
Abstract
Introduction:
As recent studies demonstrate an ongoing debate surrounding outcomes and complications with respect to different total hip arthroplasty (THA) approaches, patient-reported outcome measures (PROMs) may provide valuable information for clinician and patient decision-making. Therefore, our systematic review aimed to assess how surgical approach influences patient-reported outcomes.
Methods:
5 online databases were queried for all studies published between January 1, 1997 and March 4, 2022 that reported on PROMs across various surgical approaches to THA. Studies reporting on PROMs in primary THA patients segregated by surgical approach were included. Articles reporting on revision THA, hip resurfacing, and arthroscopy were excluded. Mantel-Haenszel (M-H) models were utilised to calculate the pooled mean difference (MDs) and 95% confidence interval (CIs).
Results:
No differences between the DAA and other approaches were observed when evaluating HOOS (MD −0.28; 95% CI, −1.98–1.41; p = 0.74), HHS (MD 2.38; 95% CI, −0.27–5.03; p = 0.08), OHS (MD 1.35; 95% CI, −2.00–4.71; p = 0.43), FJS-12 (MD 5.88; 95% CI, −0.36–12.12; p = 0.06), VAS-pain (MD −0.32; 95% CI, −0.68–0.04; p = 0.08), and WOMAC-pain (MD −0.73; 95% CI, −3.85–2.39; p = 0.65) scores. WOMAC (MD 2.47; 95% CI, 0.54–4.40; p = 0.01) and EQ-5D Index (MD 0.03; 95% CI, 0.01–0.06; p = 0.002) scores were found to significantly favour the DAA cohort over the other approaches. Only the EQ-5D index score remained significant following sensitivity analysis.
Conclusions:
Superiority of any 1 approach could not be concluded based on the mixed findings of the present analysis. Although our pooled analysis found no significant differences in outcomes except for those measured by the EQ-5D index, a few additional metrics, notably the WOMAC, HHS, FJS-12, and VAS-pain scores, leaned in favour of the DAA.
Introduction
Total hip arthroplasty (THA) is considered 1 of the most successful, cost-effective, and popular surgical interventions in medicine.1–3 Most commonly indicated for symptomatic osteoarthritis (OA), THA has been shown to consistently improve pain scores and quality of life both long and short-term postoperatively. 4 In a recent analysis by Kurtz et al., 5 the annual use of THA is estimated to increase by 174% between 2010 and 2020. These trends naturally raise the question of how to optimise the procedure to achieve superior patient outcomes.
Although there are several approaches to the hip joint, the most adopted techniques include the direct anterior (DAA), posterior (PA), and direct lateral (DLA) approaches. Differences in risk of adverse clinical outcomes such as dislocation, abductor insufficiency, nerve injury, and fractures has been shown to differ across techniques. 6 As such, the optimal approach proves to be an area of contention, with no strong consensus demonstrated in the current literature. PA has historically been associated with increased dislocation rates due to soft tissue damage, especially without adequate joint capsule repair. 7 However, a recent retrospective study of approximately 6000 propensity score-matched THA recipients found that risk of major complications within 1 year, including deep infection, dislocation, and need for revision, was significantly increased for the DAA group within 1 year following surgery. 8 Another single-institution study noted similar complication rates across DAA, PA, and DLA groups, but noted significantly higher rates of revision after DAA due to increased peri-prosthetic fractures. 9
Outside of surgical outcomes, patient-reported outcome measures (PROMs) are increasingly utilised in orthopaedic arthroplasty registries. These broadly measure self-reported aspects of health-related quality of life, such as pain, stiffness, and function. PROMs are promising tools that can play a key role in informing clinical decision-making, patient-centered care, as well as reimbursement decisions.10–12 Notably, there are currently no comprehensive pooled analyses of PROMs following THA comparing surgical approaches, representing a gap in the literature that may elucidate further benefits and drawbacks of each surgical approach. As recent studies and meta-analyses demonstrate an ongoing debate surrounding clinical outcomes and complication risks with respect to approach, PROMs may provide valuable information for clinician and patient decision-making.8,13 To that end, the present analysis aims to assess how surgical approach influences patient-reported quality of life.
Methods
Literature search
Pubmed, MEDLINE, EBSCO Host, and Google Scholar online databases were queried for all studies published between 01 January 1997 and 04 March 2022 that reported on PROMs across various surgical approaches to THA. The following MeSH and keywords were employed to search the literature in combination with “AND” and “OR” Boolean operators: “Arthroplasty, Replacement, Hip[MeSH]”; “total hip arthroplasty”; “total hip replacement”; “THA”; “approach”; “surgical approach”; “surgical technique”; “Patient Outcome Assessment[MeSH]”; “functional outcome”; “patient outcome”; “patient reported outcome”; “PROM”.
Eligibility criteria
The following criteria were established prior to query to identify studies for inclusion: (1) English, full texts were available; (2) reported on primary THA patients; (3) studies reporting PROMs segregated by surgical approach to THA (DAA, PA, DL, AL); (4) reported raw data in a fashion that could be implemented into a pooled analysis. Given the similarities between the posterior and posterolateral approach, patients undergoing either of the 2 approaches were grouped into the PA category. 14 Exclusion criteria included: (1) duplicate studies across databases; (2) single or double case reports; (3) systematic reviews or meta-analyses; (4) studies reporting on revision THA; (5) studies reporting on hemi-arthroplasty; (6) studies reporting on hip resurfacing; (7) studies reporting on arthroscopy; (8) studies reporting on patients undergoing THA for femoral neck fracture; (9) studies reporting on minimally invasive surgical techniques; (10) studies reporting on surgical approaches other than DAA, PA, PLA (posterolateral approach), DLA, or ALA (anterolateral approach); (11) longitudinal studies reporting on the same set of patients. If articles utilised the same database or were conducted by identical authors, only the most recent article was taken into account to avoid over-representing a study and double-counting patients. However, if the patient populations or the time frame between the articles were deemed substantially different, multiple articles from the same author were included. A meta-analysis was conducted on outcomes that were: (1) described with adequate pooled analysis data (mean, standard deviation, and sample size) in at least 2 of the included studies; and (2) reported in 2 or more of the included studies. A total of 8 outcomes satisfied the aforementioned conditions: Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Hip disability and Osteoarthritis Outcome Score (HOOS), Harris Hip Score (HHS), Oxford Hip Score (OHS), EQ-5D EuroQol 5-dimension (EQ-5D) index, Forgotten Joint Score-12 (FJS-12), WOMAC-pain, and visual analogue scale (VAS)-pain.
Study selection
3 independent reviewers conducted our analysis of the literature in abidance with the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines (Figure 1). 15 Following the initial query, 432 articles were identified following the exclusion of duplicates. Subsequent evaluation of the titles and abstracts resulted in 95 remaining articles for full-text evaluation. Utilising the pre-determined inclusion and exclusion criteria, 24 articles were included in the final analysis.16–39 Each article’s reference list was evaluated in a stepwise manner, and no additional studies were included.
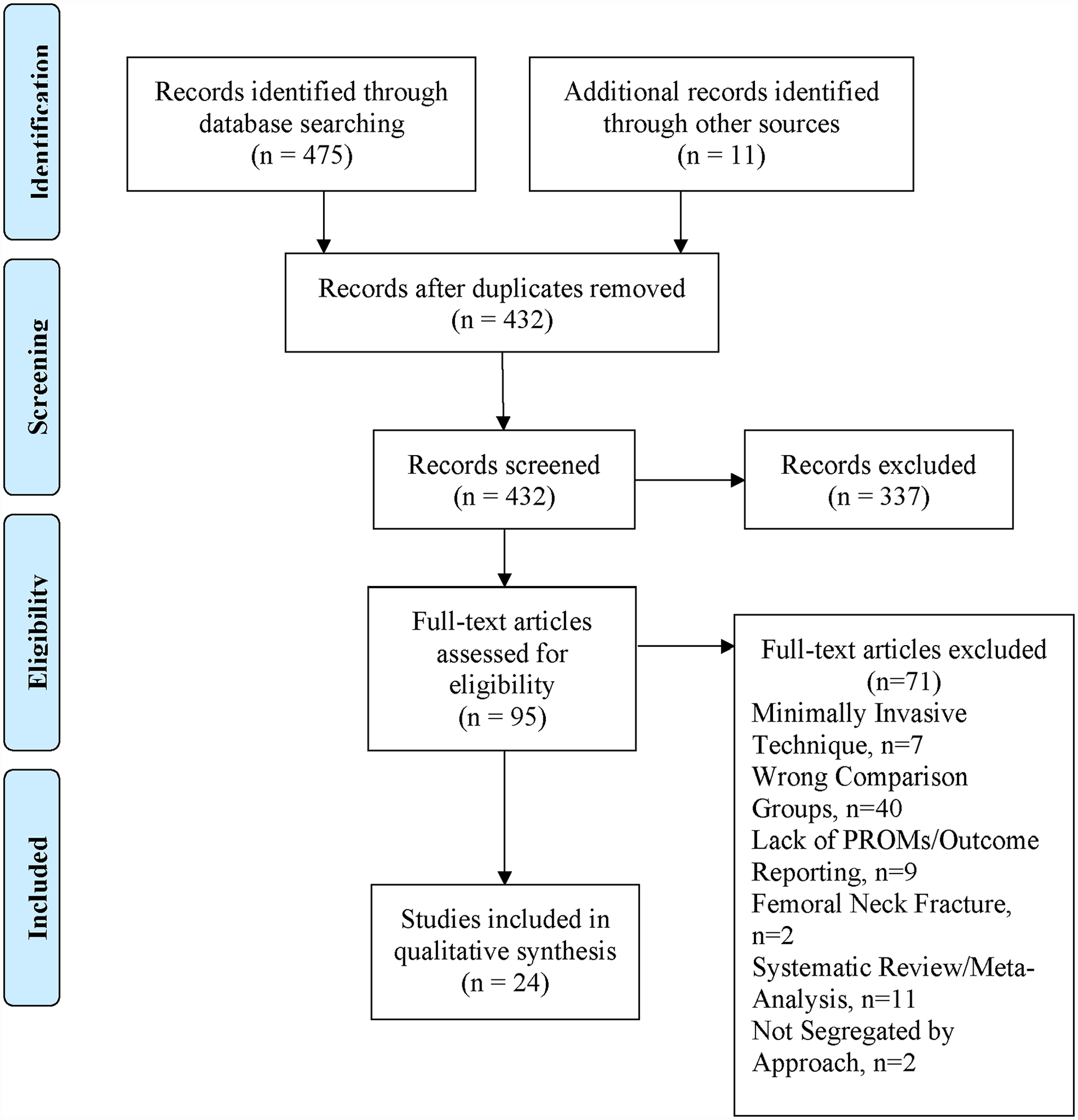
Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) diagram demonstrating article selection process.
Methodological quality assessment
Risk of bias was evaluated for all included studies. The Methodological Index for Non-Randomized Studies (MINORS) tool was utilised for all non-randomised studies. 40 This tool consists of 12 methodological criteria scored between 0 and 2 to total up to an ideal global score of 24. Based on the global score, bias levels are categorised as follows: 0–6 (very low quality), 7–12 (low quality), 13–18 (moderate quality), 19–24 (high quality). 41 On the other hand, the Detsky scale was applied to all included randomised control trials. 42 The Detsky scale assesses methodological quality utilising a maximum of 3–4 points for each bias domain. According to prior literature and methodology, scores of ⩾75% classified studies as high quality. 43 2 independent reviewers applied these tools to assess risk of bias in each included study. Any disagreements were resolved by a third reviewer.
Statistical analysis
To compare patient-reported outcome measures across surgical approaches for primary THA patients, a meta-analysis was performed. As the PROMs are continuous variables, a mean difference (MD) along with its 95% confidence interval (CI) was calculated between groups. For evaluating the level of heterogeneity among the eligible studies, I 2 values were utilised and classified as follows: low (0–25%), moderate (25–50%), and high (>50%) heterogeneity. 44 Mantel-Haenszel (M-H) models were utilised to evaluate the pooled effect of surgical approach on PROMs following THA. I 2 values ⩽ 50% warranted a M-H fixed effects model, while a M-H random effects model was utilised for I 2 values > 50%. 44 All pooled analyses were conducted on RevMan software version 5.4 (The Cochrane Collaboration, London, England, UK). Forest plots were generated to illustrate pooled analysis. A p-value < 0.05 was deemed significant. As our analysis used publicly available and deidentified data, it was exempt from Institutional Review Board (IRB) approval.
Sensitivity analysis
Multiple sensitivity analyses were done to evaluate the robustness of each study. Each study was removed from the pooled analysis one at a time to assess how each study affected the overall pooled effect. Additionally, multiple effect measures and M-H models were applied and compared. Differences in PROMs were evaluated following exclusion of any studies considered to have moderate or high bias.
Results
Included studies
The present analysis included 24 articles reporting on a total of 22,605 THAs (DAA: 8,121, PA: 11,943, LA: 2,541). The demographics from each included study are depicted in Table 1.
Summary of included studies.
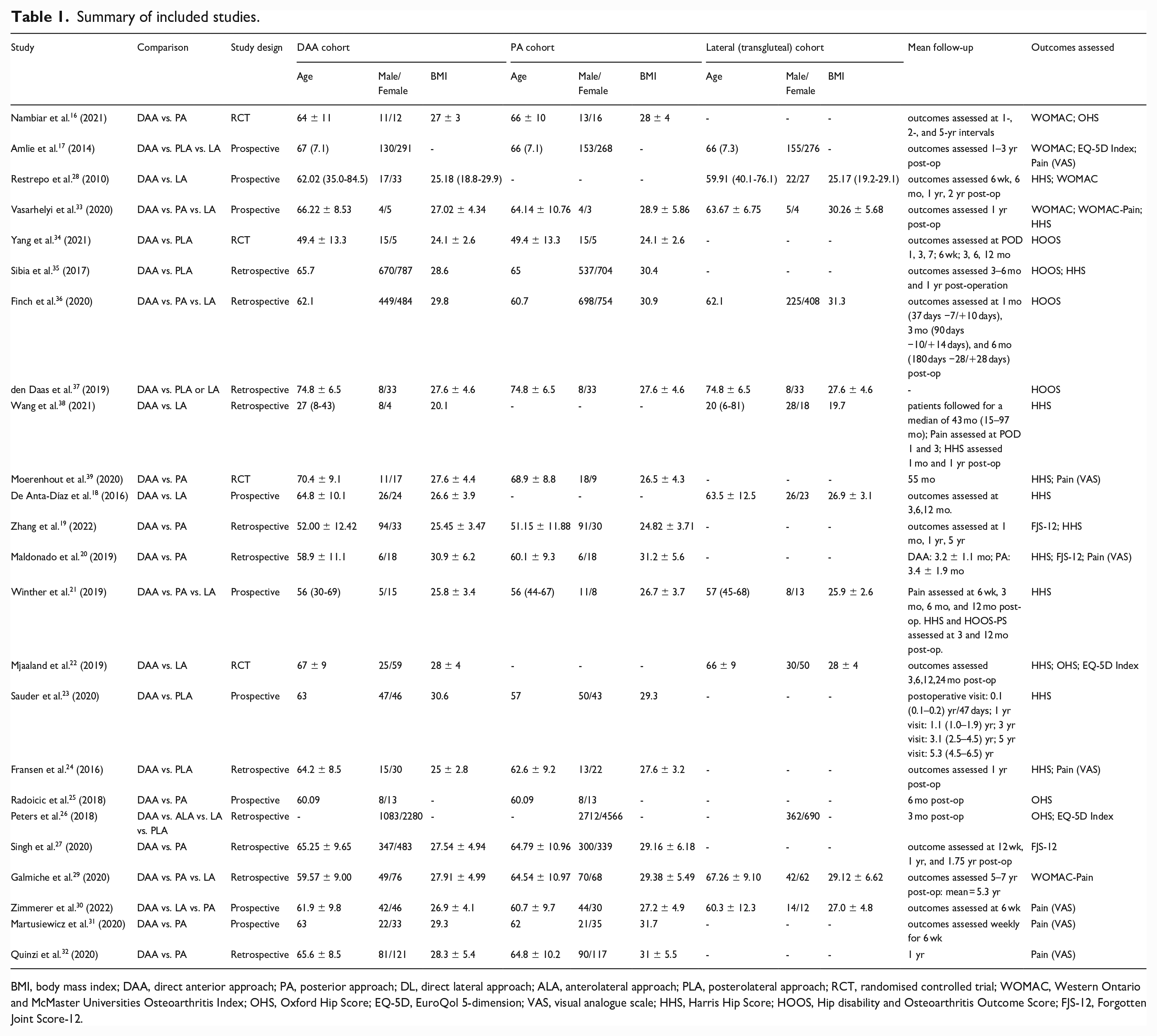
BMI, body mass index; DAA, direct anterior approach; PA, posterior approach; DL, direct lateral approach; ALA, anterolateral approach; PLA, posterolateral approach; RCT, randomised controlled trial; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index; OHS, Oxford Hip Score; EQ-5D, EuroQol 5-dimension; VAS, visual analogue scale; HHS, Harris Hip Score; HOOS, Hip disability and Osteoarthritis Outcome Score; FJS-12, Forgotten Joint Score-12.
Risk of bias assessment
The average MINORs score for the 19 non-randomised studies included in our analysis was 18.1 (standard deviation [SD] 2.02). 11 studies were of moderate quality, and 8 studies were high quality. The average Detsky score for the 5 RCTs was 18.9 (SD 0.89). All 5 studies were deemed high quality.
HHS
The Harris Hip Score (HHS) was the most utilised PROM with 12 studies comparing DAA to other approaches (Table 1).18–24,28,33,35,38,39 6 of the 12 included studies provided data that could be used for pooled analysis. While the general trend of the HHS scores seemed to favour the DAA, this difference between DAA and other approaches was not significant under the random-effects model (MD 2.38; 95% CI, −0.27–5.03; p = 0.08) (Figure 2).
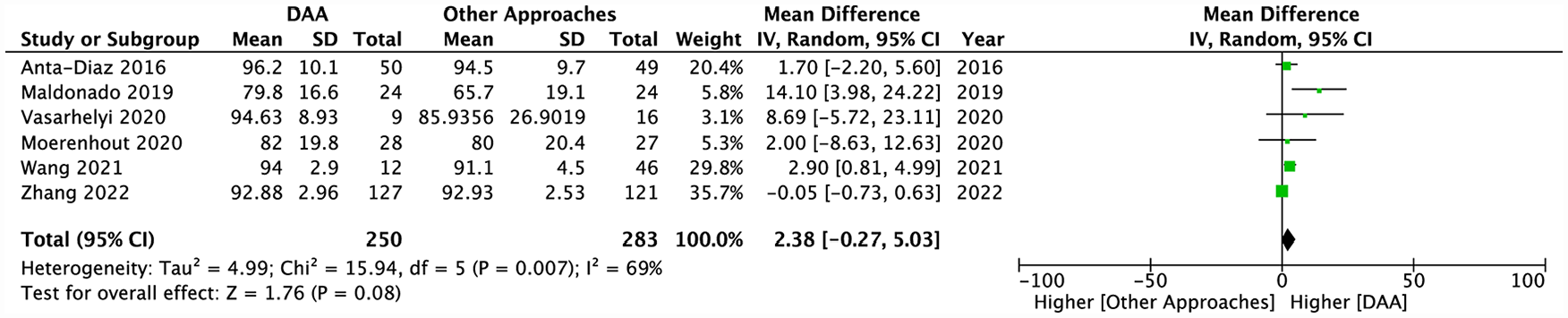
Pooled analysis comparing post-operative HHS scores between the DAA and other approaches.
Of the remaining 6 studies not included in the pooled analysis, 3 evaluated the differences between DAA and PLA.23,24,35 At the earliest follow-up point of 3–6 months, Sibia et al. 35 found that the HHS favoured the DAA group (DAA: 95.3 vs. PLA: 89.1, p < 0.001), which was further confirmed after adjusting for preoperative differences in HHS and body mass index (BMI) between the 2 cohorts. However, at a later follow-up of 1 year, no significant differences in HHS scores were noted between the DAA and PLA groups (DAA: 94.9 vs. PLA: 95.7, p = 0.478). 35 Similarly, Fransen et al. 24 noted no significant differences in median HHS scores at 1 year follow-up (DAA: 96.5 vs. PLA: 97, p = 0.072). In contrast to Sibia et al., 35 Sauder et al. 23 observed that the HHS favoured the PLA group at the earliest time-point (1.5 months postoperatively) with the DAA group being less likely to reach the HHS patient acceptable symptom state (PASS) than the PLA group (DAA: 30% vs. PLA: 47%, OR: 0.454, p = 0.015). Nonetheless, longer term follow-ups of 1, 3, and 5 years revealed no significant differences in the proportion of patients who reached the HHS PASS between those who underwent DAA versus PLA. 23
Comparing DAA to LA, although Restrepo et al. 28 found significant differences at the earliest follow-up of 6 weeks (DAA: 93.64 vs. LA: 88.80, p = 0.03), significance was lost at the latest follow-up of 2 years (DAA: 97.34 vs. LA: 97.55, p = 0.72). Mjaaland et al., 22 on the other hand, observed no statistically or clinically significant differences across all time-points, including 3 month, 6 month, 1 year, and 2 year follow-ups. In line with this observation, Winther et al. 21 similarly noted no differences in HHS scores across 3 different approaches (DAA vs. PA vs. LA) at any of the follow-up points (p > 0.07).
WOMAC
A total of 4 articles reported on total Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores between DAA and other approaches to THA (Table 1).16,17,28,33 Data were able to be pooled for 2 of the 4 included studies. With the fixed-effects model, DAA was found to have a significantly higher WOMAC score than other approaches (MD 2.47; 95% CI, 0.54–4.40; p = 0.01) (Figure 3). However, this finding was determined to be not significant following sensitivity analysis.

Pooled analysis comparing post-operative overall WOMAC scores between the DAA and other approaches.
When evaluating functional and radiographic outcome differences between the DAA and PA, Nambiar et al. 16 found no differences in median WOMAC scores across different time points within a 5-year follow-up period. Specifically at the 5-year follow-up, the median WOMAC score reported for the DAA group was 6 (range 0–81) and 7 (range 0–59) for the PA group (p = 0.96). 16 However, when comparing DAA and LA, mixed evidence was presented. Despite improvements in functional outcomes for both DAA and LA, Restrepo et al. 28 observed no significant difference in WOMAC scores 2 years postoperatively (DAA: 2.24 vs. LA: 1.90, p = 0.60). Interestingly, at an earlier follow-up of 6 weeks, the LA group had a significantly higher WOMAC score of 9.70 compared to the DAA group’s score of 4.40 (p = 0.001). 28
HOOS
The Hip Disability and Osteoarthritis Outcome Score (HOOS) was evaluated by a total of 4 articles (Table 1).34–37 Of the 4 included studies, data could be pooled from 2 articles. Using the fixed-effects model, no significant differences in HOOS scores were noted between the DAA and other approaches (MD −0.28; 95% CI, −1.98–1.41; p = 0.74) (Figure 4).

Pooled analysis comparing post-operative overall HOOS scores between the DAA and other approaches.
The remaining articles not included in the pooled analysis reinforced this finding. When evaluating DAA versus PLA, Sibia et al. 35 observed that HOOS scores did not favour either approach at both the 3–6 month and 1 year follow-up time-points. At the 3–6 month follow-up, the reported HOOS score was 87.0 for the DAA group and 88.8 for the PLA group (p = 0.238). For the 1-year follow-up, the HOOS score was 91.4 and 93.1 for the DAA and PLA groups, respectively (p = 0.312). Similarly, Finch et al. 36 found no differences in adjusted HOOS Jr. scores at 1, 3, and 6 month follow-ups. In particular, at the longest follow-up of 6 months, the adjusted HOOS Jr. scores were 85.6 (95% CI, 84.5–86.6) for the PA group, 85.0 (95% CI, 83.3–86.6) for the LA group, and 85.7 (95% CI, 84.4–86.9) for the DAA group. 36
OHS
A total of 4 articles reported on the Oxford Hip Score (OHS) in DAA versus other approaches (Table 1).16,22,25,26 2 of the 4 studies could be included in our pooled analysis. By the random-effects model, no differences were found in OHS scores between the DAA and other approaches (MD 1.35; 95% CI, −2.00–4.71; p = 0.43) (Figure 5). In line with this result, Nambiar et al. 16 noted no differences in OHS scores at all follow-ups between DAA and PA. At the latest follow-up time-point of 5 years, the median OHS scores for DAA and PA were 46 and 47 (p = 0.93), respectively. 16

Pooled analysis comparing postoperative OHS scores between the DAA and other approaches.
On the other hand, when comparing 4 different approaches (DAA vs. ALA vs. PLA vs. LA), Peters et al. 26 observed the greatest improvement in OHS scores in the DAA cohort (16.69), which was followed by PLA (16.10), LA (15.30), and ALA (15.27). After adjusting for confounding variables and baseline differences, the DAA group was found to have significantly greater improvement than the PLA and LA cohort. 26
EQ-5D
The EQ-5D index was utilised to evaluate patient outcome in a total of 3 studies (Table 1).17,22,26 With the fixed-effects model, pooled data from 2 of these analyses demonstrated significantly higher EQ-5D index scores (i.e. higher health status) for DAA over other approaches (MD 0.03; 95% CI, 0.01–0.06; p = 0.002) (Figure 6). Although not included in the pooled analysis, when comparing DAA versus ALA versus LA versus PLA, Peters et al. 26 noted no significant differences in EQ-5D index score improvements across all approaches.

Pooled analysis comparing post-operative EQ-5D Index scores between the DAA and other approaches.
FJS-12
The Forgotten Joint Score (FJS-12) was evaluated by a total of 3 articles comparing DAA versus PA (Table 1).19,20,27 Though the FJS-12 scores tended to favour DAA, pooled data from all 3 of these studies demonstrated no significant differences in FJS-12 scores between the DAA and PA group (MD 5.88; 95% CI, −0.36–12.12; p = 0.06) (Figure 7).

Pooled analysis comparing post-operative FJS-12 scores between the DAA and PA.
Pain
The present analysis utilised WOMAC pain subscale scores and the visual analogue scale (VAS) to evaluate postoperative pain in DAA versus other approaches. A total of 2 articles compared WOMAC pain subscale scores between DAA and other approaches (Table 1).29,33 Using the fixed-effects model, pooled data from both these articles exhibited no significant differences in WOMAC pain subscores between DAA and other approaches (MD −0.73; 95% CI, −3.85–2.39; p = 0.65) (Figure 8).

Pooled analysis comparing post-operative WOMAC-Pain subscale scores between the DAA and other approaches.
The most utilised tool for evaluating postoperative pain was the VAS score, reported by 8 articles (Table 1).17,20,22,24,30–32,39 Data could be pooled for 4 of the 8 studies. Under the random-effects model, although VAS scores tended to be higher in other approaches (i.e. greater pain), no significant differences were ultimately noted between DAA and other approaches (MD −0.32; 95% CI, −0.68–0.04; p = 0.08) (Figure 9).

Pooled analysis comparing post-operative VAS scores between the DAA and other approaches.
The remaining studies not included in the pooled analysis presented similar evidence regarding the superiority of DAA over other approaches for VAS pain scores. Fransen et al. 24 demonstrated no differences in 1-year postoperative VAS scores between the DAA (median [interquartile range] (IQR): 0 [1]) and PLA (0 [0]) cohorts (p = 0.773). Martusiewicz et al. 31 observed significantly lower inpatient VAS pain scores (p < 0.05) in the DAA group than the PA group, but at the time of discharge, VAS scores were comparable between the 2 cohorts. In another study investigating the VAS pain outcomes across 3 approaches (DAA vs. PLA vs. LA), Amlie et al. 17 noted similar outcomes between the DAA and PLA cohort. However, the VAS pain scores were found to heavily favour the DAA over the LA (p = 0.007). 17
Discussion
In this systematic review and meta-analysis of 24 studies, PROMs for 22,605 THAs were compared revealing no differences in pooled scores for WOMAC, HOOS, HHS, OHS, FJS-12, and pain (WOMAC and VAS) across the anterior, posterior, and lateral approaches for THA. Conversely, the EQ-5D index demonstrated a significant difference following sensitivity analysis with higher scores in the DAA group compared to other approaches.
Utilising PROMs for evaluation of outcomes after THA creates the inherent challenge of addressing ceiling effects. A ceiling effect is considered present if more than 15% of respondents achieve the highest possible score. 45 The FJS-12 was developed to have greater discriminatory power for the well-performing patients after arthroplasty, and it better differentiates hip-related outcomes in patients with a successful THA compared to the OHS.46,47 In this study, the OHS in addition to the FJS-12 showed no difference in outcomes when comparing DAA to other approaches despite having improved discriminatory capacity. With the discriminatory power among well-performing patients of the FJS score, showing no difference in scores among the hip approaches in the pooled analysis reinforces the findings in this study.
This study identified potential early differences in PROMs by surgical approach in the early post-operative period, particularly for WOMAC, HHS, OHS, and VAS-pain outcome scores. Sibia et al. 35 adjusted HHS for preoperative score and BMI, confirming higher HHS scores for DAA than PLA at 3–6 month follow-up. Similarly, Restrepo et al. 28 found the DAA to have better WOMAC and HHS at 6 weeks compared to LA. Additionally, Sauder et al. 23 found the PLA to have better HHS compared to DAA at early time points. None of these studies, however, found any differences between approaches at later follow-up. Although PROMs were not the primary outcome, a systematic review and meta-analysis of early outcomes within 90 days of THA by Miller et al. 13 suggests that DAA patients have less pain and reported better hip function in the early post-operative period over the PLA group. Our study was not able to confirm or contest these findings with respect to PROMs in the early postoperative period as most of the early PROMs in this study were not pooled for analysis and individual studies had mixed results in the early post-operative period. However, by pooling PROMs at the latest follow ups, this study has addressed inherent differences in study populations and surgeons allowing for generalisability of our results.
The EQ-5D score was the only PROM found to show a difference after pooling the scores from Amlie et al. 17 and Mjaaland et al., 22 indicating higher EQ-5D scores for the DAA compared to other approaches after sensitivity analysis. Amlie et al. 17 identified marked ceiling effects in the WOMAC and EQ-5D scores and did not perform statistical testing between the groups; however, they highlighted that the average EQ-5D scores for the LA were lower than PLA and DAA at 0.80 compared to 0.86 and 0.86 respectively. Furthermore, Mjaaland et al. 22 compared the DAA and the LA, demonstrating a statistical difference in EQ-5D scores at 12 months with scores 0.83 and 0.77 for the DAA and DLA, respectively. Importantly, post-operative limp has been shown to correlate with lower PROMs. Amlie et al. 17 analysed the effect of limping on PROMs and adjusting scores for patients with postoperative limp. The significant differences in PROMs found in their study were eliminated after correction for limping. In their study, patients who underwent THA with the DLA were twice as likely to report post-operative limp than the DAA or the PLA. 17 Therefore, pooling the data of these 2 studies likely reached the power to detect a difference between the DAA and other approaches in our study. Nonetheless, in both pooled studies, the average difference between the scores was 0.06. The minimal clinically important difference (MCID) for the EQ-5D is 0.074. 48 Despite finding a statistical difference after pooling the scores, given that the difference between the scores is less than the MCID, this finding of statistically higher EQ-5D scores for DAA compared to the combined PLA and DLA approaches in our study is likely not clinically significant.
Our analysis has some limitations. Several studies reported each PROM, but pooling the data was only appropriate for 2–6 studies for the PROMs analysed. Additional metrics (i.e. HOOS-pain) were excluded due to under-reporting. Although final time points were combined for comparison, inconsistencies in these time-points make it challenging to make a firm conclusion on the optimal approach to THA. The inconsistent time-points reported across the included studies as well as the limited data available for pooled analysis further complicated the stratification of our results by time-frame (i.e. short-term vs. long-term outcomes). However, the majority of the included studies, especially those included in our pooled analysis, reported on mid- to long-term outcomes (>1 year) and thus, using the PROMs from the latest follow-up is unlikely to change our results. Additionally, some studies reported PROMs from a cohort of patients for a range of several years of postoperative follow-up. Therefore, we were unable to characterise the differences in PROMs across THA approaches for each time-point of available follow-up. A comparison of THA approaches at early-, mid-, and long-term follow-ups remains necessary. Additionally, surgeon experience and indications for a particular THA approach and control for patient comorbidities was not able to be incorporated into our analysis due to the limited data availability. Finally, this study focused on a comparison of DAA to the other approaches by combining the PROMs of PA, PLA, and DLA approaches, and thus, individual approach comparisons is warranted. Despite these limitations, this comprehensive systematic review and meta-analysis was able to successfully analyse the most commonly used PROMs in THA across the literature to compare the DAA to PA, PLA, and LA for THA.
Conclusion
The present study found that patients having their THA through an anterior approach had statistically equivalent PROMs to posterior and lateral approaches. Differences were noted among studies in the early postoperative period for certain outcomes, but with further follow-up, no differences were found between the various approaches. Ultimately, surgical approach should be determined by surgeon experience and preference for the individual patient. Further studies pooling data at more time intervals and subgroup analyses between individual approaches are needed to complete our understanding of how approach affects PROMs after THA.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AFK: Research support from Signature Orthopaedics; paid presenter or speaker for: DePuy Synthes, Zimmer Biomet; paid consultant for: DePuy Synthes, Zimmer Biomet; owns stock or stock options in: Zimmer Biomet, Johnson & Johnson, and Procter & Gamble; receives IP royalties from: Innomed.
All other authors declare that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.