
Abstract
Background:
Short stems are designed with a bone preservation philosophy in mind. This study aims to compare the outcomes/complications and survival of a collarless fully hydroxyapatite (HA)-coated conventional tapered stem and a HA-coated partial neck-retaining uncemented short stem in patients ⩽55 years old at medium-term follow-up.
Methods:
We retrospectively studied 247 uncemented THAs operated between 2010 and 2014, comparing 146 patients treated with the fully HA-coated collarless stem (Group A) with 101 patients treated with a partial neck preserving, HA-coated short stem (Group B). 87 and 62 males were in groups A and B, respectively (p = 0.11). The mean age of the series was 46 years (17–55) (p =0.16). The mean follow-up of groups A and B were 9.9 (7–12) years and 9.7 (7–12) years, respectively (p =0.21).
Results:
Mean Harris Hip Score improved from 55 to 92 in group A (p <0.001) and from 54 to 95 in group B (p <0.001), without differences between groups. Mean femoral neck length preservation in groups A and B was 13.6 (0–28) mm and 26 (11–38) mm, respectively (p =0.001). 13 (8.9%) and 1 (1%) patients in groups A and B presented postoperative complications, respectively (p =0.008). The conventional stem group had more aseptic loosening (Group A 3.4% vs. Group B 0%, p =0.06) along with more Symptomatic radiolucent lines (Group A 3.4% vs. Group B 0%, p =0.06).
Conclusions:
Both conventional and short stems showed excellent implant survival rates and functional outcomes at a mean follow-up of 9.8 years. However, complications and radiolucent lines were more frequent with a collarless conventional-length stem. Bone preservation of the femoral neck and diaphysis may be preferred in active young patients.
Keywords
Background
It is predicted that by 2030, 52% of primary total hip arthroplasties (THAs) will be implanted in patients <65 years old, whereas the most significant growth is expected in patients aged 45–55 years. 1 However, given the young age at surgery, a proportion of the patients will undergo hip revision surgery. In this sense, bone stock is an essential factor to consider in the subsequent surgical reconstruction.
In order to improve survivorship and outcomes, numerous uncemented designs have been developed. The CORAIL stem (DePuy-Synthes, Warsaw, IN, USA) has been commercially used since 1986. Several studies have evaluated the short-, medium- and long-term outcomes of the first generation CORAIL stem. Vidalain2–4 evaluated the initial cohort of 2956 first-generation stems and found a 99% survivorship at 5 years, 98% at 10 years and 96% at 23 years of follow-up. A recent paper reviewed the performance of this design in the Norwegian Arthroplasty Register showing a 30-year survival of the standard collarless stem of 88.4%, 93.3%, and 94.4% using stem revision for any non-infectious cause, aseptic loosening, and periprosthetic fracture of the femur as endpoints, respectively. 5
Given that the age of clinical indications for THA has changed over the last few years towards younger patients with higher activity demands, 6 short femoral stems are an alternative, minimising stress-shielding and preserving bone stock for future generations revisions in this young population.7,8 Thus, different short stem designs have been developed in the past decade, not to outperform the results obtained with many successful conventional stems but to reproduce those with less femoral bone compromise,9,10 a more physiological load transfer to the femur, with the potential of facilitating an eventual removal.11,12 The MiniHip stem (Corin Group PLC, Cirencester, UK) is a short, HA-coated, partial neck-preserving design rated with 10A ODEP categorisation. 13
Because clinical and radiographic comparisons between conventional and short stems are scarce,14,15 it remains unclear whether a short stem shows similar outcomes and survivorship as a conventional uncemented well-known design. Therefore, we asked: what is the survival up to a mean follow-up of 9 years of a standard collarless fully HA-coated conventional tapered stem and an HA-coated short stem in young and active patients?
Patients and methods
Patients
This study was performed following the 1964 Declaration of Helsinki principles and was approved by the Institution’s Research Ethics Board. Informed consent was obtained from all participants, and consent to publish was obtained for the patients whose radiographs appear in this manuscript.
We prospectively studied a consecutive series of 1100 primary THAs operated on between 2010 and 2014, of which 20 were cemented, 247 were hybrid, and 833 were cementless. Of the uncemented femoral components, 210 were excluded because they were copies of the original CORAIL stem, 506 were fully-tapered HA-coated stems (CORAIL), (Group A) (Figure 1(a)), and 117 were partial neck preserving, HA-coated short designs (MiniHip stem), (Group B) (Figure 1(b)). We excluded 300 cases in Group A for not being young and 60 because they were lost to follow-up. 16 cases were excluded in Group B, 14 of them for not being young and 2 were lost to follow-up.
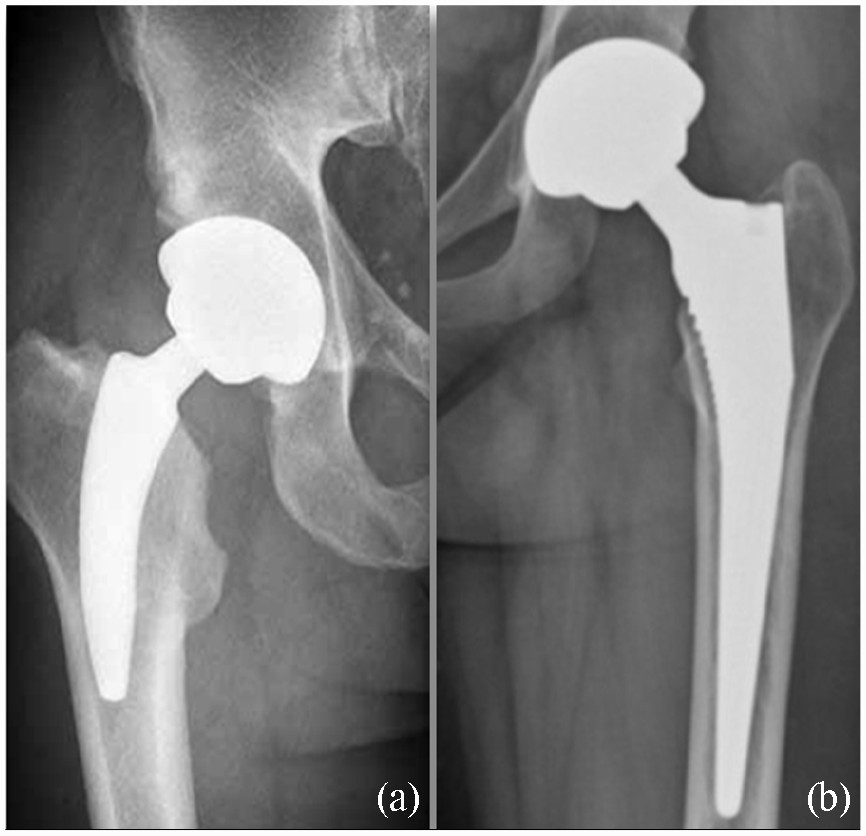
(a) Postoperative AP radiographs showing the partial neck-retaining HA-coated short MiniHip TM cementless stem (Corin Group PLC, Cirencester, UK) and (b) the fully HA-coated tapered CORAIL TM cementless stem (DePuy-Synthes, Warsaw, IN).
Group A finally included 146 patients treated with the fully hydroxyapatite-coated CORAIL stem operated by 3 surgeons, and Group B included 101 patients treated with a partial neck retaining MiniHip short-stem operated by a fourth surgeon.
Inclusion criteria for short stems were patients ⩽55 years old or those between 56 and 60 years who regularly practised impact sports before THA. These patients needed to have an adequate metaphyseal bone stock, an intact femoral neck, a competent medial calcar, and a sufficient distal lateral femoral cortex to achieve the anatomical restoration described by the designers. 16
11 and 16 patients had 1-stage bilateral THAs in groups A and B, respectively. Data were retrieved from the institution’s prospectively collected electronic database, digitalised since 2006. The mean age of the series was 46 years (17–55) (p =0.16). There were 87 and 62 male patients in groups A and B, respectively (p =0.11). Obese patients were defined as having body mass index (BMI) ⩾ 30 kg/m2. Mean follow-up was 9.4 years (7–11 years) for Group A and 9.1 years (7–10 years) for Group B (p =0.07). Detailed demographic characteristics are shown in Table 1.
Demographic characteristics of the series.
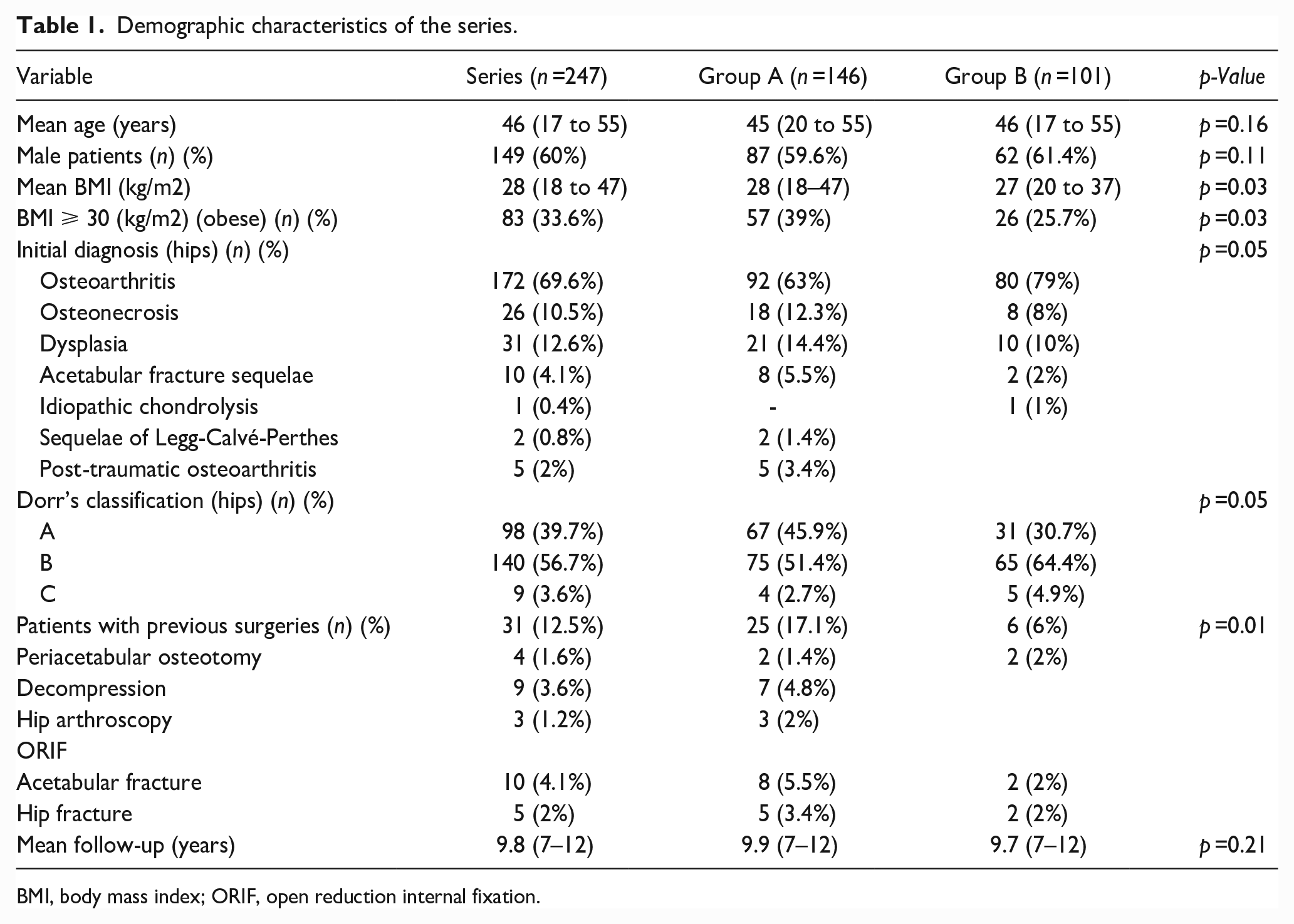
BMI, body mass index; ORIF, open reduction internal fixation.
Surgical technique
4 experienced hip surgeons performed all surgeries in laminar-flow theatres under epidural hypotensive anaesthesia through a posterolateral approach.
The CORAIL is a non-modular, non-anatomical, fully HA-coated, nonporous forged titanium alloy stem. It has a proximal trapezoidal cross-section and a tapered distal design. They were inserted in a broach-only technique with bone-preserving rasps. Lateralisation of the canal entry is essential to prevent varus alignment and undersizing. It is recommended to gradually enlarge the broach size until it contacts the medial and lateral cortices, obtaining axial and rotational stability. The prosthesis should be seated until the most proximal end of the coating surface is in line with the neck osteotomy. 17
The MiniHip stem is a short, partial column implant with neck-preserving osteotomy. 9 It is a calcar-loading stem with a rounded cross-section, classified as a type 2B, according to Khanuja’s classification. 18 The femoral neck osteotomy is done at the head-neck junction because bone stock preservation is needed for axial and torsional stability. 19 Implants are inserted in a slight varus position following the neck curvature and then orientated into the correct alignment, achieving cervico-metaphyseal fit. 16 Intraoperatively, we used Woolson’s method to calculate leg lengthening. 20 Implant sizes and bearing surfaces are summarised in Table 2.
Postoperative results.
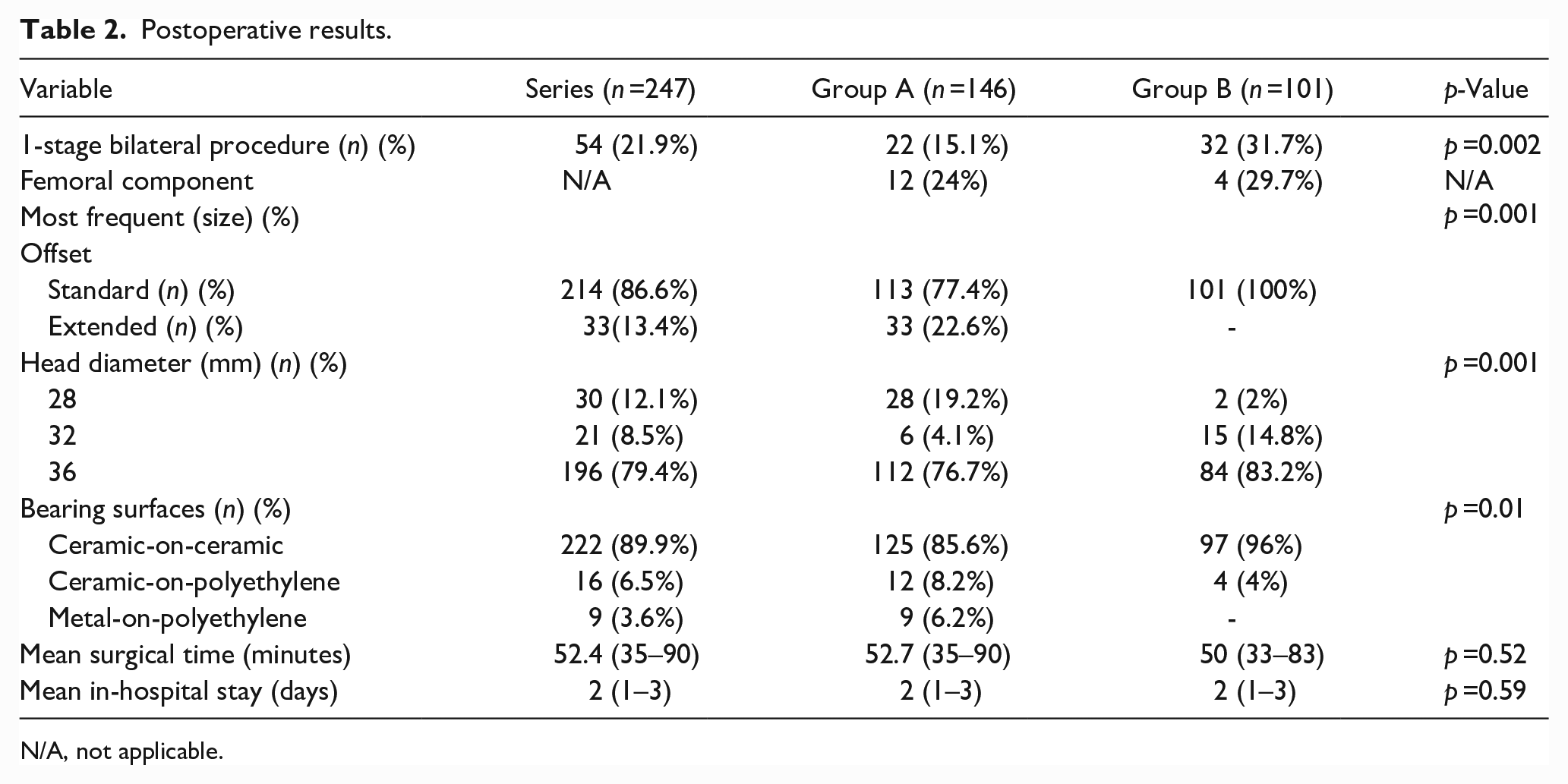
N/A, not applicable.
All patients received 3 prophylactic doses of intravenous cefazolin (1g/8hr). Routine thromboembolic prophylaxis was indicated during the first postoperative month, consisting of 40 mg subcutaneous low-molecular-weight heparin/day in patients with high risk and 325 mg aspirin/day in patients with low risk. 21 The same rehabilitation protocol for both groups included early mobilisation after surgery and ambulation with a walker and full weight-bearing for 15 days. Afterwards, we encouraged patients to progressively return to normal daily activities as tolerated with a cane for 15 days, depending on their clinical evolution and follow-up radiographs.
Clinical evaluation
The patients were reviewed at 2 and 6 weeks, 3 months, 1 year, and yearly thereafter. Clinical outcomes were assessed pre- and postoperatively with the Harris Hip Score (HHS). 22
Radiological evaluation
Standardised supine anteroposterior (AP) pelvic radiograph with both hips in 20° of internal rotation and no abduction and lateral (L) radiograph of each hip were obtained immediately postoperatively and in each follow-up control. 2 independent observers not involved with the surgeries evaluated all radiographic measurements (FDD, CL), comparing the immediate postoperative control with those made at the latest follow-up.
Dorr’s classification was used to assess proximal femoral morphology. 23 Leg-length discrepancy (LLD) 24 and femoral offset (FO) 25 were measured on standardised AP radiographs. The femoral neck length was measured by measuring the distance between the lesser trochanter and the osteotomy level. The diaphyseal stem invasion was measured using the most distal end of the implant and the lesser trochanter. Regarding alignment, varus/valgus angulation was assessed by measuring the angle between the stem’s long axis and the long femoral axis. 26 A difference of >5° was defined as varus or valgus for Group A. As Group B stems preserved part of the femoral neck, varus alignment was not considered in this cohort.
A femoral radiolucency was defined as any irregular line between the implant and the bony interface, and periprosthetic osteolysis was defined as progressive bone loss >5 mm using Gruen’s classification. 27 Femoral stem subsidence was determined using Loudon and Charnley’s method. 28 Loosening was defined as subsidence >3 mm or a varus/valgus shift >3° around the stem. 29 Postoperative radiographs were evaluated to detect eventual progression. Stem fixation was assessed using Engh’s method, 30 and bone remodelling was assessed by measuring lateral cortex hypertrophy, femoral neck hypertrophy, and its resorption. 31 The Brooker classification was used to determine the extent of heterotopic ossifications, if any. 32
Complication rate analysis
We registered all complications according to the Dindo-Clavien classification. 33 Periprosthetic femoral fractures (PFFs) were categorised by Duncan and Masri’s classification.34,35 We considered a septic failure as any case requiring revision surgery due to a surgical site infection (SSI). We defined an aseptic failure whenever any revision surgery was performed for non-infectious causes, with the component’s consequent removal.
Statistical analysis
Continuous variables were expressed as means and ranges or medians and interquartile ranges (IQRs) depending on whether they had a normal distribution. Categorical variables were reported as frequencies and percentages. Continuous variables were compared using the independent-samples t-test, where data were normally distributed, and the Mann-Whitney U-test otherwise. Categorical variables were compared using chi-square and Fisher exact tests. Kaplan-Meier survival curves were estimated considering those complications that required revision surgery with implant removal as an endpoint. We performed a multiple regression analysis to determine independent risk factors associated with symptomatic metaphyseal femoral radiolucency, including statistically significant variables in univariate analysis or clinically relevant. Odds ratios (OR) were reported with their 95% confidence intervals (CI). Variables were considered statistically significant at the p-value < 0.05. All analyses were performed using Stata13 statistical software (Stata Corp., College Station, TX, USA).
Results
Clinical evaluation
There was no difference in mean surgical time and mean in-hospital stay between both groups. None of the patients in either group required a blood transfusion. There was a significant improvement in the HHS score when comparing preoperative and postoperative values in both groups (p <0.001). Mean HHS improved from 55 (34–78) to 92 (71–99) in Group A and from 54 (34–79) to 95 (75–99) in Group B, without differences between groups at the latest follow-up (p =0.26). Table 2 shows implant characteristics and postoperative results per group.
Radiological evaluation
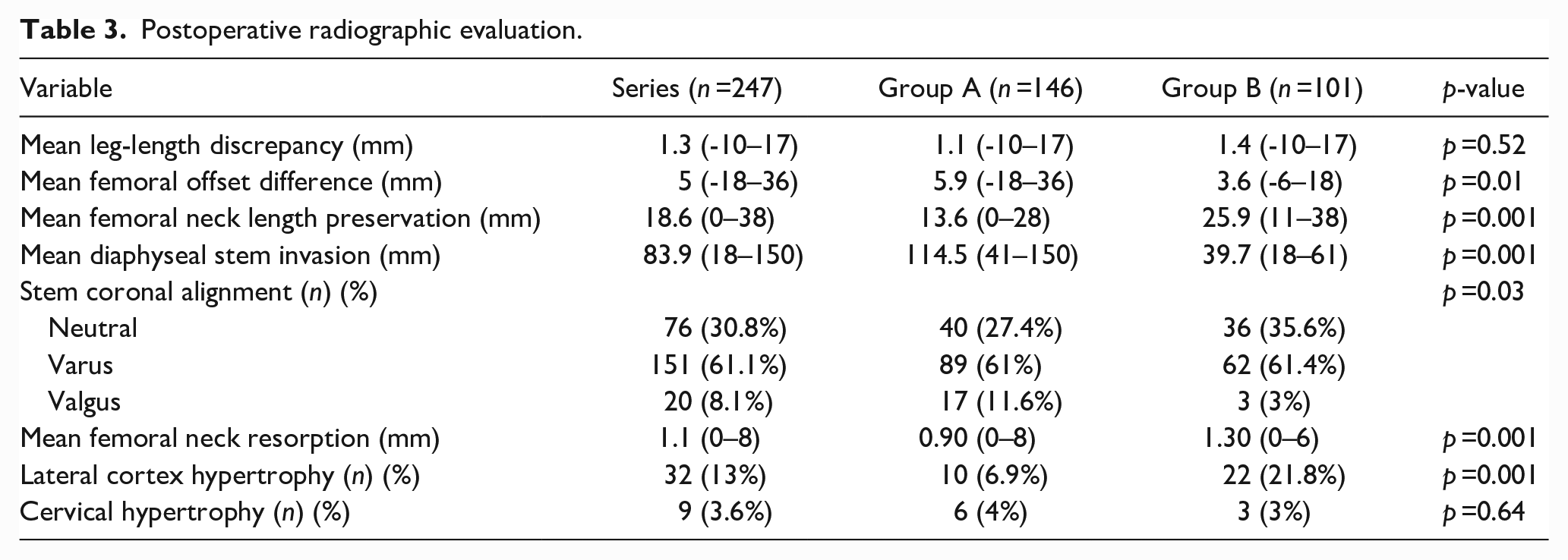
Postoperative radiographic measurements are summarised in Table 3. 5 (3.4%) THAs had symptomatic metaphyseal radiolucency around the stem in group A (p =0.06). They were all in Gruen zones 1, 7, 8 and 14 and were detected after the first postoperative year, with radiographic progression and clinical relevance during follow-up (Figure 2). There was no evidence of periprosthetic osteolysis around the femoral component in any group. 6 (4%) cases in group A and 5 (5%) cases in group B showed initial femoral subsidence <3 mm, without further progression, remaining asymptomatic to the latest follow-up (p =0.75). 5 (3.4%) and 2 (2%) patients in both Groups A and B respectively subsided at 4 mm and then stabilised, remaining asymptomatic to the latest follow-up (p =0.50).
Postoperative radiographic evaluation.
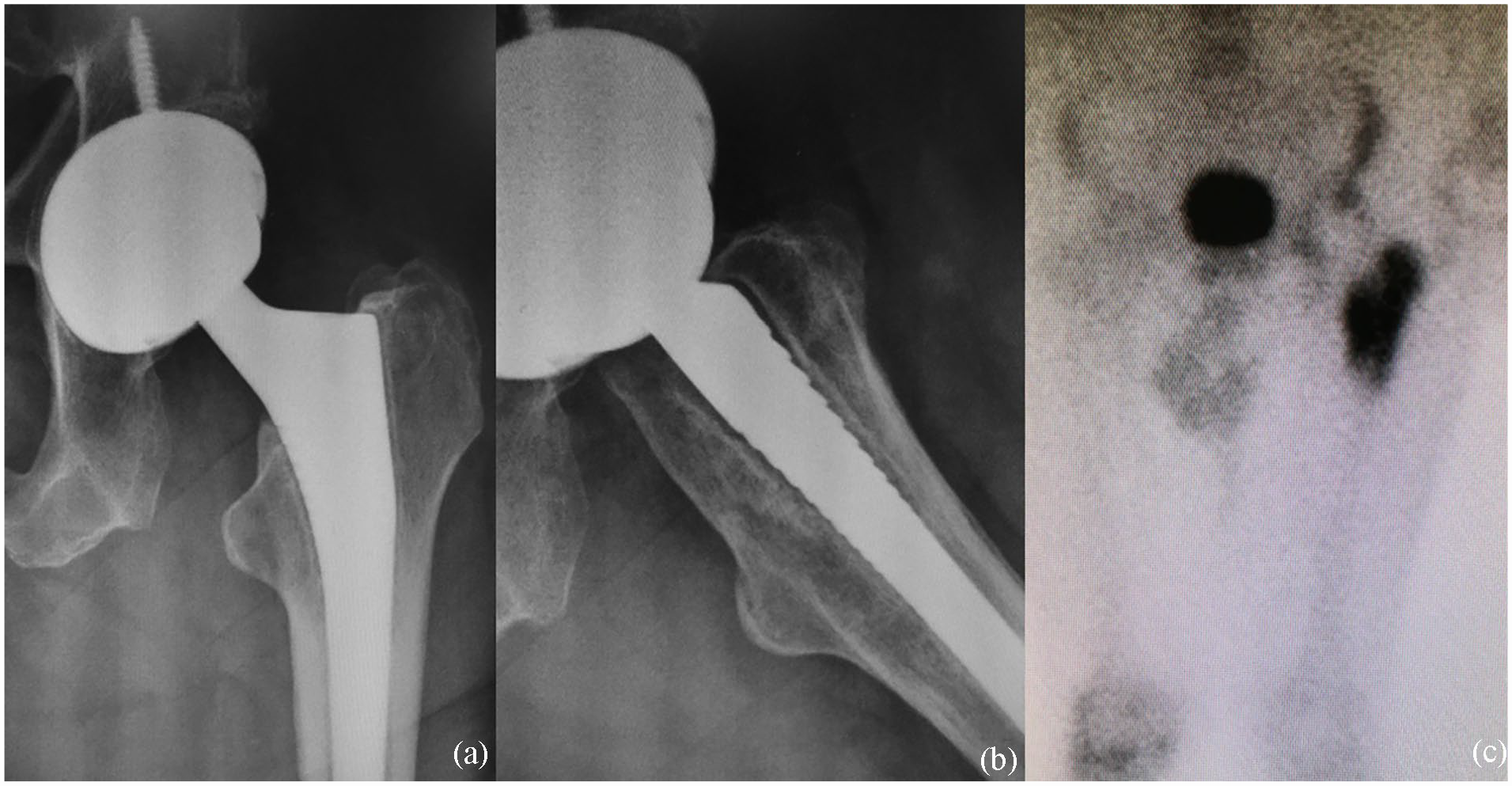
12-month (a) AP and (b) L radiographs evidence metaphyseal radiolucency in Gruen zones 1,7, 8, and 14 in a symptomatic patient and (c) the bone scan depicts hyperactivity in the proximal femur.
5 cases in Group A presented an aseptic femoral stem loosening, treated with 1-stage revision surgery (p =0.06), and 1 case suffered a septic failure that was surgically treated with a 2-stage procedure (p =0.41). According to Engh’s method, all remaining femoral components were fixed with signs of bony ingrowth. Lateral cortex hypertrophy was seen in 10 cases in group A and 22 in group B (p =0.001). Neck hypertrophy was evidenced in 6 cases of group A and 3 cases of group B (p =0.64).
Complication rate analysis
5 hips (3.4%) in Group A and 3 (3%) in Group B presented an intraoperative PFF (p =0.84). All of them except 1 were undisplaced calcar fractures without compromise beyond the lesser trochanter (Vancouver A2) and therefore were treated with cerclage wires and partial weight-bearing without sequelae. The remaining patient in group B was revised the same day to a conventional HA-coated stem (Metafix, Corin Group PLC, Cirencester, UK) due to the lateral cortex perforation (Vancouver A1). Intraoperative PFFs were unrelated to postoperative subsequent thigh pain, and all fractures healed without complications.
We recorded 13 (8.9%) and 1 (1%) postoperative complications in groups A and B, respectively (p =0.008). No significant differences were evidenced in PFFs, infection, or instability. 1 patient with a short stem had a Vancouver B2 PFF after an accidental fall 45 days after THA. The patient underwent 1-stage stem revision surgery with a modular uncemented fluted component (ZMR, Zimmer, Warsaw, IN, USA). Regarding infection outcomes, 2 hips in Group A and 1 in Group B had an acute SSI, which were successfully treated with debridement, antibiotics, and implant retention (DAIR). 1 patient (0.7%) in Group A had a single dislocation treated with closed reduction and prophylactic bracing for 45 days without further episodes of instability.
Symptomatic metaphyseal femoral debonding was evidenced in 3.4% of patients in Group A (5 vs. 0, p =0.06). All patients reported thigh pain during impact sports activities and activities of daily living. All cases are under follow-up, either awaiting surgery or without certainty to undergo the procedure. Table 4 shows the detailed complications in each group.
Detailed complications per period in each group.
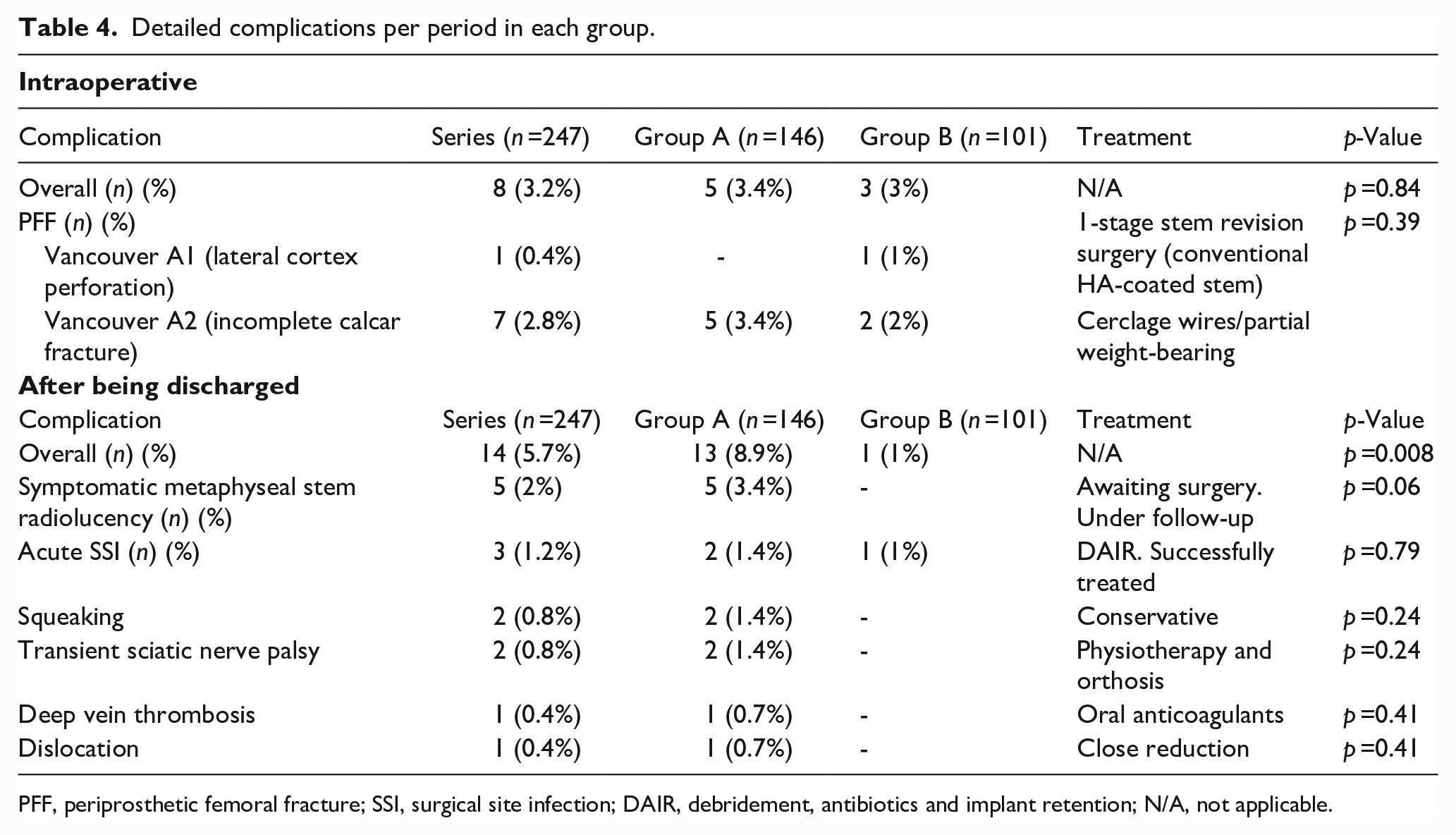
PFF, periprosthetic femoral fracture; SSI, surgical site infection; DAIR, debridement, antibiotics and implant retention; N/A, not applicable.
Aseptic stem loosening was more frequent in Group A than in Group B (5 [3.4%] vs. 0, p =0.06), with 4 patients being revised to a modular uncemented fluted stem (ZMR), and 1 to a long-cemented stem (Versys, Zimmer Biomet, IN, USA).
At a mean time of 9.8 years (123.5 months) of follow-up, taking revision of the stem for any reason as the endpoint, survival was 95.9% and 99% for groups A and B, respectively (p =0.15) (Figure 3). With aseptic loosening as the endpoint, survival rates were 96.6% and 100% for groups A and B, respectively (p =0.06). Table 5 shows stem failures in each group.
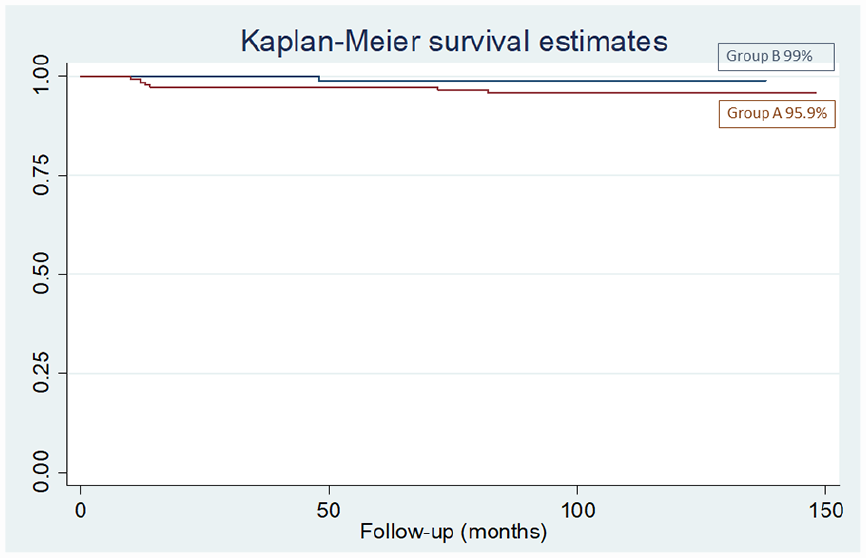
Kaplan-Meier curves. At a mean time of 9.3 years (116.3 months) of follow-up, taking revision of the stem for any reason as the endpoint, survival was 95.9% and 99% for groups A and B, respectively (p = 0.15).
Detailed stem failures per group.
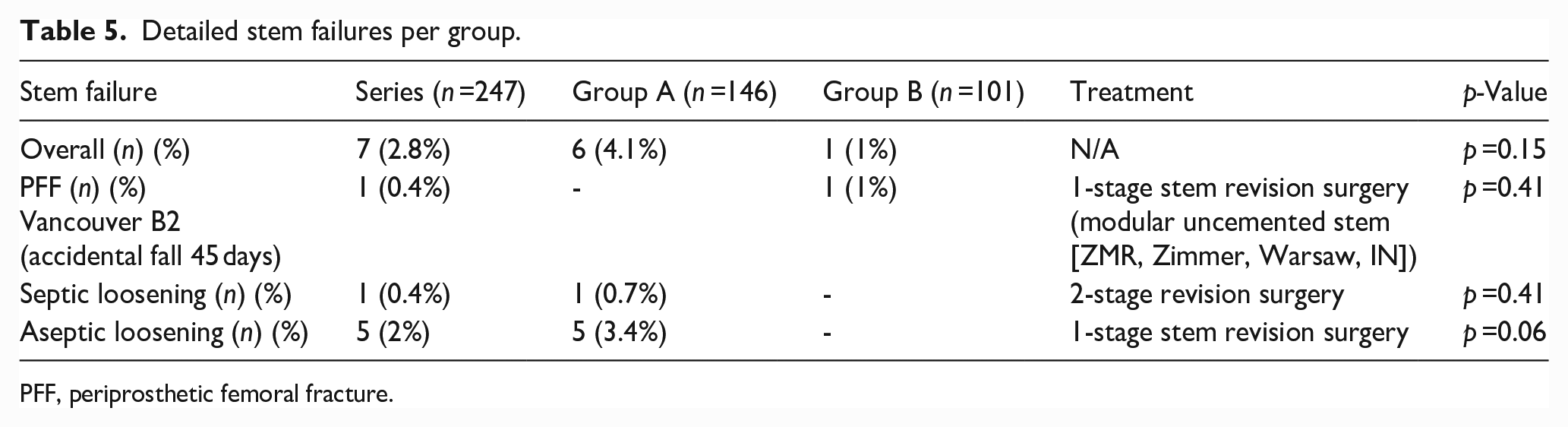
PFF, periprosthetic femoral fracture.
Variables associated with symptomatic metaphyseal femoral radiolucency
With regards to demographic variables, both groups had similar age (p =0.16), gender (p =0.11) and follow-up (p =0.07). In both groups, osteoarthritis was the most frequent preoperative diagnosis (92 [63%] in Group A and 80 (79%) in Group B, [p =0.05]), and Dorr B-type femur was the most prevalent [75 (51.4%) in group A and 65 (64.4%) in group B, (p =0.05)]. Statistically significant variables included mean BMI [higher in Group A compared to Group B (28 kg/m2 vs. 27 kg/m2, [p =0.03]), and patients with previous surgeries (25 [17.1%] in Group A and 6 [6%]in Group B, [p =0.01]) (Table 1).
Different postoperative variables were analysed, including implant characteristics and radiographic measurements. Regarding femoral stems, size 12 (24% [8–16]) was the most frequent in Group A and size 4 (29.7% [1–9]) in Group B. In both groups, standard offset stems were the most frequently implanted (113 [77.4%] in Group A and 101 (100%) in Group B, [p =0.001]), and ceramic-on-ceramic bearing couples were the most frequently used (125 [85.6%] in Group A and 97 [96%] in Group B, [p =0.001]). Statistically significant difference was observed in mean femoral offset (5.9 mm in Group A and 3.6 mm in Group B, [p =0.01]), mean femoral neck length preservation (13.6 mm in Group A and 25.9 mm in Group B, [p =0.001]) and mean diaphyseal stem invasion (114.5 mm in Group A and 39.7 mm in Group B, [p =0.001]) (Tables 2 and 3).
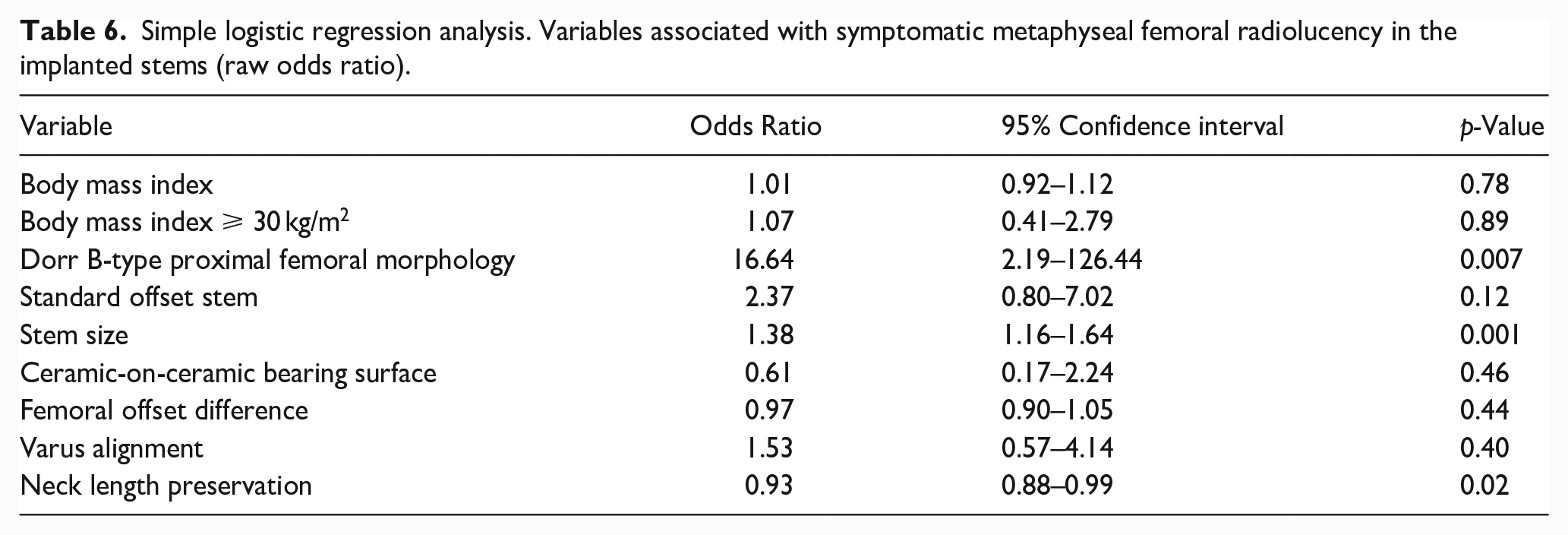
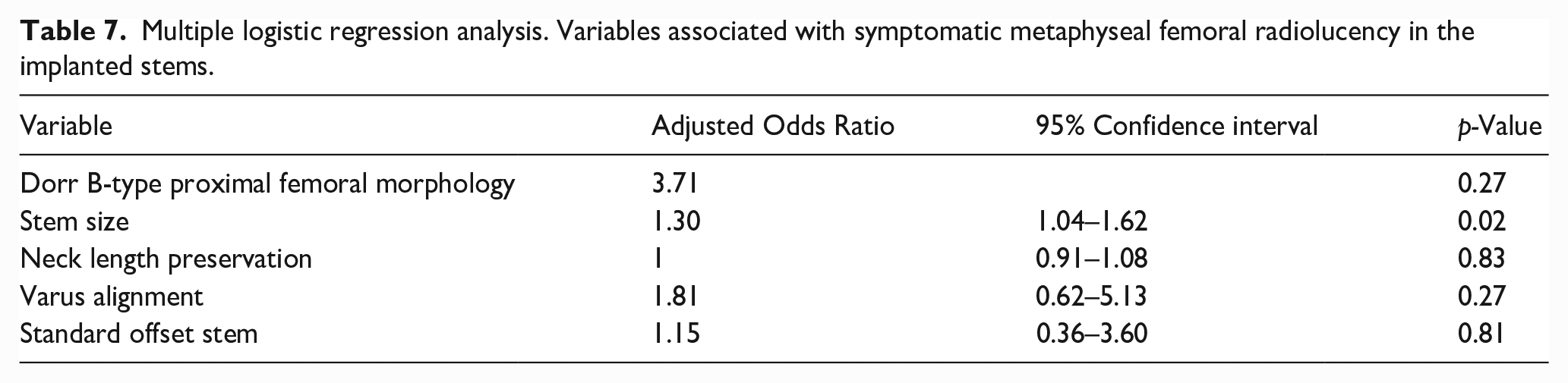
The simple and multiple logistic regression analysis results are shown in Tables 6 and 7. In the simple regression analysis, Dorr B-type femoral morphology was associated with a higher probability of symptomatic metaphyseal debonding when comparing Dorr B-type and not Dorr B-type stems (odds ratio [OR] 16.64; 95% CI, 2.19–126.44; p =0.007). However, it finally lost significance after adjusting for confounders (multiple, OR 3.71; 95% CI, 0.35–39.10; p =0.27). Smaller stem sizes, treated as a continuous variable, and considering that both groups had most medium stem sizes, were associated with a higher probability of symptomatic metaphyseal radiolucency in both regression models (simple, OR 1.38; 95% CI, 1.16–1.64; p =0.001) (multiple, OR 1.30; 95% CI, 1.04–1.62; p =0.02). While neck length preservation was a protective characteristic to avoid symptomatic metaphyseal radiolucency in the simple model (OR 0.93; 95% CI, 0.57–1.13; p =0.02), it lost significance after performing the multiple regression (OR 1; 95% CI, 0.91–1.08; p =0.83). No significant association was found between stem varus alignment and symptomatic metaphyseal radiolucency after adjusting for confounders (OR 1.81; 95% CI, 0.62–5.13; p =0.27). There was no significant difference in the incidence of symptomatic metaphyseal debonding between standard and high offset stem designs (multiple model, OR 1.15; 95% CI, 0.36–3.60, p =0.81).
Simple logistic regression analysis. Variables associated with symptomatic metaphyseal femoral radiolucency in the implanted stems (raw odds ratio).
Multiple logistic regression analysis. Variables associated with symptomatic metaphyseal femoral radiolucency in the implanted stems.
Discussion
In this comparative study, including 2 different stem designs in young patients, both designs presented similar intraoperative and perioperative complication rates, mean 9.8-year survival rates, and postoperative scores for pain and function, with a mean diaphyseal stem invasion of 114.5 mm in Group A and 39.7 mm in Group B.
Our study was not without limitations. First, its retrospective nature correlated with the biases exclusive to the study design. The sample size of the series resulted in a small number of cases included in both groups, restraining the production of more accurate statistical analyses. It can be argued that the lack of statistical significance observed in some of the variables analysed can result from a beta-type error (underpowered study). However, to our knowledge, it is the only study comparing the clinical and radiological outcomes of these 2 stem designs in primary uncemented THA. Second, implant selection depended on the surgeon’s choice, and we only evaluated a cohort of a specific conventional and short stem; thus, our results cannot be generalised to other designs. Third, our survival rates should be considered best-case estimates. Because there was a different follow-up period between both groups, we expect that some of these patients may yet undergo a revision arthroplasty for any reason at a longer follow-up. Fourth, this study has not analysed the effect of experience and surgical technique. Even though all surgeons involved were fellowship trained in high-volume centres, for the conventional stem group (Group A), 3 different surgeons performed the cases, while a different single surgeon performed the short stems (Group B). Fifth, we did not analyse the different HA coating between both stems. The conventional stem (Group A) is fully HA coated, while the short stem (Group B) has a roughened surface with HA coating without the involvement of the distal end. In this sense, the results might be influenced by the surface characteristics and not only by the stem design. Finally, the gold standard method for analysing initial implant stability is radiostereometric analysis, 36 or EBRA-FCA, 37 which can also measure stem subsidence without the need for tantalum markers using standard pelvic radiographs. Unfortunately, we could not perform this kind of evaluation due to the lack of resources in our centre when this study was developed.
The performance of short stems in primary THA has been investigated.38–40 A short femoral stem is desirable for bone preservation, especially in young patients. Physiological loading of the proximal femur may prevent stress shielding and preserve the bone stock of the femur. Since the life expectancy of THA may be less than the longevity of young patients, and a possible revision surgery might be needed, a partial neck-retaining short femoral stem could be an adequate implant in the case the performance of a time-proven stem is achieved. If this were the case, a short stem could be revised to a conventional stem, but to our knowledge, there is no evidence of this advantage in the literature.
Despite potential improvements in proximal loading, stress-shielding in the calcar and greater trochanter remains a problem for most designs at short to medium-term follow-up.41,42 Therefore, many studies investigated patients who underwent treatment with a femoral neck-preserving short stem to allow more proximal load transfer and reduce the stress-shielding effect.43,44 However, no studies directly compared specific femoral stems, such as a short and a conventional design after primary cementless THA.
In our series, symptomatic metaphyseal debonding was evidenced in 3.4% of patients with a CORAIL stem compared with 0% in the short stem group. Debonding of the CORAIL stem was defined in 2017 as an early metaphyseal loosening with a prevalence of 2%. 45 Risk factors for this complication in the original description were a Dorr B-type proximal femur, a BMI >25 kg/m2 and a hard-on-hard bearing surface. The higher prevalence in our series could be explained because of the percentage of obese patients in Group A (39%), Dorr B-type proximal femurs (56%) and ceramic-on-ceramic bearings (85%) of the Group A stems. However, 64% of the femurs in Group B presented this femoral anatomy, 95% of the stems in group B used this bearing surface, and no debonding was observed in this cohort. This complication was recently quoted in a study by the Norwegian Arthroplasty Registry, including >51,000 CORAIL stems and up to 30 years of follow-up. They observed 10-year survivorship free of stem revision (all causes including infection) of 97.6% (95% CI, 97.2–98.0%) for the standard collarless stem and 99% (95% CI, 98.8–99.2%) for the standard collared stem. 5 We could not perform a comparison because the collared version of this design arrived in our country in 2018.
Despite these findings, we found favourable clinical results with significant improvement in the HHS when comparing preoperative and postoperative values, without differences between both groups at the latest follow-up.
Our study found a 3.2% rate of intraoperative complications in both groups. 5 hips in group A and 3 in group B suffered an intraoperative PFF with no statistical significance. Molli et al. 46 retrospectively studied 658 THAs comparing a short-tapered stem versus a standard-length stem, and they observed a higher rate of intraoperative complications with the standard-length stem, with no difference in implant survival rates between groups at an 8–62 months follow-up. In our series, all of them except 1 were undisplaced calcar fractures without compromise beyond the lesser trochanter and were, therefore, successfully treated with cerclage wires without postoperative subsequent thigh pain.
Additionally, there was no difference between groups in terms of patient satisfaction, consistent with a previous meta-analysis and cohort studies with long-term follow-up.47–49
Conclusion
In this series, both conventional and short stems showed 96% and 99% implant survival rates and excellent functional outcomes after primary THA in young and active patients at a mean of 9.8 years follow-up. Complications and radiolucent lines were more frequent in the conventional stem group. Even though more robust evidence is required, and surgeons can use either of these designs, short stems might be a feasible alternative as they preserve more bone stock for a future revision in this group of active young patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.