
Abstract
Background:
COVID-19 infection first emerged in December 2019 in China and has since rapidly spread to become a worldwide pandemic. Orthopaedic surgery suffered a significant decline in the volume of surgical cases, while the orthopaedic trauma services maintained or increased the activity. Emergency operations for proximal femur fractures (PFF) in the elderly population assumed levels comparable to before the pandemic, with the 1-year mortality rate ranging from 14% to 36%.
Aims:
To determine whether patients with PFF affected by COVID-19 have a higher risk of postoperative mortality through a systematic review and meta-analysis.
Methods:
PubMed, Web of Science, Scopus and BMC were searched from January 2020 to January 2021 to identify original studies reporting the mortality in COVID-19 patients after PFF surgery. Study and participants’ characteristics, mortality rate and odds ratio (OR) were extracted. Risk of bias assessment was carried, and visual inspection of the funnel plot was used to assess publication bias. A random-effects model for meta-analysis was adopted.
Results:
Among 656 articles that came from the search query and hand-search, 10 articles were eligible after applying inclusion and exclusion criteria. Overall, the sum of the study participants was 1882, with 351 COVID-19 positive patients (18.7%) and a total number of 117 deaths, with an overall mortality rate of 33.3%. The mortality rate of COVID-19 positive patients varied from 14.8% to 60% and was higher than of those without COVID-19, with OR ranging from 2.424 to 72.00. The inverse variance method showed an OR = 3.652. All studies showed a statistically significant p-value.
Conclusions:
The postoperative mortality in hip fracture patients with concomitant COVID-19 was 3.65 times higher than the mortality in non-COVID patients. The currently available literature demonstrates that COVID-19 infection represents a substantial risk factor for postoperative mortality in the already susceptible hip fracture population.
Introduction
Coronavirus disease 2019 (COVID-19) first emerged in December 2019 in China and has since rapidly spread to become a worldwide pandemic. As of February 2021, there are more than 102 million cases and about 2 million deaths. 1
Healthcare systems have been uniquely affected. Elective surgeries were cancelled, non-priority healthcare services were postponed, directing all focus on COVID-19 patients, leading to reallocation of funds. 2 Hospital admissions due to other causes decreased.3,4 Orthopaedic surgery suffered a significant decline in the volume of surgical cases. 5 Orthopaedic trauma services have declined in some countries,6,7 but have maintained or increased activity in others,8,9 especially in elderly patients. 10 Emergent surgeries as proximal femur fractures (PFF) in the elderly population assumed levels comparable to before the pandemic, with the 1-year mortality rate ranging from 14% to 36%.11,12
Previous studies stated that earlier surgery was associated with a lower risk of death and lower postoperative pneumonia rates and pressure sores among elderly patients with PFF fracture. These results suggest that reducing delays may reduce mortality and complications. 11 However, those favouring a delay on the treatment of PFF defend the need to optimise the patients’ medical status (such as COVID-19 infection status), thereby decreasing the risk of perioperative complications.13,14 The question arises concerning the best medical practices for patients who have both hip fracture and COVID-19 at the time of presentation.
A previous systematic review on COVID-19 patients after hip surgery was carried out in September 2020, with data from the first wave of COVID-19, showing higher mortality of COVID-19 patients after operation. 15 However, as knowledge and more robust evidence arise from more multicentre studies throughout 2020, it is essential to review the information so that the evidence level is improved. Therefore, we need to determine whether patients with PFF affected by COVID-19 and go to surgery have a higher risk of mortality.
The objective of this study is to perform a systematic review and meta-analysis of the current literature reporting on the early outcomes of patients with PFF and COVID-19 infection who underwent surgical intervention. The meta-analysis aims to assess the risk of mortality in this patient population compared to non-COVID patients with PFF.
Methods
Search strategy and studies selection
For this systematic review and meta-analysis, a reviewing panel of 4 researchers searched electronic databases PubMed, Web of Science, Scopus, Biomed Central from January 2020 to January 2021 to identify original studies reporting the mortality in COVID-19 patients after proximal femur fracture surgery or providing data on the postoperative mortality. For this process, we used PRISMA guidelines, as showed in Figure 1.
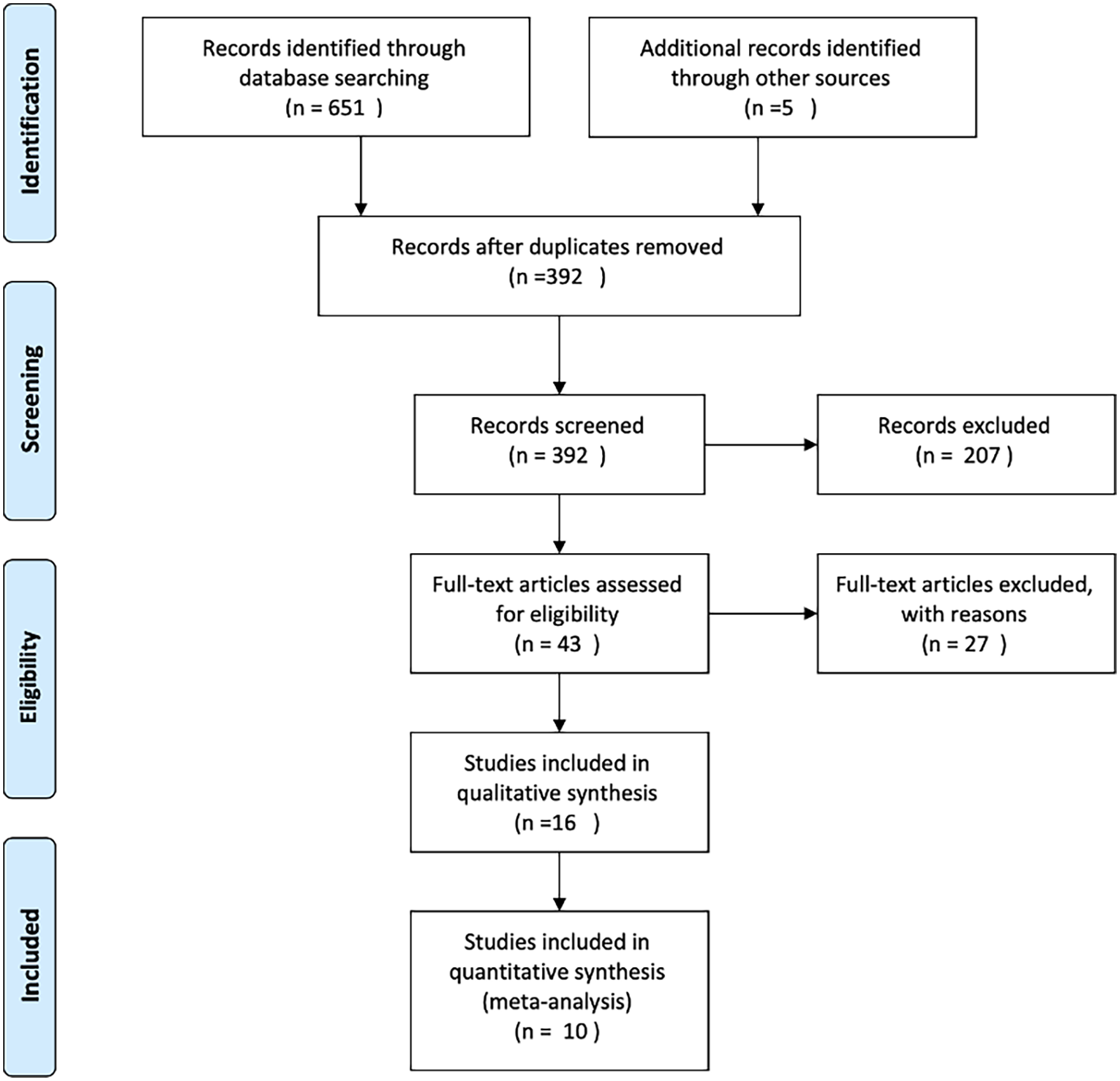
PRISMA flowchart of the search strategy and selection of studies.
The search query was defined:
(“COVID-19” OR “SARS-CoV-2” OR “Coronavirus” OR “2019-nCoV”) AND (“Fracture”)
Where it was possible, a more thorough search with MeSH Terms was carried out.
Search 1: “fracture” [MeSH Terms] OR “fracture” [All Fields]
AND
Search 2: “coronavirus” [MeSH Terms] OR “coronavirus” [All Fields] OR “COVID” [MeSH Terms] OR “COVID” [All Fields] OR “SARS-CoV-2” [All Fields] OR “2019-nCoV” [All Fields]
The inclusion criteria in this study were: (1) included COVID-19 patients; (2) related to trauma context; (3) all languages included. This last criterion was included so that language bias was minimised.
The criteria for exclusion of studies applied were the following: (1) do not have COVID-19 patients; (2) studies not involving humans (e.g., in vitro or animal research); (3) non-eligible publication types, such as review articles, editorials, comments, protocol study and guidelines or case reports; (4) drugs experiments/trials (5) presenting data in a non-eligible format or not possible to extract; (6) duplicate studies or evaluating the same sample; (7) other fields of work; (8) exclusively elective or another type of surgery.
The retrieved references were analysed independently in line with pre-defined criteria to determine eligibility for inclusion. The references’ lists of the systematic reviews of studies addressing the frequency of infection or its association with other outcomes were also screened to identify potentially eligible original reports further. When more than one report referred to the same study, the 1 presenting the results with more detail or providing data for the largest sample was considered, although any of the reports could be used to obtain information on the study characteristics. The disagreements between the reviewers in independent assessments were resolved by consensus or after discussion with another researcher.
The qualitative analysis phase was carried out by 3 people (JC, TF, AL) and reviewed by JC. This step evaluated the existence of the outcome of interest and its complete analysis, the control group (non-COVID patients), any possible duplication of participants across studies, and the existence of elective or any other surgery not related to proximal femur fracture.
Data extraction phase
Risk of bias assessment (RoB) was carried out by AI and JC, using the Cochrane Risk of Bias in non-randomised Studies – of Exposures (ROBINS-E), and robvis (National Institute for Health Research) for the graphic design of the RoB.16,17 The analysis of risk of bias consisted of 7 different domains: Domain 1 (D1) analysed for confounding factors; D2 checked for bias in the selection of participants into the study; D3 evaluated the bias of classification of exposure/intervention; D4 checked the existence of bias due to systematic differences in the intended exposure/intervention, while D5 would classify the studies according to the level of missing data; D6 is the domain related with bias in the measurement of outcomes and, finally, D7 is concerning the bias related with selective reporting of results from the study. 17
The data was extracted by 3 people (JC, TF, AL). Data collected included the characteristics of the study, namely type, duration and location of study, as well as patient’s mean age, the total number of patients submitted to surgery, number of patients with and without COVID-19, and the postoperative mortality in patients with COVID-19. Odds ratio (OR), 95% confidence intervals (95% CI) and respective p-values were collected. Due to its variability, these were converted to a logarithmic scale for data analysis purposes.
The qualitative synthesis was performed for mortality risk in patients with a proximal femur fracture affected by COVID-19 and submitted to the surgery. Most studies provided only crude odds ratios. For the1 study providing crude and adjusted estimates, the latter was used in the meta-analysis. A visual inspection of the funnel plots was used for assessment of publication bias.
A random-effect model for meta-analysis was adopted because we assumed a greater study-level variability due to differences between characteristics of studies and study populations. The weights were assigned for individual studies included in the meta-analysis on the basis of the inverse variance method.
In order to analyse and comprehend the reasons for heterogeneity, several forest plots were conducted using the different characteristics of the study, such as type of study, mean age, duration, and country of study.
Statistical analysis was conducted using MedCalc version 19.3 and IBM SPSS Statistics version 27 (IBM Corporation).
Results
Of the 656 articles that came from our search query from the 4 sources of information and hand-search, 392 were left after removing duplicates. After screening of the titles and abstracts for eligibility, 43 articles were promoted for full-text review. Only 10 articles were eligible after applying inclusion and exclusion criteria in the last phase.
Specific characteristics of each of these articles are present in Table 1. From the ten articles selected, three were prospective cohorts,18–20 while the remaining seven were retrospective.21–27 Half of the articles were conducted during one month,18,19,21,23,26 while 3 were conducted during two months,20,22,24 and the remaining had a 3-month span.25,27 As for the mean age, most of the studies had a mean age of patients >80 years old,18–21, 23 –26 except for two.22,27 Only two were conducted in the United States,20,26 whereas the remaining were conducted in the United Kingdom.18,19,21–25,27 Moreover, five studies showed the longer time from admission to surgery for COVID-19 patients,19–21,23,26 whereas only two had a shorter time for COVID-19.22,24 The remaining three did not specify the information for each of the groups.18,25,27
Included studies.
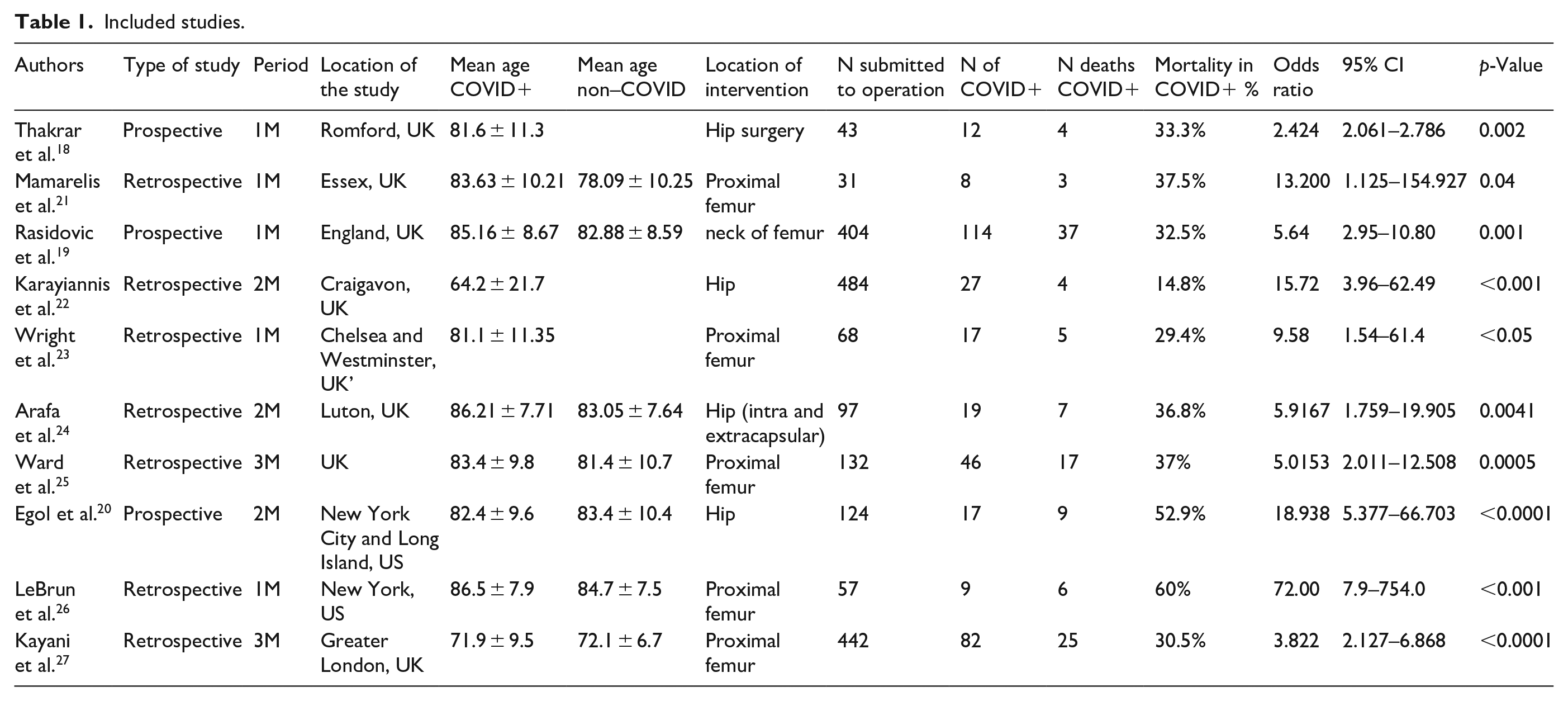
Overall, there were 1882 participants in the studies, with 351 COVID-19 positive patients (18.7%). From these, there were a total of 117 deaths, with an overall mortality rate of 33.3%.
Regarding the size of the studies, three studies had >400 participants submitted to surgery,19,22,27 while five had <100 patients.18,21,23,24,26
As for the results of the studies, our outcome of interest had different values according to the study and size of population. The mortality rate of COVID-19 positive patients was higher in all studies than of those without COVID-19. In these studies, the rate varied from 14.8% to 60%, with OR values ranging from 2.424 (95% CI, 2.061–2.786, p = 0.002) to 72.00 (95% CI, 7.9–754.0, p < 0.001). All studies showed a statistically significant p-value.
In order to understand the level of bias, we evaluated the risk of bias, (Figure 2) 16 which was fairly low, even though half of the studies had an overall risk of bias classified as low and the other half had a moderate risk of bias. Particularly in the domains, two of the studies showed high risk of bias in the classification of exposure and in the selection of reported results, respectively.
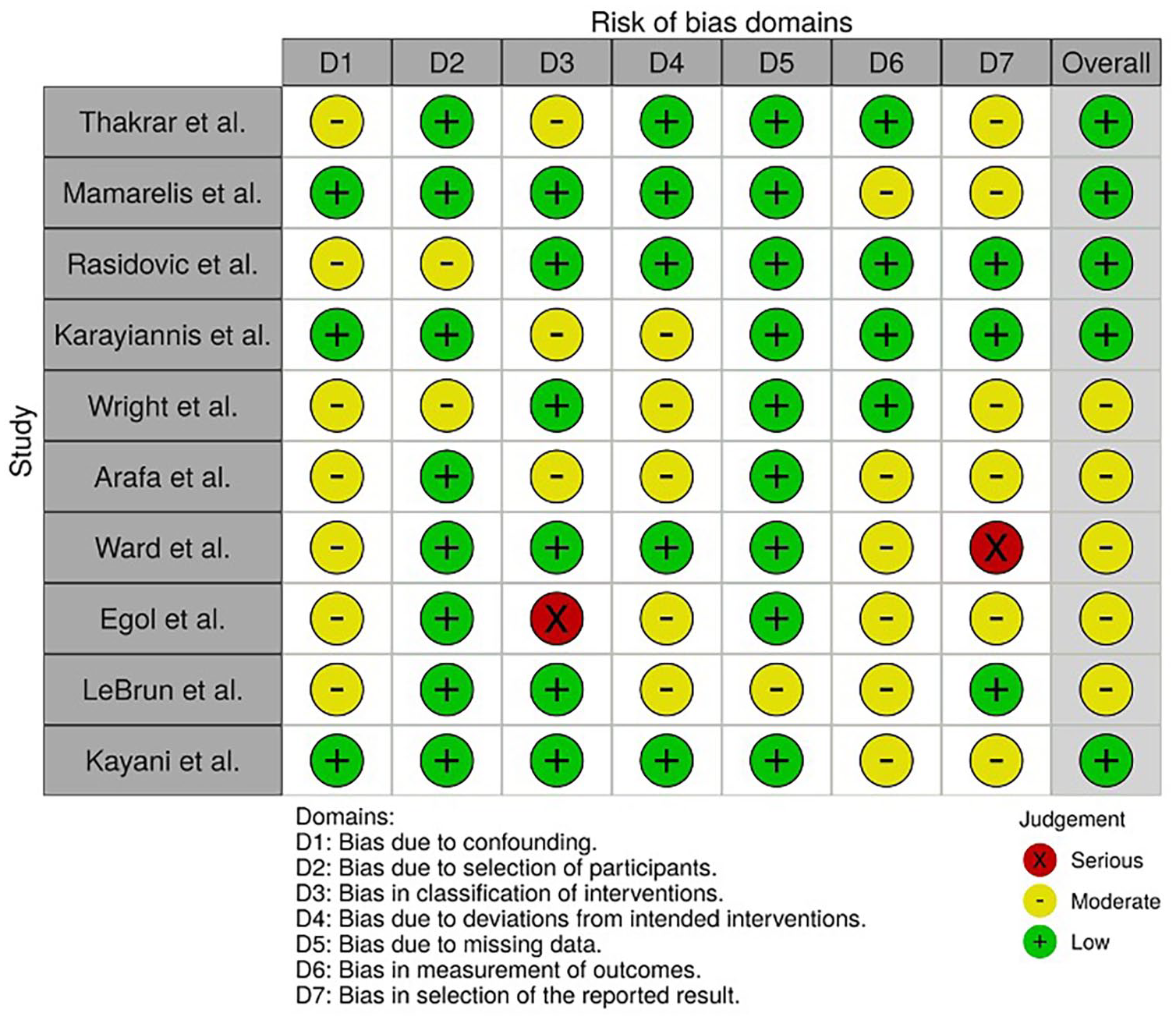
Risk of bias assessment in non-randomised studies, of exposures.
Furthermore, it was relevant to analyse the presence of publication bias. A funnel plot was drawn (Figure 3), using the logarithmic values of odds ratio (lnOR) and of standard error (SE), which showed a symmetric plot. Together with the funnel plot, the Egger’s regression test was calculated, with a p-value of 0.0486, with a 95% CI of (0.0128–3.261).
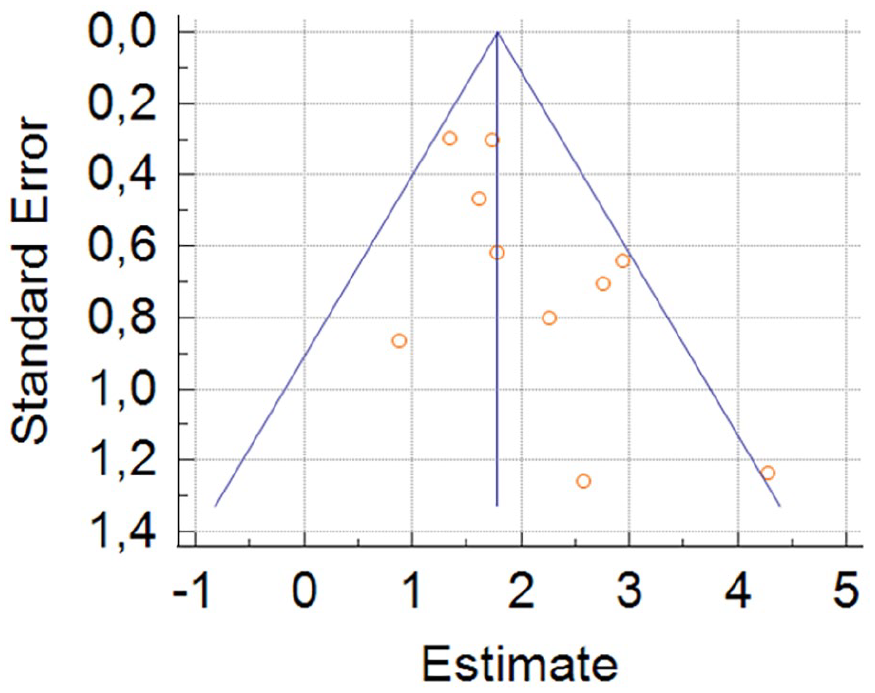
Funnel plot showing fair symmetry of the articles included in this review.
A forest plot was conducted (Figure 4) in order to understand the relative weight of each of the ten articles in our meta-analysis, which can be seen in the image below. The overall logarithmic OR of the studies was of 1.911 (95% CI, 1.473–2.349, p < 0.001). This corresponds to an OR of 3.652 (95% CI, 2.170–5.518).
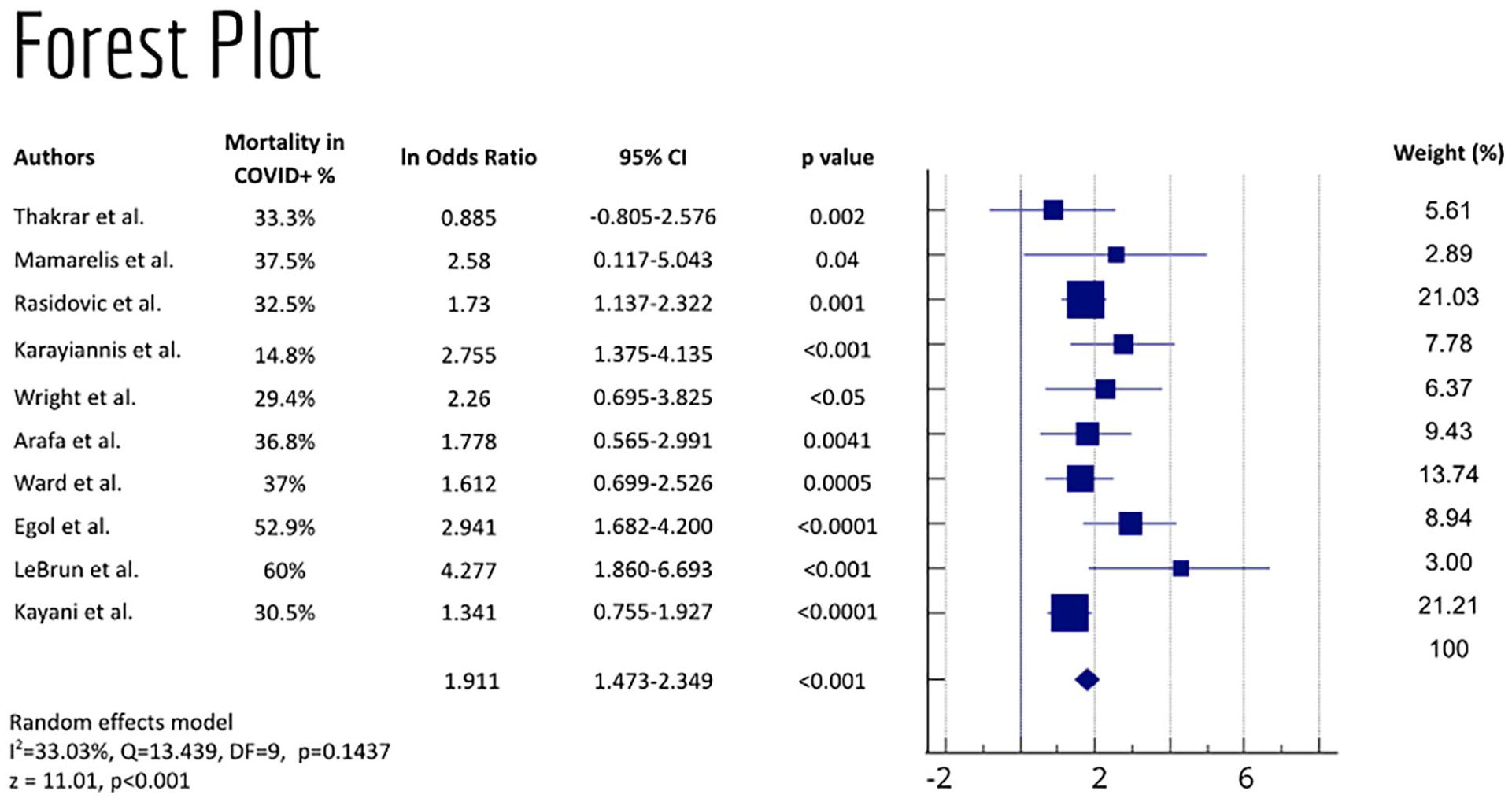
Forest plot of all the articles included in our study, and respective weights.
Regarding heterogeneity, this review presented a I2 = 33.03% (p = 0.1437), indicating a low level of heterogeneity. To comprehend the reasons for this heterogeneity, further forest plots were done taking into account the different characteristics, including duration and type of study, mean age of patients, and location where the study was conducted. Most of them are available in the supplementary material (Supplemental Figures 1 and 2).
The analysis per type of study, which were conducted via forest plots, showed an increased heterogeneity, with I2 of 33.64% in the 7 retrospective studies and I2 = 53.42% in the 3 prospective studies. Retrospective studies showed a lnOR of 1.659 (95%CI, 1.328–1.991, p < 0.001), while prospective studies had an lnOR of 1.912 (95%CI, 0.964–2.859, p < 0.001). Regarding publication bias, an Egger’s test shows stronger evidence of this bias in retrospective studies (p = 0.0066), being the opposite in prospective studies, with a p = 0.9286.
The forest plot for 1-month studies showed a lnOR of 2.005 (95% CI, 1.200–2.810, p < 0.001) and an increased I2 (32.00%), slightly lower than that of our initial analysis. An Egger’s test shows no evidence of publication bias (p = 0.3761).
The studies were also analysed according to age of participants included (Figure 5), which included eight articles with patients over 80 years old. For these, the lnOR present was of 1.97 (95% CI, 1.481–2.466, p < 0.001) and I2 = 21.84%, with an Egger’s test with no evidence of bias (p = 0.2027).
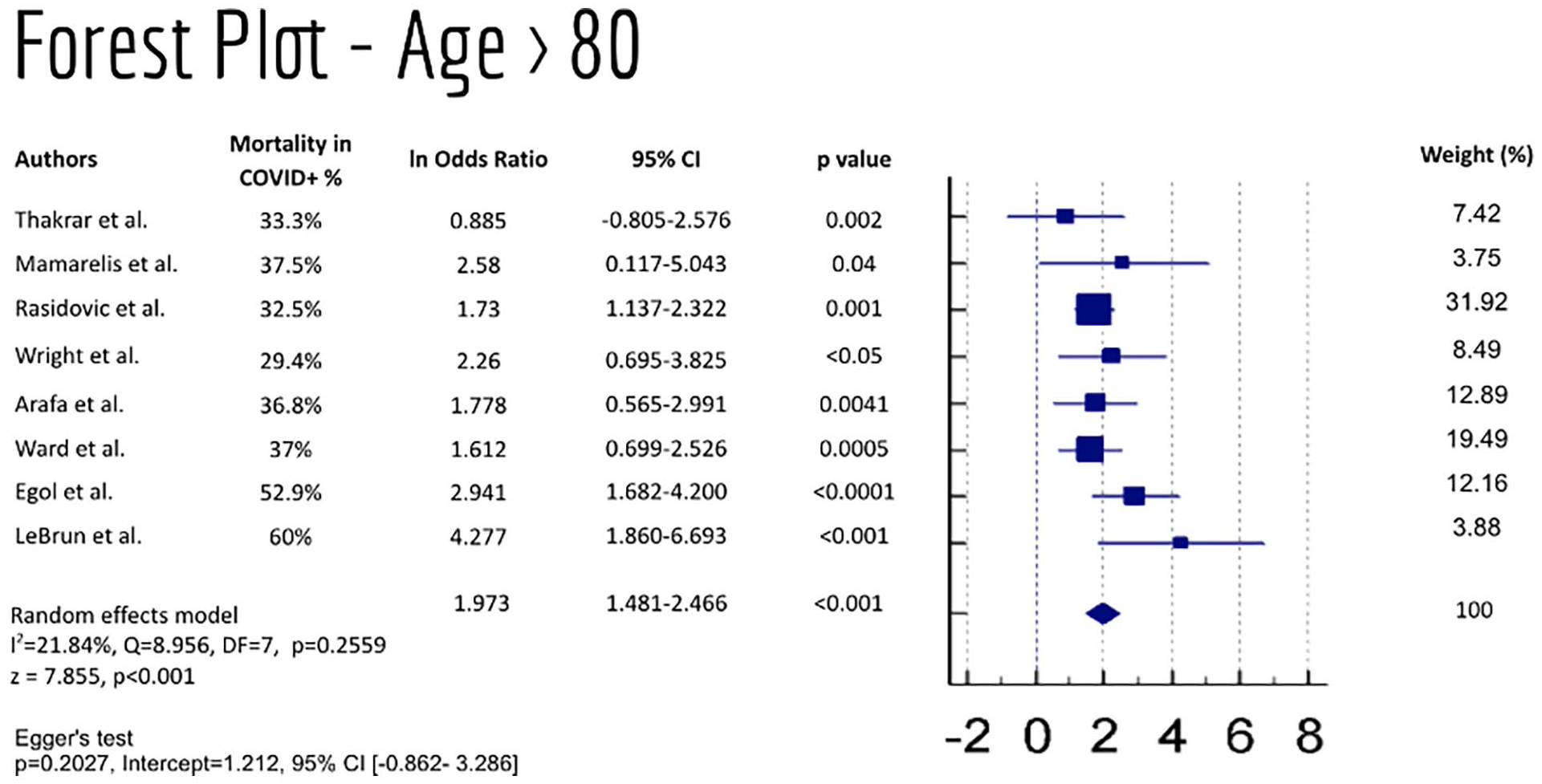
Forest plot of studies with patients with mean age >80, and respective weight.
Lastly, an analysis of the eight studies conducted specifically in the United Kingdom were sorted out for a forest plot (Figure 6). The respective lnOR was of 1.659 (95% CI, 1.328–1.991, p < 0.001), which corresponds to an OR of 2.752 (95%CI 1.764-3.964). The heterogeneity analysis showed a I2 = 0% in the random effects model, with a p = 0.591. The Egger’s regression test showed a p = 0.2256, showing no evidence of publication bias.
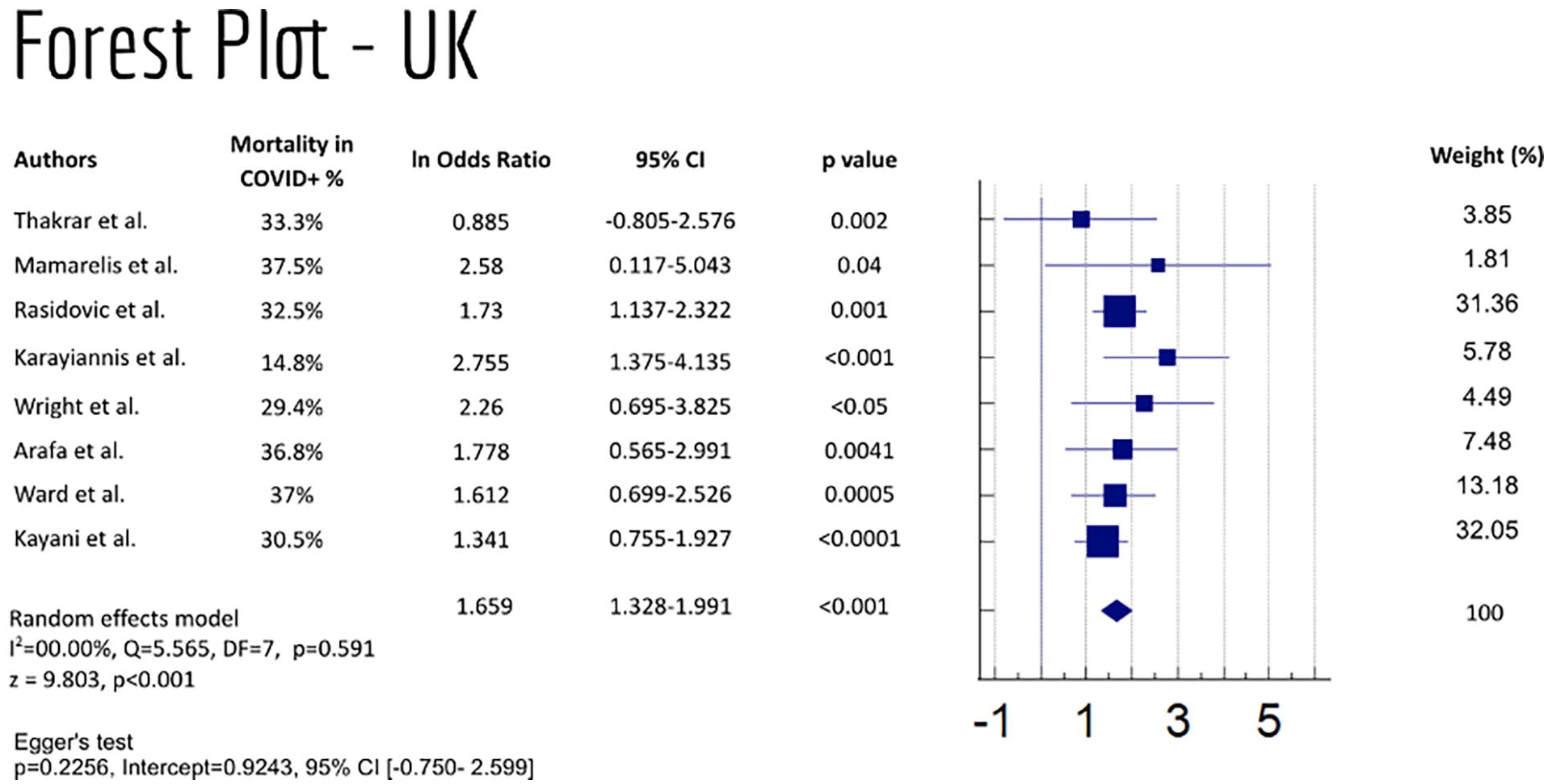
Studies conducted in the United Kingdom with COVID-19 patients submitted to PFF surgery, and respective study weights.
Discussion
This systematic review and meta-analysis measured mortality rate in patients with proximal femur fracture, affected by COVID-19 and submitted to surgery. The general population across studies covers 1882 patients, of which 351 presented COVID-19 infection. There was a fair representativeness (18.7%) in the patients’ overall population submitted to surgery treatment after PFF.
The risk of bias assessment indicated a moderate to low risk of bias, and the I2 = 33.03% demonstrated an acceptable level of heterogeneity. The meta-analysis demonstrated an OR between the two groups of 3.652 (95% CI, 2.170–5.518).
A heterogeneity analysis was conducted to understand the reasons for this variability. While the type and duration of study did not provide any answer for this, the participants’ mean age decreased the I2 to 21.84%, with a similar lnOR. The exclusive analysis of UK studies allowed to lower the heterogeneity to I2 = 0% (p = 0.591), with OR = 2.752. All these values support the stances that the COVID-19 infection contributes to a higher mortality rate in these patients, and that there might be country-level differences in the main outcome.
Therefore, the overall OR suggests that COVID-19 patients have a 3.65 times higher mortality risk after surgery for a proximal femur fracture compared to non-COVID-19 patients. This suggests COVID-19 is a contributing factor in worsening health status and consequently increasing the likelihood of death.
Another systematic review on hip fracture surgery used Risk Ratios to evaluate 10 studies in a pooled effect analysis, 15 obtaining a significant Risk Ratio of 5.66 (95% CI, 4.01–7.98), and a I2 = 30% (p = 0.17). These results are in line with our study on PFF surgery, despite the marginal effect of publication bias (p = 0.0486).
Across the selected studies, the time between admission to surgery varied, with half of the articles showing longer times until the start of the procedure.19–21,23,26 This might be related to the need for more protection measures in these patients and their stabilisation before surgery. However, some of the articles report shorter period until surgery for COVID-19 patients,22,24 which might also be related to the lower number of surgeries during the pandemic.
This study aimed to provide more robust evidence of the higher mortality of COVID-19 patients submitted to PFF surgery, having many strengths in the analysis conducted. We included individual hand search studies besides the ones from the 4 databases, allowing a more diverse set of articles in this review. Moreover, language bias was avoided by including all languages in our searches. It provided a heterogeneity analysis that allowed us to understand the existing differences. The authors conducted a rigorous process for selecting articles to obtain the studies that fulfilled our inclusion criteria and presented with the evidence needed for the comparison and further quantitative synthesis.
This review presents some limitations. The publication bias may influence the data selected to compose the meta-analysis. As expected, inaccurate studies, generally carried out with small sample sizes, may have its results influenced by chance. Another limitation of our study was that grey literature was not searched for, which might cause further bias.
In this review, we utilised combined information from prospective and retrospective studies. The COVID-19 infection increases mortality in both types of studies. However, one cannot determine whether an observed heterogeneity is due to a data collection or disease process from data alone. When such estimates are heterogeneous, likely causes of the heterogeneity include recall bias in retrospective studies. Such heterogeneity may provide interesting clues about data collection or disease processes for further examination.
Further research is needed to assess longer-term morbidity and mortality in this population and establish protocols on evaluating and treating these patients and evaluate the timing for the surgery, considering optimisation before surgery.
Conclusion
In summary, the postoperative mortality in hip fracture patients with concomitant COVID-19 infection who underwent emergency operative treatment was 3.65 times higher than the mortality in non-COVID patients who were submitted to the same emergency treatment.
The currently available literature demonstrates that COVID-19 infection represents a substantial risk factor for postoperative mortality in the already susceptible hip fracture population.
As information related to COVID-19 is constantly changing, more studies are needed to understand other characteristics related to morbidity and timing of surgery.
Supplemental Material
sj-pdf-1-hpi-10.1177_11207000221116764 – Supplemental material for Mortality in COVID-19 patients after proximal femur fracture surgery: a systematic review and meta-analysis
Supplemental material, sj-pdf-1-hpi-10.1177_11207000221116764 for Mortality in COVID-19 patients after proximal femur fracture surgery: a systematic review and meta-analysis by Tânia Freitas, Abdulrazak Ibrahim, António Lourenço and José Chen-Xu in HIP International
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.