
Abstract
Introduction
To describe a novel surgical approach in the management of subluxated cataracts.
Methods
A 70-year-old Caucasian male with a subluxated cataract in the left eye was referred to our clinic at the Azienda Ospedaliero-Universitaria di Bologna- Ophthalmology Unit. The ophthalmic examination revealed a best-corrected visual acuity (BCVA) of 20/200 in the left eye with monocular diplopia and a severely subluxated NO6/NC6 cataract and the fundus examination did not reveal any vitreoretinal abnormalities. The right eye had 20/20 BCVA and was pseudophakic. After a 300° conjunctival peritomy, a single 25-gauge valved trocar 4 mm was inserted from the limbus in the inferotemporal quadrant, where the cataract was mainly dislocated and a corneal paracentesis to reduce the anterior chamber intraocular pressure was performed. Subsequently cohesive viscoelastic was progressively injected in the retrolental space through the trocar, to recenter and elevate the subluxated cataract. Thereafter, a complete centered capsulorhexis was performed, four capsular hooks were inserted to stabilize the bag, and complete phacoemulsification was performed with intact posterior capsular support. In the end, given the lack of capsular support elements such as the Cionni ring or Ahmed segment, a sutureless scleral fixated intraocular lens was implanted.
Results
One week after surgery, the BCVA was 20/25, and the final BCVA at 6 months was 20/20, without any complications.
Conclusions
Retrolental cohesive ophthalmic viscoelastic injection could represent a novel effective surgical approach in recentering and elevating subluxated cataracts, facilitating the capsulorhexis, and reducing the risk of a pars plana approach.
Introduction
Surgical management of cataract subluxation is challenging, as severe zonular dialysis can preclude the preservation of the capsular bag. Modified capsular tension rings (CTR) and Ahmed capsular tension segments (CTS) help promote stability of the IOL-capsule system in patients with severe zonular weakness, whereas standard CTR are largely used in moderate zonular dialysis.1,2 Adequate stabilization of the capsular bag-intraocular lens (IOL) complex is essential to preserve an intact posterior capsular diaphragm and minimize the risk of complications.3,4
Continuous curvilinear capsulorhexis (CCC) is largely considered the most important step in cataract subluxation, as any discontinuity in the capsule is a contraindication for CTR insertion.
Recently, Chee et al described a surgical technique in cases of posterior dislocation of the lens that consists in harpooning the lens with a 27 G needle bevel facing forwards to levitate the lens to its anatomical location and to perform capsulorhexis. 5 Moreover, Krix-Jachym et al described a sutureless surgical technique in which iris retractors were permanently fixed to the sclera to stabilize the capsular bag-IOL complex. 6
The present study aims to describe a new surgical approach that could represent an innovative technique in assisting surgeons with patients with cataract subluxation.
Methods
A 70-year-old Caucasian male patient with a subluxated cataract in the left eye was referred to our clinic at the University of Bologna Hospital. The patient had no concomitant diseases, and he did not report any previous trauma in the past weeks. The ophthalmic examination revealed a best corrected visual acuity (BCVA) of 20/200 in the left eye with monocular diplopia and a severely subluxated NO6/NC6 cataract, according to the Lens Opacities Classification System III (LOCS) grading system. 7 At the slit lamp examination, there were no signs of pseudoexfoliation syndrome in the anterior chamber, and the fundus examination did not reveal any vitreoretinal abnormalities. The right eye had 20/20 BCVA and was pseudophakic. The study protocol adhered to the tenets of the Declaration of Helsinki. Written informed consent, including consent to publish, was obtained from the participant. Ethical approval from the local Institutional Review Board “Comitato Etico di Area Vasta Emilia Nord” was not required for this study.
Surgical technique
Surgery was undertaken under peribulbar anesthesia. Two corneal marks at 0°–180° were applied and a 300° conjunctival peritomy was performed in preparation for a scleral fixated IOL implant.
After adequate diathermy, a single 25-gauge valved trocar 4 mm from the limbus was inserted in the inferotemporal quadrant, where the cataract was mainly dislocated. A nasal 1.2 mm paracentesis was performed to reduce the intraocular pressure of the anterior chamber. A 27G angled cannula was gradually introduced through the trocar in the retrolental space and simultaneously cohesive viscoelastic (Healon pro-Johnson & Johnson, Inc) was progressively injected. The lens subsequently appeared more centered and stable (see Figure 1). A main superior tunnel incision (2.25 mm) was performed. A complete centered capsulorhexis, with the progressive implant of 4 capsular hooks (MST Capsule Retractors, Chang Modification. MicroSurgical Technology Redmond, WA) placed through 4 paracenteses to stabilize the bag was achieved and complete phacoemulsification, with total removal of epinucleus and cortex, was performed with intact posterior capsular support. Then, since an Ahmed segment or Cionni ring were not available and a zonular disinsertion was present, a sutureless scleral fixated intraocular lens was implanted. No intraoperative or postoperative complications were encountered. One week after surgery, BCVA was 20/25, and the final BCVA at 6 months’ follow-up visit was 20/20, without any complications.
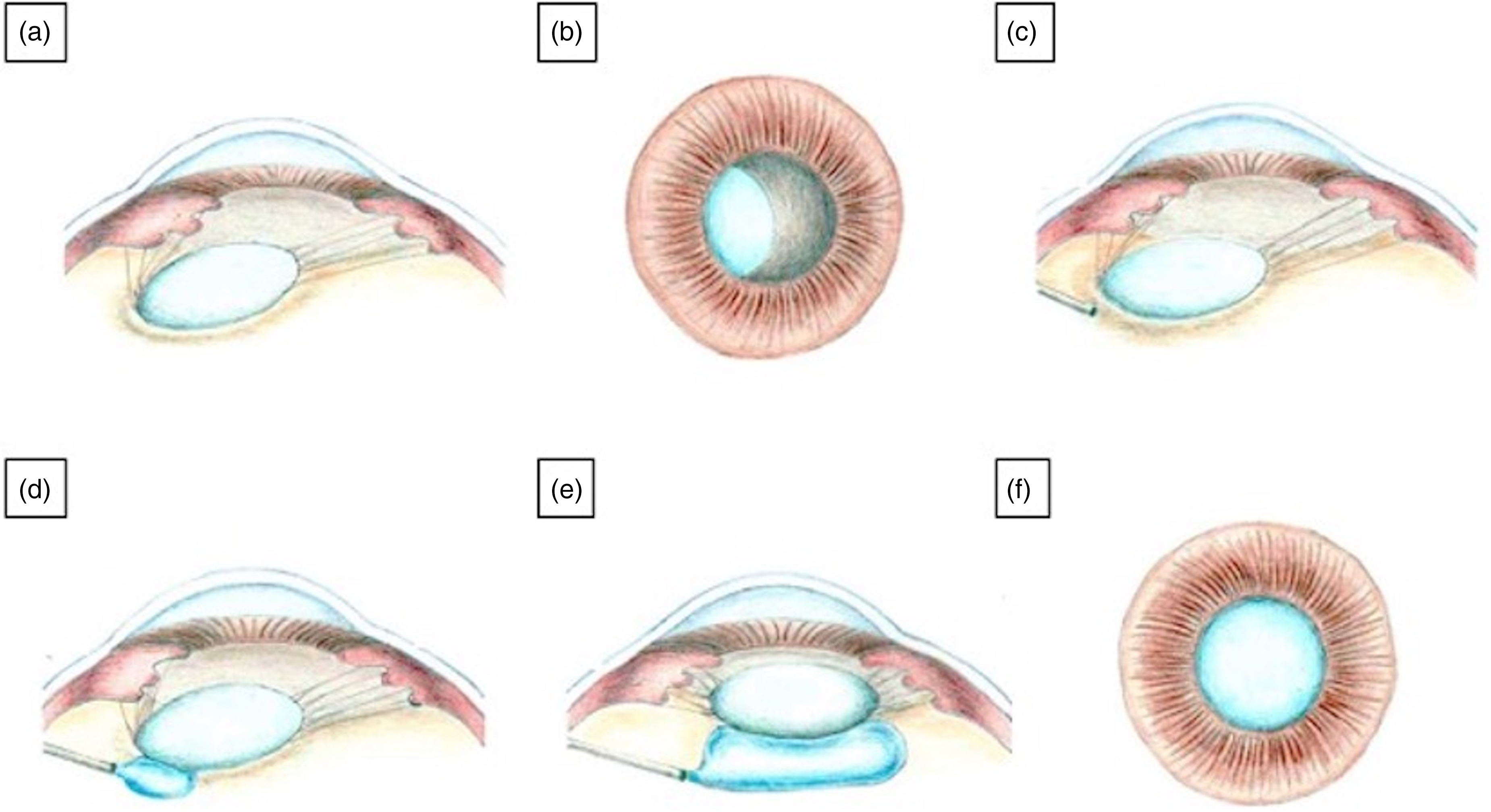
(a) and (b) Lens subluxation with a preserved capsular bag is depicted. (c) and (d) After insertion of a 27G angled cannula through a 25-gauge valved trocar 4 mm from the limbus, cohesive viscoelastic is injected in the retrolental space. (e) and (f) The lens is now more centered and stable, facilitating the capsulorhexis.
The associated Online Supplemental Digital Content 1 demonstrates the key steps of the surgical procedure. The surgery was performed by a single surgeon (D.I.).
Discussion
Surgical management of subluxated cataracts is challenging and the choice of the best surgical approach depends on the extent of zonular dialysis.
When the capsular bag is preserved and zonular dialysis is less than 90°, a successful surgical outcome can be obtained with careful surgery and inserting an IOL in the lens bag; however, in cases in which cataract subluxation is determined by a progressive disorder, a standard CTR should be placed. On the other hand, when zonular dialysis is greater than 90° the risks of intraoperative lens luxation or postoperative IOL dislocation are higher and the capsule should be supported during surgery. In these circumstances, flexible iris hooks, capsular retractors, and standard CTR should be mandatory. Moreover, modified CTR 1 and CTS 2 have the advantage that they can be permanently sutured to the sclera, and they are indicated in those eyes that present more than 6 h of zonular disruption. 8 However, when the capsular bag is compromised, an anterior vitrectomy should be performed at the beginning of surgery to avoid vitreous traction. 4 Moreover, an alternative technique for IOL placement should be considered according to the surgeon's skills and experience. 9 In cases of traumatic lens subluxations, the lens may be dislocated posteriorly, requiring a pars plana lensectomy with posterior vitrectomy. Other previously described surgical techniques are pars plana vitrectomy and intravitreal phacofragmentation, 10 pars plana vitrectomy and intravitreal phacoemulsification, 11 and perfluorocarbon liquid assisted phacoemulsification combined with pars plana vitrectomy.12,13
The creation of a centered and well-sized capsulotomy is widely recognized as the most difficult step in subluxated cataract surgery, as zonular instability reduces the counter-traction forces that facilitate the capsulorhexis. Femto-laser capsulotomy has been increasingly used, as it minimizes the amount of stress on the already compromised zonules. However, it is contraindicated in those eyes that present an anterior capsule that is too tilted or too posteriorly displaced. 14
A technique for managing a sinking dropped nucleus, posterior assisted levitation (PAL), was described by Packard and Kelman. 15 ,16 In brief, PAL consists of inserting a spatula downward via the pars plana with its tip inclined to the posterior pole of the eye, placing it behind the nucleus. The spatula lifts the partially dropped nucleus forward into the anterior chamber. Surgery is completed by extending the wound and expressing the nucleus or by phacoemulsification with the protection of a sheet glide. Moreover, Chang and Packard described a modified PAL technique using sodium hyaluronate 3.0%–chondroitin sulfate 4.0% (Viscoat) in 8 eyes with a posterior capsule rupture and a descending nucleus. 17 lifshitz et al in 2012 described the Planned-PAL (P-PAL) using the previously mentioned PAL technique in severe subluxated cataracts: with this technique, the subluxated lens (cum capsule) was pushed and lifted forward into the anterior chamber by the spatula and removed througha sclerocorneal incision. 18
On this basis, our technique founds its rationale. When there are no vitreoretinal abnormalities, the injection of Healon in the retrolental space lifting the subluxated cataract has two main advantages: the opportunity to perform a centered capsulorhexis and to offer a posterior support to stabilize the anterior chamber intraoperatively. Moreover, the use of Healon is gentler compared to the spatula allowing the preservation of the posterior capsule. Furthermore, the use of the Ahmed segment or Cionni ring allows the implant of the intraocular lens in the bag. Alternatively, different techniques of scleral fixated intraocular lens implantation revealing a good profile of safety and efficacy can be implemented. 19 ,20 One complication that may be encountered after surgery is a transient increase of the intraocular pressure secondary to the use of viscoelastic substances. However, the intraocular pressure elevation is usually temporary, peaking at 4 to 7 h postoperatively and returning to baseline within several days. 21 Moreover, it can be easily managed with topical or systemic medications.
In conclusion, retrolental cohesive ophthalmic viscoelastic injection could represent a novel effective surgical approach in recentering and elevating subluxated cataracts, to facilitate the capsulorhexis and reduce the risk of a pars plana approach.
Supplemental Material
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.