
Abstract
Purpose
Cataract surgery is a fundamental procedure in ophthalmology, yet intraoperative complications such as anterior vitrectomy can compromise surgical outcomes. This systematic review and meta-analysis (CRD42025637001) aim to compare the incidence of anterior vitrectomy in cataract surgeries performed by ophthalmology residents versus experienced surgeons and assess factors contributing to surgical complications.
Methods
A systematic search was conducted across EMBASE, MEDLINE, CINAHL Plus, Web of Science, ClinicalTrials.gov, PQDT Global, ARVO and AAO for studies published after 2000 that reported on anterior vitrectomy incidence in cataract surgery. Eligible studies included randomized controlled trials and observational studies. Meta-analysis was performed using STATA v. 18.0.
Results
Out of 1,190 screened studies, five studies (four retrospective cohort, one prospective cohort) involving phacoemulsification, extracapsular cataract extraction (ECCE), and femtosecond laser-assisted cataract surgery (FLACS) were included, encompassing a total of 4,918 cataract surgeries, and 208 anterior vitrectomy (AV) cases. The random-effects meta-analysis demonstrated a significant AV incidence for residents (ES = 0.04, 95% CI: [0.01, 0.06]), while the incidence for experienced surgeons was not statistically significant (ES = 0.03, 95% CI: [−0.03, 0.09]). High heterogeneity was observed among the included studies (I² = 92.1% for residents and I² = 96.7% for surgeons).
Conclusion
Residents may have a higher incidence of AV, highlighting the potential benefits of structured surgical training, early exposure, and mentorship in reducing intraoperative complications. Future research should explore simulation-based training and technology-assisted surgery to improve resident proficiency and patient outcomes.
Keywords
Introduction
Among 94 million blind or visually impaired people worldwide, cataract is one of the most common causes. 1 A WHO initiative in 2020 found that an estimated 15.2 million people above 50-years-old were blind, with an additional 78.8 million with moderate to severe visual impairment due to cataract. 2 Fortunately, most cases of visual impairment and blindness due to cataract are avoidable and reversible. 1
Enhancing surgical competence in cataract surgery is critical for optimizing patient outcomes, including shorter recovery time, enhanced visual outcomes, and reduced risk of complications. Intraoperative complications, such as posterior capsule rupture (PCR) and vitreous prolapse impede immediate success of the surgery, increases likelihood of additional procedures, and negatively impacts visual outcomes.3,4 Therefore, minimizing these intra-operative complications is a critical piece of the training and development of cataract surgical competence.
Unplanned anterior vitrectomy is typically performed in cases of intraoperative complications, such as PCR with vitreous prolapse. 5 As such, the incidence of anterior vitrectomy may serve as a proxy for the safety and efficacy of techniques and skills of the surgeons. 6 A lower incidence of anterior vitrectomy may suggest better preservation of the posterior capsule and fewer intraoperative challenges, reflecting higher surgical competence and technique. Furthermore, anterior vitrectomy has been found to be a major risk factor for severe complications, such as retinal detachment (RR 18.5), intraocular lens (IOL) dislocation (RR 21.1), endophthalmitis (RR 3.6), and cystoid macular edema (RR 17.3).7,8 Therefore, the incidence of anterior vitrectomy may serve not only as an indicator for intraoperative success but also has broader long-term impacts on patient outcomes.
Earlier exposure in training and more opportunities to perform cataract surgeries were found to be associated with less surgical complications among ophthalmology residents. 6 However, no literature to date has comprehensively examined the relationship between the incidence of anterior vitrectomy between ophthalmology attendings and residents. Thus, this systematic review and meta-analysis aims to address this gap. Through synthesizing existing evidence, this review seeks to bring highlight the importance of enhancing surgical practices and improving patient outcomes in cataract surgery.
Methods
Ethical statement
This systematic review and meta-analysis utilized data exclusively from published studies and did not involve human participants and therefore, did not require any ethical approval.
Study design
This systematic review and meta-analysis was registered with PROSPERO (registration number: CRD42025637001) and follows the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines. 9 A PICOT framework was developed to guide the review (Supplemental Table 1), focusing on adult patients undergoing cataract surgery by residents and experienced surgeons using various techniques, with the incidence of anterior vitrectomy as the primary outcome. Secondary outcomes included intraoperative complications, postoperative complications, patient recovery time and visual outcomes.
Search strategy
A search was conducted across the following electronic databases: EMBASE (Ovid), MEDLINE (Ovid), CINAHL Plus (EBSCO), Web of Science, ProQuest Dissertations and Theses Global (PQDT Global), American Academy of Ophthalmology (AAO), The Association for Research in Vision and Ophthalmology (ARVO) and Clinical Trials.Gov covering the period from database inception to January 16, 2025. All records obtained were uploaded to Covidence (Veritas Health Innovation, Melbourne, Australia) for screening and management. No restrictions were applied to study design, language or year of publication.
The search strategy was developed in collaboration with a research librarian at the Schulich School of Medicine & Dentistry and validated by a senior researcher (MM). A sample search strategy and keywords for EMBASE (Ovid) are available in Supplemental Table 2.
Study selection
Studies were included if they were written in English, published after the year 2000 to reflect modern surgical techniques, involved adult patients (≥18 years old) undergoing cataract surgery, and reported outcomes regarding anterior vitrectomy and surgical outcomes. Eligible studies were those involving primary research such as randomized controlled trials (RCTs) or observational studies (case series, cohort studies etc.).
Screening of titles and abstracts were conducted independently by two reviewers (SA, FB). Full-text studies were retrieved and reviewed for eligibility, with reasons for exclusion documented (language, population, study design, intervention, outcome, date). Disagreements during the screening process were resolved through consensus or consultation with a third reviewer (XL). A PRISMA flow chart summarizes the study selection process for inclusion in the systematic review and meta-analysis (Figure 1).
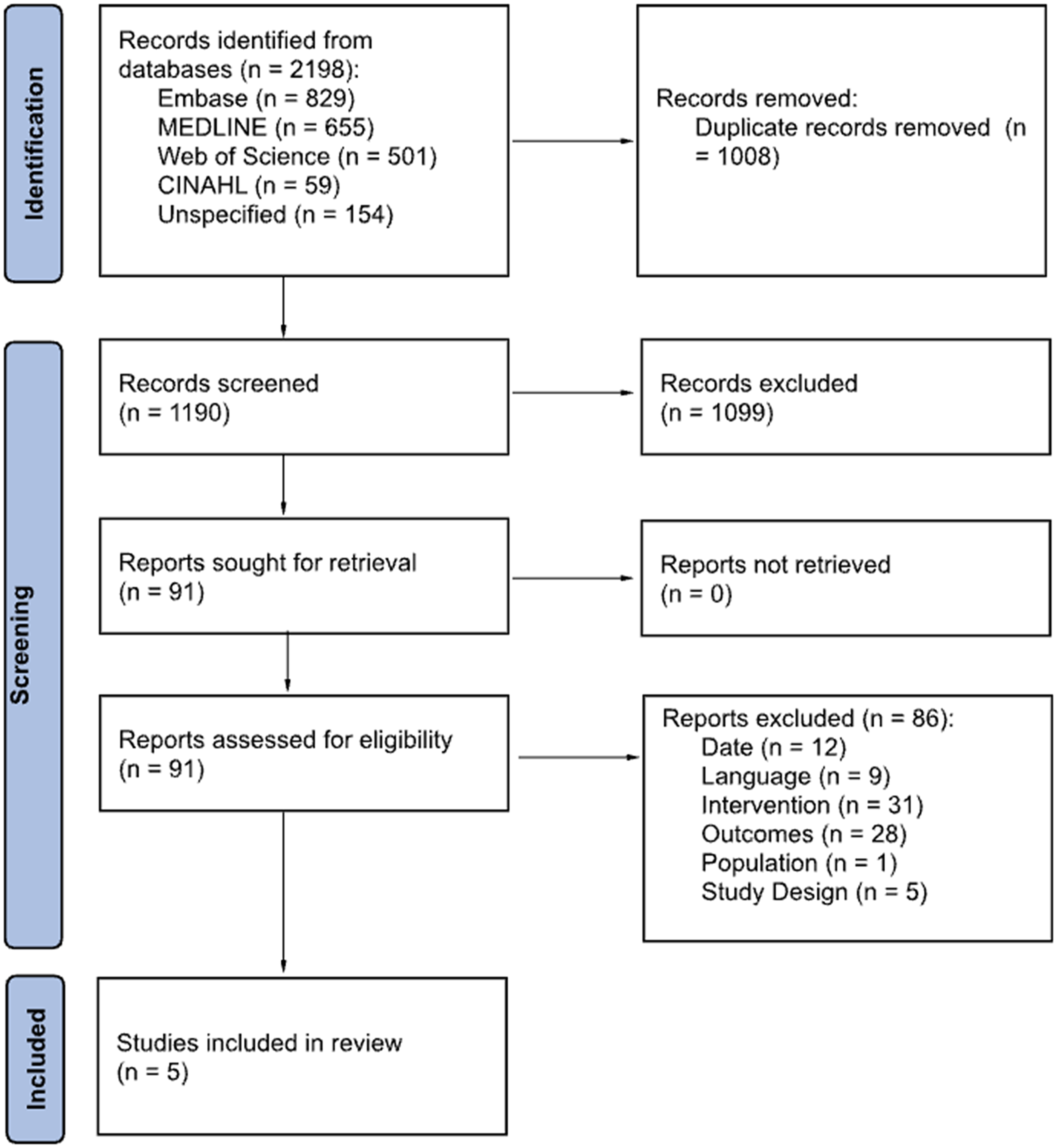
PRISMA flow diagram demonstrating the identification, screening and inclusion phases of the systematic review and meta-analysis.
Data extraction and synthesis
Data was extracted from the full-text screening by two independent reviewers (SA, FB) using predefined data extraction forms. Data extracted included study characteristics (authorship, publication year, country, design, and sample size), patient demographics (age, sex, comorbidities), surgical techniques, and surgical outcomes. Regarding surgical outcomes, the following measures were extracted: incidence of anterior vitrectomy, risk ratios, odds ratios, hazard ratios, intraoperative complications, postoperative complications, visual outcomes, recovery time, and patient satisfaction.
A meta-analysis was completed using STATA v. 18.0 (STATA Corporation, College Station, TX, USA). Incidence of anterior vitrectomy in cataract surgery was the effect size (ES) in the meta-analysis. The results from the studies comparing the incidence of anterior vitrectomy in cataract surgeries performed by resident versus attending surgeons were synthesized. A random-effects model was chosen to address high heterogeneity amongst the included studies. Heterogeneity between and within studies was assessed using the I² statistic and the χ² test. High I² values and large χ² statistics indicated significant heterogeneity. Forest plots were produced to show the pooled estimates of the effect sizes for both resident and attending surgeons’ group. A funnel plot was created for the assessment of risk of publication bias.
Risk of bias assessment
The assessment of the risk of bias in studies included in the full-text screening were completed by two independent reviewers (SA, FB). For observational studies, the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool was utilized and assessed study quality for bias due to confounding, selection, classification of intervention, deviations from intended interventions, missing data, measurement of outcomes, and selection of the reported result (Sterne et al., 2016). Differences in bias assessment were resolved through consensus or consultation with a third reviewer (XL).
Results
Study characteristics
Figure 1 provides the PRISMA flow diagram summarizing the results of the literature search. From the 1190 studies, 91 were used for full-text assessment of which five met the inclusion criteria for statistical analysis. Four of the studies were retrospective cohort studies and one was a prospective cohort study. There was a wide array of different cataract surgery techniques that were used, three were phacoemulsification, one was phacoemulsification with extracapsular cataract extraction (ECCE), and one was femtosecond laser-assisted cataract surgery (FLACS). Although secondary outcomes were part of the protocol, consistent data were not reported across the included studies to permit synthesis or meta-analysis. Table 1 provides an overview of the data-extracted from all the studies.
Summary of the five included studies.
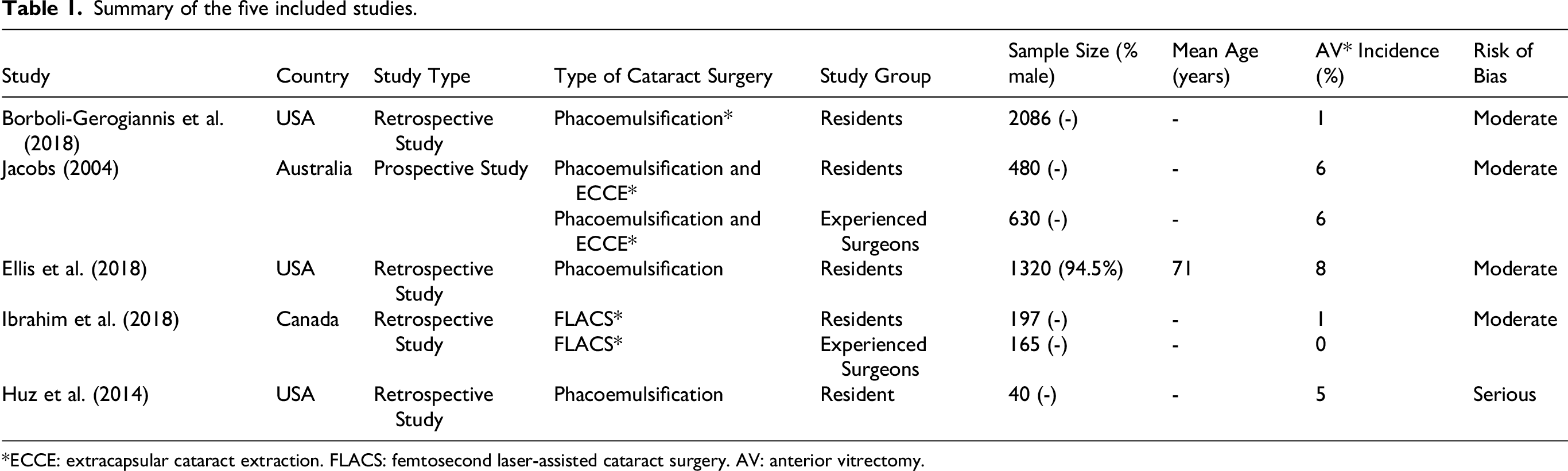
*ECCE: extracapsular cataract extraction. FLACS: femtosecond laser-assisted cataract surgery. AV: anterior vitrectomy.
Risk of bias assessment
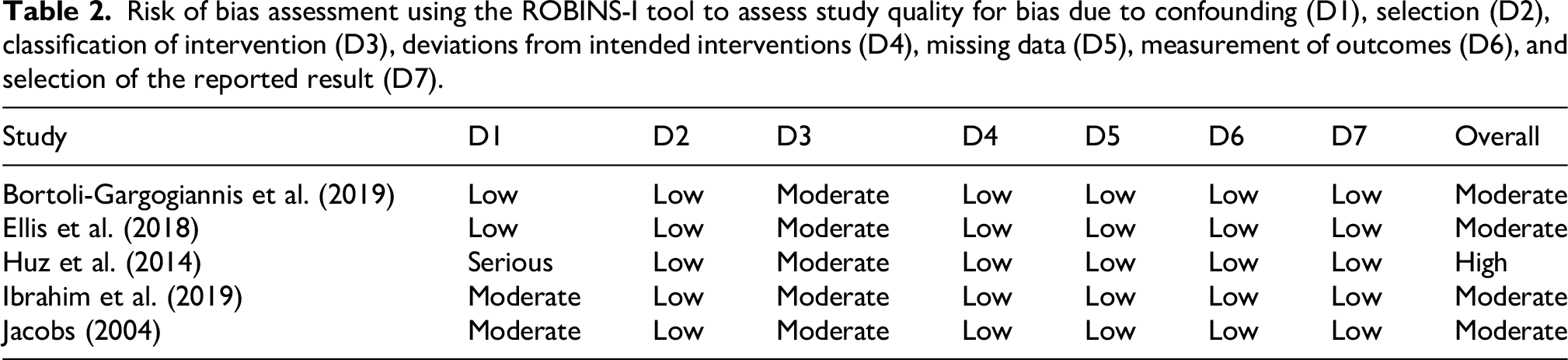
Table 2 shows the risk of bias assessment on the included studies. Overall, four studies were considered “moderate” risk of bias6,10–12 and one study was graded “serious” risk of bias. 13 The primary concerns across studies were related to bias due to confounding (D1) and classification of interventions (D3). Three studies were rated as having moderate or serious concerns in D1, largely due to limited control for factors such as patient complexity, surgical difficulty, or case selection differences.11–13 In addition, all five studies were rated as having moderate risk in D3, reflecting inconsistencies or insufficient detail in how surgeon experience (resident vs. attending) was defined and categorized.
Risk of bias assessment using the ROBINS-I tool to assess study quality for bias due to confounding (D1), selection (D2), classification of intervention (D3), deviations from intended interventions (D4), missing data (D5), measurement of outcomes (D6), and selection of the reported result (D7).
Meta-Analysis of anterior vitrectomy in cataract surgeries
Amongst the included studies, the total number of anterior vitrectomy cases were 208 of 4918 surgeries. The mean AV incidence was 4% for experienced surgeons and 3% for residents. Five studies provided information on the incidence of anterior vitrectomy in cataract surgeries performed by residents, and two provided information on surgeries performed by attending surgeons (Figure 2). Significant within and between study heterogeneity was observed among studies reporting on both residents (I² = 92.1%, p = 0.00) and attending surgeons (I² = 96.7%, p = 0.00). A clinically significant difference was observed for residents performing cataract surgery (ES = 0.04; 95% CI: [0.01, 0.06]). In contrast, a clinically non-significant difference was observed for attending surgeons (ES = 0.03; 95% CI: [−0.03, 0.09]).
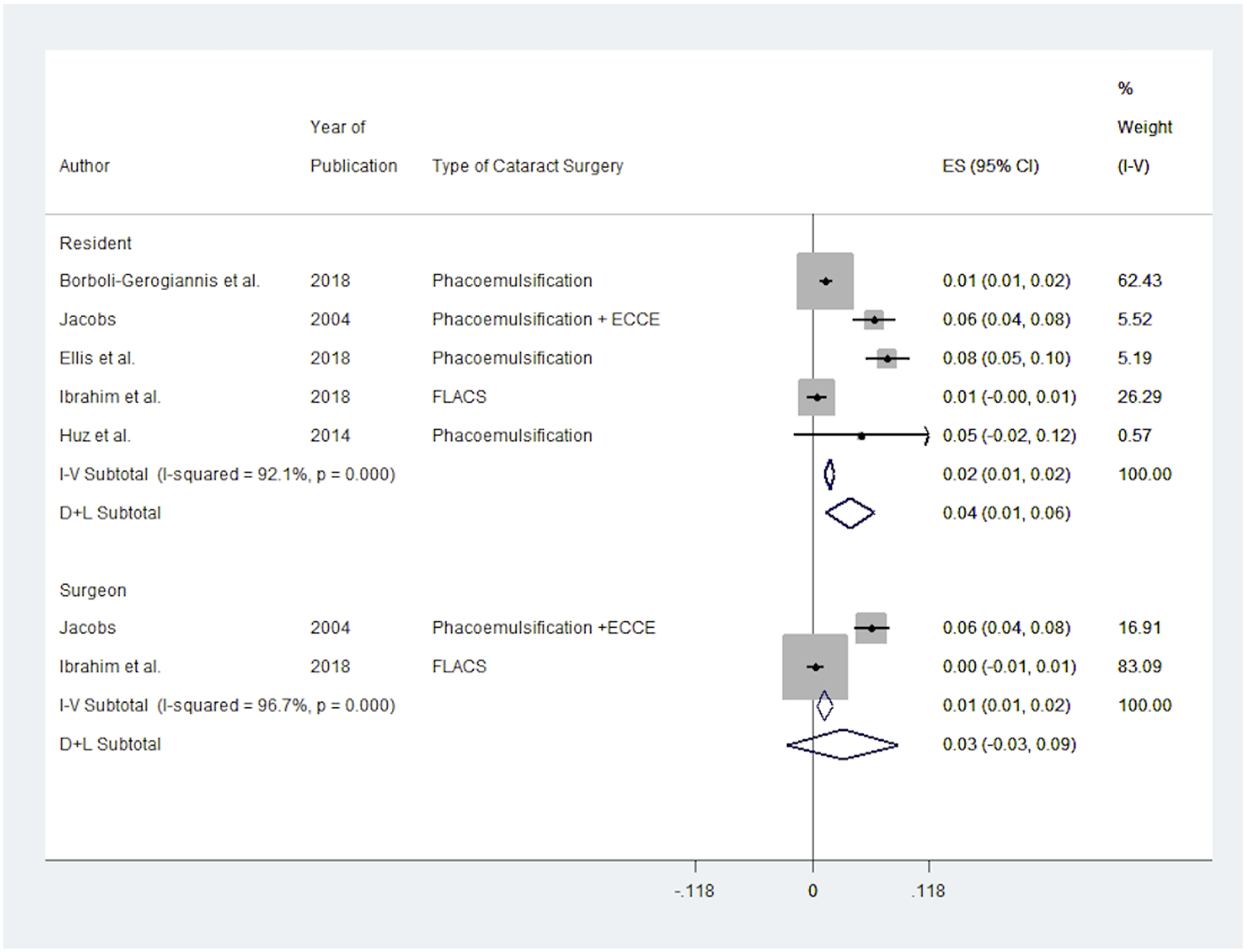
Forest plot of anterior vitrectomy incidence in cataract surgery between residents and surgeons. The pooled estimate indicates a higher anterior vitrectomy incidence among residents.
The funnel plot of the studies (Figure 3) demonstrates the incidence of anterior vitrectomy in cataract surgeries. Visual inspection of the plot shows studies scattered from top center of the plot to bottom right of the plot. Three studies are at the top along the central line of the plot and other studies are scattered from middle to bottom right of the plot. The funnel plot suggests a risk of publication bias, which may distort the findings in favor of positive outcomes.
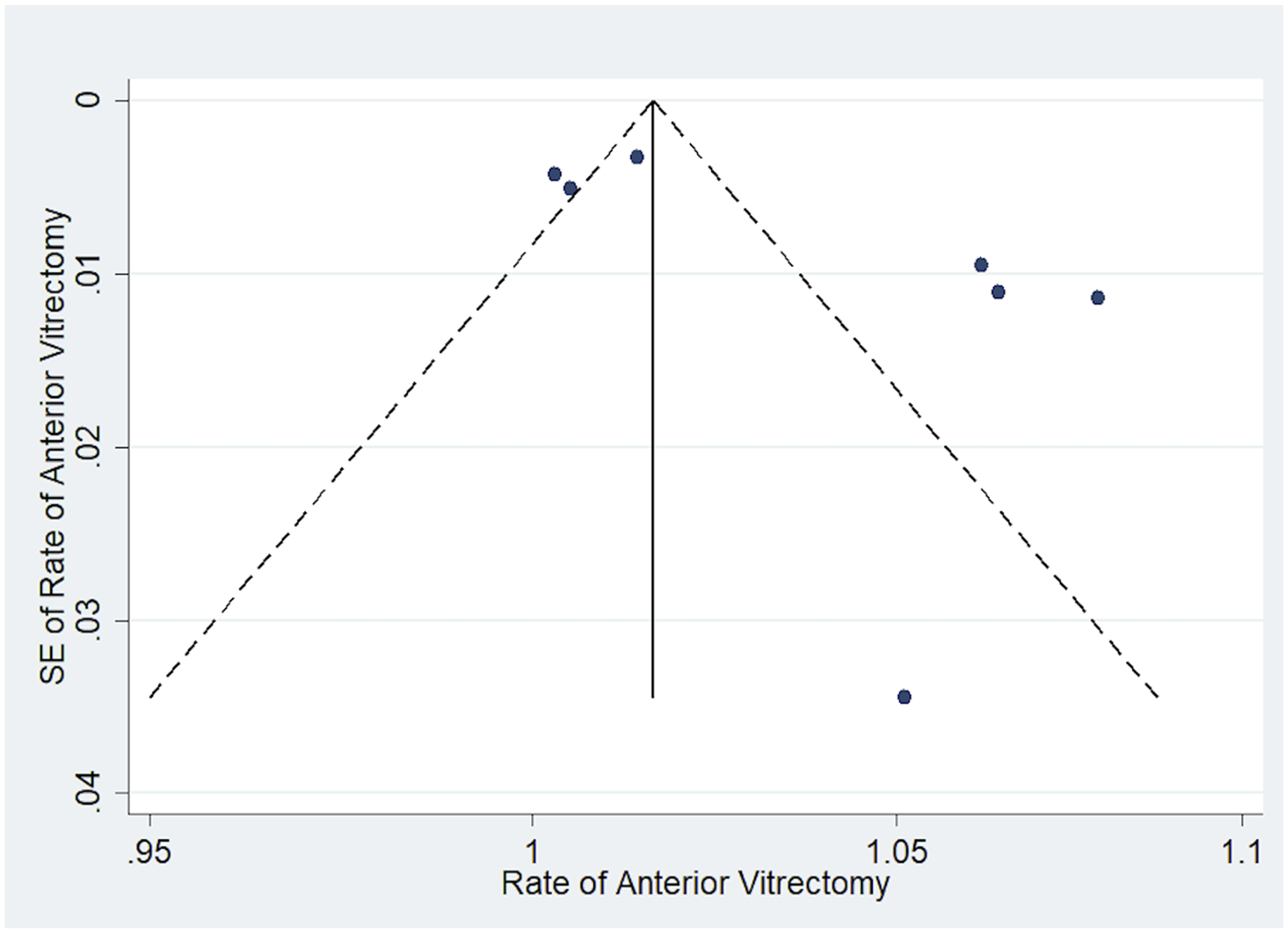
Funnel plot for publication bias assessment on anterior vitrectomy incidence. The distribution suggests heterogeneity, however, no strong evidence of bias is observed.
Discussion
This systematic review and meta-analysis examined the incidence of anterior vitrectomy in cataract surgeries performed by both residents and attending surgeons. The meta-analysis results indicated a significant incidence of anterior vitrectomy in cataract surgeries performed by residents, compared to a non-significant incidence in those performed by attending surgeons. These findings need to be interpreted cautiously due to high heterogeneity and the limited number of studies involving attending surgeons. While the difference suggests that residents may be more susceptible to complications during cataract surgeries, it highlights the importance of targeted training and supervision to improve surgical outcomes for residents.
Anterior vitrectomy, typically performed in cases of posterior capsule rupture (PCR) and vitreous prolapse, is a critical indicator of intraoperative safety and surgical competency.14,15 The potentially higher incidence amongst residents may reflect their relative inexperience and the learning curve associated with acquiring proficiency in cataract surgery. 6 A study by Balas et al. investigated the learning curve associated with cataract surgery and noted that basic surgical competency was achieved after 80 cases and the level of surgical finesse was achieved after 300 cases. This points towards the significant learning curve associated with cataract surgery and can explain why residents may have higher anterior vitrectomy rates. 16 Furthermore, a study investigating phacoemulsification and unplanned anterior vitrectomy found that anterior vitrectomy rates are higher amongst less experienced physicians. The investigators found that the rate of vitreous loss during cataract surgery was 2% by consultants, 4% by specialist registrars and staff grades, and 10% by senior house officers. 5 It is important to acknowledge other factors that may explain the higher incidence among residents. These can include greater case complexity in training settings, variation in institutional supervision policies, and the learning environment itself.6,10–13 Residents may also be selectively assigned more challenging patients (mature cataracts, pseudoexfoliation, or zonular instability), each of which increases the risk of intraoperative complications. Furthermore, residents may perform the more technically demanding portions of a procedure (e.g., capsulorhexis or nucleus disassembly), disproportionately exposing them to risk. Differences in supervision policies across institutions, as well as variability in documentation and complication reporting practices, may also influence recorded outcomes and AV incidence between groups.
Nonetheless, our study results could point towards the value of structured surgical training that emphasizes early skill development, adequate supervision, and simulation-based practice. For example, Borboli-Gerogiannis et al. reported a dramatic decrease in the rate of PCR and anterior vitrectomy (7.7% to 1.4%) following the implementation of a surgical curriculum that emphasized skills transfer using simulation tools, detailed case reviews, and immediate feedback. 10 Similarly, Ellis et al. highlighted those residents introduced to cataract surgery earlier in their training demonstrated significantly lower rates (2.1% compared to 7.6%) of anterior vitrectomy. This early exposure may have allowed residents to develop proficiency in a gradual manner, reducing the risk of major complications over the course of their training.6,17 Interestingly, the anterior vitrectomy rate in the early-exposure cohort remained stable at 1–2% throughout their entire training, supporting the notion of early skill development and greater case volume in achieving proficiency in cataract surgery.6,18,19 lastly, a prospective study by Jacobs showed that although trainees performed a great number of procedures (43.6 per 3 month rotation), they were able to remain comparable with consultants in terms of complication rates due to hands-on training and adequate supervision. 12
The variability in anterior vitrectomy incidence across the included studies underscores the impact of patient complexity and surgical technique. For instance, Huz et al. reported a relatively high 5% rate of anterior vitrectomy in resident-performed surgeries on challenging mature cataracts. 13 On the other hand, Ibrahim et al. showed that FLACS offers precision and reproducibility, potentially reducing complications when integrated into resident training. In particular, FLACS enabled consistent capsulotomy size and centration, reduced phacoemulsification energy and improved wound healing. However, the FLACS surgical technique came with challenges, such as suction breaks and capsular tags. 11 These findings suggest that patient selection, surgical approach, and the integration of advanced technologies play pivotal roles in determining surgical outcomes.
For residency programs, the findings of this review may have important implications for training and surgical safety. As demonstrated by Borboli-Gerogiannis et al. and Ellis et al., early exposure to surgical procedures and robust mentorship are critical for flattening the learning curve and reducing complications.6,10 Furthermore, the use of advanced technologies like FLACS could further enhance resident training by simplifying challenging surgical steps. 11 To minimize complications such as anterior vitrectomy, residency programs could continue to refine their training methodologies. Simulation-based training, including the use of high-fidelity surgical simulators, could offer residents an opportunity to practice critical steps of cataract surgery in a controlled, risk-free environment. 20 Additionally, enhanced supervision during live surgeries can ensure that residents receive real-time guidance and feedback. 21 Implementing competency-based curricula with clear benchmarks for skill acquisition can further ensure that residents achieve proficiency before advancing to more challenging cases. 22 lastly, incorporating exposure to high-risk scenarios, such as mature cataracts or zonular instability, can better prepare residents for managing complex intraoperative situations. 23 Overall, residency programs may need to invest in advanced training tools, standardized curricula, and supportive mentorship frameworks to ensure continued improvements in surgical safety and outcomes.
Limitations and future directions
The small number of included studies reduces the statistical power and generalizability of the results. However, our key objective was to comprehensively examine the relationship of the incidence of anterior vitrectomy between ophthalmology attendings and residents. Therefore, by synthesizing existing evidence, this review aimed to highlight the importance of enhancing surgical practices and improving patient outcomes in cataract surgery.
The random-effects model was computed to synthesize the outcomes due to significant heterogeneity (I2 > 90%) found among the included studies. Several factors may contribute to this variability. First, the included studies were conducted in different geographic regions, including North America, Australia, and Europe, where healthcare infrastructure, surgical volume, and resident supervision policies may differ. Second, differences in patient demographics, such as age, comorbidities, and cataract density, may have influenced the incidence of anterior vitrectomy. Similarly, the variability in surgical techniques across studies (phacoemulsification, ECCE and FLACS) may introduce additional complexity, as each technique carries unique risks and technical challenges. Lastly, institutional differences in defining and documenting anterior vitrectomy may have affected reported incidence. These factors collectively highlight the complexity of comparing AV incidence across heterogeneous real-world settings.
Although one included study was published in 2004, it was retained to enhance data representation. Importantly, this study employed phacoemulsification and ECCE, both of which remain relevant surgical techniques in the current era. 12 Nevertheless, we recognize that advancements in surgical technology over the past two decades, such as the adoption of continuous curvilinear capsulorhexis, improved phacoemulsification tips, and the introduction of divide-and-conquer techniques, may limit the generalizability of older studies to current clinical practice. In parallel, ophthalmology residency programs have undergone significant evolution, increasingly incorporating structured simulation-based training, wet-lab practice, competency-based assessments, and earlier surgical exposure.23,24 These improvements have likely contributed to a reduction in complication rates among contemporary trainees. Consequently, older studies may overestimate the incidence of AV and may not accurately reflect the outcomes achievable through modern training approaches and surgical standards.
Lastly, the lack of granular data on surgeon experience levels, patient characteristics, and surgical complexity limits the ability to explore subgroup differences and identify specific risk factors associated with anterior vitrectomy.
Future research should focus on addressing these limitations through prospective, multicenter studies, and RCTs that standardize reporting of intraoperative complications, surgeon experience, and patient demographics. Investigating the impact of advanced training interventions (virtual reality simulators and structured mentorship programs) could help identify strategies to further reduce complications among residents. Additionally, exploring the role of emerging technologies, such as real-time intraoperative guidance systems, may provide new avenues for enhancing surgical precision and safety.
Conclusion
In conclusion, the limited available evidence suggests there could be a higher reported incidence of anterior vitrectomy among residents. These findings suggest that there may be potential areas for improving resident education and surgical safety; however, conclusions should be interpreted with caution due to study limitations and variability. By thoughtfully addressing any potential gaps in training and standardizing research methodologies, the ophthalmology community could continue to advance surgical safety and optimize patient care.
Supplemental Material
sj-docx-1-ejo-10.1177_11206721251380886 - Supplemental material for Anterior vitrectomy incidence in cataract surgery among experienced surgeons and residents: A systematic review and meta-analysis
Supplemental material, sj-docx-1-ejo-10.1177_11206721251380886 for Anterior vitrectomy incidence in cataract surgery among experienced surgeons and residents: A systematic review and meta-analysis by Salem Abu Al-Burak, Fahad Butt, Xiaole Li, Amit X Garg, Cindy ML Hutnik and Monali S Malvankar-Mehta in European Journal of Ophthalmology
Footnotes
Acknowledgements
The authors thank Katie Holmes, librarian at the Schulich School of Medicine & Dentistry, for her invaluable assistance in developing and refining the systematic search strategy. The authors also acknowledge the support of the Pragmatic Trials Training Program at Western University.
Ethical considerations
This study is a systematic review and meta-analysis of previously published studies and did not involve new research with human participants, human tissue, or data. Therefore, ethical approval was not required.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Data availability
All data generated or analyzed during this study are included in this published article and its supplementary materials. No additional datasets were generated.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding was provided by Pragmatic Trials Training Program, UWO.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.