal pelvic plane, and the plane of the transverse acetabular ligament was used for cup anteversion. The acetabulum was widened and deepened using an acetabular file, with an anteversion angle of 15°. The severe ossification of the acetabulum made the process of filing the socket extremely difficult. The reaming of the acetabulum was started directly medial to the floor, beginning with the use of a small reamer, followed by sequentially larger reamers, in the anticipated position of the implanted component. The anterior and posterior walls of the acetabulum were filed down to the subchondral bone, and the deepening was continued until the superficial surface of the internal pelvic cortex was reached. The acetabular prosthesis was placed after sufficient exudation had occurred. A 48-mm acetabular cup was placed that successfully covered 70% of the acetabular bone, and the acetabular prosthesis was completely and tightly fitted to the acetabular wall without the need for screw fixation.

Intraoperative condition of the patient. (a) Severe ossification of the acetabulum. (b) Deformation of the femoral head, wear-and-tear destruction of the articular cartilage and hardening of the bone and (c) Narrowing or absence of the femoral marrow cavity.
During the reconstruction of the femur, direct intraoperative inspection and intraoperative fluoroscopy revealed that the femoral medullary cavity was extremely narrow or even absent (Figure 2). Distal expansion was first performed using 1- to 4-mm Kirschner wires in sequence (Figure 3), and the file depth was determined using preoperative X-ray measurements and intraoperative trials. After widening the medullary cavity to the appropriate width using a solid drill, it was further widened to the appropriate size for the prosthetic stalk using a medullary expander, the stability of the prosthesis was checked, a trial mould and ball were placed and the left hip joint was repositioned. After intraoperative fluoroscopic examination, the prosthesis (a Tri-lock standard femoral stem, size 0, with a 32-mm ceramic ball head and a 48-mm acetabular cup with a pure titanium coating) was properly positioned (Figure 3).

Intraoperative fluoroscopic images of the patient. (a) Intraoperative fluoroscopy revealed an extremely narrow femoral medullary cavity, through which a Kirschner wire was passed to assist with dilation and (b) After intraoperative fluoroscopy, the prosthesis was properly positioned.
Routine postoperative prophylaxis against infection (cefazolin sodium 1 g, intravenous, four times daily for 24 hours) and lower-extremity deep-vein thrombosis (low molecular-weight heparin sodium, subcutaneous, 4250 μg daily, until discharge) were employed. On the second postoperative day, the patient performed active partial weight-bearing hip activities using crutches. Pathological examination showed that the left femoral head included a large amount of cartilage-like matrix and disorganized bone trabeculae, inter-trabecular fibrous tissue hyperplasia, a small bone marrow cavity and a lack of hematopoietic cells (Figure 4).
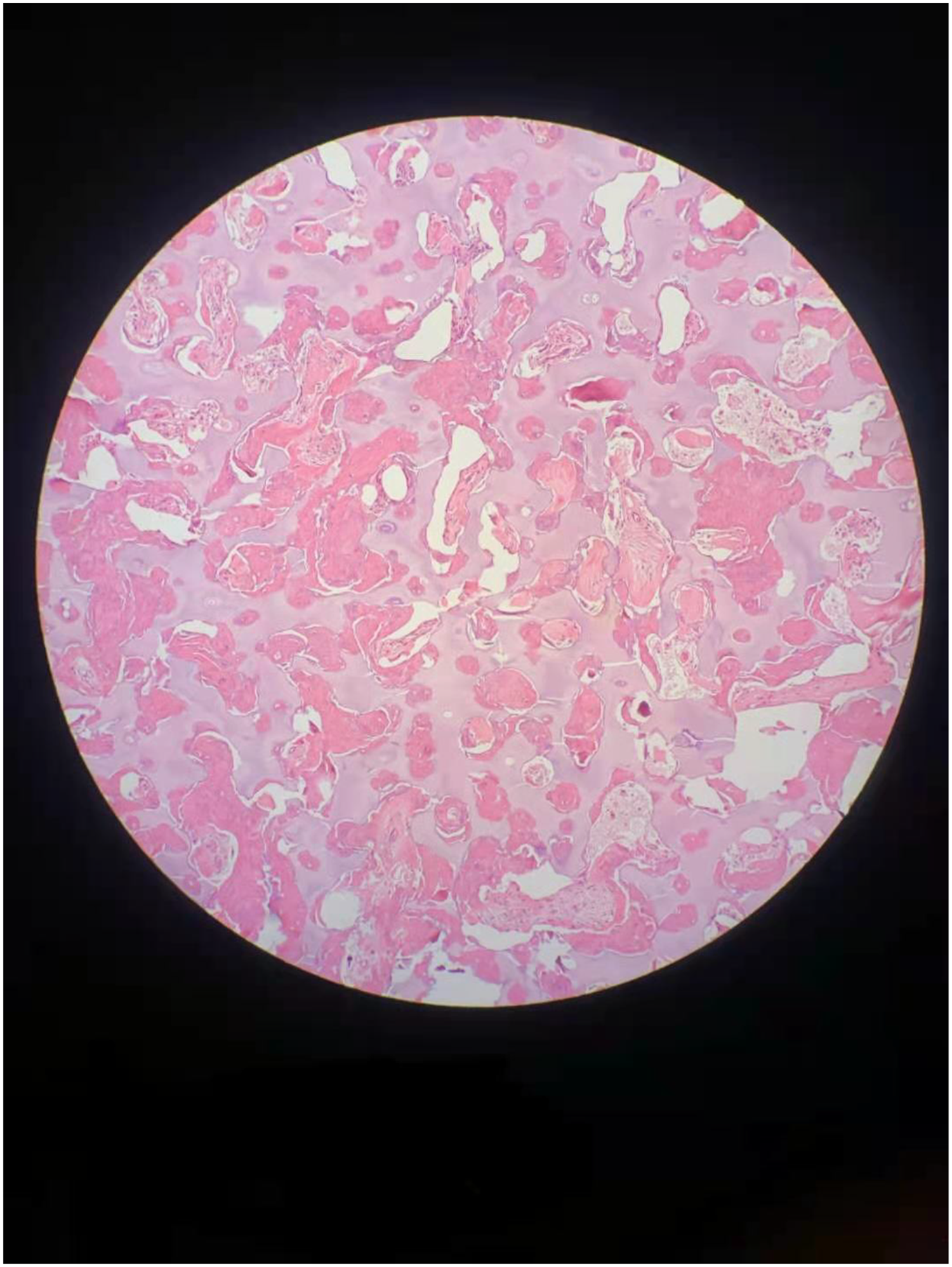
Section through the femoral head. Section through the femoral head that was removed intraoperatively, stained with hematoxylin and eosin and magnified 100×. This shows a large amount of cartilage-like matrix and disorganized bone trabeculae, inter-trabecular fibrous tissue hyperplasia, a narrow bone marrow cavity and a lack of hematopoietic cells.
The patient’s preoperative Harris hip function score was 40, but 1 year postoperatively, her Harris score was 95 and her postoperative hip function had improved. At the most recent follow-up examination, the patient showed no claudication or other postoperative complications, the active and passive activities of the left hip joint were good, and there was no pain or discomfort. Her activities of daily living had greatly improved, and she had no difficulty walking unaided and up and down stairs. The postoperative X-rays are shown in Figure 5.

Postoperative X-ray images of the patient. (a) Postoperative X-ray, showing equal lengths of the lower limbs, proper positioning of the prosthesis, good recovery of the length of both lower limbs and correction of the pelvic tilt and (b) X-ray obtained 1 year postoperatively, showing a blurred acetabular fracture line, equal length of both lower limbs and a correction of the pelvic tilt.
Discussion and review
Total hip arthroplasty for the treatment of ADOP with hip osteoarthritis or non-union of a periprosthetic hip fracture can be associated with a good outcome. 7 To date, there have been very few reports of the technical challenges and postoperative outcomes of total hip arthroplasty in patients with ADOP. We performed a total hip arthroplasty for the treatment of this condition in the present patient. She had severe osteosclerosis of her acetabulum; therefore, we used an acetabular file to reconstruct her acetabulum, filing it until a 48-mm acetabular trial mould could be stably positioned, so that a relatively large ball head (32-mm diameter) could be used, to reduce the risk of postoperative dislocation. The challenges associated with the surgery included the cutting of the femoral neck, 8 the preparation of the femoral canal, and the possibility of intraoperative fracture of the reconstructed femur.
Many researchers have reported methods of overcoming the difficulties associated with marrow expansion, owing to the hard, fragile femoral bone and narrow marrow cavity. Some have concluded that total hip arthroplasty is a safe and effective procedure for use in patients with osteopetrosis if there is careful preoperative planning. 9 In the present case, we accurately measured the patient’s bone density, her degree of medullary stenosis, and the difference in length between her two lower extremities by means of complete preoperative imaging to more fully assess the brittleness of the bone, the difficulty of marrow expansion and the complexity of repositioning. Such patients have high bone density and extremely brittle bones, which greatly increases the risks of intraoperative fracture and saw blade breakage. 10 We were extremely cautious and gentle during the procedure, and had adequate saw blades available, as well as internal fixation devices for intraoperative fractures. The patient’s femoral marrow cavity was extremely narrow, with a maximum width of 5.3 mm. To minimize the resistance to pulp cavity expansion, we prepared a small-headed, high-speed grinding drill, a Kirschner wire and a small-bore soft drill. This greatly reduced the difficulty associated with the enlarging of the medullary cavity and reduced the risk of fracture during the expansion process. The patient’s affected limb was approximately 6 cm shorter than the contralateral limb, which greatly increased the difficulty of repositioning, and the S-ROM prosthesis was prepared for total hip arthroplasty in combination with subtrochanteric osteotomy.
In a previous report, the use of total hip arthroplasty for the successful treatment of ADOP in combination with osteoarthritis of the hip was reported. The patients remained asymptomatic and pain-free at her 1-month, 1-year, and 2-year postoperative follow-up appointments, and the position of the prosthesis was acceptable. The investigators strongly recommended that surgeons prepare small dilation tools and small prostheses prior to such procedures to cope with the narrow medullary cavities and high risk of femoral fractures. 9 Individualized femoral stem prostheses and intramedullary guidance systems have also been used for hip replacement in patients with osteopetrosis, 11 but the biggest drawback of customized prostheses is their high cost.
The choice of hip arthroplasty prosthesis for patients with osteopetrosis may also be an issue worth exploring. The small area of sclerotic, high-quality cancellous bone that characterizes osteopetrosis may prevent the adhesion of cement, but can still permit stable fixation of the implant. 12 Fracture healing may be poor in patients with osteopetrosis, and in theory, the stability of bone-growing non-cemented prostheses may be compromised. However, Matsuno and Katayama reported three cases in which a non-cemented prosthesis was used and no loosening was identified. 13 The present patient had a history of fractures that healed well and no previous history of non-union. Moreover, during intraoperative acetabular reconstruction, the cancellous bone showed appropriate exudation, and we inserted a biotype prosthesis that showed good initial stability and was associated with no problems at the 1-year postoperative follow-up examination.
In addition, the risk of acetabular fracture during hip arthroplasty in patients with stone bone disease should not be ignored. Previous studies have shown a very high incidence of intraoperative acetabular fractures, which can be fixed with the aid of screws, and the operator should begin by cautiously reaming the socket using a small-diameter acetabular file. 14 In the present case, a fracture occurred during the placement of the acetabular prosthesis, but intraoperative fluoroscopy did not reveal any significant displacement, so additional fixation was not used. After acetabular reconstruction is completed, the cartilage and bone cortex on the acetabular surface are lost and the exposure of the cancellous bone surface greatly increases the risk of fracture. The problems of pelvic tilt and the unequal lengths of the patient’s lower extremities were solved in the present case, which greatly improved the quality of life of the patient. Previous studies have shown that the degree of postoperative recovery of pelvic tilt is inextricably linked to the degree of preoperative hip flexor contracture and spinal deformity. 15 In the present case, the patient’s pelvic tilt and the substantial difference in the lengths of her lower limbs were shown to have been corrected on the X-ray obtained 5 days postoperatively. Such a rapid correction is extremely rare in clinical practice. We believe that after the patient’s hip pain had been relieved and the centre of rotation of the acetabulum had been corrected, owing to the elasticity of the muscles, fascia and ligaments around her spine and hip joint and the short period of time during which she had had lower limb length disparity, compensatory scoliosis and pelvic tilt, such that no obvious structural changes had developed, her pelvic balance and lower limb length were rapidly restored.
In addition, total hip arthroplasty in patients with osteopetrosis is associated with greater risks of complications such as perioperative infection, periprosthetic fracture, fracture non-union and sciatic nerve injury. 16 Owing to narrowing or disappearance of the medullary cavity, bone marrow vascularity is reduced and the white blood cell function of patients with osteopetrosis is impaired. Antibiotics should be administered during the perioperative period to prevent postoperative infection. Patients are predisposed towards periprosthetic fractures related to the fragility of the bone in patients with osteopetrosis, and therefore they should be advised to move around carefully following surgery. Researchers have shown that some patients develop postoperative symptoms of sciatic nerve injury, possibly because of sciatic nerve traction caused by limb lengthening, prolonged intraoperative retractor compression or iodine irrigation. 17 To avoid complications such as fracture and excessive stretching of the sciatic nerve, surgeons are advised to handle these tissues gently.
In conclusion, large studies of the long-term outcomes of total hip arthroplasty for the treatment of osteopetrosis and its related complications have not been performed. Therefore, the optimal strategy for the use of total hip arthroplasty in such patients is unclear. The present patient underwent total hip arthroplasty under fluoroscopic and Kirschner wire guidance using a Tri-lock all-ceramic biotype prosthesis. Follow-up examinations showed good clinical results: 1 year postoperatively, her Harris score was 95, her hip function had improved and her leg length had been restored. However, longer-term follow-up is required. The treatment used in the present case may represent a viable option for the treatment of these rare cases. The present study has some limitations: only one case was studied, the patient was followed for only 1 year and she did not undergo genetic testing. Additional case reports of successful treatment and larger studies are needed to help clinicians reach a consensus regarding the best treatment for such patients.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231187803 - Supplemental material for Total hip arthroplasty for the treatment of a hip disorder complicated by autosomal dominant osteopetrosis: a case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605231187803 for Total hip arthroplasty for the treatment of a hip disorder complicated by autosomal dominant osteopetrosis: a case report by Congcong Wei and Huijie Li in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605231187803 - Supplemental material for Total hip arthroplasty for the treatment of a hip disorder complicated by autosomal dominant osteopetrosis: a case report
Supplemental material, sj-pdf-2-imr-10.1177_03000605231187803 for Total hip arthroplasty for the treatment of a hip disorder complicated by autosomal dominant osteopetrosis: a case report by Congcong Wei and Huijie Li in Journal of International Medical Research
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
The Institutional Review Board of the Ethics Committee does not require a full review or approval for case reports. Verbal consent was obtained from the patient through telephone interviews during the investigation and reporting, and all the necessary patient information was collected and anonymized. We obtained the written informed consent of the patient to publish their clinical details.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.