
Abstract
Purpose
Various surgical techniques have been described for managing persistent macular holes after an unsuccessful vitrectomy with internal limiting membrane (ILM) peeling. However, the closure and functional improvement rates after these procedures are limited. Therefore, the aim of this study was to evaluate the usefulness of radial retinal incisions (retinotomies) in eyes with persistent large macula holes despite previous vitrectomy with ILM peeling.
Design
In a retrospective case series, closure rate and best-corrected visual acuity (BCVA) were evaluated in eyes with persistent macular holes after an unsuccessful vitrectomy that included posterior vitreous detachment and ILM peeling.
Subjects
22 eyes of 22 patients (10 men and 12 women) underwent re-vitrectomy with radial retinal incisions. All the patients had undergone an unsuccessful surgery before.
Methods
Small-incision re-vitrectomy with radial retinal incisions (retinotomies) and air tamponade was performed.
Main Outcome Measurements
For all eyes, high-definition SD-OCT scans (SD-OCT Spectralis, Heidelberg Engineering GmbH, Germany) of the macula were routinely performed before surgery; 1 week and 1 month after surgery; and at final follow-up. Additionally, age, gender, axial length, macular hole diameter, biomicroscopic fundus evaluation and best-corrected visual acuity (BCVA) in logMAR and Snellen at baseline, 1 and 4 months after operation, and at the final follow-up visit were analyzed.
Results
The mean baseline macular hole diameter was 668.5 ± 226.8 μm. At the final examination, 16 (72.72%) of the 22 macula holes were closed. Visual acuity increased in 17 eyes, was stable in 3 eyes, and decreased in 2 eyes owing to central retinal atrophy in both. The mean BCVA increased from logMAR 1.04 ± 0.29 at baseline to 0.57 ± 0.31 (Snellen 0.11 ± 0.05 to 0.33 ± 0.18). In all successful cases, macula hole closure was attained after 3 days, and none of the eyes showed macula hole recurrence.
Conclusion
The results of this limited case series suggest that radial retinal incisions of the rim in persistent macula holes after initial surgery with ILM peeling increase the success rate of macula hole closure and results in a relevant increase in BCVA. However, as the number of eyes included in this series is limited, the results must be confirmed in a study with a larger sample size.
Keywords
Introduction
A full-thickness macular hole (FTMH) is a foveal dehiscence of all retinal layers that commences at the level of the internal limiting membrane and extends up to, but not including, the retinal pigment epithelium (RPE, Figure 1). The International Vitreomacular Traction Study (IVTS) group in 2013 subclassified FTMHs into small (<250 μm), medium (>250 to ≤400 μm), and large (>400 μm) according to the smallest aperture measured with spectral domain optical coherence tomography (SD-OCT).1,2 At the time of diagnosis, nearly half of FTMHs are large. 1
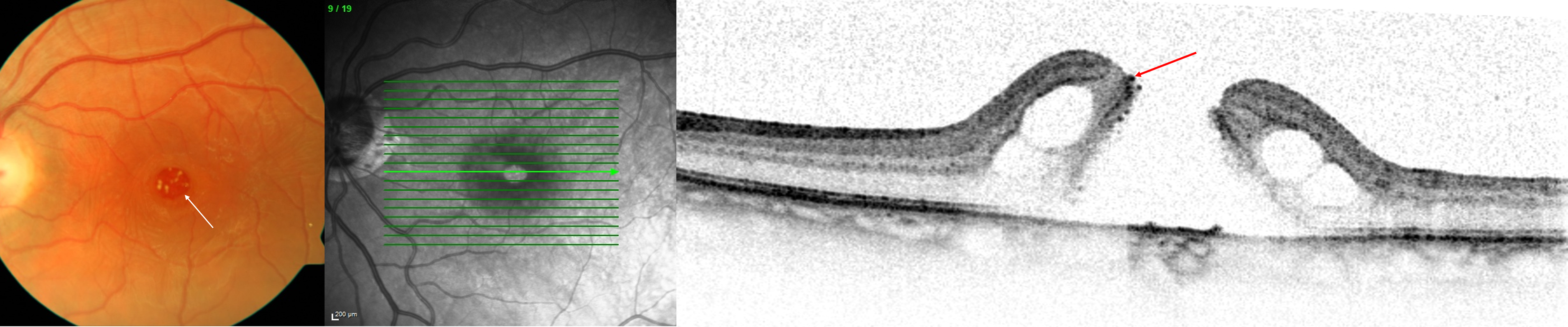
Typical appearance of a persistent macula hole presenting a fibrous-like ring at its rim, which may inhibit relaxation of the rim. White (left) and red (right) arrows indicate fibrous-like rings.
Pars plana vitrectomy (PPV) with induction of posterior vitreous detachment and internal limiting membrane (ILM) peeling is currently recognized as the gold standard treatment, with a closure rate of 91%–98%.3–7 Despite these encouraging outcomes, persistent FTMHs occur in 7%–44% of cases.8,9
Multiple surgical techniques for persistent FTMHs have been proposed. However, despite the many different strategies, no consensus has been reached regarding a standard treatment. The closure rate after reoperation for FTMHs has been reported to be as high as 47%–69%.10–16
Surgical approaches might involve repeated PPV with ILM re-peeling and endotamponade with long-lasting gas, 10 membranectomy and autologous serum, 17 autologous transplantation of ILM, 18 autologous retinal transplant, 19 lens capsular flap transplantation, 14 induction of macular detachment with a balanced salt solution (BSS),16,20–23 silicone oil tamponade, 24 autologous platelet concentrate,25,26 amnion membrane plug,15,27 and radial retinal incisions.28,29
The easy and straightforward technique for perifoveal radial retinal incisions (retinotomies) for persistent FTMHs has been described in single cases by other authors. It was successfully applied in persistent macular holes after vitrectomy and ILM peeling by our group in a larger number of eyes. In this retrospective case series, closure rate and Snellen visual acuity were evaluated in eyes with persistent macular holes after an unsuccessful vitrectomy with posterior vitreous detachment, ILM peeling, and endotamponade (air) with 3-day face-down positioning. Twenty-two patients (22 consecutive eyes) over a period of 6 years were included in this case series.
Methods
For all eyes, high-definition SD-OCT scans (SD-OCT Spectralis, Heidelberg Engineering GmbH, Germany) of the macula were routinely performed before surgery; 1 week and 1 month after surgery; and at final follow-up. The following parameters were retrieved from the patient files: age, gender, axial length, macular hole diameter on SD-OCT, observational period, and best-corrected visual acuity (BCVA) in logMAR and Snellen at baseline, 1 and 4 months after operation, and at the final follow-up visit (mean, 15.7 months).
All patients underwent an extensive eye examination, including best-corrected visual acuity (BCVA) testing, dilated fundus examination with slit-lamp biomicroscopy, and OCT at baseline and at the last follow-up.
Persistence of FTMH was defined as a FTMH that persisted after previous vitrectomy with ILM peeling for macular hole closure. The FTMHs were grouped according to the classification proposed by the IVTS group. 1 On the basis of the results of detailed analyses of the patients’ SD-OCT images, FTMHs were classified in clinical stages according to the IVTS Group classification system. Persistent macular holes with rims attached to the RPE and no cystic changes were not considered to need further surgery. The FTMH mid-length diameter (MLD) was measured on SD-OCT using the caliper function. The MLD was measured at the narrowest aperture of the FTMH.
Three-port 25-gauge small-incision vitrectomy was performed under peribulbar anesthesia in all patients by one experienced eye surgeon (CP). Vitrectomy included removal of the remaining anterior vitreous. Brilliant Blue G 0.125 mg (0.25 g/L; ILM-BLUE D.O.R.C, The Netherlands) was used to check for residual ILM around the macular hole. None of the cases had remaining ILM. Three radial retinal incisions (retinotomies) into the rim of the macular hole were made using vertical scissors (Disposable Vertical Microscissors: 25 gauge / 0.5 mm, DORC®). The incisions were placed and oriented to create minimal damage to the retinal nerve fibres (Figures 2 and 3). Due to an elevated rim in all cases, this could be performed without additional retinal tissue elevation or subretinal fluid injection (compare Figure 1).
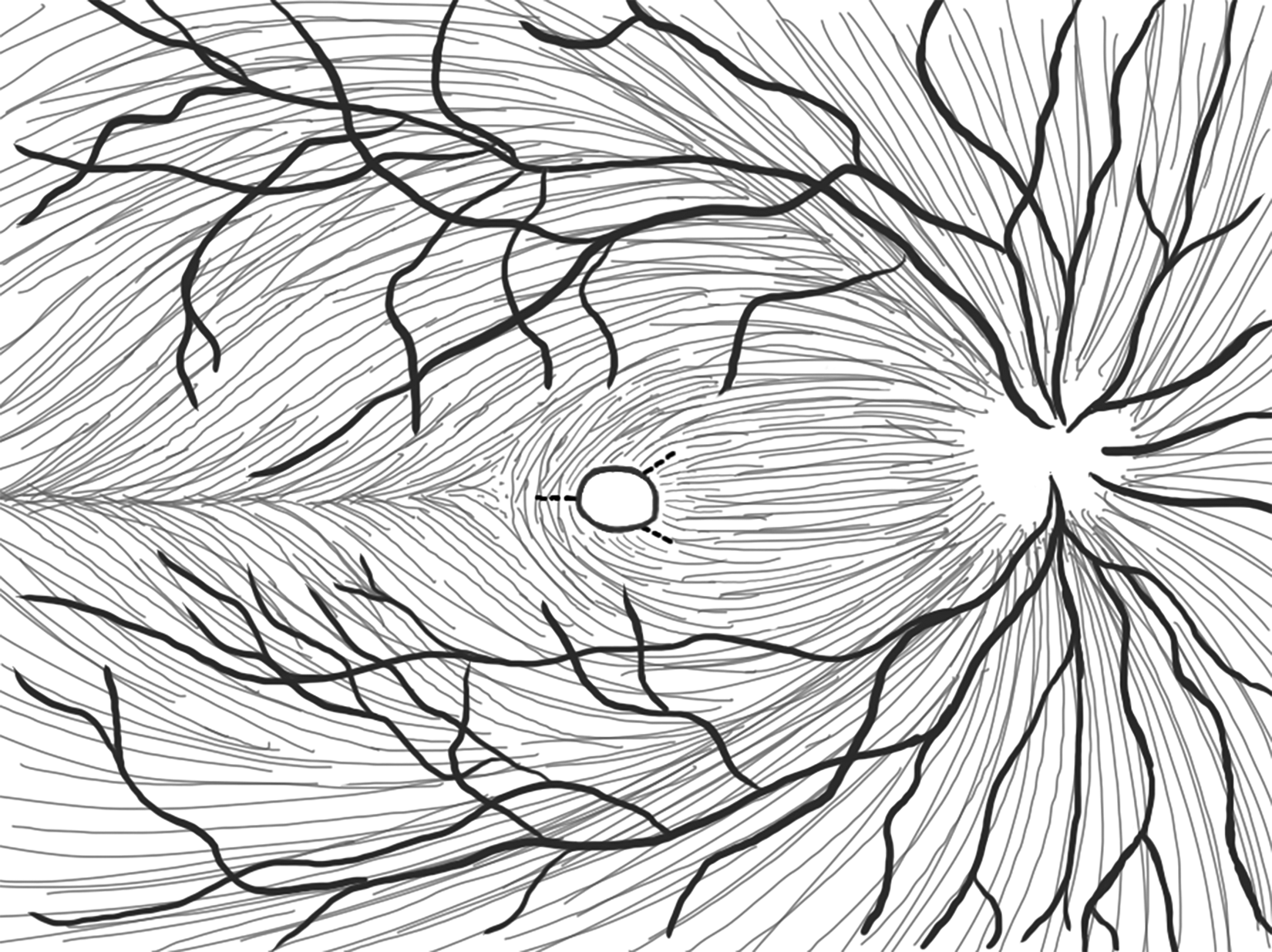
Radial retinal incisions (retinotomies) for the treatment of persistent macula holes. The incisions are located where damage to the retinal nerve fibres and central papillo-macula bundle of nerve fibres are best avoided.
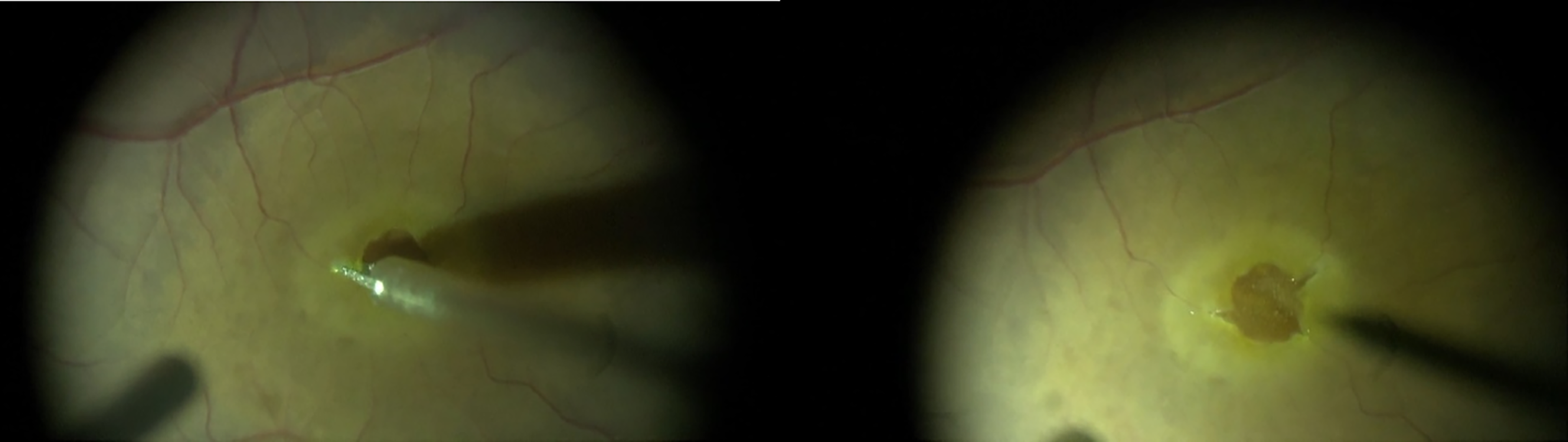
Radial retinal incisions (retinotomies) for the treatment of persistent macula holes. The incisions were made with a vertical scissor in the temporal, nasal superior, and nasal inferior positions to avoid the papillo-macular bundle of nerve fibres.
Finally, air tamponade was applied, and the patient was advised to maintain face-down positioning for 3 days.
According to the American Academy of Ophthalmology AAO, closure of the FTMH is defined as a flattening of the retina and reattachment of the whole circumferential rim to the retinal pigment epithelium. 30 We defined a successful closure of the macular hole as continous tissue in the fovea and graded it according to the definition of Rossi et al. and based on the postoperative OCT images. 31 Type O was counted as persisting FTMH (no closure). Macular hole closure was rated by two independent medical doctors and retinal specialists (C.P., H.C.).
Statistical analyses, including descriptive statistics, were performed for all outcome measures. Normal distribution of the data was tested using the Kolmogorov-Smirnov test. Parametric (paired t test) or non-parametric t tests (Wilcoxon matched-pairs signed-rank test) were applied to compare the preoperative and postoperative data.
The significance level was set at 0.05, and the results are reported as means and standard deviations, if not stated otherwise. In the statistical analyses, the MedCalc Statistical Software version 19.6 (MedCalc Software bv, Ostend, Belgium; https://www.medcalc.org; 2020) was used.
All patients signed an informed consent, the study adhered to the Declaration of Helsinki and was approved by the local ethics committee.
Results
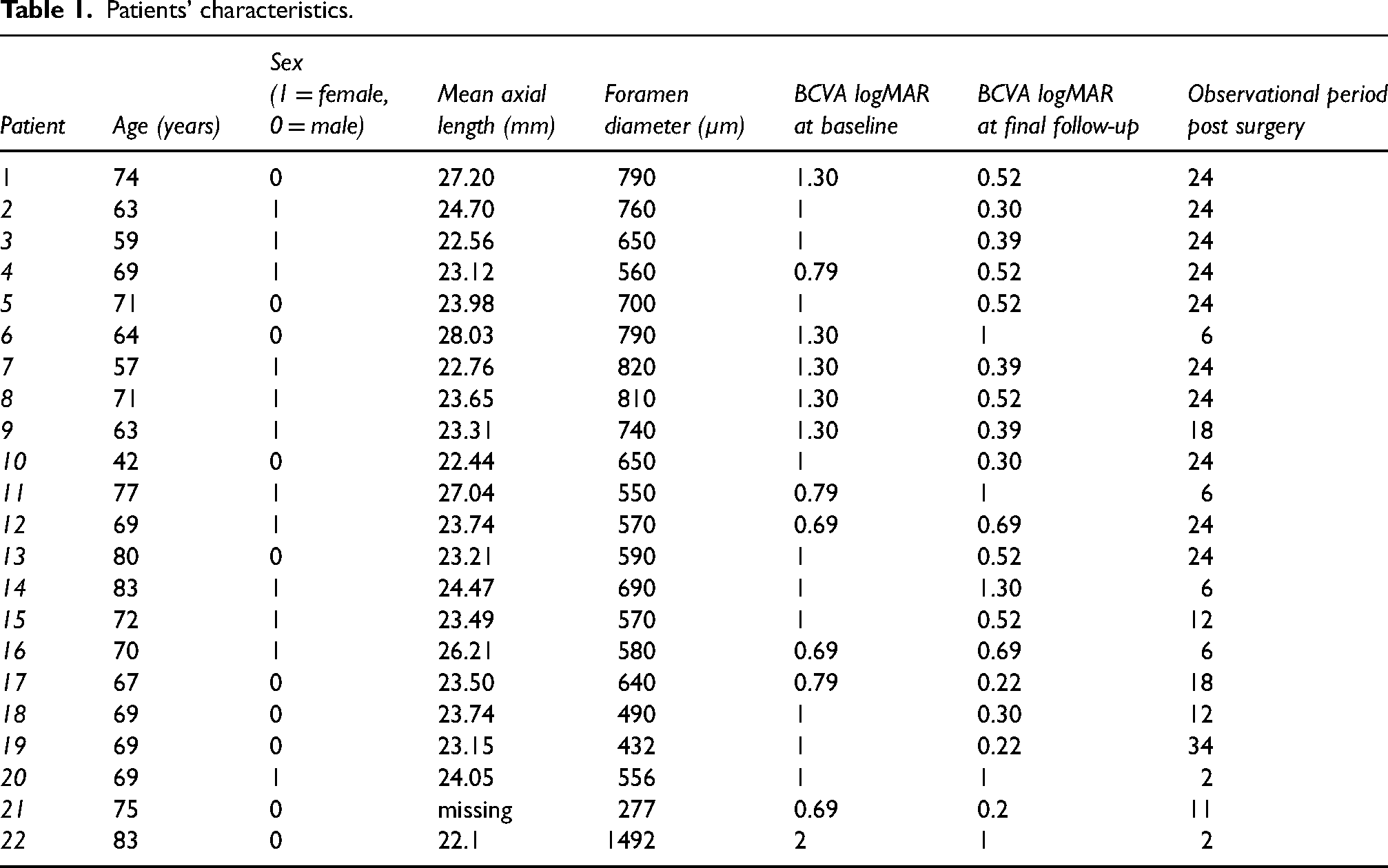
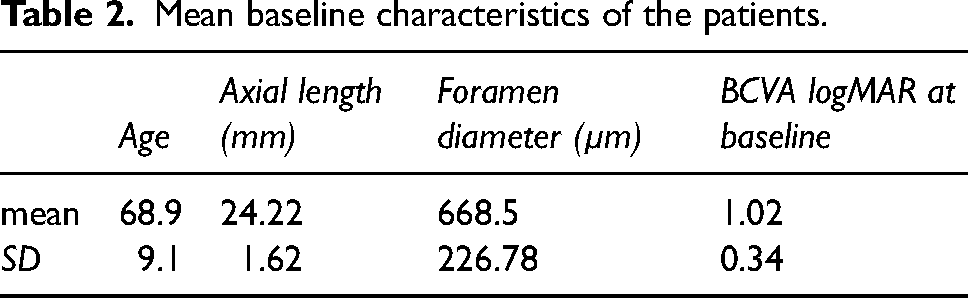
A total of 22 eyes of 22 patients (10 men and 12 women) underwent re-vitrectomy with radial retinal incisions. All the patients had undergone unsuccessful macular hole surgery before. The mean age at surgery was 68.9 ± 9.1 years (range, 42–83 years), and the mean axial length was 24.22 ± 1.62 μm. Of the 22 eyes, 20 (90.9%) had one unsuccessful prior surgery with ILM peeling for FTMHs and two had 2 prior surgeries. The mean baseline BCVA (logMAR) was 1.04 ± 0.29 (baseline BCVA Snellen: 0.11 ± 0.05), and the mean FTMH MLD was 668.5 ± 226.8 μm (range, 418–1000 μm; Tables 1 and 2).
Patients’ characteristics.
Mean baseline characteristics of the patients.
In 72.72% (16/22 eyes) of the eyes, type 1 closure of the FTMH was achieved after 3 days (Table 1, Figure 4), with a mean postoperative BCVA (logMAR) of 0.57 ± 0.31 (postoperative BCVA Snellen: 0.33 ± 0.18) at 17.0 ± 9.35 months after operation (Table 1). In 27.27% (6/22 eyes), type O presented post-surgery. Type OC appeared in 5 eyes, Type OB in one eye, type 1A in 14 eyes and type 1B in 2 eyes (Table 1).
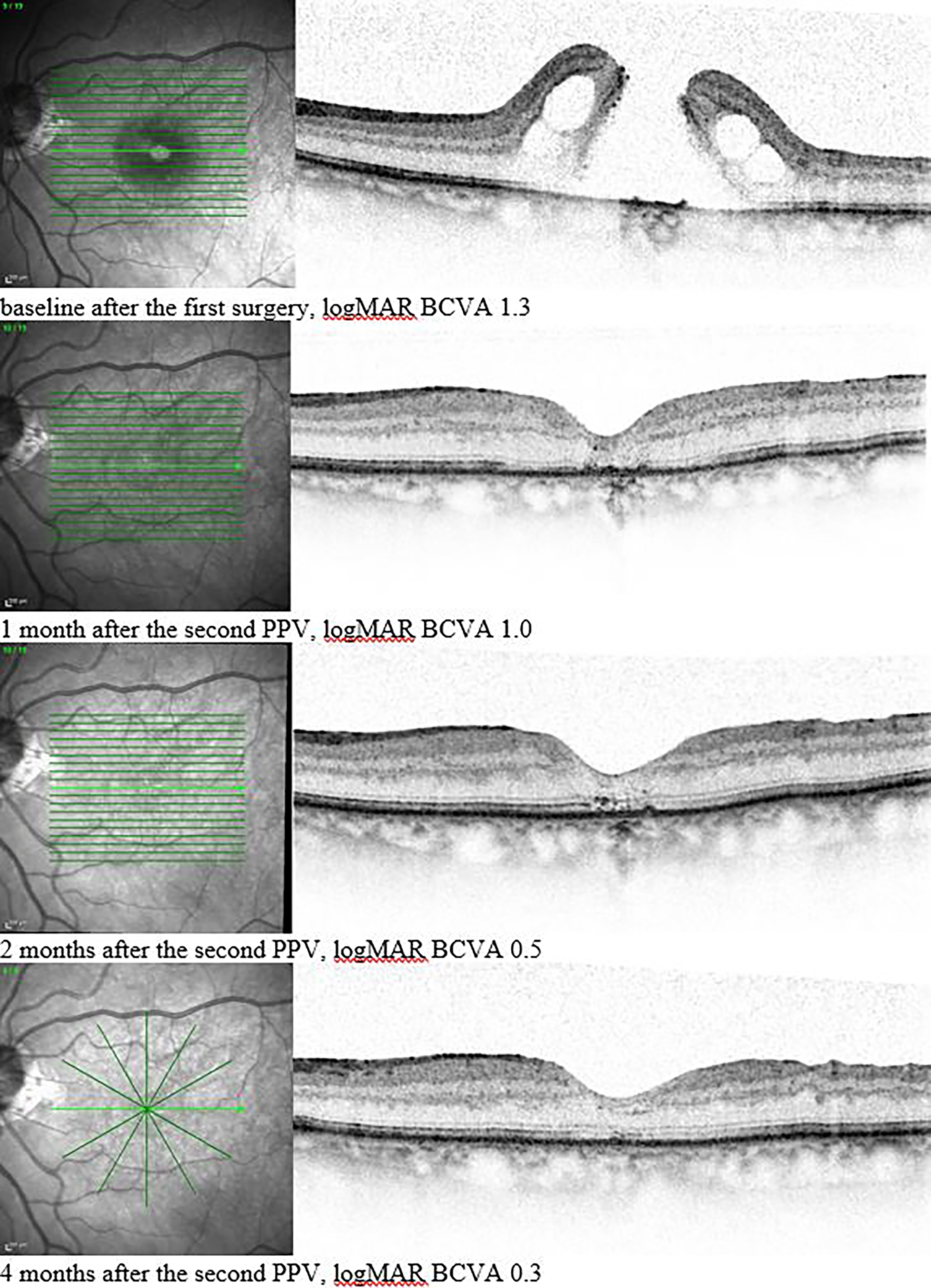
A large persistent macula hole after re-vitrectomy and treatment with relaxing radial retinal incisions and air tamponade. OCT images from the top to bottom were taken at baseline (after the first unsuccessful surgery) and 1, 2, and 4 months after re-vitrectomy. Note the restoration of the outer retina over time. In this particular case, the follow-up function in the OCT was not used to best depict the foveal structure. We are aware that this may limit the information on the morphologic correlation to other eye structures. 32
Visual acuity increased in 17 eyes, was stable in 3 eyes, and declined in 2 eyes. No reopening was observed during the observation period. The reference of microstructural changes on OCT, such as disruption of the ellipsoid zone or atrophy, are included in the closure classification according to Rossi et al. In no case, surgical complications led to appearance of microstructural changes or atrophy. Minor intraoperative hemorrhage did occur in 27,3% (6/22 eyes), but did not need any surgical intervention. Microstructural changes such as atrophy appeared in those eyes with type O.
In the Wilcoxon test for paired samples, the median differences in preoperative and postoperative BCVA logMAR and Snellen BCVA were −0.5 (p = 0.0003; 95% confidence interval, −0.68 to −0.24; Figure 5) and 0.23 (p = 0.0004; 95% confidence interval, 0.15–0.32), respectively.
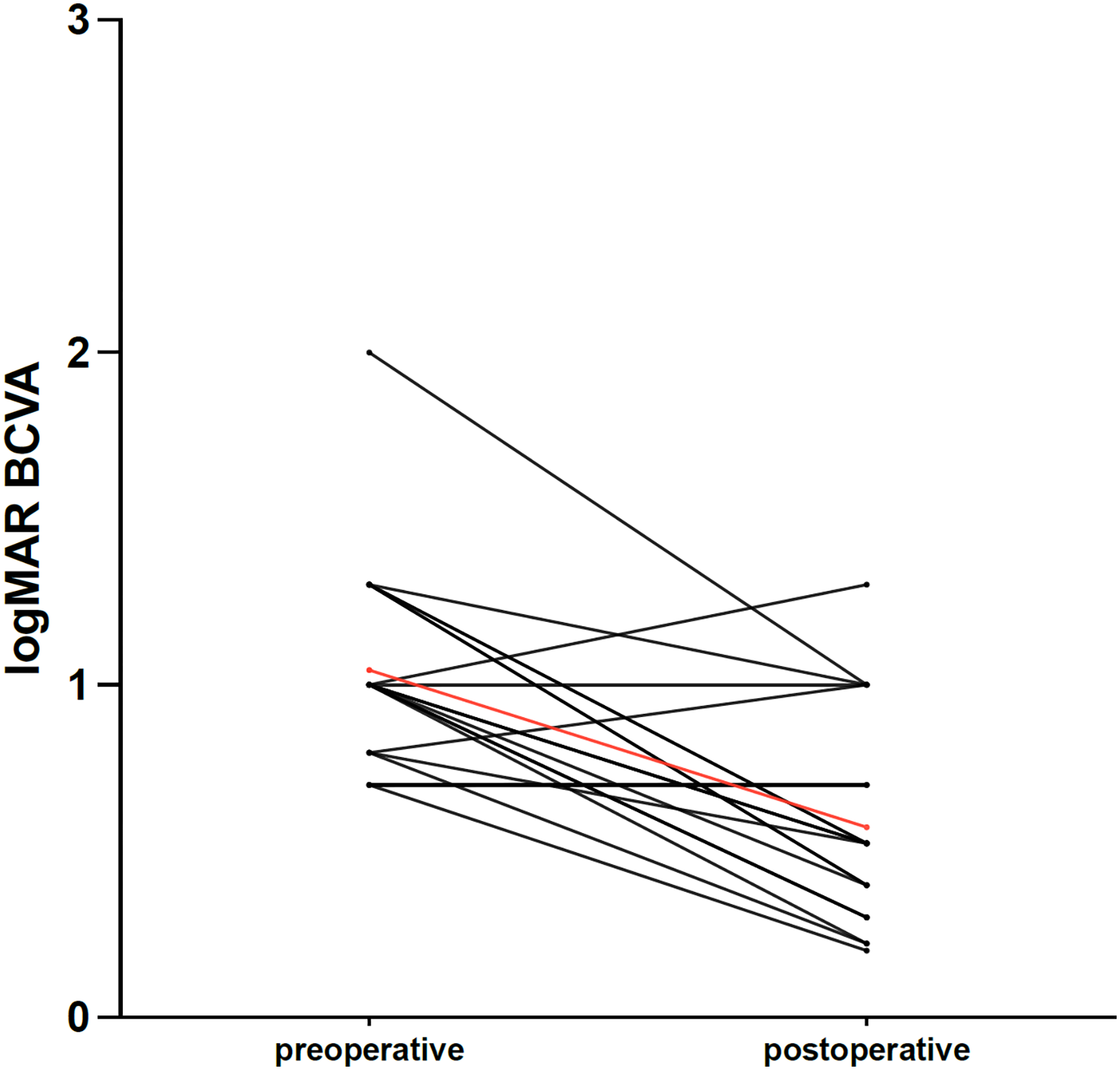
Individual evolution and average difference (in red) between preoperative and postoperative BCVA logMAR.
Discussion
The Vitrectomy for Macular Hole Study and the Moorfields Macular Hole Study have shown a clear benefit of surgical treatment for FTMHs.17,33 The primary closure rate after vitrectomy has been reported to range from 91% to 98%.3–7 A reliable prognostic factor for surgical success is the size of the initial macular hole and the absence of subretinal fluid at the border of the macular holes. 34 Defects of <400 µm have success rates of 92%–97%, whereas those of >500 µm have success rates <50%.9,28
For vitreoretinal surgeons, the management of macular holes that fail to close is challenging. FTMHs are caused by epiretinal tangential traction. Peeling the ILM and thereby eliminating tractive forces were found to be important steps for improving closure rates and preventing reopening.7,35,36 In a systematic review, the reopening rate was reported to be 7% without ILM peeling (125/1756 eyes), compared with 1% (44/3,724 eyes) with ILM peeling. 8
Large FTMHs might persist despite elimination of all tractive elements. Ip et al. reported persistent FTMHs in up to 44% of cases. 9 Anatomical closure of large FTMHs is desirable, even if the patient's objective BCVA does not improve, as it might minimize the central scotoma. 37
No general consensus has been reached regarding the management options for recurrent or persistent macular holes because of the insufficient large sample sizes in the current literature and the lack of randomized clinical trials. Multiple strategies have been proposed. An overall consensus is that secondary adhesions may prevent the hole from closing.
Michalewska et al. and Alpatov et al. described a surgical technique in which the borders of the hole were mechanically pushed together with forceps to relax tension and decrease the size of the hole.38,39 The anatomical results were slightly improved, but with poor functional success.
Gonvers et al. first introduced the application of a subretinal BSS around the fovea during the annual Jules-Gonin-Meeting 2002. 23 Meyer et al. suggested that secondary adhesions between the RPE and the retina prevent proper healing; thus, applying subretinal BSS around the fovea might solve this problem. 21
Reis et al. showed improvement of BCVA with complete closure of stage IV macular holes using a perifoveal incision technique after a previous failed closure in 7 patients 28 : five perifoveal retinal incisions were done radial as deep as the RPE near the borders of the hole. All seven patients had successful closure and a BCVA gain, the mean visual acuity gain was 5.6 lines, compared to 4.7 lines (logMar chart) in this patient collective. The incisions showed by Reis et al. are very similar to the ones demonstrated, and, as discussed later in more detail, may possibly favour healing through early RPE regeneration after trauma, as demonstrated by Michalewska et al. 38 The advantage of the demonstrated technique is, that less incisions are necessary, probably causing less trauma to the retina.
Charles et al. reported successful FTMH closure after temporal relaxing retinotomy in 5 (83%) of 6 patients 29 : through a vertical incision on the temporal parafovea and a simultaneous inward repositioning of the temporal retinal bridge using a 25-gauge soft-tip cannula, a vertical elongation and horizontal shortening of the macular hole is approached. This leads to an altered retinal configuration, which may allow for macular hole closure. The creation of a retinotomy in healthy retina causes traumatic damage to the underlying RPE because the retina is fully adherent, which is not the case in the presented technique with incisions placed in the elevated retina. Further, a retinotomy in healthy retina might well create an additional scotoma, which could not be demonstrated by Charles et al. due to poor fixation. In contrast to the study results of Charles et al, the visual outcomes presented in this case series are significantly better with a higher number of patients: Charles et al. reported, that 50% (3/6 eyes) had a stable visual acuity logMar 1 or below and failed to increase postsurgical. In comparison in the presented case series, only 22,7% eyes failed to improve significantly in visual acuity (three remained stable, two decreased due to central atrophy).
Smiddy also made short incisions at the margin of the hole to stimulate retinal gliosis but did not publish the outcome. 40
Our rationale for this surgical approach is based on the observation of a fibrous ring-like structure at the rim of persistent macula holes (Figure 3), which was suggested to prevent relaxation and closure of macula holes. 41 Perifoveal radial retinal incisions are used to counteract the stabilizing effect of this ring (Figures 1–3) and achieve persistent anatomical closure (Figure 4). The incisions are made in the temporal, nasal superior, and nasal inferior positions to avoid the papillo-macula bundle of nerve fibres and to best follow the course of the nerve fibres to minimize damage (Figures 1 and 2).
These results demonstrate that radial retinal incisions (retinotomies) are a straightforward, reasonable technique that leads to successful anatomical closure in >70% of cases of persistent FTMHs that are usually difficult to manage. Furthermore, this method results in a significant and relevant improvement in BCVA. Another advantage is, that it is an easy method without the need of external material like amnion membrane or complex preparations of patientś blood samples.
The exact pathophysiology of persistent FTMHs and the exact mechanism of hole closure are still widely unknown. Furthermore, various surgical approaches can result in macular hole closure with a highly variable success rate. However, a success rate of >70% was not achieved by other methods in larger case series. One might argue that performing perifoveal radial full-thickness retinal incisions might lead to hemorrhage, comparable to autologous platelet/serum concentrate technique. However, hemorrhage was observed only in a minority of cases in our approach (27,27%). Besides relaxing the tension of the rim of the macular hole using perifoveal radial incisions, retinal gliosis stimulation and, consequently, centripetal movement of the retinal tissue are suggested.28,40,42 Furthermore, a deep full-thickness incision through the retinal tissue might stimulate cell migration and proliferation. Such regenerative processes have been observed to occur in vivo after local trauma and have been described previously. 43 Further studies are necessary to identify the composition of the observed fibrous-like ring structure at the rim of persistent macula holes.
In summary, perifoveal radial incisions may provide vitreoretinal surgeons with a valuable alternative technique for closing persistent macular holes. In our case series, 72% of the eyes showed anatomical closure of the macular hole, with a significant mean visual improvement in logMAR BCVA of −0.47 (Snellen BCVA, 0.21) and no reopening during follow-up.
There are several limitations. This is a retrospective study with a lack of randomization to a control group. Furthermore, the number of eyes in this case series is limited. It would be valuable and great to confirm the present study results in a randomized controlled prospective study with a control group, a larger population size and a comparison to other methods. 44 However, implementation of such a study could pose some difficulties, as the caseload of patients with persistent FTMH is limited in all clinics. 44
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.